
Abstract
Objective:
This study determined whether a private room or open ward design better met optimal environmental conditions for a neonatal intensive care unit with regard to sound level, light level, temperature and humidity.
Background:
Multiple-bed designs for hospital neonatal intensive care units were the standard until recently. Now, private room designs promise to provide better conditions for neonate development and patient care quality.
Methods:
The study compared an eight-bed open ward design with a private room design of a 45-bed neonatal intensive care unit, measuring the environmental parameters of sound, light, temperature, and humidity before and after the construction and occupation of a new private room unit.
Results:
Average light levels were higher in the private room design because of the increased number of windows, but both designs were within the recommended levels. Mean temperature readings were two degrees cooler in the private room environment, and readings were more stable. Mean humidity readings in the two environments were the same, but humidity levels in the private room design were more stable. Median sound level in the private room design was lower than the open ward design, but the range was similar.
Conclusion:
The private room design allows for a more controlled patient care environment that can be maintained within a smaller range of variation nearer optimal environmental conditions.
Although there have long been standards for general hospital design, the neonatal intensive care unit (NICU) is a highly specialized patient care environment that lacked specific design standards until they were proposed by the Committee to Establish Recommended Standards for Newborn ICU Design (2007) and published in the Journal of Perinatology by the current committee chairman, Robert White (2007). Neonates can sense their environment and respond to it, but they are unable to protect themselves against environmental extremes because of immature homeostatic systems. The NICU must be designed to optimize the environmental conditions that neonates need. Research has established optimal conditions and recommended ranges for neonatal development with regard to light, sound, temperature, and humidity, and the current standards include specifications for these factors.
Most early NICUs used a multibed ward design. One common format has multiple patients in incubators or bassinets in one room with a team of nurses providing care for all the infants. Newer designs for adult and pediatric hospital units use a private room concept, which increases privacy, reduces noise, and lessens the risk of infection. A trend toward single-patient room neonatal intensive care nurseries has emerged to provide appropriate environmental stimuli for each child while also increasing privacy for families. Although the private room concept has been used for adult and pediatric units for several years, it is unclear whether a private room design facilitates optimal environmental conditions for neonates better than a multibed room design.
The study hospital is a 390-bed community teaching hospital that includes a 45-bed level-IIIB NICU. In 2007, the hospital built a new NICU and changed its design from eight-patient open-ward pods to a new space with all private rooms. The environmental factors of sound, light, temperature, and humidity were measured in both spaces to determine whether the private room design optimized the environmental conditions for neonatal growth and development. Each aspect of the NICU environment was measured in three ways: how closely the average readings in each environment matched optimal conditions; how often each environment had readings outside the recommended range; and how stable the environment was, as measured by analysis of variance of the parameters.
Methods
General Information
Neonates were kept in incubators (Hill-Rom Air-Shield model C2000 Infant Incubator or Giraffe® Omnibed, GE Healthcare), cribs (HARD Manufacturing Co., Inc.), or open bassinets.
Multibed Ward Design
Both the multibed and private room designs consisted of 45 beds, with 32 beds designated as critical care and 13 as a step-down level for patients whose condition did not require intensive nursing care. The multibed design consisted of eight-bed wards with patients separated by partial walls or privacy curtains for visual but not sound separation. Floors were carpeted and ceilings used acoustical panels to reduce sound. Background lighting was indirect, with one individually controlled direct task light per cubicle.
Each cubicle had individual light control but was open to ambient light from the end of the room. Each eight-bed ward had one thermostat to control temperature. Humidity was controlled by the building heating, ventilation, and air conditioning (HVAC) system and was not adjustable by room. The unit used an overhead intercom system for communication.
Private Room Design
The private room design was used for 45 rooms. The 32 critical care rooms were on the fourth floor of the building and the 13 intermediate-care or step-down rooms were on the third floor of the same building, beneath the critical care rooms. Most rooms were approximately 11 feet wide by 14 feet deep. The corner rooms were larger because of their irregular shape, and several larger rooms were single but capable of holding two incubators if needed for twins. Most rooms had a six-foot-wide doorway closed by a curtain rather than a rigid door. A few of the smaller rooms had a four-foot opening. All of the rooms on exterior walls had full-width (11 feet by 3.5 feet or 88.5 square feet) windows consisting of high-efficiency tinted glazing, a translucent roll-down blind, and an opaque roll-down shade to control light. The glazed area was five feet above the floor, and the layout of the room places the patient's head toward the window wall. Each room had a hand-washing sink on the right wall and a computer desk on the left wall. Each room had an individual thermostat. The flooring was resilient linoleum, and the ceiling was acoustical tile. Lighting in each room consisted of one small night-light 12 inches above the floor, four dimmable general lighting fixtures centered in the room, and one direct task light directly over the patient. Ambient lighting in the unit was cycled to increase to day level (18–37 foot-candles) at 6:30 a.m. and lower to a night level (less than 4.6 foot-candles) at 7:30 p.m.
Environmental Measurements
Investigators took environmental measurements at the head of the bed in each occupied patient space. Measurements were not taken if the rooms or cubicles were unoccupied by a patient or if the patient was under special precautions. If an environmental measure was unusual, a comment on its cause was noted during data collection. Open ward measurements were taken approximately every other day in February and March of 2007. There were 31 measurement periods, 16 during the day between approximately 10 a.m. and 11 a.m., and 15 during the night, between 11 p.m. and midnight. Measurements were scheduled to avoid bedside rounds to keep from interfering with patient care activities. Private room environment measurements were taken in February and March of 2009. There were 21 private room measurement sessions over 27 days. Fourteen measurements were taken during the day and seven at night.
Sound Measurement
Sound measurements were taken near the patient's head with equipment running. If an alarm or overhead page sounded during a reading, it was included in the sound reading. Readings were taken using a dosimeter (Extech Instruments Digital Sound Meter, model 407736 for manual readings or Noise Pro DXL for continuous readings) set on the “A” range and “S” response settings. Two sound readings of 30 seconds each were taken over a 90-second period; a 30-second reading was followed by a 30-second wait and another 30-second reading. For continuous sound levels, data were expressed as median value using the Mann-Whitney U Test for comparing median levels to compare the data sets and Levene's test for homogeneity of variance to compare the distribution.
Light Measurement
Light was measured using a digital light meter (Extech Instruments Heavy Duty Light Meter, model 407026) with the sensor placed near the patient's head. Lighting and window shades were not changed for the light readings. Readings were collected in foot-candles. Data were expressed as mean value with two-tailed t-test for comparison of the data sets and Levene's test for homogeneity of variance to compare distribution. If lighting conditions were unusual (setting of shades or task lighting), this was noted during data collection.
Temperature and Humidity Measurements
Ambient temperature and humidity readings were taken in each occupied patient space using an electronic thermometer and hygrometer (Extech Instruments Temperature/Humidity Pen, model 70956). The meter was held near the patient's body in each room, and the reading was recorded as soon as the meter stabilized. Data were expressed in degrees Fahrenheit and percentage of relative humidity and compared using mean and standard deviation with two-tailed t-test for comparison of the two data sets and Levene's test for homogeneity of variance to assess the degree of variation.
Results
Sound Measurements
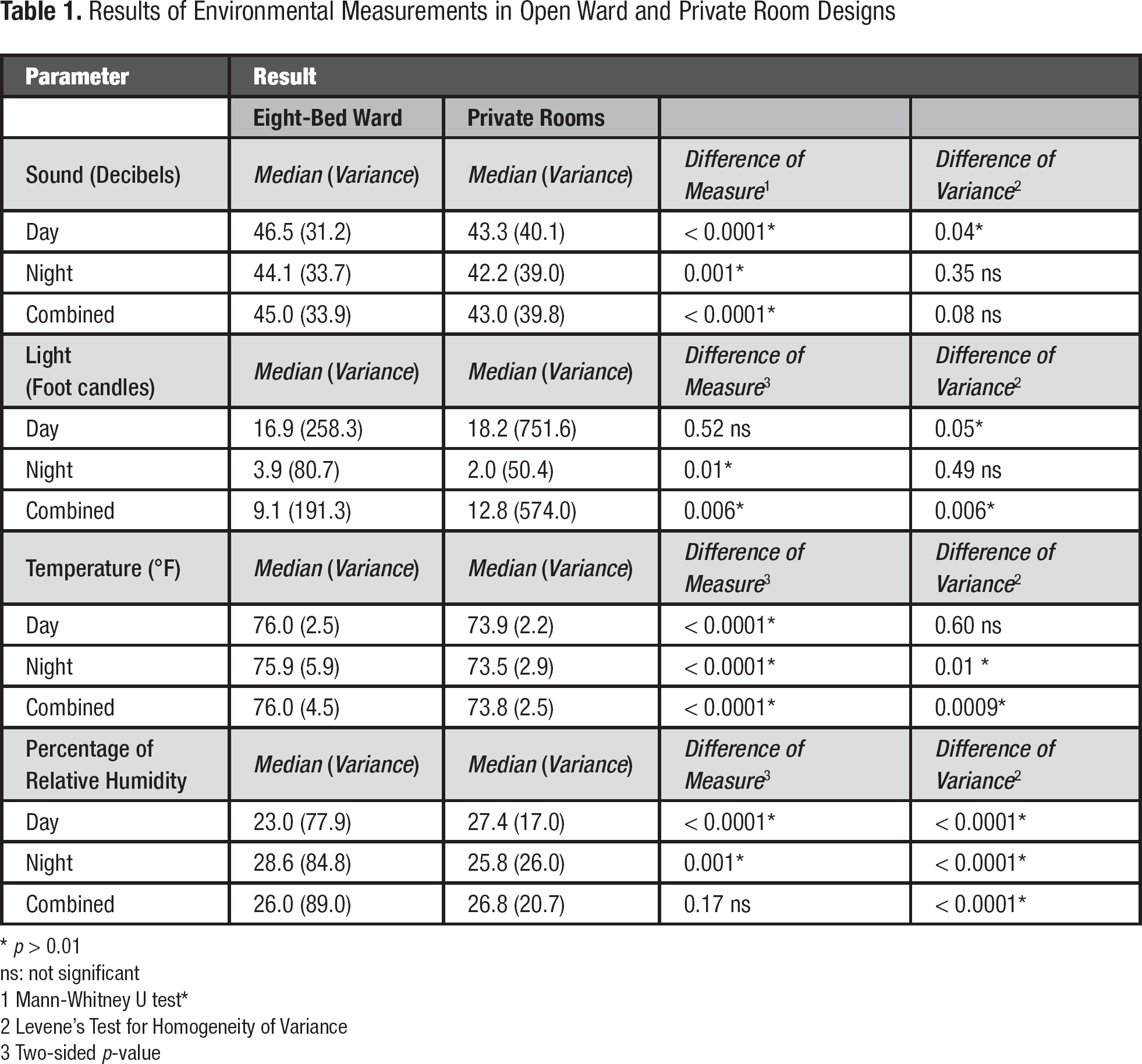
The recommended maximum sound level for the NICU environment is an hourly average of 45 decibels and a single-point maximum of 65 decibels (American Academy of Pediatrics, 1997). Figure 1 and Table 1 show the distribution and statistical analysis of sound values. The median value of sound measurements collected in the open ward NICU was 45.0 with a range of 31.8 to 78.0. The median sound value in the private room NICU was 43.0 with a range of 30.2 to 70.9. The difference between the median sound readings in the two units was statistically significant (p < 0.0001); the private room environment was quieter. The variance of sound readings in the two environments was not significantly different.
Results of Environmental Measurements in Open Ward and Private Room Designs
p > 0.01
ns: not significant
Mann-Whitney U test*
Levene's Test for Homogeneity of Variance
Two-sided p-value
Distribution of sound readings in open ward and private room designs.
Five of 1,024 sound readings taken in the open ward nursery environment were above 65 decibels. Six of 757 sound readings taken in the private room environment were above 65 decibels. Three of the latter were taken while the baby in the room was crying, two while an alarm was sounding, and one while a nurse was talking on the telephone. Other cases in which there was an identifiable source of sound above the background included equipment alarms, water running in a sink, a baby crying, people talking, someone opening a package, and a parent talking on a telephone.
Light Measurement
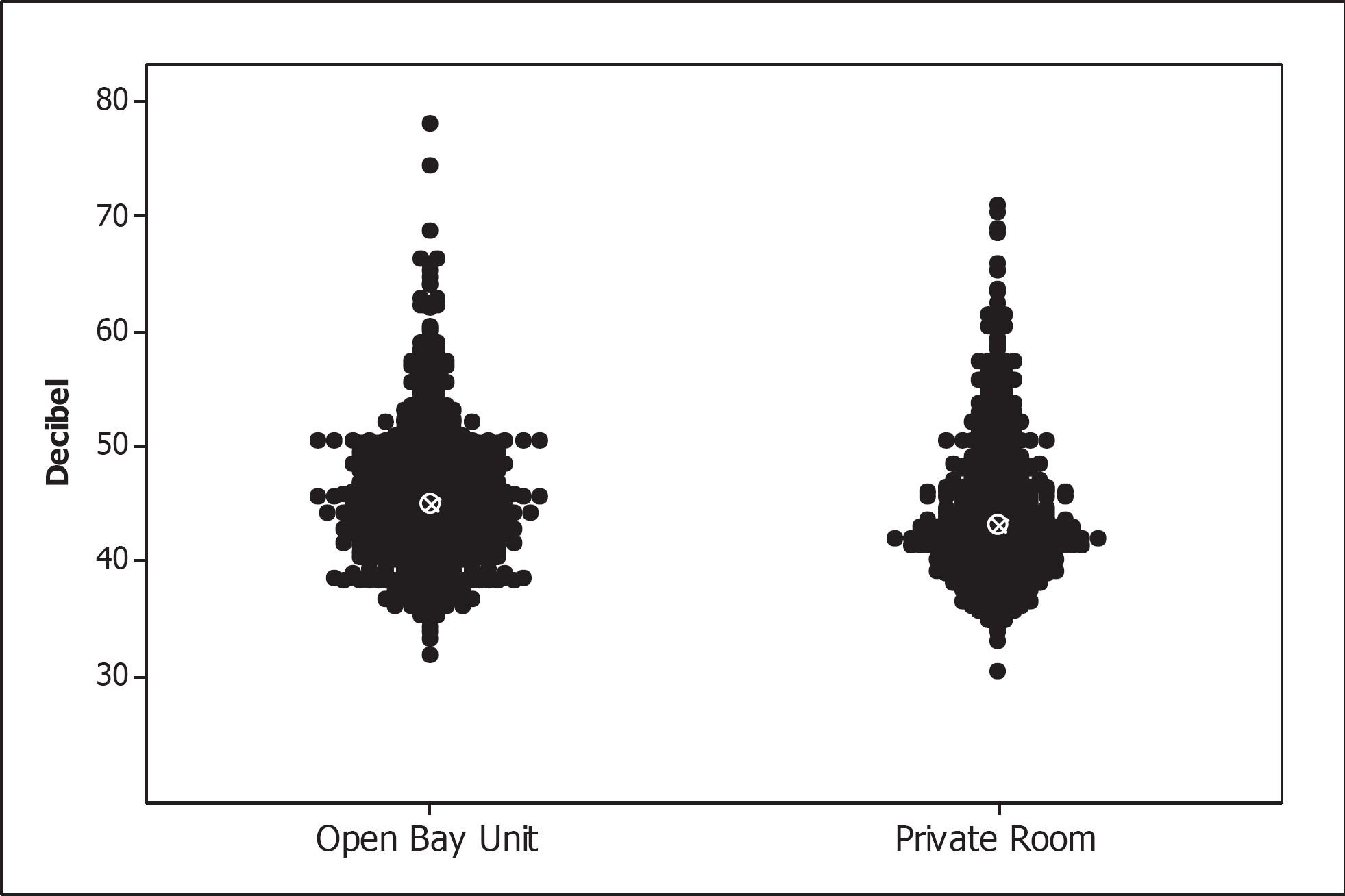
The maximum recommended light level for the NICU is 60 foot-candles. Figure 2 and Table 1 show the distribution and statistical analysis of light readings. The mean reading in the open ward NICU was 9.1 with a range of 0.1–112.6. The mean reading in the private room design was 12.8 with a range of 0.0–249.0. This difference was statistically significant but the mean light levels of both NICUs were well below the recommended maximum light level of 60 foot-candles.
Distribution of light intensity readings in open ward and private room designs.
The homogeneity of variance between the open ward and private room designs was significantly different (p = 0.006), with the private room setting showing more variance of light intensity because of the presence of larger windows in most rooms, resulting in more variation in light levels during the daytime.
Ten of 814 readings (five daytime readings and five nighttime readings) exceeded the 60 foot-candle limit in the open ward setting. These readings were obtained when all the lights were on. There were 14 of 382 readings (13 during the day and one at night) in which the light level in private rooms exceeded 60 foot-candles. Two such readings were caused by the use of the task light; the other 12 high readings were daytime measurements taken in rooms with windows when the blinds were up.
Temperature Measurement
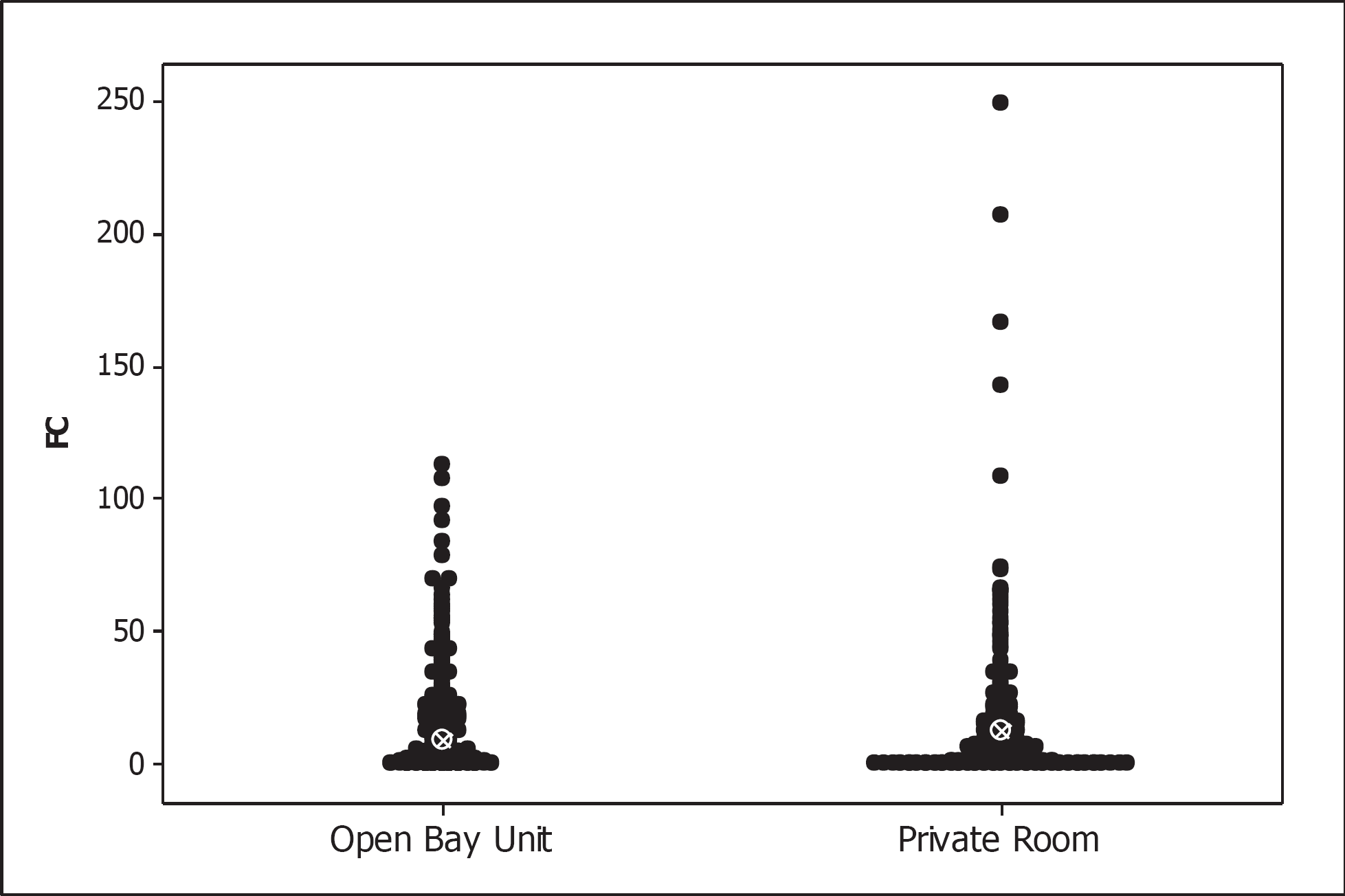
The recommended temperature range for the NICU is 72–78 °F. Figure 3 and Table 1 show the distribution and statistical analysis of temperature values. The mean of all the open ward temperature measurements was 76.0 °F with a range of 71.1–84.5 °F. The mean temperature of all the private room measurements was 73.8 °F with a range of 65.3–77.5 °F. The open ward NICU was significantly warmer than the private room NICU (p < 0.0001), although the mean temperature of both units was within the recommended range.
Distribution of room temperature readings in open ward and private room designs.
The variance of the open ward NICU temperature readings was 4.5. The variance of the private room NICU readings was 2.5, indicating that private rooms showed more temperature stability than the open ward design (p = 0.0009).
Only a few open ward beds had temperature readings below 72 °F, but readings exceeded 78 °F 51 times out of 376 readings (13.6%) in 14 of the 31 measurement periods. Ten of the 14 periods of high temperature samplings were at night, so heat gain from outside conditions or sunlight could not explain the high readings. The open ward design produced warm spots that often exceeded the recommended temperature.
The private room NICU showed temperature readings that were outside the 72–78 °F range 41 times out of 362 readings. All of the readings outside the range were below 72 °F. Ten of the periods were daytime and six were night, indicating that the ventilation system rather than heat gain or loss from the outside was influencing the readings. Although 41 readings were outside the range, most of the readings were between 71 °F and 72 °F, and the most common reading was 71.9 °F—barely below the desirable range. Only six readings were below 70 °F. A total of 32 of the 41 low readings were taken in rooms in the same area, and almost all of those were taken in a row of nine adjacent rooms.
Humidity Measurements
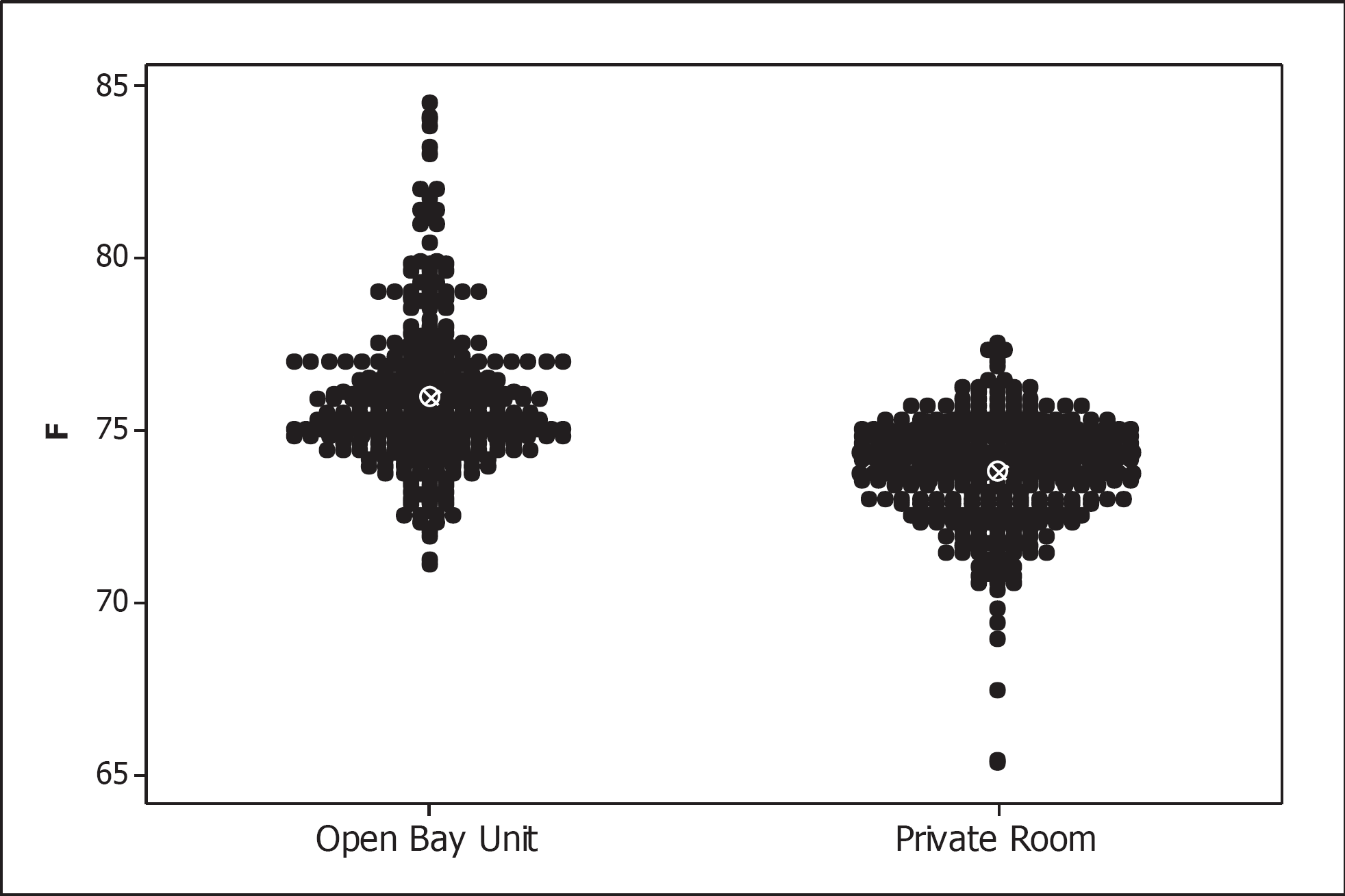
The recommended range for the NICU is 30–60% relative humidity. Figure 4 and Table 1 show the distribution and statistical analysis of humidity values. The mean of all the humidity readings of the open nursery NICU was 26.0% with a range of 10.7–49.0%. The mean of the private room NICU was 26.8% with a range of 16.7–47.4%. The difference between the means was not significant. The mean humidity level of both designs was below the recommended level. No humidity readings in either NICU exceeded 60%. Humidity readings in the open nursery NICU showed a two-peak distribution, with most readings in the 20% range and a cluster of readings in the 40–50% range. All the high readings were taken during two consecutive days, and all the readings on these days were high. There is no documented explanation for these high readings.
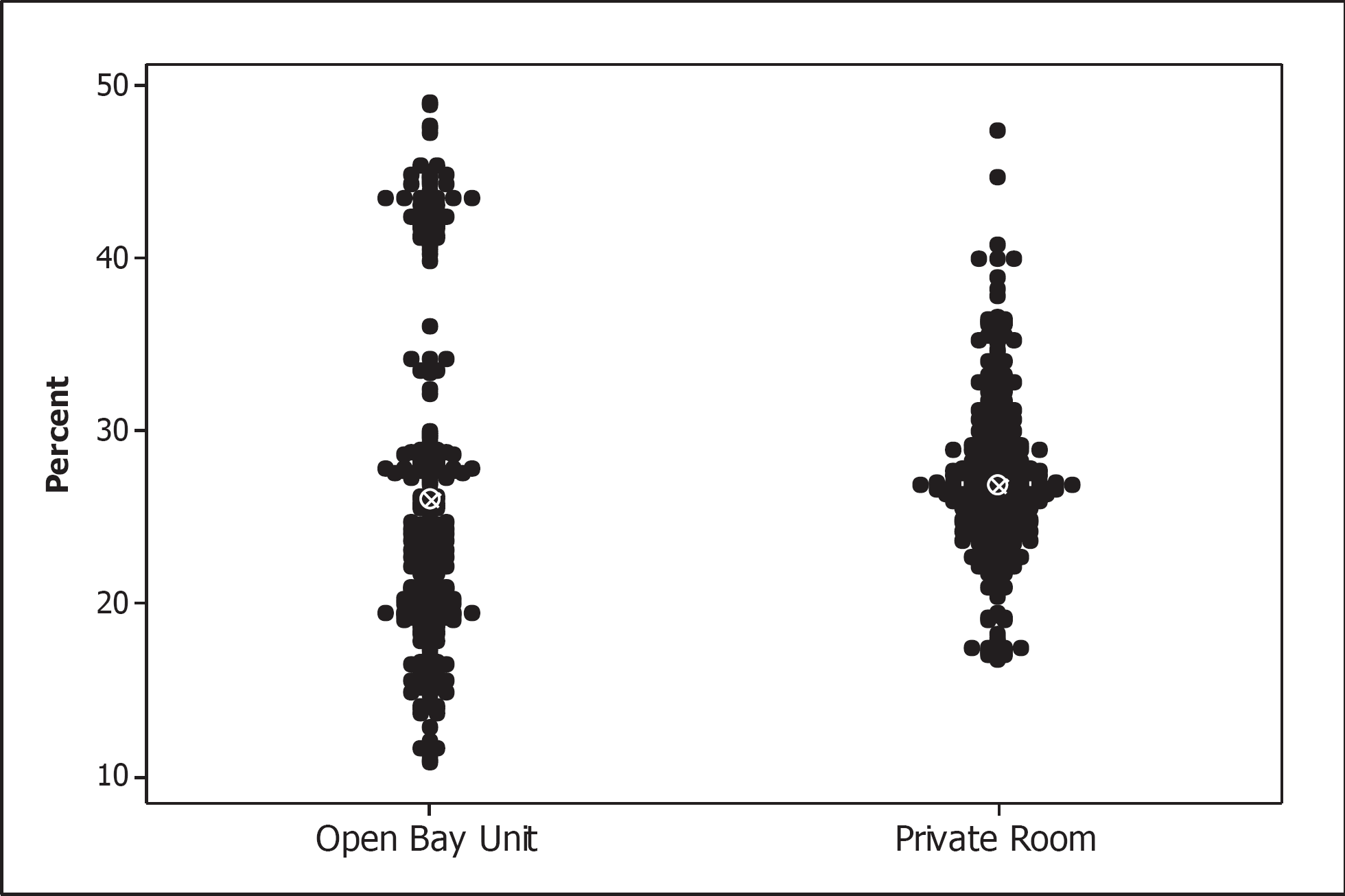
Distribution of room humidity readings in open ward and private room designs.
The humidity readings in the two units varied significantly. The open nursery NICU humidity readings showed a variance of 89.0, and the variance of the private room NICU readings was 20.7 (p < 0.0001), indicating that the ventilation system in the private room NICU supplied air with more stable humidity.
Discussion
Neonates are medically fragile and require a narrow range of environmental conditions to avoid adverse effects. Conditions that may be tolerable for older patients can cause distress or harm to neonates. Standards for optimal NICU design have been published and updated periodically as new research findings emerge. Single-patient rooms have become the preferred design for all hospitals, although the private room concept was applied to the NICU several years after it became the standard for adults and pediatrics. The hospital redesigned its 45-bed open ward NICU to a private room design in 2007. Measurements were taken to determine whether private rooms facilitated optimal environmental conditions for neonates.
High sound levels can damage the hearing of neonates, disturb their sleep, and produce a variety of unwanted physiologic responses (American Academy of Pediatrics, 1997). Both of the NICU designs measured were very quiet. Both employed sound-reducing products like sound-absorbent flooring, ceiling, and wall coverings. The median sound levels in both NICUs (45 and 43 decibels) were at the level of human whispering. Only five readings above the recommended maximum 65 decibels were taken in the open nursery NICU and six readings in the private room NICU. All the high readings were accounted for by temporary noises such as patient crying, equipment alarms sounding, or someone talking on the telephone.
This study showed a two-decibel median reduction in sound from the open ward to the private room design. This result is similar to those of Chen and colleagues (2009) and Stevens et al. (2007). Both of these studies found a 4.5-decibel reduction in private rooms.
Sound is mainly the result of human activity. A level III NICU was shown to have higher sound levels than a level II NICU, presumably because of more noise-generating devices (Levy, Woolston, & Browne, 2003). One might expect that sound levels would be higher in the day than during the night because of more human activity. Noise levels in the NICU during the day are typically higher than at night (Matook, Sullivan, Salisbury, Miller, & Lester, 2010), although one study (Darcy, Hancock, & Ware, 2008) did not show a difference between daytime and nighttime readings. Noise can come from unexpected sources. One study showed that motorized paper towel dispensers were a source of avoidable noise (Brandon, Ryan, & Barnes, 2007).
Lighting in patient care areas requires balancing several competing objectives. Natural light is more environmentally responsible if it can replace part of the artificial light. Natural light and views of nature are considered desirable for the psychological benefit of staff and visitors, so windows have become a common feature of new hospitals. Typical hospital windows, however, contribute levels of light in the daytime that exceed the maximum recommended light levels for neonates, so windows in patient rooms must be tinted and shades used to prevent the admission of too much light.
Typical hospital windows, however, contribute levels of light in the daytime that exceed the maximum recommended light levels for neonates.
Lighting in a multibed NICU tends to be set at the level needed by the patient who requires the most light. In contrast, a private room design allows for individualization of light for each patient and average light levels are significantly lower (Stevens et al., 2007). The most common room layout in the private room NICU employs an 88.5-square-foot window. This study found that the windows in the private room NICU contributed to nearly all of the ambient light readings that exceeded the recommended maximum. Several high light readings were taken when task lights were left on in the room, but no patient care was being given at the time and the task light should have been turned off—a human error. One can control the individual light exposure of neonates in incubators by using covers over the incubator (Lee, Malakooti, & Lotas, 2005), but patients in cribs or bassinettes are subject to the ambient light level in the room (Lasky & Williams, 2009).
The results of this study suggest that NICU designs with generous windows in patient rooms may call for guidelines that establish blind and lighting settings that reach 60 foot-candles and preclude staff from turning on all the artificial lights when the window shades are open to prevent the ambient light level from exceeding the maximum. It may be desirable for NICU lighting to be controlled by ambient light sensors and variable lighting controls that would not allow the total light level in the room to exceed a preset limit unless task lighting were needed for a procedure. A coordinated system of light control would enable the cycling to be programmed into all rooms and eliminate the need for manual staff control of each room.
Nicu temperature should be adjusted to be optimal for the patient, not for the staff or visitors.
Neonates' ability to maintain stable body temperature develops as they grow, so the optimal temperature range for the NICU is fairly narrow, 72–78 °F. Modern HVAC systems supply air that is remarkably constant in temperature, but people can change the thermostat settings, and windows and equipment may contribute to heat loss or gain in localized spaces.
These data show that the private room design produced a more stable temperature. When the open ward nursery temperatures were out of the recommended range, they were too warm. When the private room temperatures were out of range, they were too cool. In the open nursery design, each nursery had a thermostat. In the private room design, each room has a thermostat. The HVAC system in the NICU might benefit from programming a preset temperature range into the thermostats that would allow the temperature to vary only from 72 °F–78 °F. Temperature perception is subjective, and parents and staff may differ in their comfort preferences, but the NICU temperature should be adjusted to be optimal for the patient, not for the staff or visitors.
In this study, more temperature variation was seen at night; variation was less during the day. Temperature variation in the open ward environment was the result of high temperatures at night, when temperatures were sometimes above 80 °F. This was possibly caused by staff manipulation of the thermostat rather than instability in the HVAC system. Temperatures within one eight-bed ward were more unstable than the others. It was common in the open ward nursery to have a temperature variation of up to 6 °F when measurements were made at different points within that room. Readings taken in spaces near windows tended to be cooler, and readings in the center of the nursery were warmer, reflecting the lower efficiency of the older windows.
Mean humidity levels in the two NICU designs were nearly identical, although the private room design showed more stability in the readings. Humidity levels in both NICU designs were too low. Sampling periods for both units were in the months of February and March, when outside ambient air was cold and required heating before distribution through the HVAC system. Outside humidity levels ranged from 29–88% during the open nursery readings and from 43–93% during the private room readings, so there was ample humidity in the supply air to meet the recommended levels. These data suggest that these HVAC systems may remove too much moisture from the supply air, and attention should be paid to maintaining the recommended humidity levels to avoid discomfort in patients, staff, and visitors.
This study clearly demonstrates that a private room design can be superior to a multibed open design for achieving optimal environmental conditions for the development of neonates. Some improvements in environmental control would be possible by retrofitting an existing space with new equipment and changing staff behavior, but this study supports the conclusion that the private room design alone achieves significant advantages over other designs.
Footnotes
Acknowledgments:
The authors acknowledge the significant contributions and support of the following individuals: Stephanie N. Means, Shannon Bowerson, and Lauren Lambert (Western Michigan University); Kuanwong Watcharotone, PhD (Western Michigan University and Bronson Methodist Hospital); Karen Fleetwood; Seth Malin, MD; Peggy Malnight, RN; Jamie McCune, RN: Mary Steinke, RN; Tina Sullivan, RN; and Jackie Wahl, RN (Bronson Methodist Hospital).