
Abstract
Preeclampsia is an important cause of maternal and perinatal morbidity, especially in first-time pregnant adolescent women. Although prevention of preeclampsia has been attempted for many decades, effective intervention can only be achieved upon the full elucidation of the risk factors and mechanisms of disease. As the pathogenesis of preeclampsia during adolescence may differ from that in older women, preventive interventions should be tailored accordingly. During adolescence, 4 putative drivers of preeclampsia can be identified. First, uterine immaturity in very young teenagers is likely a major cause of defective deep placentation and adverse reproductive outcome, underscoring the importance of educational programs and public health initiatives focused on teen pregnancy prevention. Second, the association between adolescent obesity and preeclampsia merits further studies on the benefits of weight loss and dietary interventions to improve pregnancy outcome. Third, there is a need for greater awareness of the link between cardiovascular risk factors in young women and early-onset preeclampsia associated with atherosclerosis of the uteroplacental arteries. Finally, infrequent menstruations may prolong uterine immaturity because of lack of “menstrual preconditioning.” This risk factor may be amenable to pharmacological/hormonal preconditioning prior to conception.
Keywords
Introduction
How to prevent preeclampsia (PE) has been debated for more than 70 years. 1 A landmark publication was a report by Hamlin in The Lancet in 1952 entitled “Prevention of preeclampsia.” 2 Allegedly inspired by the astonishing low incidence of PE in Ethiopia, 3 Hamlin, who worked at The Women’s Hospital, Sydney, Australia, reported a marked reduction in the incidence and severity of PE, as well as eradication of eclampsia, following implementation of an Ethiopian-like diet (high-protein, high-vitamin, and low-carbohydrate) and strict weight control in pregnancy. 2 Despite the apparent success of this dietary intervention, the focus soon shifted toward drug prevention. In 1985, Beaufils et al published the first randomized pilot study on the use of dipyridamole and aspirin to prevent PE. 4 This was followed in 1986 by the study from Wallenburg et al, 5 which reported the first randomized, double-blind, placebo-controlled trial of low-dose aspirin only for the prevention of pregnancy-induced hypertension (PIH) and PE. Forty-six normotensive women, deemed at risk of PE because of a rise in blood pressure following intravenous angiotensin II infusion, were randomized to either low-dose aspirin (60 mg/d) or placebo at 28 weeks of pregnancy. The incidence of PIH, PE, or eclampsia in the placebo group was 25%. In the treatment arm, only 4.2% of the women had mild PIH and none had PE. 5 More than 3 decades on, the debate around aspirin prevention of PE and other obstetrical disorders shows no signs of abating. 6 A major hurdle in any prevention program is to tailor or personalize the intervention to individual risk factors. A recent reanalysis of seminal but often neglected studies on uterine development and maturation led us to conclude that the pathological triggers of PE in adolescents may differ from that in adult women. 7 Since the consequences of a pathological pregnancy are especially troublesome for teenage girls, we expand here on the biological processes that make adolescence a vulnerable developmental period for pregnancy and explore which preventative interventions should be considered to mitigate the risk of poor reproductive outcome in young and very young women.
Adolescent Pregnancy and Risk of PE
The global adolescent birth rate has declined from 65 births per 1000 women in 1990 to 47 births per 1000 women in 2015. 8 Although these figures suggest overall progress, the overall population of adolescents continues to grow and projections indicate that the number of adolescent pregnancies will increase globally by 2030, with the greatest proportional increases in first-time pregnant adolescent women in Africa. 9 Adolescent pregnancy is not a problem confined to low- and middle-income countries. For example, in the United States alone, a total of 229 715 babies were born in 2015 to women aged 15 to 19 years, for a birth rate of 22.3 per 1000 women in this age-group. 10 Although the rates are declining across all ethnic groups in the United States, they still remain much higher compared to many other developed countries. In the European Union, the United Kingdom continues to have a high birth rate in 15- to 17-year-olds (6.8 per 1000), especially when compared to countries such as Denmark (1.1 per 1000) or the Netherlands (1.3 per 1000). 11
First-time pregnant adolescent girls are at increased risk of obstetrical disorders, including preterm birth (PTB) and PE (Figure 1). For example, a recent population-based epidemiological study by Leppalahti et al in Finland found that the youngest group of teenagers (13-15 years) is at increased risk of PE and PTB compared to 16-year-olds. 12 The study concluded that the younger the expectant mother, the greater the risks of neonatal and maternal complications, including PE. Another study carried out in a tertiary center in Greece showed significantly higher incidence rates of PTB, preterm premature rupture of the membranes, PIH, and PE among teenage mothers aged 12 to 19 years. 13 The authors stressed that obstetricians should be aware of these increased risks in order to improve obstetrical outcome of childbearing teenagers. A retrospective investigation from Turkey and a prospective study from India also reported a higher incidence of PE in young first-time mothers, aged 12 to 19 and 13 to 19 years, respectively. 14,15 Further, Kawakita et al reported a retrospective cohort study from 19 hospitals in the United States with 43 537 first-time pregnancies in women younger than 25 years, which included 1189 young adolescents (age <16 years), 14 703 older adolescents (age 16-19.9 years), and 27 645 young adults (age 20-24.9 years). Again the authors found that young adolescents are at increased risk of a range of adverse pregnancy complications, including PE and PTB. 16 On the other hand, Blomberg et al found no increased risk of adverse neonatal outcome in teenagers, except for PTB before 32 weeks. 17 In this Swedish study, very young teenagers were grouped with the older teenagers, which may have masked the effect of age on the incidence of PE.
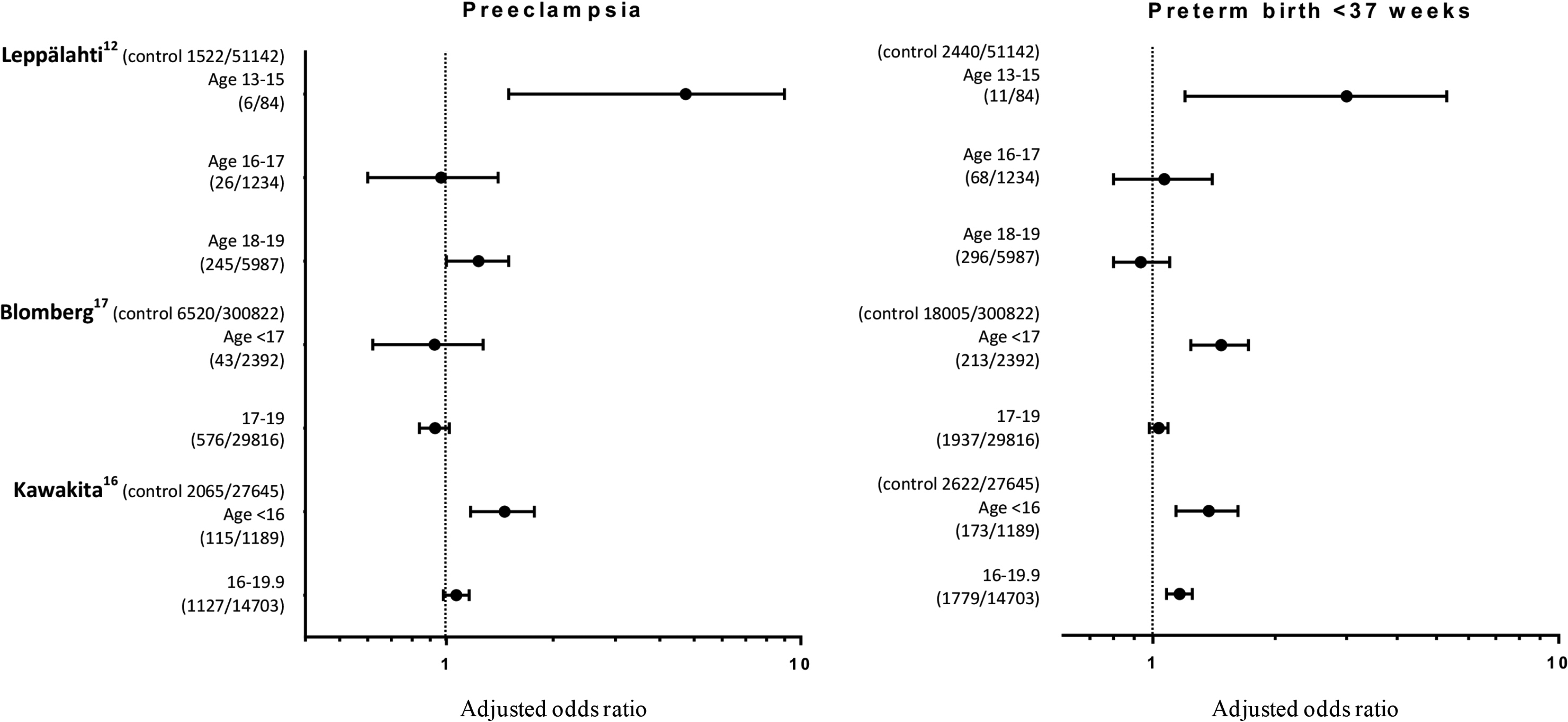
Forest plots of adjusted odds ratios of preeclampsia and preterm birth in adolescents stratified by age. The y-axis indicates the frequency of preeclampsia (left panel) or preterm birth (right panel) in each age group. The age range of control patients in the studies of Leppalahti et al, Blomberg et al, and Kawakita et al was 25 to 29, 25 to 29, and 20 to 24.9 years, respectively.
Uterine Factors in Adolescent PE
It is widely accepted that major obstetrical syndromes, including PE, fetal growth restriction (FGR), and PTB, are the consequence of severe uteroplacental vascular pathology with origins in early pregnancy. 18 The formation of a deeply invasive hemochorial placenta requires intense tissue remodeling of the uterus involving all endometrial cellular compartments. 19 It has been argued that regular cycles of menstrual shedding and tissue regeneration are essential to bestow the uterus with the essential plasticity and stress resistance to accommodate the intense tissue remodeling and vascular adaptation effected by the deeply invading trophoblast. 20 The concept that “menstrual preconditioning” is important for successful pregnancy is supported by the observation that gynecological age, defined by age in years at conception minus age at menarche, is a better predictor of adverse pregnancy outcome in adolescent mothers than chronological age. 21 Further, large population-based retrospective cohort studies consistently found that the incidence of adverse pregnancy outcome increases with decreasing maternal age, independently of known sociodemographic confounders of teenage pregnancy. 22 All these observations point toward intrinsic uterine factors as being the primary drivers of the increased risk of complications in very young mothers.
Defective Deep Placentation
Deep placentation involves progressive remodeling of ∼50 spiral arteries into large sinusoidal vessels capable of meeting the metabolic demands of the growing fetus throughout pregnancy. 18 Using methods developed by Hamilton and Boyd for anatomical studies, 23 uterine spiral artery changes associated with PE were first investigated in 14 cesarean hysterectomy specimens, including 3 specimens with the placenta in situ. 24 These specimens were obtained from 8 normotensive women and 6 patients with severe hypertensive disease. Full-size, step-serial tissue sections of the placental bed were made to trace the spiral arteries from the inner myometrium, also termed the uterine junctional zone (JZ), up to their opening in the intervillous space. This method not only enabled tracing back sinusoidal decidual vessels to their origins in the myometrium, and thereby identified these vessels as remodeled uteroplacental spiral arteries, but also revealed for the first time the vascular pathology associated with PE. 24,25 The primary site of vascular anomalies in PE is the proximal part of the spiral arteries within the uterine JZ. 26,27 Apart from a few vessels that supply the very center of the placenta, JZ spiral arteries in PE do not exhibit evidence of adequate physiological remodeling and retain their musculoelastic structures. 28 Moreover, in case of PE superimposed on preexisting hypertension, atherosclerosis was prominent in JZ spiral arteries (Figure 2). Robertson et al 25 noted that these arterial lesions in the placental bed have significance far beyond pregnancy. Indeed, the relation between altered hemodynamics and arterial disease, as well as the regression of atherosclerosis upon involution of the uterus during the postpartum, may be relevant to our understanding of systemic arterial disease.
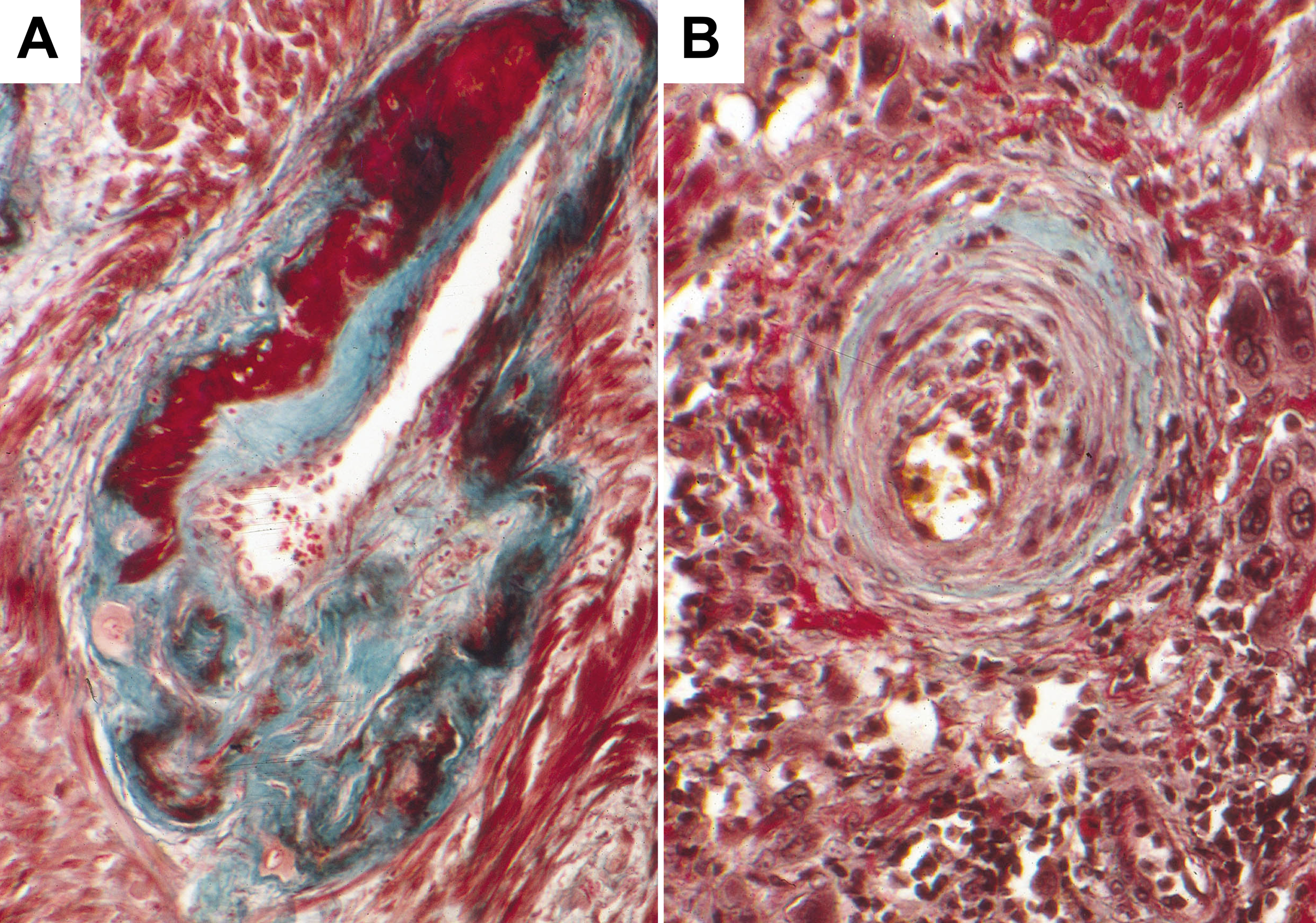
Masson’s trichrome staining of junctional zone spiral arteries in pregnancy. A, Cross section through a physiologically transformed uteroplacental artery in the inner myometrium during a normotensive pregnancy (original magnification: ×150). B, Acute atherosclerosis of an uteroplacental vessel in a pregnancy complicated with preeclampsia and fetal growth restriction (original magnification: ×180).
Impaired Uterine Decidualization
Decidualization occurs in all mammalian species in which implantation involves breaching of the endometrial luminal epithelium by the embryo and invasion of the underlying stroma. 19 This universal maternal response to an invasive conceptus is defined by the transformation of endometrial stromal cells into epithelioid decidual cells with specialized functions. Decidualizing stromal cells first actively encapsulate the implanting embryo 29,30 and then form a nutritive and immune-privileged matrix that enables coordinated trophoblast invasion. 31 Upon decidualization, differentiating stromal cells become highly resistant to environmental stress signals. 32,33 Several molecular mechanisms underpin this quasi-autonomous, stress-resistant state of decidua cells, including silencing of circadian gene expression, 34 inhibition of stress pathways such as c-Jun N-terminal kinase, 35 attenuated inositol trisphosphate signaling, 36 global cellular hypoSUMOylation, 37,38 downregulation of the metabolic stress enzyme O-linked N-acetylglucosamine (GlcNAc) transferase (OGT), 39 resistance to microRNA-mediated gene silencing through loss of argonaut proteins, 40 and marked upregulation of free radical scavengers. 33 Furthermore, there is evidence that the decidual response is spatially organized, as differentiating cells that surround the terminal spiral arteries produce a distinct cytokine and chemokine profile implicated in homing trophoblast toward maternal vessels. 41 Perivascular stromal cells also harbor many clonogenic mesenchymal stem-like cells (MSCs). 42,43 Although the precise role of these MSCs in pregnancy is not yet known, sufficient progenitor cells are arguably essential to ensure that the endometrium has the adaptive capacity (ie, plasticity) for rapid expansion in pregnancy and to accommodate trophoblast-mediated spiral artery remodeling. 43
In view of the multitude of functions exerted by decidual cells, perturbations in this differentiation process may not only render the fetomaternal interface vulnerable to various stressors but also compromise vascular remodeling in pregnancy. A recent study provided direct evidence of impaired decidualization in PE. Using laser microdissection to isolate the decidua from tissue sections of the fetomaternal interface, Garrido-Gomez et al demonstrated that decidual gene expression is profoundly abnormal in preeclamptic pregnancies. 44 Furthermore, the authors examined the decidualization potential of cultured endometrial cells isolated from biopsies following a normal or preeclamptic pregnancy. Based on the severely blunted secretion of prolactin and insulin-like growth factor binding protein 1 in primary cells differentiated in culture, the authors concluded that decidualization defects in the endometrium may persist for many years after an affected pregnancy. 44
Intrinsic Decidual Resistance
A blunted response of primary endometrial stromal cells to deciduogenic signals is not specific to PE. The same phenomenon, commonly referred to as “progesterone resistance,” has been associated with various reproductive disorders, most prominently endometriosis. 45 It has been argued that “progesterone resistance” is a misnomer as these endometrial stromal cells are also unresponsive to other essential cues for decidualization, including cyclic adenosine monophosphate (cAMP) signaling and human chorionic gonadotropin. 46,47 Further, the term “progesterone resistance” implies that “normal” endometrial stromal cells are intrinsically progesterone responsive but lose this ability under pathological conditions. In fact, the opposite is true; human endometrial cells are not innately responsive to differentiation signals but acquire the ability to decidualize at some point following the menarche. 21,48 The most compelling evidence for intrinsic or ontogenetic “decidual resistance” of human endometrium at birth has come from an autopsy study published by Ober and Bernstein in 1955. 49 Despite exposure to very high concentrations of unbound estrogens and progesterone in utero, Ober and Bernstein found that the endometrium was either inactive or weakly proliferative in 68% of neonates and term fetuses. Evidence of secretory changes in the glandular compartment was observed in 27% of cases, but the incidence of decidual or menstrual changes was only 5%. These findings are corroborated by the observation that overt neonatal uterine bleeding affects approximately 4% to 5% of female babies during the first week of life. 50 Thus, the human endometrium can already be responsive to deciduogenic signals at birth, but in the vast majority of newborn girls, it is not.
Uterine Maturation and Spontaneous Decidualization
During childhood, the uterus remains an immature organ, both physically and in terms of hormone responsiveness, as outlined previously. 21 Maturation commences some years before the menarche with marked uterine growth in response to rising estradiol levels. The onset of regular ovulatory menstrual cycles sometime after the menarche could be considered as evidence of uterine maturity. The term “perimenarche” has been coined to describe this lag period between the menarche and the onset of regular ovulatory menstrual cycles. 51 The perimenarcheal stage varies tremendously; it may be as short as a few months or as long as 5 years or more. 21 This variability is explained by the fact that regular cycles depend on convergence of 2 processes: (1) establishing robust feedback loops that control the hypothalamic–pituitary–ovarian (HPO) axis and (2) acquisition of endometrial responsiveness to progesterone signaling and other deciduogenic cues. Socioeconomic factors and metabolic variables, such as nutritional status and body mass index (BMI), exert a strong influence on the maturation of the HPO axis. 52 This raises the possibility that metabolic disorders, especially child obesity, cause asynchrony between the maturation processes in the uterus and HPO axis, thus increasing the likelihood of a pregnancy occurring in an as yet immature uterus. 21
Under a progesterone-dominant environment, endometrial cellular “stress” has emerged as an evolutionary conserved, obligatory trigger for decidualization. 53 For example, scratching the endometrium in progesterone-primed mice, or exposure of the uterine lumen to an oil drop, is sufficient to trigger a massive decidual response. 54,55 Furthermore, neonatal uterine bleeding is more prevalent following preeclamptic or postterm pregnancies, 56,57 indicating that in utero stress also sensitizes the fetal endometrium to decidualization. A recent study highlighted the importance of rapid estradiol-mediated growth and proliferation stress prior to ovulation on the sequence of events after ovulation that renders the endometrium receptive to embryo implantation during the midluteal phase of the cycle. 58 Following menstruation, rapid proliferation not only increases the endometrial thickness multifold over in approximately 10 days but also imparts replication stress on some but not all stromal cells. After the ovulatory rise in circulating progesterone levels, increasing intracellular cAMP levels in endometrial stromal cells impose a cell cycle block at G0/G1. Cell cycle exit is a prerequisite for differentiation. However, prestressed stromal cells do not differentiate into specialized decidual cells but instead undergo acute cellular senescence (Figure 3). Unlike chronic senescence associated with aging, acute senescence is a tightly orchestrated biological process implicated in wound healing, tissue repair, and development. 59 Typically, acute senescent cells secrete tissue-specific inflammatory mediators with defined paracrine functions and self-organize their elimination by various immune cells. This is also the case in the human uterus; acutely senescent endometrial cells during the midluteal phase mount a transient inflammatory response that renders the human endometrium receptive for implantation. 60 As the cycle unfolds, interleukin 15-activated uterine natural killer cells then target and selectively clear these senescent cells through granule exocytosis, de facto rejuvenating the endometrium at the time of embryo implantation. 58
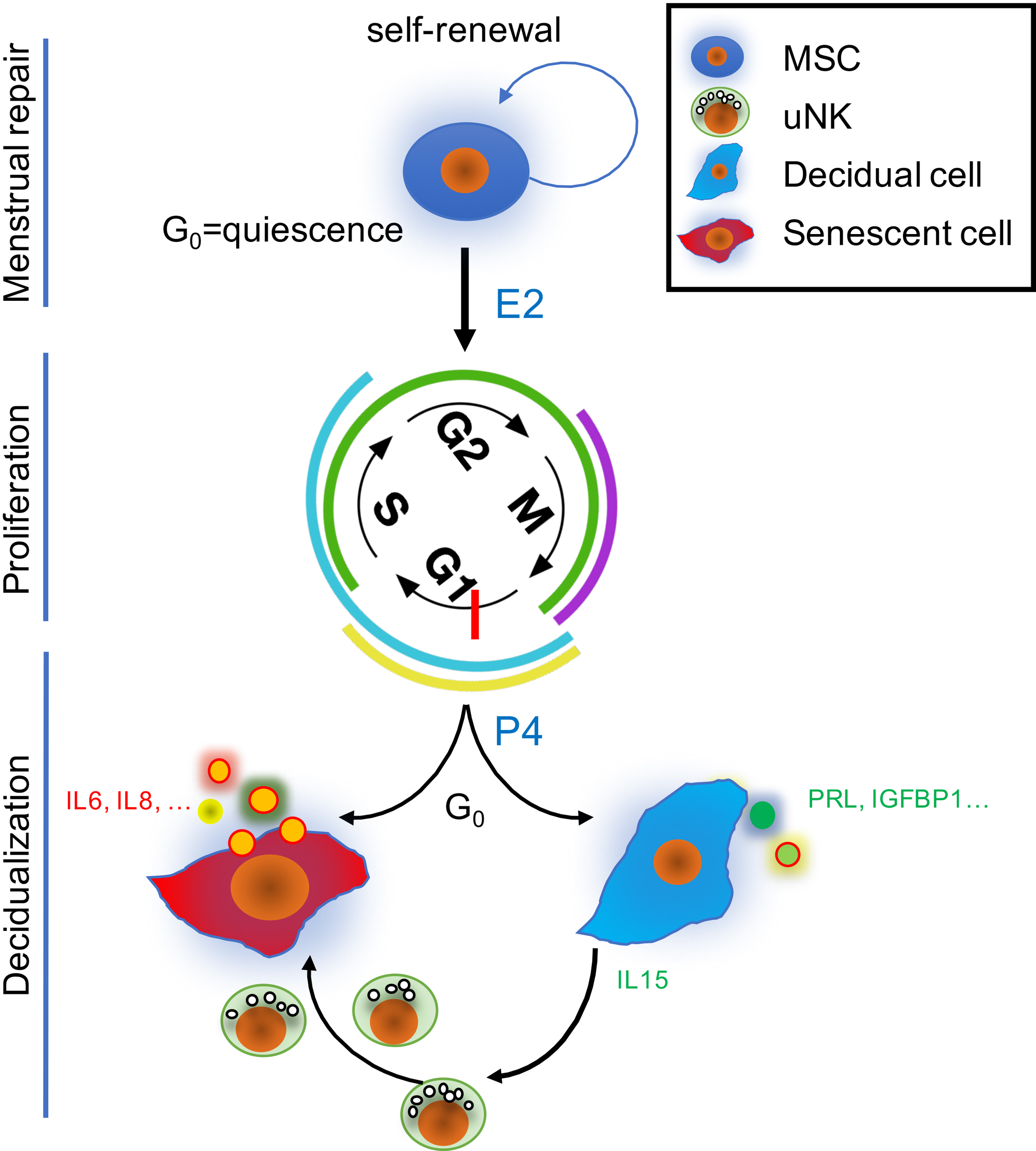
Acute cellular senescence upon decidualization generates an endogenous stress signal in cycling endometrium. Menstruation activates endometrial mesenchymal stem/progenitor cells (MSCs), leading to tissue repair. This is followed by rapid estradiol (E2)-mediated tissue proliferation, imposing variable degrees of replication stress on stromal cells. After ovulation, rising progesterone levels (P4) trigger cell cycle exit at G0/G1. Consequently, some cells differentiate into specialized decidual cells, whereas others become acutely senescent and secrete a host of inflammatory mediators that kick-start endometrial remodeling for implantation. Activated uterine natural killer (uNK) cells then target and clear senescent decidual cells through granule exocytosis. IGFBP1 indicates insulin-like growth factor binding protein-1; IL, interleukin; PRL, prolactin.
In light of these novel findings, it seems likely that the rising estradiol levels and prolonged endometrial growth prior to menarche play a critical role in transforming the endometrium into a progesterone-responsive tissue capable of mounting a spontaneous decidual response during the midluteal phase of the cycle. 21 However, while the onset of regular cycles after the end of the perimenarche signals that the uterus is capable of generating a robust endogenous stress response essential for decidualization and embryo implantation, this does not necessarily mean that it is already equipped to cope with the massive stress imposed by deep placentation.
Extrinsic Factors in Adolescent PE
Based on the emerging understanding of the mechanisms that underpin uterine maturation during the perimenarche, it has become clear that adolescence is a precarious period for pregnancy. Uterine vulnerability may be further compounded by extrinsic factors, such as obesity and other risk factors associated with cardiovascular disease (CVD). Put differently, comorbidities that increase the risk of PE in adults may have a disproportional impact on pregnancy outcome in young adolescents.
Obesity and Excessive Gestational Weight Gain
The prevalence of obesity continues to increase in children and adolescents. In national surveys from the 1960s to the 1990s, the prevalence of overweight children grew from 5% to 11%. Childhood obesity increases the risk of hypertension, type 2 diabetes mellitus, dyslipidemia, left ventricular hypertrophy, nonalcoholic steatohepatitis, obstructive sleep apnea, orthopedic problems, and psychosocial problems. 61 Once considered rare, primary hypertension in children has become increasingly common. Obese children are approximately 3 times more likely to develop hypertension than nonobese children. In addition, the risk of hypertension in children increases across the entire range of BMI values and is not defined by a simple threshold effect. 62,63 Like in adults, a combination of factors, including overactivity of the sympathetic nervous system, insulin resistance, and endothelial cell dysfunction, may contribute to obesity-related hypertension in children. 64
Several studies highlighted the impact of BMI on the risk of PE in teenage pregnancies. For example, a retrospective cohort analysis of 730 teenage deliveries (≤18 years old) identified prepregnancy maternal obesity (BMI ≥ 30) and excessive gestational weight gain (GWG) as major risk factors for the development of PE. 65 A recent meta-analysis strongly reinforced the notion that BMI should be considered a predictor of PE. In this analysis, which included 23 studies with almost 1.4 million participants, PE was associated with overweight (odds ratio [OR] = 1.73; 95% confidence interval [CI], 1.59-1.87) and obesity (OR = 3.15; 95% CI, 2.96-3.35). 66
Considerable progress is being made in parsing the mechanisms that link obesity to abnormal responses in the endometrium. Antoniotti et al studied the impact of advanced glycation end products (AGEs), that is, proteins or lipids that become glycated as a result of exposure to sugars, on endometrial cell function. 67 Advanced glycation end products are elevated systemically in obesity and are derivatives of fat- and sugar-related molecules. In a series of experiments, the authors demonstrated that elevated levels of AGEs activate inflammatory pathways in endometrial epithelial cells, cause endoplasmic reticulum stress in endometrial stromal cells, impair decidualization, and inhibit trophoblast invasion. 67 Further, EOGT (EGF domain-specific O-linked GlcNAc transferase) was recently identified as a nutrient-sensing enzyme that is selectively expressed in the endometrium during the window of implantation. 39 Like its canonical counterpart OGT, EOGT acts downstream of hexosamine biosynthetic pathway. This metabolic pathway produces uridine diphosphate-N-acetylglucosamine (UDP-GlcNAc) from the conjugation of glucose with amino acid-derived amine, lipid-derived acetyl, and the nucleotide uridine, thus sampling all core cellular metabolism in the process (Figure 4). The EOGT uses UDP-GlcNAc to modify specific cell surface and proteins earmarked for secretion. Strikingly, knockdown of EOGT in decidualizing endometrial stromal cells abolishes the expression of adropin, 39 a recently discovered peptide hormone that promotes various indices of vascular health, including endothelial cell proliferation, migration, and angiogenesis. 68 By suppressing monocyte–endothelial cell adhesion, adropin also exerts important antiatherosclerosis actions. 69 Expression of EOGT and adropin in midluteal endometrial biopsies correlates inversely with BMI, suggesting a direct pathway that links obesity to uteroplacental disease in pregnancy. 39 Moreover, low circulating adropin levels have been associated not only with high BMI, insulin resistance, endothelial dysfunction, and coronary atherosclerosis but also with severe PE. 70,71
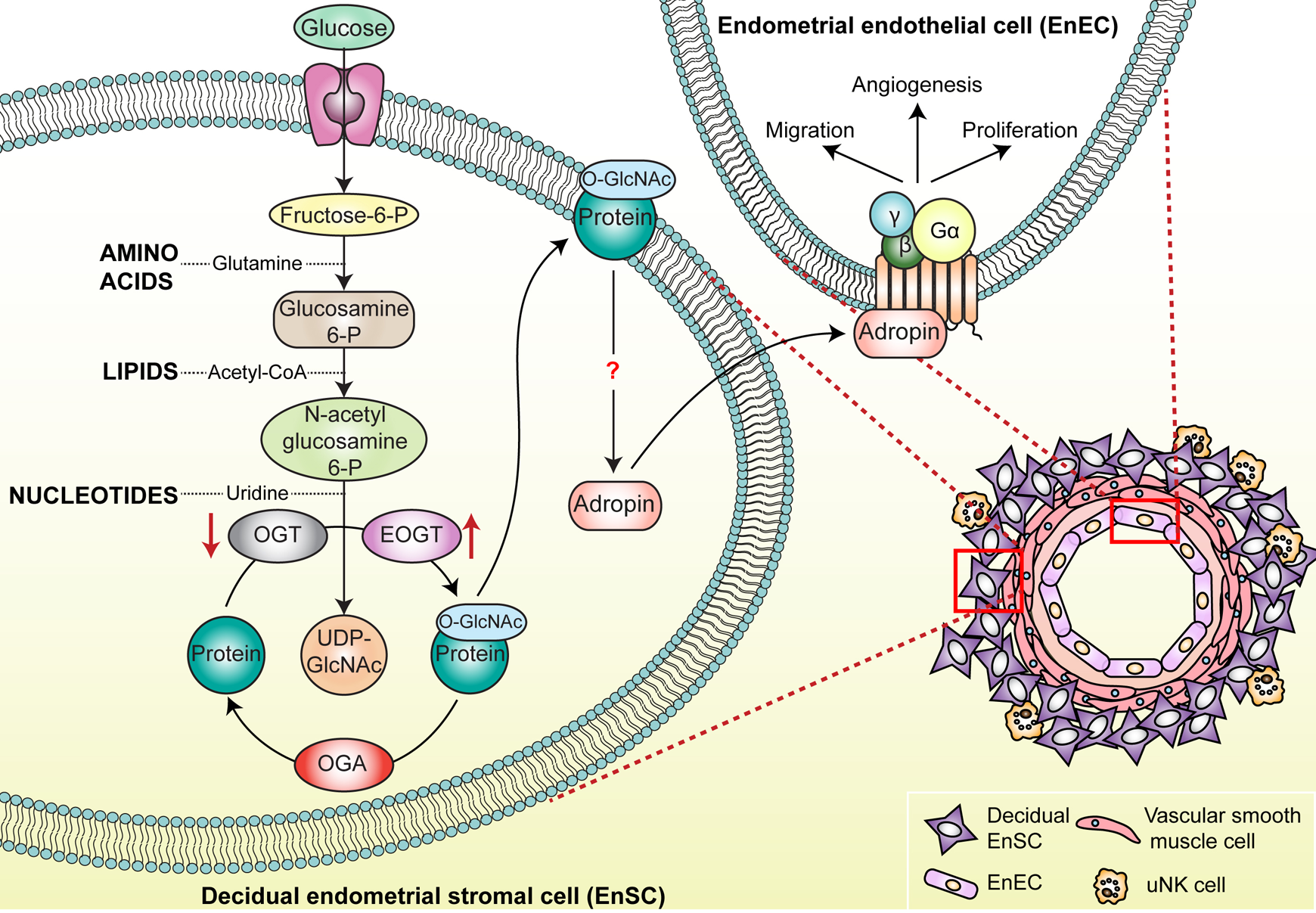
Schematic illustrating the production of uridine diphosphate N-acetylglucosamine (UDP-GlcNAc) via the nutrient-sensing hexosamine biosynthetic pathway (HBP) in decidualizing endometrial stromal cells and subsequent protein O-GlcNAcylation by EOGT (EGF domain-specific O-linked GlcNAc transferase; left). The EOGT controls the expression of the peptide hormone adropin, which promotes indices of vascular health including migration, angiogenesis, and proliferation in endometrial endothelial cells (top right) of the emerging spiral arteries (bottom right). Fructose-6-P indicates fructose 6-phosphate; glucosamine-6-P, glucosamine 6-phosphate; N-acetylglucosamine-6-P, N-acetyl-
Thus, the incontrovertible link between obesity and PE should provide additional impetus to implement public health measures and educational programs to tackle the current epidemic. In pregnancy, the focus should be on strict prevention of excessive GWG—as advocated by Hamlin in 1952. 2 More than 60 years later, a Cochrane review of 49 randomized controlled trials involving 11 444 women yielded high-quality evidence, confirming that diet, exercise, or both during pregnancy are effective in lowering the risk of excessive GWG, in reducing the incidence maternal hypertension, and in improving pregnancy outcome, particularly in high-risk women. 72
Transgenerational Hypertension and Early-Onset CVD
In the absence of physiological spiral artery remodeling, the JZ uterine vessels are prone to developing acute atherosis, characterized by changes in lipid metabolism, intravascular inflammation, macrophage infiltration, and endothelial cell dysfunction. 73 The term “atherosis” refers to vascular disease at the fetomaternal interface in PE. When affecting the JZ arteries, these lesions are indistinguishable of atherosclerosis, the primary driver of CVD. Autopsy studies on young people who died of accidental causes established that atherosclerosis begins as early as 10 years of age. 74 By the age of 15, a majority of adolescents have evidence of early atherosclerotic lesions and subsequent progression is determined by the conspicuous determinants of cardiovascular health: BMI, non–high-density lipoprotein cholesterol, blood pressure, blood glucose, and smoking status. 75 As the number of cardiovascular risk factors increases, so does the pathological evidence for atherosclerosis in the aorta and coronary arteries. 76 Importantly, atherosclerosis occurs to a greater extent and at a lower level of hypertension in the placental bed than would be expected in other organs, 25 an observation that may be particularly pertinent for the “unconditioned” spiral arteries in the adolescent uterus.
The consequences of PE in adolescent mothers are far-reaching, both for the mother and her offspring. In 1986, Sibai et al reported that, compared to an age-matched, normotensive control group, young women who developed severe PE in their first pregnancies not only had a higher incidence of PE in their second (46.8% vs 7.6%, P < .0001) and subsequent pregnancies (20.7% vs 7.7%, P < .001) but were also much more likely to develop chronic hypertension (14.8% vs 5.6%, P < .001). 77 A prospective follow-up study over 2 decades of 2868 children born to 2804 mothers found that 30% of 20-year-olds with hypertensive blood pressures were born following a hypertensive pregnancy. 78 Preeclampsia was associated with a 3-fold increased risk of being hypertensive by age 20. Young adults born following hypertensive pregnancies were also more than twice as likely to have a global lifetime risk score of developing CVD of ≥40%. 78 Another large cohort study of maternal–offspring pairs (n = 6619) reported that children born after a hypertensive pregnancy have consistently higher blood pressure across childhood and into early adulthood. 79 Notably, maternal blood pressure at 8 weeks’ gestation, but not the subsequent rise in blood pressure during pregnancy, was positively associated with the blood pressure in the offspring during childhood. The authors posited that this observation is evidence of shared genetic or environmental factors between the mother and child. 79 Nevertheless, a systematic review and meta-analysis of 18 studies, providing cumulative data on 45 249 individuals, demonstrated that in utero exposure to PE is associated with higher systolic (2.39 mm Hg, 95% CI, 1.74-3.05; P < .0001) and diastolic (1.35 mm Hg, 95% CI, 0.90-1.80; P < .00001) blood pressure and increased BMI during childhood and young adulthood. 80
Because the pathological basis of CVD starts in childhood, Goodling and Johnson 81 highlighted recently the importance of primordial prevention of cardiovascular risk factors (ie, before they even occur) during childhood and assessment and primary prevention of CVD during adolescence and early adulthood. By their own admission, identifying, implementing, and disseminating effective interventions in these age groups is challenging. Arguably, pregnancy represents the best opportunity to assess cardiovascular risk factors, address health behavior, and implement dietary and lifestyle measures that improve the health outcome for the mother and her offspring. In case of PE, preventative measures should be reinforced throughout childhood of the offspring and into adulthood to break the cycle of intergenerational hypertension and poor cardiovascular health (Figure 5).
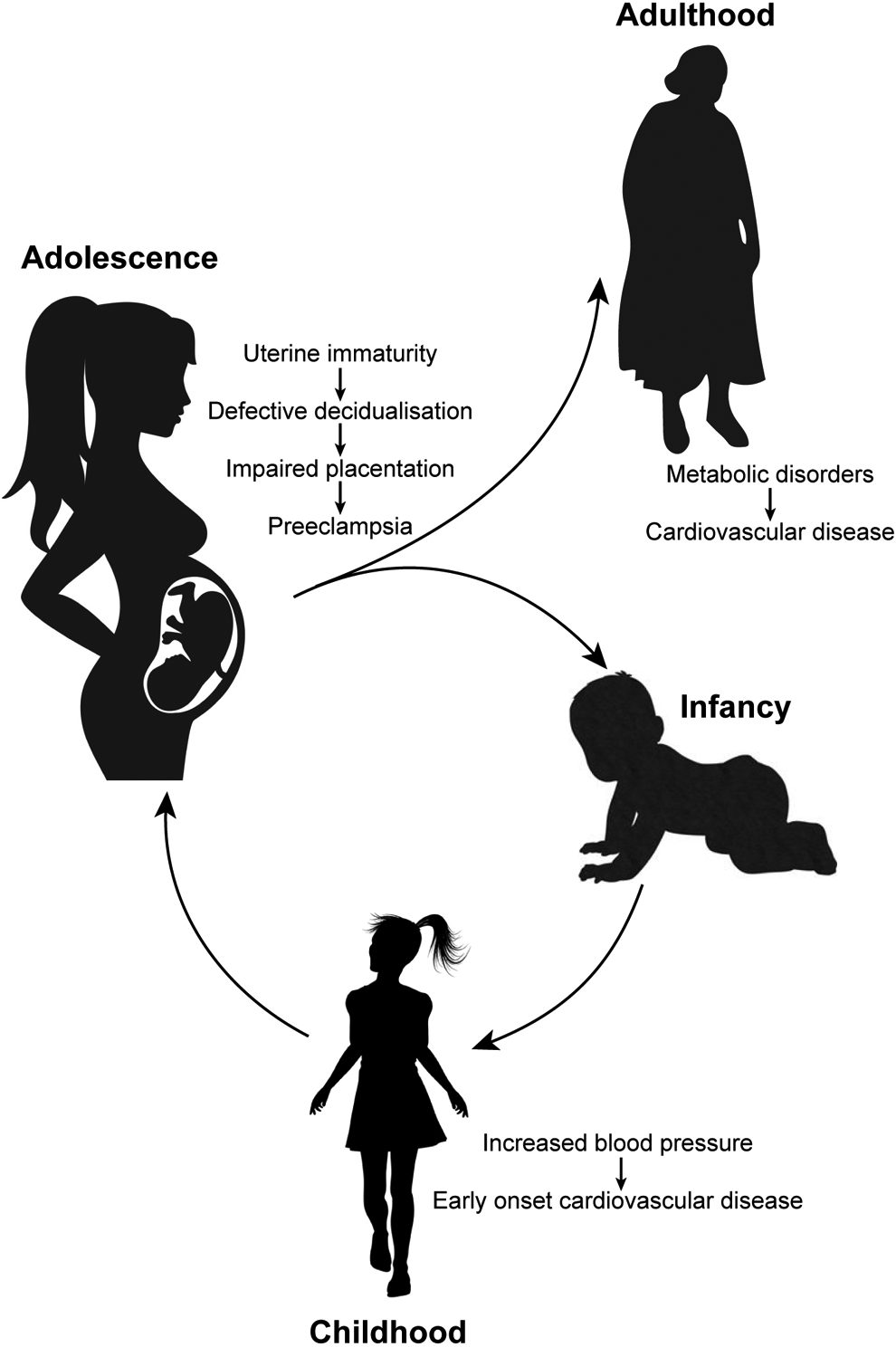
Schematic depiction of the impact of adolescent PE on the long-term health of the mother and her offspring. PE indicates preeclampsia.
Prevention of Adolescent PE
The most glaring and effective way of reducing the burden of obstetrical disorders during adolescence is to reduce teen pregnancy rates. Spurred on by recent trends, the US Centers for Disease Control and Prevention now consider teen pregnancy prevention both a top priority and a “winnable battle” in public health. 82 Despite this optimism, the challenge across the world remains formidable. In 2011, the World Health Organization and the UN Population Fund published joint guidelines on how countries can prevent adolescent pregnancies and reduce poor reproductive outcomes. 83 The most salient recommendations include reducing marriage before the age of 18 and increasing the use of contraception by adolescents at risk of unintended pregnancy. Nevertheless, about 15 million girls are married each year before the age of 18 years, and UNESCO estimated that 90% of births to girls aged 15 to 19 years occur within marriage. In view of these disturbing statistics, it is clear that public health measures to reduce teen pregnancy rates need to be complemented by targeted lifestyle and medical interventions that mitigate the risk of PE and other obstetrical disorders in young mothers, whether or not the pregnancy was planned. In addition to tackling comorbidities (obesity and other cardiovascular risk factors) as already outlined, there is a need to reflect on the role of drug interventions, either prior to pregnancy to accelerate uterine maturation or in pregnancy to reduce the risk of adolescent PE.
Pharmacological Preconditioning
Compared to other organs, the adult uterus is unique in many aspects: It is imbued with seemingly unlimited capacity to regenerate and repair, it is capable of accommodating a semiallogenic conceptus without triggering immune rejection, and it can form, repeatedly, an uteroplacental vascular tree that accommodates ∼20% of cardiac output by late pregnancy. As outlined before, none of these critical uterine functions are programmed at birth but acquired gradually after the onset of cyclic menstruations through a process coined “menstrual preconditioning.” 20 The term “preconditioning” refers to the paradoxical but ubiquitous biological phenomenon that a brief exposure to a harmful stimulus at a dose below the threshold for tissue injury provides robust protection against, or tolerance to, the injurious effects of a subsequent more severe insult. In recent years, different preconditioning strategies (ie, ischemic, pharmacological, remote, and local) have been studied intensively because of their promise in preventing ischemia–reperfusion injury in a variety of organs, including the brain, heart, kidney, and lung. 84,85 At a cellular level, inflammation has been shown to trigger epigenetic memory of injury by maintaining chromosomal accessibility to key stress response genes, enabling a more rapid and heightened response to subsequent challenges. 86 There is ample clinical evidence of endogenous uterine preconditioning after the menarche. As aforementioned, gynecological age is a better predictor of adverse pregnancy outcome in adolescent mothers than chronological age. 21 A prior birth confers a strong protective effect against PE, whereas a prior induced abortion confers a weaker protective effect. 87,88 However, analysis of 20 846 primiparous women participating in the Norwegian Mother and Child Cohort Study demonstrated that the protective effect of 2 prior induced abortions is similar to that of one birth. 89 The latter observation is important as it demonstrates the cumulative effect of injury on uterine memory and subsequent ability to cope with hyperinflammation imposed by deep trophoblast invasion in pregnancy.
Recently, we expressed the opinion that young adolescent women and patients with polycystic ovary syndrome (PCOS) share a number of reproductive features, including frequent anovulation, infrequent menstrual shedding and repair, persistent decidual resistance, and increased risk of defective deep placentation as manifested by the higher incidence of major obstetric syndromes. 90 We also argued that there is a role for pharmacological preconditioning of the uterus in these women, either by inducing ovulation (eg, with clomiphene citrate) or cyclic withdrawal bleeds (eg, with medroxyprogesterone acetate or norethisterone) for a period of time prior to conception, to mitigate the risk of placental disorders in pregnancy and improve long-term health outcomes for both the mother and her baby.
Drug Prevention in Pregnancy
Since the publication of the first clinical trial in 1985, 4 aspirin has become the drug of choice for the medical prevention of PE. However, its efficacy has been debated ever since. More than a decade after the initial successful trials, Sibai pointed out that while early single-center trials demonstrated an average reduction of PE of 70% with low-dose aspirin, 7 large multicenter trials (>27,000 women) showed minimal benefit. 91 A systematic review and meta-analysis published in 2010 seemed to settle the debate. 92 Based on analysis of 34 randomized controlled trials, the study concluded that low-dose aspirin started at 16 weeks or earlier significantly reduces the risks of PE (relative risk [RR] 0.47, 95% CI, 0.34-0.65), FGR (RR 0.44, 95% CI, 0.30-0.65), PIH (RR 0.62, 95% CI, 0.45-0.84), and PTB (RR 0.22, 95% CI, 0.10-0.49). However, low-dose aspirin was ineffective in preventing either PE or FGR when initiated after 16 weeks. 92 A subsequent study by the same team showed that the protective effect of low-dose aspirin is dose responsive. Meta-analysis of 45 randomized controlled trials with a total of 20 909 pregnant women randomized to between 50 and 150 mg of aspirin daily showed that the higher dosages of aspirin are associated with greater reduction of both PE and FGR, but only when initiated ≤16 weeks. 93 Another report using individual participant data meta-analysis on a larger sample size (32 217 women and 32 819 babies) promptly challenged the assertion that treatment needs to be initiated early in pregnancy and concluded that low-dose aspirin and other antiplatelet agents consistently lower the incidence of PE and its complications, regardless of whether treatment is started before or after 16 weeks’ gestation. 94 A recent trial highlighted the effectiveness of aspirin (150 mg daily) in preventing preterm PE (ie, before 37 weeks of gestation) in women deemed at high risk (based algorithm that combines maternal factors, mean arterial pressure, uterine artery pulsatility index, and maternal serum pregnancy-associated plasma protein A and placental growth factor), 95 although there is also evidence that aspirin may be less effective in women with chronic hypertension. 96
Over the past 3 decades, tens of thousands women have been randomized in various clinical trials, making aspirin one of the most intensively studied drug in obstetrics. 6 And yet we were unable to identify a single study evaluating the efficacy of low-dose aspirin in preventing adolescent PE and other obstetrical disorders. While clinical studies may or may not be forthcoming, there are no obvious reasons to assume that vascular adaptation in pregnancy differs substantially between adults and teenagers. In order words, serious consideration should be given to the routine use of low-dose aspirin prophylaxis in first-time pregnant adolescents, especially before the age of 16 when the risk of PE and PTB is highest.
It is important to emphasize that that the overall reduction of PE with low-dose aspirin is estimated to be 10%, 6 rendering it imperative that other preventative strategies are developed. Several drugs are currently under evaluation, including metformin, 97 pravastatin, 98 esomeprazole, 99 and sildenafil. 100 Needless to state that there is insufficient evidence of safety or efficacy to recommend usage of these drugs in adolescent pregnancies. One exception is metformin, which is increasingly used for weight management in children and adolescents. A recent systematic evidence review of the US Preventive Services Task Force concluded that the use of metformin in children and adolescents results only in very modest reductions in BMI (8 trials; n = 616; 95% CI, −1.44 to −0.29), which represents approximately 2% reduction from baseline BMI. Furthermore, pharmacotherapy with metformin in this age-group (6-19 years) was shown to confer little or no benefit on cardiometabolic parameters, including fasting glucose level. 101 Nevertheless, there is evidence that metformin may be effective in optimizing the peri-implantation endometrial environment. For example, 3-D power Doppler ultrasonography has shown that metformin treatment for 6 months significantly increases endometrial thickness, endometrial volume, and endometrial and subendometrial vascularity indices (vascularization index, flow index, vascularization flow index) in women with PCOS. 102 Another study reported that metformin reduces soluble fms-like tyrosine kinase 1 and soluble endoglin secretion from primary endothelial cells, villous cytotrophoblast cells, and preterm preeclamptic placental villous explants, suggesting a role for this multifaceted drug in the prevention or treatment of PE. 103 Clinically, the efficacy of metformin in PE prevention remains unclear. Although a recent systematic review and meta-analysis reported that metformin use in pregnancy is associated with a nonsignificant reduction of PE (RR: 0.74, 95% CI, 0.09-6.28), the authors concluded that further trials are warranted given the low quality of evidence and the clinical heterogeneity of current data. 97
Perspective
Globally, teenage pregnancies are more likely to occur in marginalized communities, often driven by poverty, poor educational attainment, and lack of employment opportunities. In pregnancy, adolescents have less access to antenatal care than older women. When combined with a sharp decline in ideal BMI and blood pressure among adolescents and young adults over the past decade, 104 the incidence of PE and other obstetrical disorders in this vulnerable age group is set to rise with lifelong consequences for the health of both the mother and child. It is evident that a series of joint-up interventions are needed to break this cycle of intergenerational ill health, starting with educational and public health initiatives to reduce the incidence of teen pregnancies and buttressed by enhanced antenatal care for young pregnant women (assessment of cardiovascular risk factors, diet and exercise programs, and low-dose aspirin prevention). In case of adolescent PE, both the mother and child may benefit from long-term, cardiovascular risk reduction interventions, although such sustained programs are often considered beyond the scope, as well as financial means, of many health-care systems. 81
From a biological perspective, the increased incidence of placental disorders in adolescence, especially very young women, lays bare several aspects of uterine physiology that are virtually unexplored. Concepts such as “uterine immaturity,” “decidual resistance,” “menstrual preconditioning,” and “acute endometrial senescence” are likely also relevant to the pathogenesis of other intransigent reproductive disorders, including endometriosis. 48 A number of common themes underlie that these emerging physiological concepts, including that endometrial responses to steroid hormones, are determined by the cumulative impact of repeated tissue “injury” associated with menstruation, miscarriage, and parturition. Another emergent theme centers on prepregnancy origins of obstetrical disorders, as illustrated elegantly by recent studies. 43,44 Defining the molecular, epigenetic, and cellular mechanisms underpinning uterine maturation and tissue plasticity is a prerequisite for effective preconception interventions that mitigate the risk of placental disorders in pregnancy. Finally, it is increasingly apparent that the developmental origins of health and disease hypothesis, based on the influential epidemiological studies of Baker and Osmond, 105 also apply to the uterus. In this respect, evaluation of neonatal uterine bleeding, which likely reflects a prior fetal uterine stress response, as a putative biomarker of poor reproductive outcome later in life, is warranted. 7,50
Footnotes
Authors’ Note
All authors significantly contributed to the preparation and write-up of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.M. and J.J.B are funded by Tommy’s National Miscarriage Research Centre.