
Abstract
Objective:
To evaluate the efficacy of tranexamic acid (TA) in decreasing blood loss during and after open myomectomy for patients with 3 or more uterine fibroids.
Methods:
This prospective randomized trial was conducted among 132 women subjected to abdominal myomectomy. Patients were equally divided into 2 groups by simple randomization. The study group received perioperative intravenous TA while the control group did not. Intraoperative blood loss was calculated by measuring the volume in the suction apparatus and weighing the surgical swabs in addition to postoperative blood loss collected via a suction drain. Hemoglobin and hematocrit values were determined preoperatively and on the third postoperative day for all cases. Any adverse effects were recorded in both groups.
Results:
No significant difference was found between the two groups regarding age, body mass index, number, and size of myomas removed. The TA group showed lower amount of blood loss (407 mL) when compared to control group (677 mL; P < .01). Risk estimation has revealed that treatment with TA resulted in decrease in risk of perioperative blood loss by 40%. In the study group, 13 (19.7%) patients required blood transfusion in contrast to 23 (34.8%) patients in the control group (P < .01). Hemoglobin and hematocrit levels were significantly lower in the control group on the third postoperative day (P value = .001) .
Conclusion:
The TA reduces blood loss during and after myomectomy for patients with multiple uterine fibroids.
Introduction
Uterine fibroids represent a major health problem, with approximately 235 million women affected throughout the world, and up to 40% of women may be diagnosed with uterine myomas at a time during their lives. However, symptomatic myomas warranting treatment are present in only 25% of cases. 1
Myomectomy is the standard surgical option for many women who have myomas and desire future childbearing or simply want to preserve their uterus. Several routes for myomectomy are available including laparotomy, laparoscopy, and hysteroscopic approaches. Some authors have advocated laparoscopic myomectomy as a preferred method of myomectomy due to reduced bleeding, better patient compliance, and reduced postoperative adhesions. Those who choose laparoscopy as a first-line therapy should have adequate laparascopic operative equipment and expertise, especially with laparoscopic suturing. 2 Moreover, laparoscopic myomectomy is a safe and effective alternative to open myomectomy with no more than 3 symptomatic uterine myomas and with myomas not larger than 7 cm. 3 On the whole, laparotomy or open myomectomy is still considered the standard technique applied to most of the patients. 4
Perioperative blood loss during myomectomy is one of the major complications of the procedure. Dissection of uterine myomas can be associated with massive blood loss that might be quite challenging to the point that hysterectomy could be indicated to control bleeding. 5
Several modalities were suggested to control bleeding during myomectomy. In a Cochrane database systematic review, Kongnyuy and Wiysonge have found the following modalities more effective in controlling myomectomy-associated bleeding compared to a placebo or no treatment: misoprostol, vasopressin, bupivacaine plus epinephrine, tranexamic acid (TA), mechanical tourniquet, and chemical dissection with sodium-2-mercaptoethane sulfonate (mesna). 4
Direct vascular damage during myomectomy is a major cause of bleeding; however, tissue injury-induced fibrinolysis is a major contributing factor in coagulopathy and bleeding. 6 The contribution of each item to the amount of bleeding during mymoectomy is not known, however, it seems logical that with sticking to the sound surgical techniques as careful dissection and control of small bleeding vessels, local tissue hemostasis will be more important in defining the amount of bleeding.
Tranexamic acid is a potent plasminogen inhibitor agent that exerts its effect by blocking lysine-binding sites on plasminogen molecules, thus enhancing the effectiveness of the patients’ own hemostatic mechanisms. Consequently, fibrinolysis is inhibited, and excessive or recurrent bleeding is reduced. 7 Therefore, TA is widely used during and after major surgical procedures including general, cardiothoracic, and orthopedic surgeries, and recently cesarean deliveries were added to the list. 8 –10
It seems plausible and appealing to apply the same principle of antifibrinolytic strategy during myomectomy. However, very few studies have addressed this issue. Caglar et al in randomized controlled study have studied the effect of intravenous TA prior to myomectomy. They found that there were no overall benefit from the use of perioperative intravenous TA. However, in a small group of patients with multiple myomas, a significant difference was shown, 11 an observation that led us to conduct this study evaluating the effect of perioperative TA on a larger number of patients with multiple uterine fibroids undergoing myomectomy
Materials and Methods
After approval of local ethics committee, this prospective randomized clinical trial was conducted among women subjected to abdominal myomectomy during the period from the start of February 2014 to the end of April 2015 at Obstetrics and Gynecology Department of Suez Canal University Hospitals. We included women scheduled for myomectomy due to intramural myomas after informed consent for participation in our study. Only women with 3 or more corporeal intramural myomas were included. Women with malignancy evidenced by dilatation and curettage (D&C) biopsy or suspected by imaging, those with history of thromboembolic disease, anticoagulant users, or those with body mass index (BMI) ≥30 were excluded. High BMI was excluded to avoid its confounding effect on duration of surgery and possibly an increased amount of bleeding caused by difficult surgery. Other exclusion criteria were women having systemic medical diseases (cardiac, hepatic, renal, etc) or TA allergy. The required sample size was calculated based on power of the study of 80% and α-error of .05. 12
Women eligible for the study (n = 132) were divided into study and control groups. Each group comprised 66 women, fulfilling the selection criteria and undergoing abdominal myomectomy. Randomization was performed by a simple randomization method using sealed envelopes, half of which contained notes labeled as “study group” and the other half was labeled as “control group.” Eligible women were asked to choose one of these envelopes to determine the group to which she would be allocated.
The study group received an explanation of the study. Ten minutes before the start of surgery, included women received 10 mg/kg of TA (Kapron, Amoun Co, Egypt) diluted in 20 mL dextrose 5% and given slowly intravenously over 5 minutes (maximum 1 g) followed by a continuous infusion of 1 mg/kg/h dissolved in 500 mL of dextrose 5% for 6 hours (maximum 1 g/6 hours), meanwhile the control group did not. This means that women enrolled in the study and the clinical care teams were not blinded to the intervention and were aware of TA administration.
Before skin incision, all patients received prophylactic antibiotic in the form of ceftriaxone 1 g intravenously (Cairo Co, Egypt). The operations were performed as standard through midline or pfannensteil incision by one or more of the authors to ensure consistency of study procedures. All patients received general anesthesia.
After skin incision, the subcutaneous fat and abdominal fascia were opened crosswise, and the rectus muscle was opened on the midline. The parietal peritoneum was opened longitudinally to reach the pelvic cavity. Subsequently, a self-retaining retractor was inserted, and intestine was packed. Uterus was inspected for number, location, and shape of myomas, and other pelvic organs were inspected for associated pathology. When possible, uterine incisions were performed on the anterior wall or the fundus in order to reduce postoperative adhesions. The incision was performed using monopolar diathermy. Intracapsular enucleation of myomas was performed by gently dissecting between the myoma and the pseudo capsule. The myoma was grasped by Collins forceps and gently enucleated out. Meticulous hemostasis was secured by low-voltage coagulation (<30 W) of feeding vessels. Myoma bed was closed by 1 or 2 layers of interrupted vicryl sutures (Vicryl 1–0 polyglactin 910; Egycryl, Taisier CO, Egypt). No mechanical tourniquet or local vaso-occlusive drugs (eg, vasopressin) were used intraoperatively.
At the end of the surgery, 1 intraperitoneal suction drain was routinely used in all patients and the volume in the drain bag was measured every 12 hours and on removing the drain. The drains were removed on the third postoperative day unless otherwise indicated. Number and size of myomas were recorded. Myoma size represented the mean size of each myoma. Enucleated myomas were sent for histopathological examination.
Total bleeding was calculated as intraoperative and postoperative blood loss. Intraoperative blood loss was estimated by the scrub nurse by drying up all blood in the surgical field with swabs and then weighing them. The weight of the dry surgical swabs (roughly 28 g for each 30 × 30 cm abdominal swabs) is measured before use and after being wet or soaked by blood. A highly accurate digital balance is used to measure the weight in grams. The weight difference is translated into the blood loss considering that 1 g is equal to 1 mL blood. The quantity of blood loss (mL) equals (weight of the used materials − weight of the materials prior to the surgery) in addition to the blood collected in the suction apparatus after evacuation. Meanwhile, postoperative blood loss was defined as the blood volume found in the suction drain. 11
Both study and control groups were checked for vital signs (blood pressure, heart rate, and respiratory rate) before and after myomectomy. The following routine investigations, CBC, PT, PTT, ALT, AST and serum creatinine, were performed preoperatively for both groups, and CBC was repeated on the third postoperative day.
Any adverse effects in either group were recorded. The need for blood transfusion either intraoperatively or postoperatively was also recorded. Intraoperative blood transfusion was governed by clinical condition and amount of blood loss. Postoperative blood transfusion was indicated if hemoglobin (Hb) percentage was <7 g/dL with relevant clinical manifestations. Women were reviewed again 1 week after the operation. In addition to the usual follow-up, women were checked for manifestations of thrombosis.
Data were processed using SPSS version 15 (SPSS Inc, Chicago, Illinois). Data quantities were expressed as mean ± standard deviation, and qualitative data were expressed as numbers and percentages. For quantitative variables, Student t test was used to test significance of difference, and χ2 was used to test significance for qualitative variables. A 2-sided P value <.05 was considered statistically significant.
Results
Baseline patient characteristics at myomectomy of both study and control groups are presented in Table 1. The mean age of patients was 35 years and 34.6 years in both groups, respectively. No statistical difference was noted regarding the mean number of myomas (4.87 in study group versus 5.11 in control group, respectively) or the mean size of myomas (9.96 cm and 10.48 cm in both groups, respectively). Both groups were also matching regarding body mass index (BMI) parity and preoperative Hb level.
Baseline Characteristics of the Studied Groups.
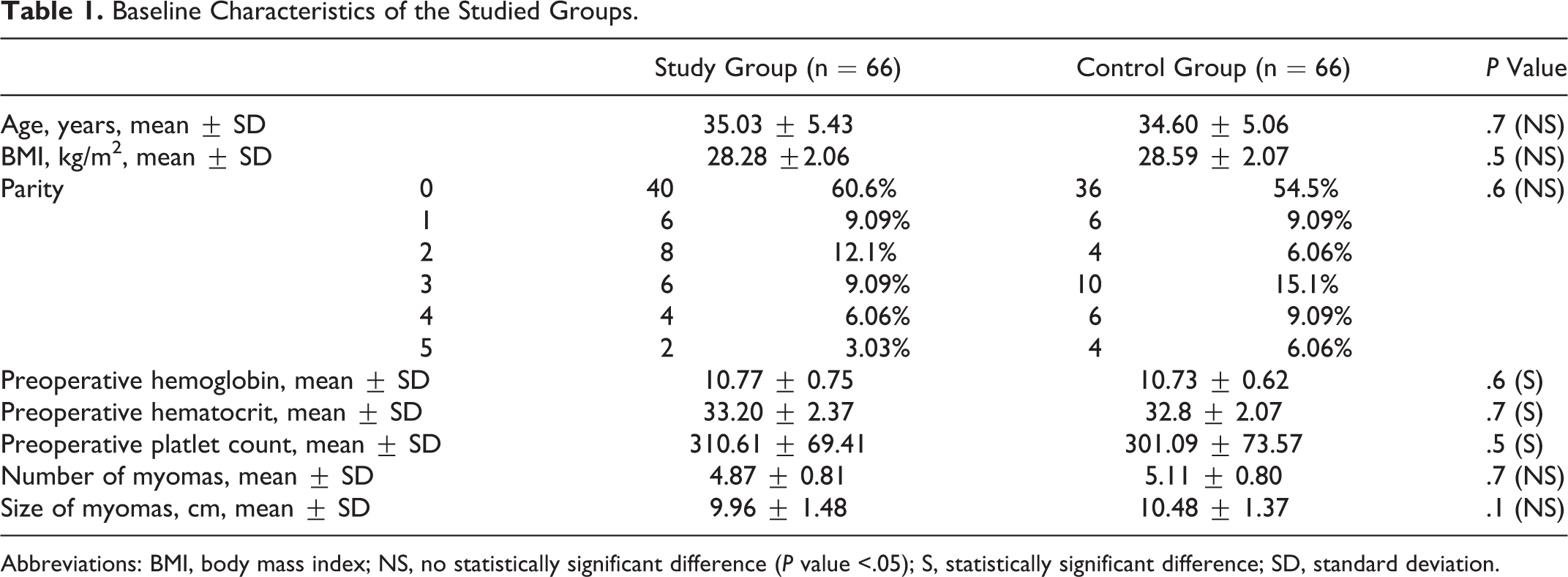
Abbreviations: BMI, body mass index; NS, no statistically significant difference (P value <.05); S, statistically significant difference; SD, standard deviation.
The study group showed shorter duration of surgery (75.9 vs 86.7 minutes for control group; P = .04) and lower total amount of blood loss (407 mL) when compared to the control group (677 mL). This total blood loss was the sum of blood lost during the period of surgery and postoperative period; both were significantly lower in study group and was 40% lower than in the control group (P < .01). Postoperative Hb and hematocrit levels were significantly higher in the study groups (9.09% and 29.00% vs 8.23% and 26.77%, respectively). No difference in postoperative platelet count was noted. Thirteen (19.7%) patients in the study group required blood transfusion in contrast to 23 (34.8%) patients in the control group (P < .01; Table 2).
Operative and Postoperative Results in the 2 Groups.
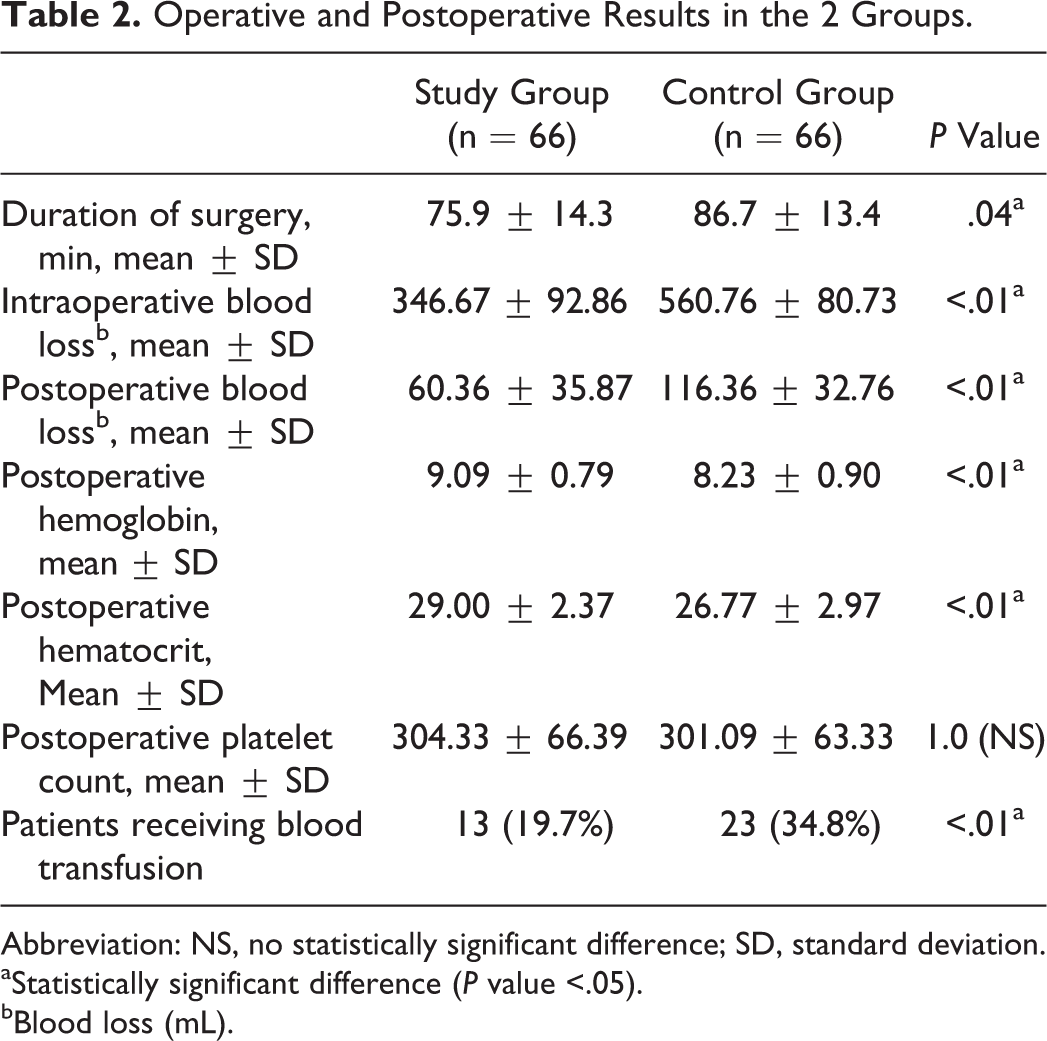
Abbreviation: NS, no statistically significant difference; SD, standard deviation.
aStatistically significant difference (P value <.05).
bBlood loss (mL).
Minor side effects in the form of nausea and vomiting were significantly higher in the study group (12.1% and 9.1% vs 1.5% and 1.5%, respectively). No patients in either group developed diarrhea. Major side effects in the form of deep venous thrombosis and anaphylaxis were also absent in both the groups (Table 3). Histopathological examination of enucleated myomas has shown no evidence of malignancy in any patient in either group.
Side Effects of the 2 Groups.
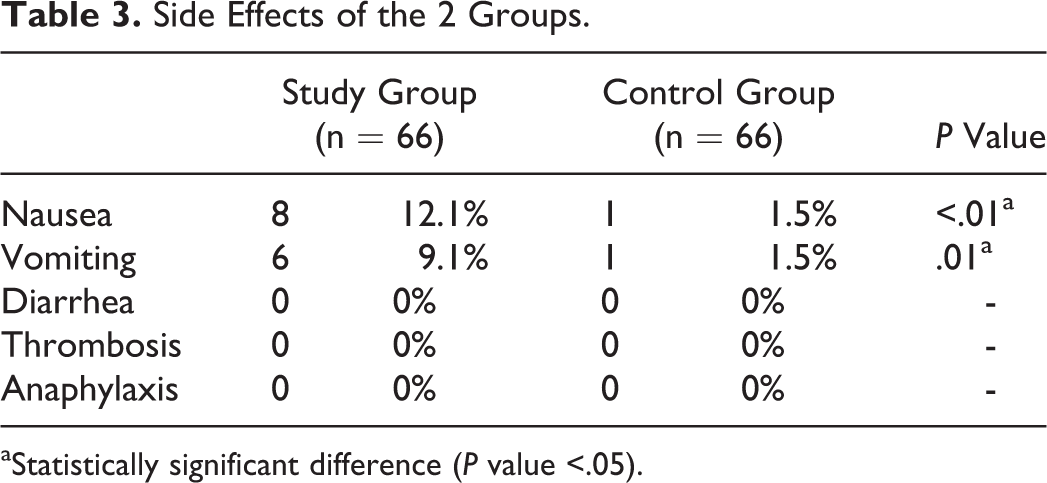
aStatistically significant difference (P value <.05).
Discussion
Our study shows that the use of TA 10 minutes prior to the start of myomectomy helps to reduce the blood loss during and after the operation. The mean difference of 270 mL represented about 40% of the total blood loss and was both statistically and clinically significant.
Tranexamic acid is one of the famous adjuvant drugs used to reduce intraoperative bleeding. It is widely studied in surgical and orthopedic fields and recently in obstetrics field with proven success. 10 We opted to study its effect during myomectomy which is a common operation performed for a relatively prevalent disease in our country. 13 The standard procedure of abdominal myomectomy was performed by one or more of the authors to ensure consistency. The regimen of intravenous TA administration was followed per instructions of the manufacturer.
The only randomized controlled study comparing the effect of preoperative intravenous TA and placebo on 100 women undergoing myomectomy 11 has shown no difference in perioperative blood loss or need for postoperative blood transfusion between the 2 groups. However, when a smaller group of patients (44 patients) with multiple myomas (3 or more) was compared to placebo, a difference in the amount of blood loss and duration of surgery was shown in favor of TA group, an observation that led us to conduct this study on such a group of patients at a wider scale. We affirmed that observation suggested in the first study by proving a beneficial effect of TA on 132 women undergoing myomectomy for multiple uterine myomas. The most probable explanation for the effect of TA to be pronounced only in this group is that excessive tissue trauma associated with dissection of multiple myomas induce excessive fibrinolysis that can be improved by the use of TA.
In the present study, no patients were excluded as a result of TA allergy, and all included women completed the follow-up with no drop out since they were in hospital throughout the course of the study. We found a statistically significant difference between the 2 groups as regards the operative duration, amount of blood loss either intra- or postoperatively, postoperative Hb concentration, and the need of blood transfusion.
It is well known that concentration of plasminogen activator is increased 30 minutes after the start of the operation and 14 Suppression of the elevation in plasminogen activator by TA to enhance the effectiveness of the patients’ own hemostatic mechanisms. Consequently, fibrinolysis is inhibited, and excessive or recurrent bleeding is reduced. 7 We anticipate that this effect is exaggerated with excessive tissue trauma as that associated with dissection of multiple uterine fibroids.
As regards side effects, there were no thromboembolic incidents in any of our 134 women in both groups. However, there were few minor side effects, mostly gastrointestinal upset in the form of nausea and vomiting in women who received TA. Current evidence states that TA is generally well tolerated. Adverse events are uncommon and usually manifest as nausea or diarrhea. 15
The study has few limitations. The study was not blinded to either patients or the clinical team, and hence a potential source of observation bias exists. Every effort was made to make the assessment of blood loss as objective as possible.
Conclusion
Tranexamic acid is an effective drug that significantly decreases blood loss during myomectomy in patients with multiple uterine fibroids with tolerable side effects, mainly gastrointestinal. Its use in those cases may be considered, especially when blood loss is expected to be high or in patients with anemia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.