
Abstract
Objectives:
This study examines the role of visibility and proximity on nurse communication patterns, perception of privacy, and efficiency in double-corridor nursing units.
Background:
Nurses are extremely important for the quality of healthcare. The literature suggests that visibility and proximity have a substantial impact on the delivery of care and staff experience. However, few studies have empirically examined nursing units in China.
Method:
Questionnaire surveys, observations, and simulations of medication administration tasks were employed.
Results:
Visibility and proximity influenced communication patterns, perceptions of privacy, and efficiency. The type of wall in the medication room could impact nurses’ perception of privacy and efficiency. A partial glass wall in the medication room could achieve balance between privacy and visibility. A medication room that is adjacent to and is easily accessed from the nurse station (NS) could provide efficient communication and efficient work. The partition type between the NS and the doctor’s office and the layout of the medication room could impact communication patterns. The relative position of the NS, medication room, and disposal room could influence the flow of medication administration tasks, and a geographically contiguous spatial layout could enhance work efficiency.
Conclusions:
The findings contribute to the body of knowledge on the impact of visibility and proximity on nurses’ communication patterns, perception of privacy, and efficiency. Recommendations to improve the design of double-corridor nursing units are also provided.
The design configurations of a layout could affect visibility and proximity in healthcare settings. The presence and locations of space boundaries, such as walls and partitions, impact the degree of visibility (Johanes & Atmodiwirjo, 2015). Simple unit shape and multiple nurse stations (NSs) could increase patient visibility (Pati, Harvey, & Cason, 2008). Proximity is another substantial design feature for teamwork and communication. The effect of the configuration of nursing units (centralized and decentralized) on proximity is supported by evidence. The visibility and proximity that are impacted by the physical environment are recognized as important environmental features that have implications for the delivery of care.
Visibility Affects Communication and Privacy
The spatial environment of healthcare settings could impact communication between nurses and team members (Gharaveis, Hamilton, Pati, & Shepley, 2018; Gum, Prideaux, Sweet, & Greenhill, 2012). Visibility impacted by physical environment (Calleja & Forrest, 2011; Gharaveis, Hamilton, & Pati, 2018; Pati, Harvey, & Pati, 2014) could improve teamwork (Lu & Zimring, 2012) and collaborative communication (Gharaveis, Hamilton, Pati, & Shepley, 2018). A previous exploratory study conducted in nursing units under special circumstances (with extra beds in corridors and patient rooms) found that physical barriers could obstruct visibility and impede communication (Chen, Xuan, & Li, 2018). Communication was the most frequent activity (Xuan, Li, & Chen, 2019), and it costs nurses a large amount of time (Hendrich, Chow, Skierczynski, & Lu, 2008). Studies have emphasized the importance of promoting communication through opportunistic meetings (Becker, 2007) and peer lines of sight (Gurascio-Howard & Malloch, 2007).
Privacy in healthcare environments is another important factor that could influence staff satisfaction and performance (Zamani, 2019). Leino-Kilpi et al. (2001) defined privacy in the physical dimension as “the degree to which one is physically accessible to others” (p. 665). The design of nursing units could affect patients’ physical privacy (Lu, Cai, & Bosch, 2016). Research has shown that solid walls (Calleja & Forrest, 2011), partitions at registration, and team rooms in pods are beneficial for improving privacy (Zamani, 2019). Understanding the balance between visibility and perception of privacy is an important issue (Fay, Cai, & Real, 2019).
Proximity Affects Communication and Efficiency
Proximity influenced by spatial design could also impact communication and efficiency. Most of the studies related to the proximity of physical environments have focused on decentralized and centralized layouts in emergency departments (EDs; Zamani, 2019) and nursing units (Fay, Carll-White, Schadler, Isaacs, & Real, 2017; Hua, Becker, Wurmser, Blissholtz, & Hedges, 2012). Decentralized pods with close proximity in EDs could increase the efficient assessment of patients (Zamani, 2019). Decentralized nursing units could create close proximity to patients, increase the number of visits to patients, and increase the opportunity for communication (Gurascio-Howard & Malloch, 2007).
A large number of studies have shown that communication plays an important role in quality care (Kilner & Sheppard, 2010; Salas, Rosen, & King, 2007). However, a literature review demonstrated that examining the impact of physical design of healthcare settings on communication was relatively rare (Gharaveis, Hamilton, & Pati, 2018). Among these studies, the majority have focused on centralized and decentralized nursing units (Fay et al., 2017; Hua et al., 2012) and EDs (Gharaveis, Shepley, Hamilton, Pati, & Rodiek, 2019; Naccarella, Raggatt, & Redley, 2019; Zamani, 2019).
The difference in design between China and the United States results from cultural differences. China is a society of collectivism; staff value proximity for team members and better visual connection within groups (Cai, Lu, & Sheward, 2019; Cai & Zimring, 2019). Few studies have been conducted on Chinese nursing units. Cai et al. (2019) investigated the Chinese nursing unit from 1989 to 2015 and found key factors that shape Chinese nursing unit design. By studying 25 nursing units in China, Lu and Wang (2014) found that a single patient room is rare, and the nursing unit in China has a larger size and longer distance from the nursing station to the patient bedside than that in the United States. The study selected a double-corridor nursing unit as it is unique in China and was adapted from a racetrack nursing unit for culture-related reasons. This type of layout could provide space for backstage communication (Cai & Ziming, 2019), privacy for staff, and better visual and proximity within team members compared with radial, triangular, cluster, single corridor, and racetrack units (Cai et al., 2019). The relationship between environmental features related to visibility and proximity and its influences on nurses’ communication patterns, perception of privacy, and efficiency in the Chinese nursing unit is less well understood. Based on the previous pilot study (Chen et al., 2018), this study aims to explore the mechanism of two types of spatial layouts of double-corridor nursing units by examining (1) how the physical environments of nursing units impact visibility and proximity and (2) what influences visibility and proximity have on communication patterns, perception of privacy, and work efficiency.
Method
Data collection methods of on-site observations, questionnaire surveys, and analysis of plan drawings were employed in this study. To obtain a better understanding of the study, the researchers had interactive walk-through tours and pilot interviews with nurses at selected units. The study was approved by the institutional review boards at the researchers’ academic institution and the research office at the hospitals.
Research Setting
Four nursing units at two hospitals in China were selected for the study. Both of the hospitals belonged to university healthcare systems. Each of the hospitals provided access to two medical inpatient nursing units.
The two types of units had largely similar patient types, number of patients per nursing station, number of nurses per nursing unit, number of beds, number of patient rooms, and physical layout (Figure 1 and Table 1). The NS size was approximately 20 m2, and the length of stay was 7–14 days at both hospitals. The selected medical units had different designs with regard to the location and configuration of the NS, medication room, and disposal room. The two major differences were as follows: (1) The medication room of the nursing unit at Hospital S was adjacent to the NS, with a sliding door connecting the medication room to the NS and another door toward the patient corridor, while at Hospital E, there was a short passage between the medication room and the NS, and the distance between the two spaces was approximately 3 m (9.8 ft). (2) The rear of the NS was enclosed by a solid partition at Hospital S, while the NS at Hospital E did not have partition.
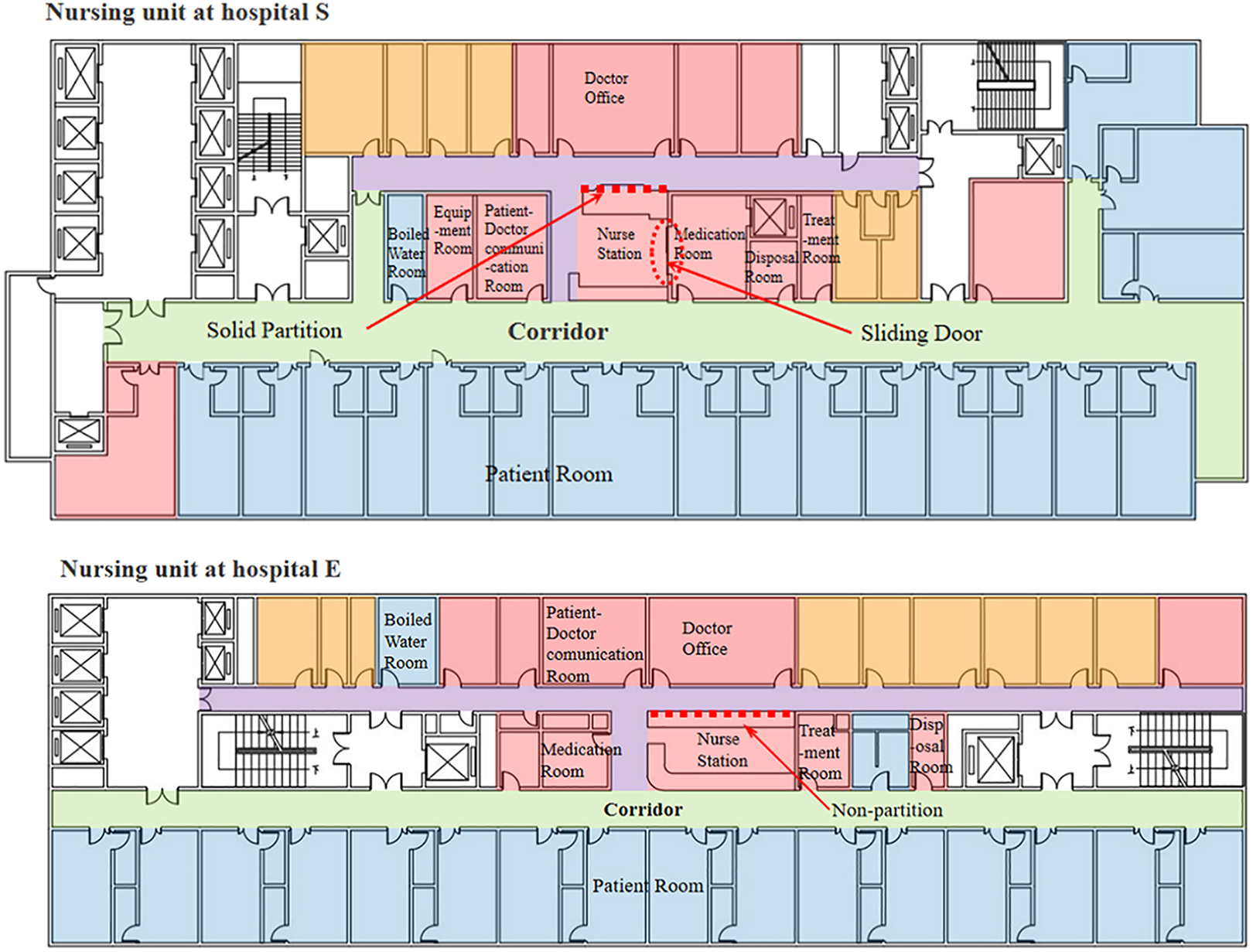
Nursing unit layouts at two hospitals.
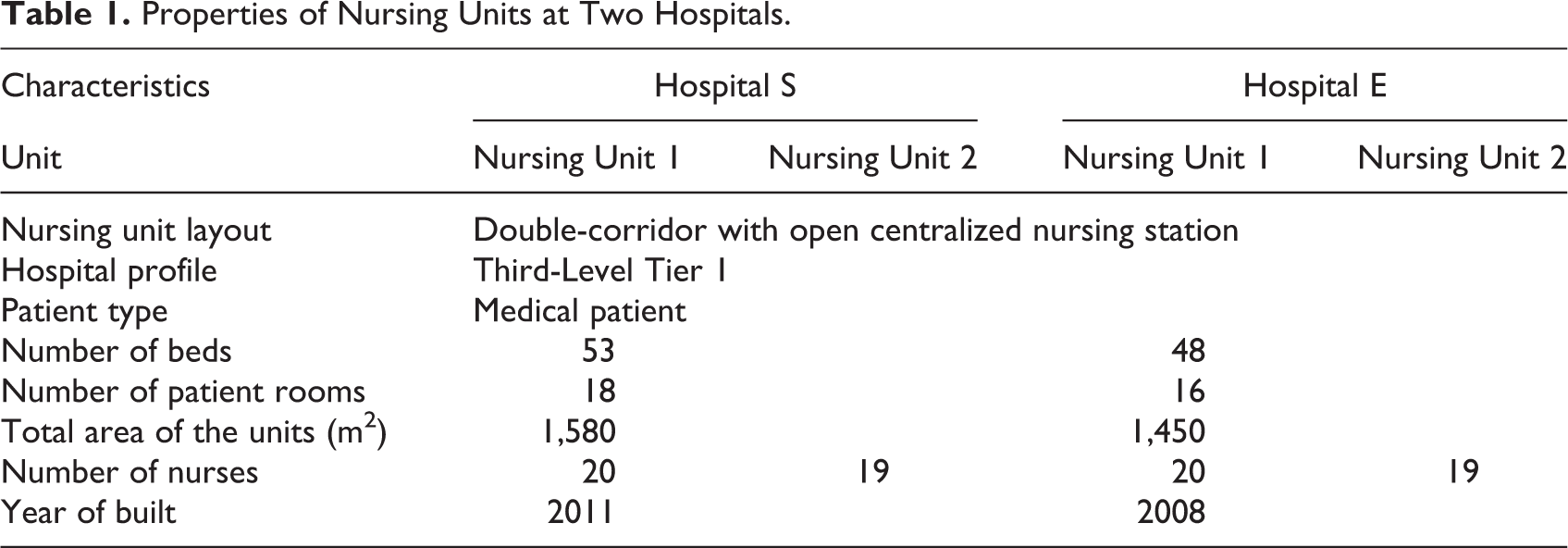
Properties of Nursing Units at Two Hospitals.
Observations
The corridors of the selected nursing units were so long that one researcher could not observe the entire unit; therefore, the nursing units were divided into three sections. One researcher stood at each section and recorded the communication patterns, locations, and frequencies on a plan drawing. Each researcher observed 480 min (9–12 a.m., 3–6 p.m., and 7–9 p.m.) of interactions in each unit; in total, 5,760 min of interactions were observed for the 4 units.
Questionnaire Survey
The questionnaire was developed in two stages. First, items of the questionnaire were identified based on relevant research literature, pilot interviews, observations, and features that reflected the characteristics of the design. Second, a draft questionnaire was created, and a pilot study was conducted to test the survey instrument. The questionnaire was sent to the nurses at two hospitals to improve the wording or delete some items to reduce the length of the questionnaire.
The final 37-question survey included three parts. Nurses were asked to respond to a survey that included a series of standardized measures and open-ended questions. The first part comprised the demographic background, which included years of experience, nursing type, and age. Part 2 comprised structured questions that asked participants to rate the perception of an item on a 5-point scale or to select the most satisfied environment feature from two or three pictures while providing further comments on why they made the choice. Part 3 comprised nonstructured questions. The participants were asked to identify and provide the three most important characteristics of the nursing unit that influenced their level of satisfaction and work efficiency. With the floor plans of the nursing units, nurses were invited to adjust the layout to be the most efficient and comfortable unit according to the respondent own experience and to make comments on the modification. The open-ended comments from the questionnaires were analyzed using a qualitative content analysis (Lincoln & Guba, 1985). The meanings in the content were extracted and then the units of information were identified, organized, and sorted according to the contents and meanings of the comments.
The questionnaires were sent to all 78 nurses in the four units and collected after 2 days. The response rates varied by unit, ranging from 78.9% to 100%. At Hospital E, the response rates were 95% (19/20) and 84.2% (16/19); at Hospital S, the response rates were 100% (20/20) and 78.9% (15/19); a total of 70 nurses returned the questionnaires.
Simulation of Work Efficiency
Delivery of medication was the activity that cost nurses most of their working time (Xuan, Li, & Chen, 2019). In this study, the medication administration task was selected as a specific task to examine the effects of the physical design of nursing units on nurses’ workflow. The work efficiency examination was developed under the assumption that the flow of a medication administration task was simulated without the use of a workstation-on-wheels (WoW) in the corridor. This assumption was made because the double-corridor layouts of the selected nursing units were the most common type in China (Cai et al., 2019); however, only some Third-Level Tier 1 Hospitals have WoWs in nursing units. The simulation of a medication administration task without WoWs can more clearly reflect the differences in walking patterns influenced by spatially related differences.
Results
Questionnaire Survey
Based on the characteristics of the design configurations in the pictures and the accompanying comments, the study found the following issues.
The effect of proximity on communication and efficiency
Regarding the position of the medication room, at Hospital E, 42.9% of the nurses chose Medication Room 1 and 57.1% of the nurses chose Medication Room 2. At Hospital S, 28.6% of the nurses chose Medication Room 1 and 71.4% of the nurses chose Medication Room 2. At both hospitals, more than half of the nurses preferred to stay in the medication room, which is adjacent to and is easily accessed from NSs (Figure 2). According to further comments, the main reason why nurses chose Medication Room 2 was that it facilitated efficient communication, connections, and work for nurses. Nurses commented that “Medication room 2 provides us with more independent space, and we have higher working efficiency”; “It is close to the NS and facilitates communication with nurses in the NS”; “It provides relatively independent space, more privacy, and less interruption”; “It is close to the NS and convenient”; and “It has access to the NS, which could improve efficient communication.”
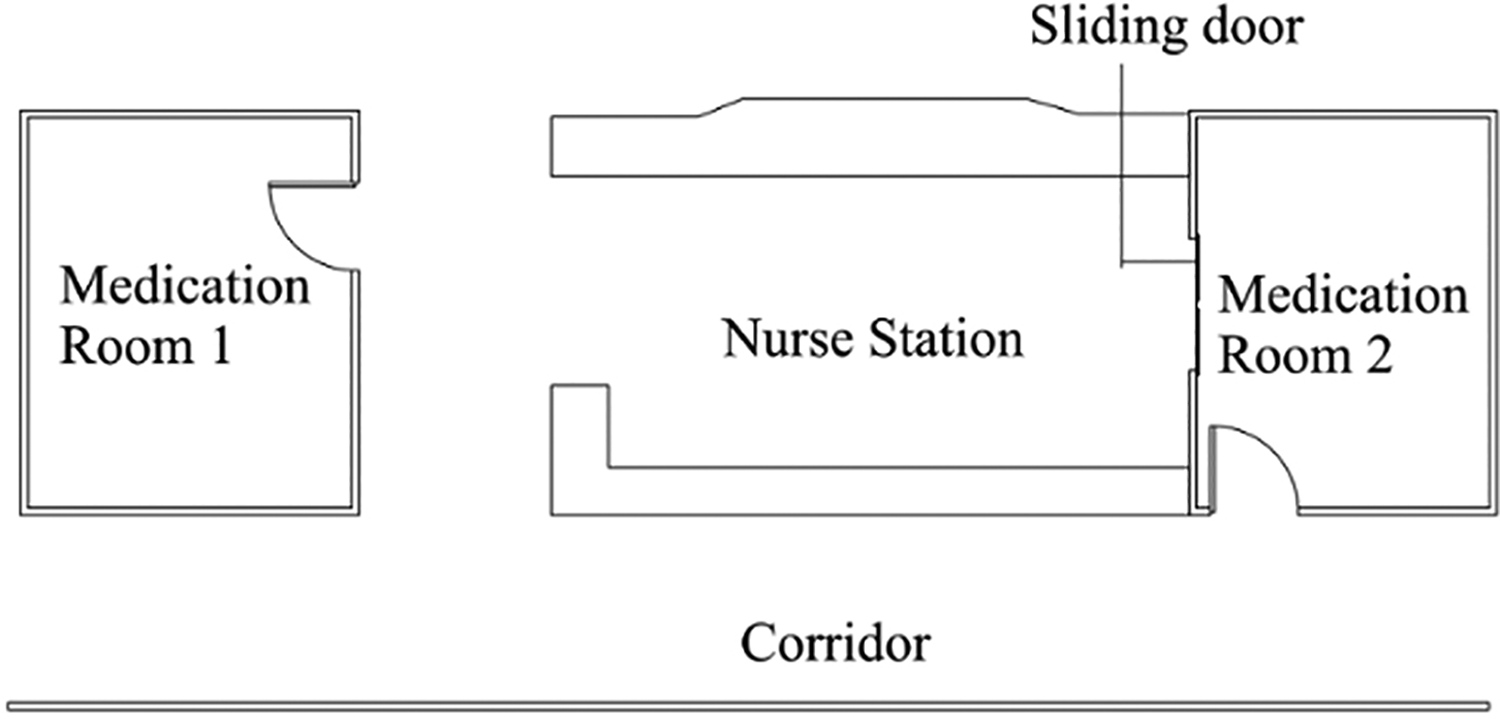
Location of medication room.
The effect of visibility on privacy and efficiency
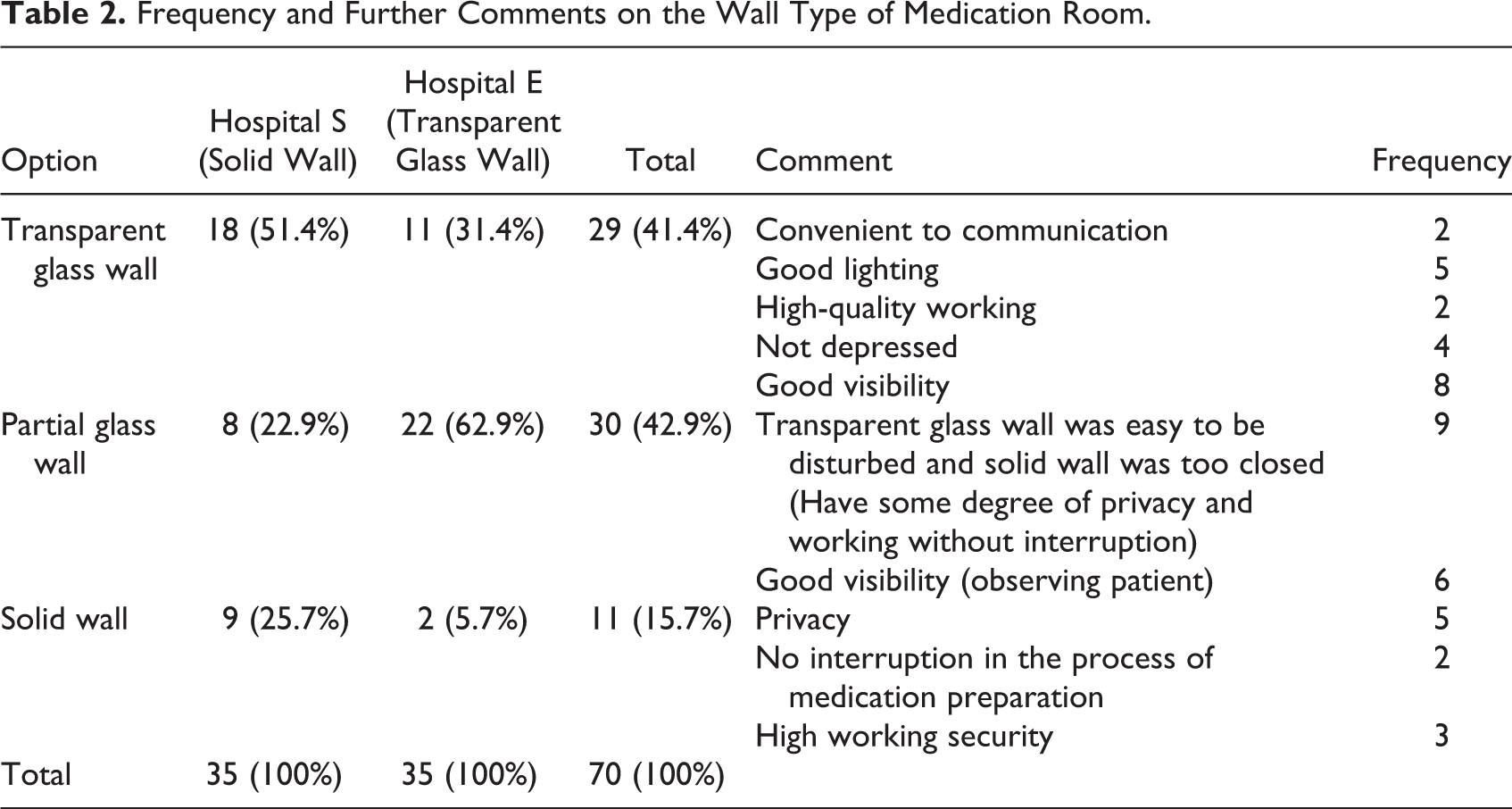
The medication room had a transparent glass wall at Hospital E and a solid wall at Hospital S. When the nurses were asked about the preference of the type of wall (Figure 3), most of the nurses at Hospital E preferred a partial glass wall, and the majority of the nurses chose a transparent wall at Hospital S. The frequency and further explanations of why they made the choices are shown in Table 2.

Type of walls of medication room.
Frequency and Further Comments on the Wall Type of Medication Room.
The effect of visibility on communication
For the partition type between the NS and the doctor office (DO; Figure 4), the rear of the NS at Hospital S was a solid partition, while there was no partition at Hospital E. At Hospital E, 11.4% of nurses chose a solid partition, 34.3% of nurses chose a glass partition, and 54.3% of nurses preferred no partition. Most of the nurses (51.4%) at Hospital S chose a solid partition rather than a glass partition or no partition (Table 3). The majority of the nurses chose the types that they were currently using at each hospital. Nurses explained that they were accustomed to the current type and were unaware of the value that other design schemes could bring to them. It is the designer’s and researcher’s responsibility to provide users efficient design to improve communication. Further comments demonstrated that without a partition, nurses could communicate conveniently and efficiently with doctors, and the atmosphere of the NS was bright and spacious. Nurses who chose no partition commented that “The space appears to be bright and large” and “The NS has good visibility of the doctor’s office, and it is convenient to communicate with doctors.”

Type of partitions at back of nurse station.
Number of Choices of Wall Types at the Rear of Nurse Station.
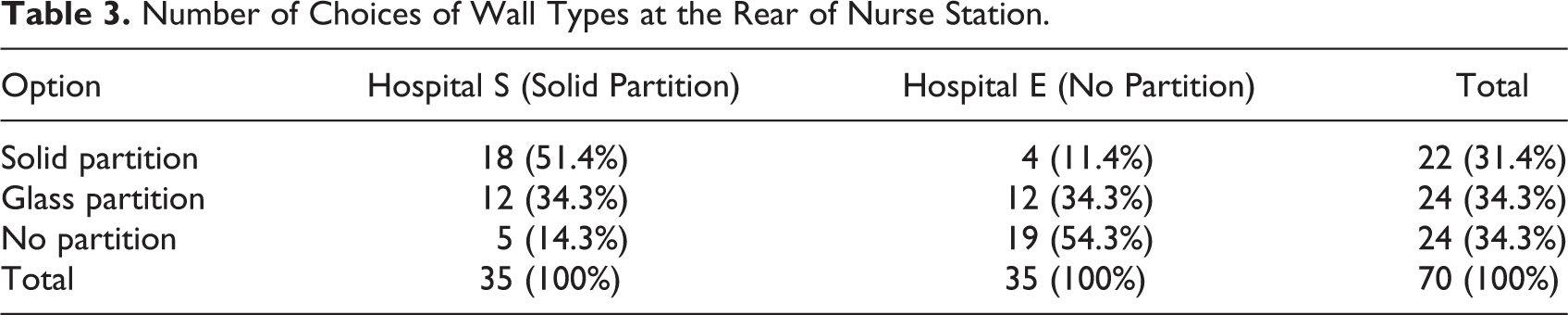
Glass partitions could have good lighting and visibility while maintaining some privacy. Nurses reported that “It could provide good lighting and some degree of privacy” and “It is convenient for us to observe the doctor’s office, and easy to communicate with doctors.”
For solid partitioning, nurses’ comments were all related to the perception of privacy. They commented that “It could protect our privacy,” and “It could give doctors and nurses private spaces.”
Improvements of nursing units proposed by nurses
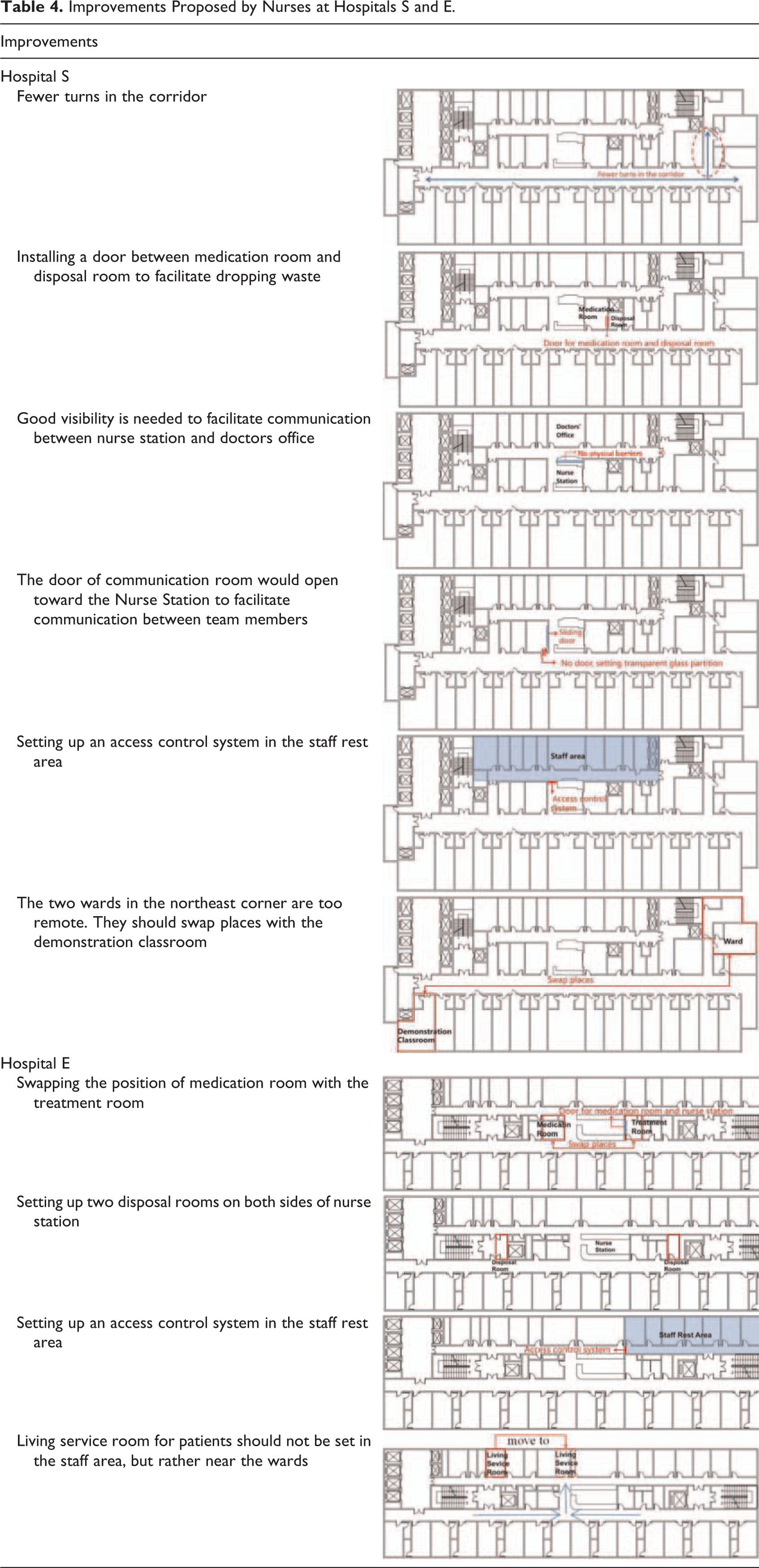
For the part of the nonstructured questions in the questionnaire, floor plans of the nursing units were provided for nurses. To make an efficient and comfortable unit, nurses could adjust the layout or equipment based on their working experience. Table 4 summarizes the nurses’ modifications and comments.
Improvements Proposed by Nurses at Hospitals S and E.
Location of WoWs
At both hospitals, the WoWs were placed beside the door of the patient room in the corridor. The WoWs were used as decentralized medication rooms, which could reduce nurses’ walking distance (Xuan et al., 2019). In this study, the nurses were asked to mark the most efficient place for the WoWs according to their working experience. By overlaying the drawings, we found that the most preferred place for the WoWs at both hospitals lies approximately at the midpoint between the NS and the end of the corridor (Figure 5). The use of WoWs could achieve a balance between proximity and visibility. When the nurses stood at the two places that they had marked for WoWs, they were close to patients, and the team members in the NS could also see them
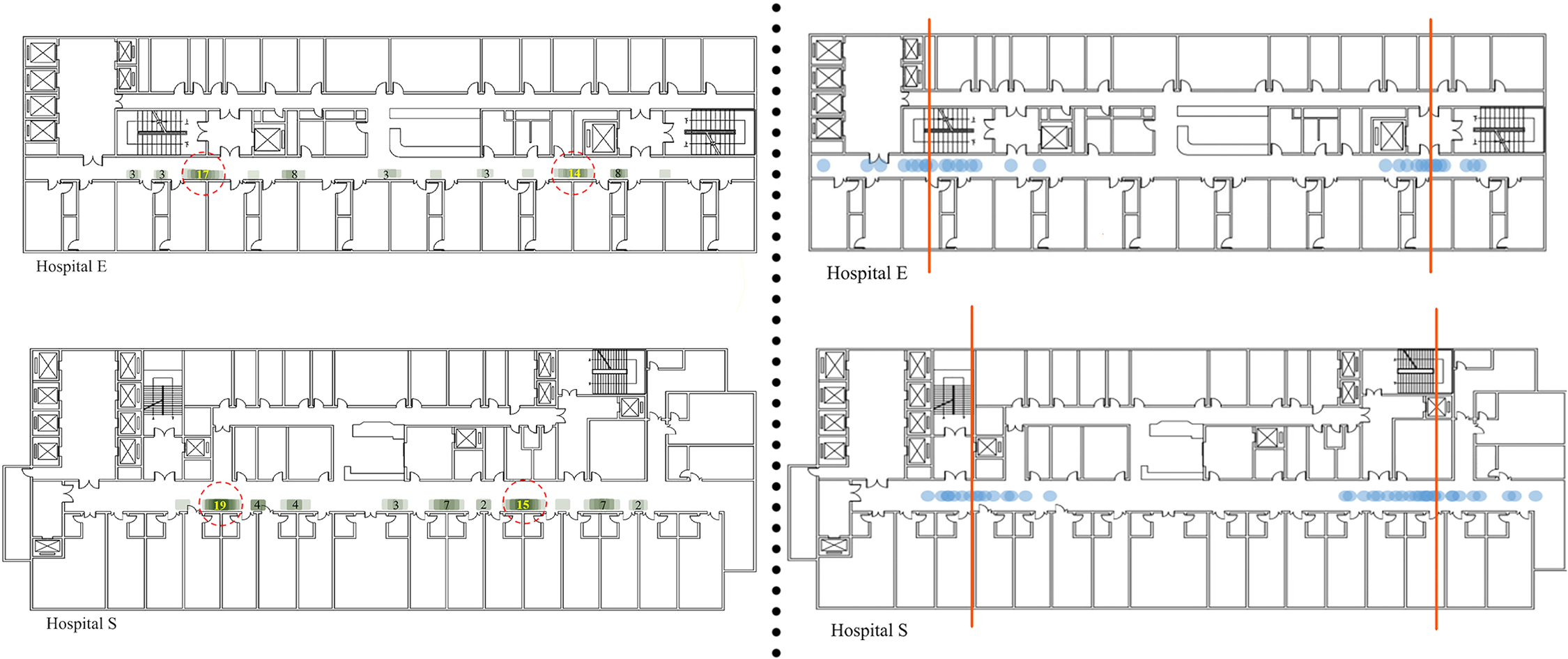
Reported location of workstation-on-wheels (left) and length of corridor (right).
The acceptable farthest boundary of the patient corridor
In the questionnaire, nurses were invited to point out the acceptable farthest boundary of the corridor based on their working experience. After overlaying the points, it is shown that the ideal length is far less than the actual length of the corridor (Figure 5). The lengths of the corridors at Hospitals S and E were 72 and 68 m (236 and 223 ft), respectively, and the ideal length of the corridor at both hospitals was approximately 48 m (158 ft). Corridor shape and length were correlated with visibility in the ICU, and shorter corridors could provide better visibility (Hadi & Zimring, 2016)
Observation
Observation was conducted to identify possible relationships between visibility and communication patterns. The visibility and proximity impacted by the physical environments could influence the communication patterns between nurses and team members.
The total numbers of communication events between nurses and team members were 391 and 447 at Hospitals S and E, respectively. Communication events between nurses and between nurses and doctors accounted for 66.4% and 33.6% of total episodes at Hospital E, respectively, and 70.1% and 29.9% of total episodes at Hospital S, respectively.
Effect of visibility on communication
Locations and means of communication between nurses and doctors could be impacted by the partition types between the NS and the doctor’s office. The contents of the communications between nurses and doctors were related to confirmation of the medication orders. The total number of communication events was 267, with 44% from Hospital S and 56% from Hospital E. At both hospitals, the most common places where the communication occurred were the NS and the doctor’s office, which accounted for 74.3% and 77.3% of the total communication episodes at Hospitals S and E, respectively. Additionally, at Hospital E, there is no solid partition between the NS and DO; nurses often stand at the NS and speak loudly to doctors in the doctor’s office. This pattern accounted for 28% of total communication events at Hospital E, while it accounted for 0% at Hospital S, which had a solid partition at the rear of the NS. Figure 6 shows the locations, ways, and frequencies of communications at both hospitals.
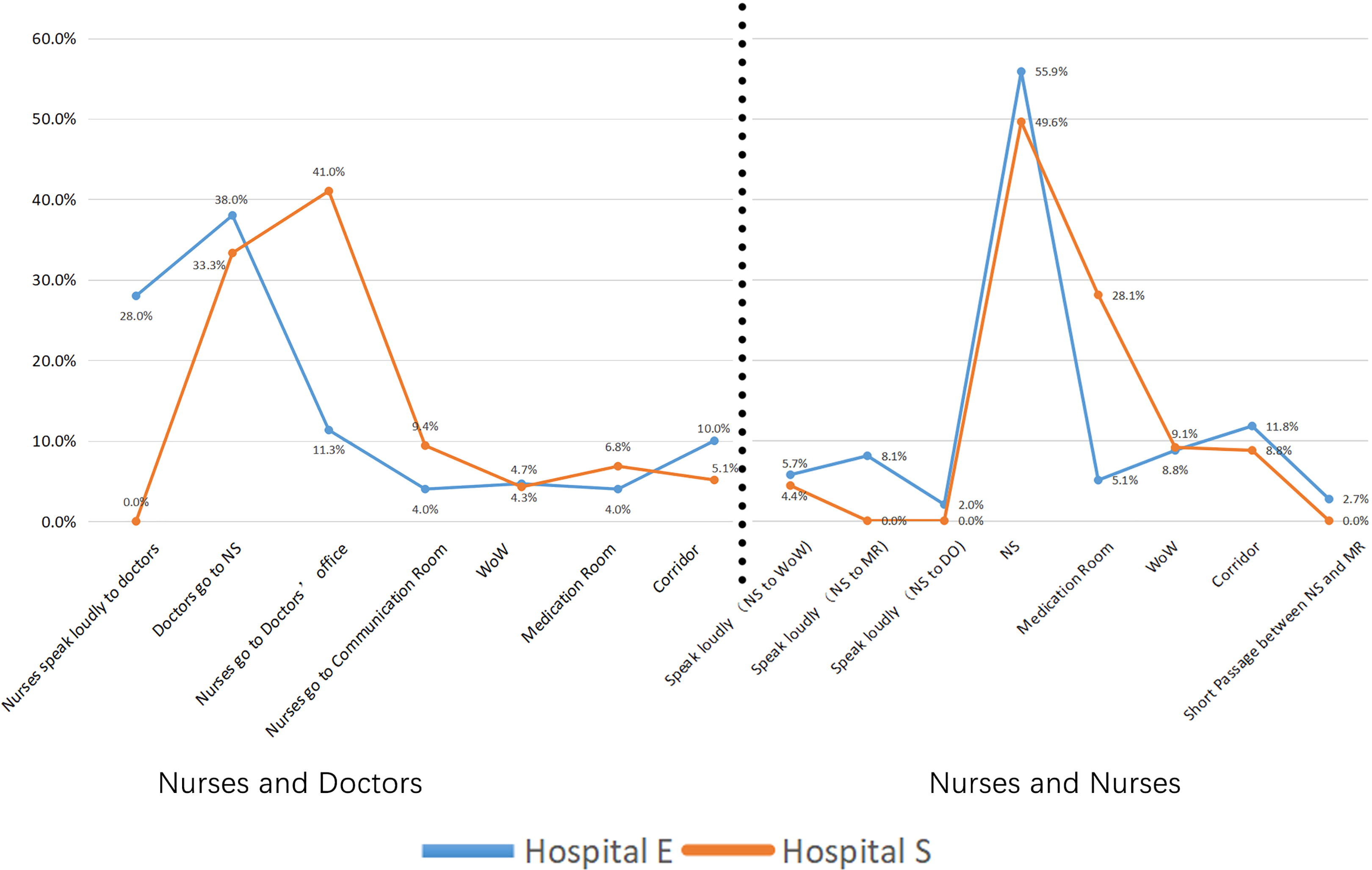
Communication pattern between nurses and doctors (left) and nurses and nurses (right).
Effect of proximity on communication
The proximity of the medication room to the NS could impact the communication patterns between nurses. The contents of the communication between nurses were related to patient’s information and medication use. The total number of communication events between nurses was 571, with 48% from Hospital S and 52% from Hospital E. The most frequently used location for communication at both hospitals was the NS (49.6% and 55.9%). At Hospital E, nurses in the NS usually spoke loudly to other nurses in the medication room, doctor’s office, and WoW, which accounted for 15.8% of total communication episodes. At Hospital S, nurses in the medication room adjacent to the NS could communicate conveniently with nurses at the NS; therefore, the percentage of communication that occurred in the medication room was much higher at Hospital S (28.1%) than at Hospital E (5.1%; Figure 6).
Simulation of Work Efficiency
Effect of proximity on efficiency
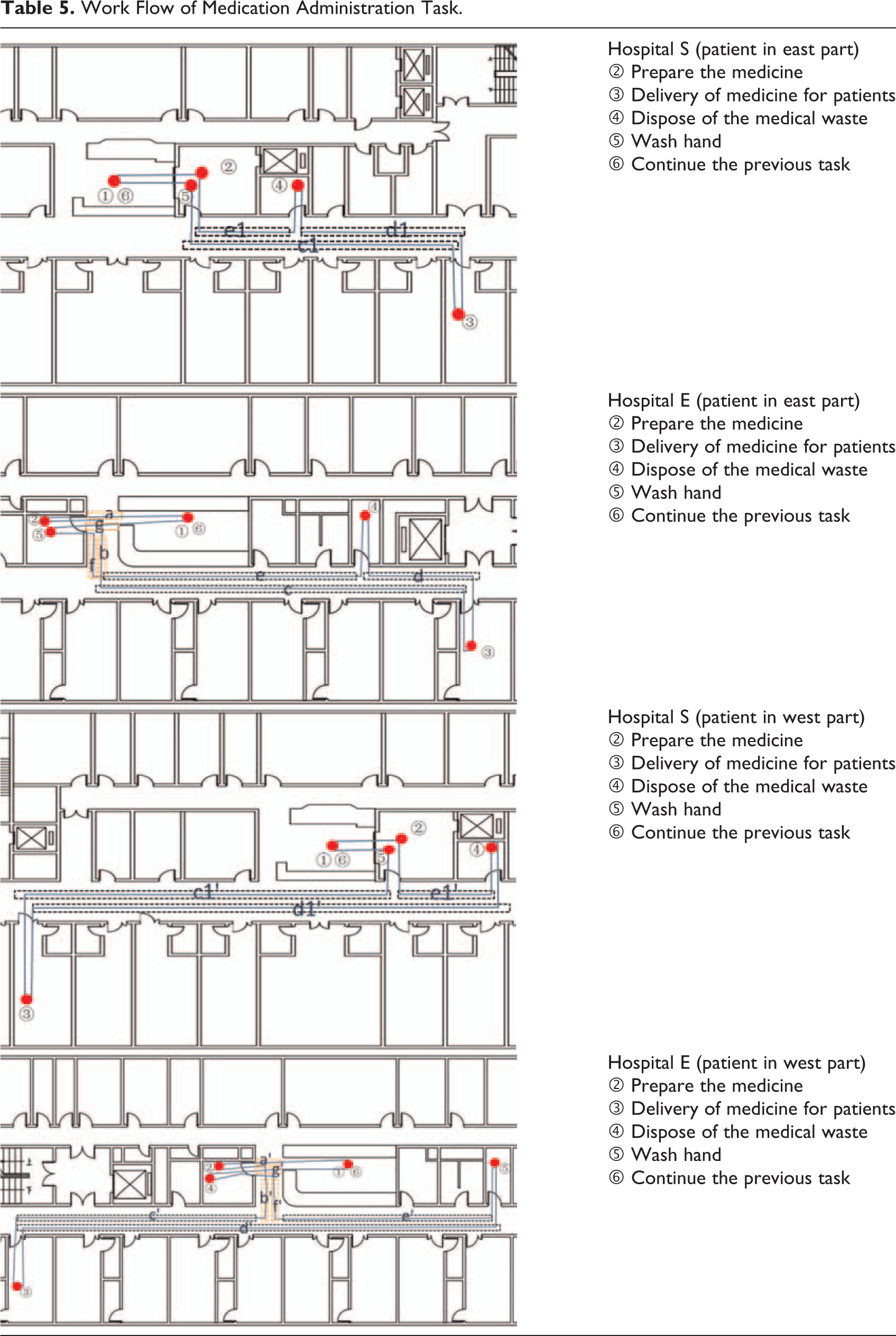
According to the observation, the medication administration task included four steps: preparing the medicine, delivering medicine for patients, disposing of the medical waste, and handwashing. The relative position of the NS, medication room, and disposal room might influence the working efficiency. At Hospital S, the location of the disposal room is next to the medication room and is located close to the midpoint of the nursing unit. The location of the disposal room at Hospital E deviated significantly from the NS and medication room. When a patient called, the nurse went to the medication room from the NS to prepare the medicine and then went to the ward. After delivering the medicine to the patient, the nurse placed medical waste in a dedicated rubbish bin in the disposal room, and then nurse went to the medication room to wash her hands and finally returned to the NS to continue the previous task. Table 5 simulated the nurses’ paths of delivering medicine to patient rooms on both sides of the NS. When nurses walked to any of the rooms on the eastside of the unit, the total walking distance was c1 + d1 + e1 at Hospital S and a + b + c + d + e + f + g at Hospital E. The walking distance to any of the patient rooms on the westside of the unit was c1′ + d1′ + e1′ at Hospital S and a′ + b′ + c′ + d′ + e′ + f′ + g′’ at Hospital E. The simulation indicated that when patients called, the nurses in Hospital E needed to cross the public corridor between the NS and the medication room twice. The red rectangle in Table 5 stands for the extra walking distance (a + b + f + g, a′ + b′ + f′ + g′). In addition, for comparison purposes, we assume that the selected patient rooms on the eastside or westside of the unit had the same distance to the midpoint of the NS at both hospitals; then, the distance of c is longer than c1. The nurses at both hospitals need to go from the ward to the disposal room on the eastside of the unit since the disposal room at Hospital E is more deviated than the one at Hospital S and the distance of d′ is longer than d1′. The simulation indicated that the nurses’ walking distance at Hospital E is longer than the distance at Hospital S. The results of the simulation should be interpreted with caution. Nurses might not necessarily follow the optimal shortest distance when administrating medicine in intensive care units (ICUs; Lu & Seo, 2012).
Work Flow of Medication Administration Task.
Discussion
Effect of Proximity on Communication and Efficiency
The study showed that the position of the medication room could influence nurses’ efficiency and communication. A medication room that is adjacent to and is easily accessed from the NS could provide efficient communication and connections for nurses in the medication room and the NS.
A previous study showed that when staff members work together in close proximity, teamwork and communication could be promoted (Becker, 2007; Ritchey & Pati, 2008), and nurses are more likely to communicate face-to-face (Cai & Zimring, 2011) and work effectively as a team (Fay et al., 2017; Zborowsky, Bunker-Hellmich, Morelli, & O’ Neill, 2010). However, having a long physical distance between other team members decreased the opportunities for staff to assist each other (Kalisch & Begeny, 2005).
A previous study demonstrated that delivery of medication was the most time-consuming activity (Xuan et al., 2019). Therefore, this study made medication administration a specific task to simulate. Nurses need to walk to many specific places to conduct a single activity (Wolf et al., 2006). The simulation showed that the more divided the disposal room is, the longer the distance the nurses need to walk. The proximity of the NS, medication, and disposal room was an important factor in reducing walking distance and enhancing working efficiency. Healthcare designers should understand the workflow of the most time-consuming task before they design a nursing unit and arrange the clinical spaces efficiently based on the flow of the task. Combining the nurses’ comments, the medication room should be conveniently accessible to the NS, the results of which were triangulated by the questionnaire survey. It would be good to arrange a disposal room or a place on both sides of the NS to reduce the distance of dropping medical waste. The location of the handwashing station was also important for work efficiency. Handwashing stations should be conveniently accessible to the NS, medication room, and disposal room.
Effect of Visibility on Privacy and Efficiency
This study showed that the type of wall in the medication room could impact nurses’ perceptions of privacy and efficiency. The physical design of the medication room in the nursing unit could impact nurses’ efficiency (Conrad, Fields, Mcnamara, Cone, & Atkins, 2010). Without having visibility to other team members would decrease the probability of providing assistance to other team members (Kalisch & Begeny, 2005). Spatial relationships and design elements might affect patients’ privacy in a nursing unit, physical barriers could protect patients’ privacy in nursing units (Lu et al., 2016), and partitions and solid walls with doors could enhance the perception of privacy in EDs (Zamani, 2019).
In the follow-up site tour, researchers found that the medication room in Hospital E was modified by the nurses, with translucent glass paper put on the window (Figure 7). The modified window was similar to the partial glass wall in Figure 3. According to nurses’ comments, with the modification of the window, they could focus on their work and still have visibility to patients. Achieving a balance between visibility and privacy was important in the design of healthcare settings (Fay et al., 2019; Lu et al., 2016).
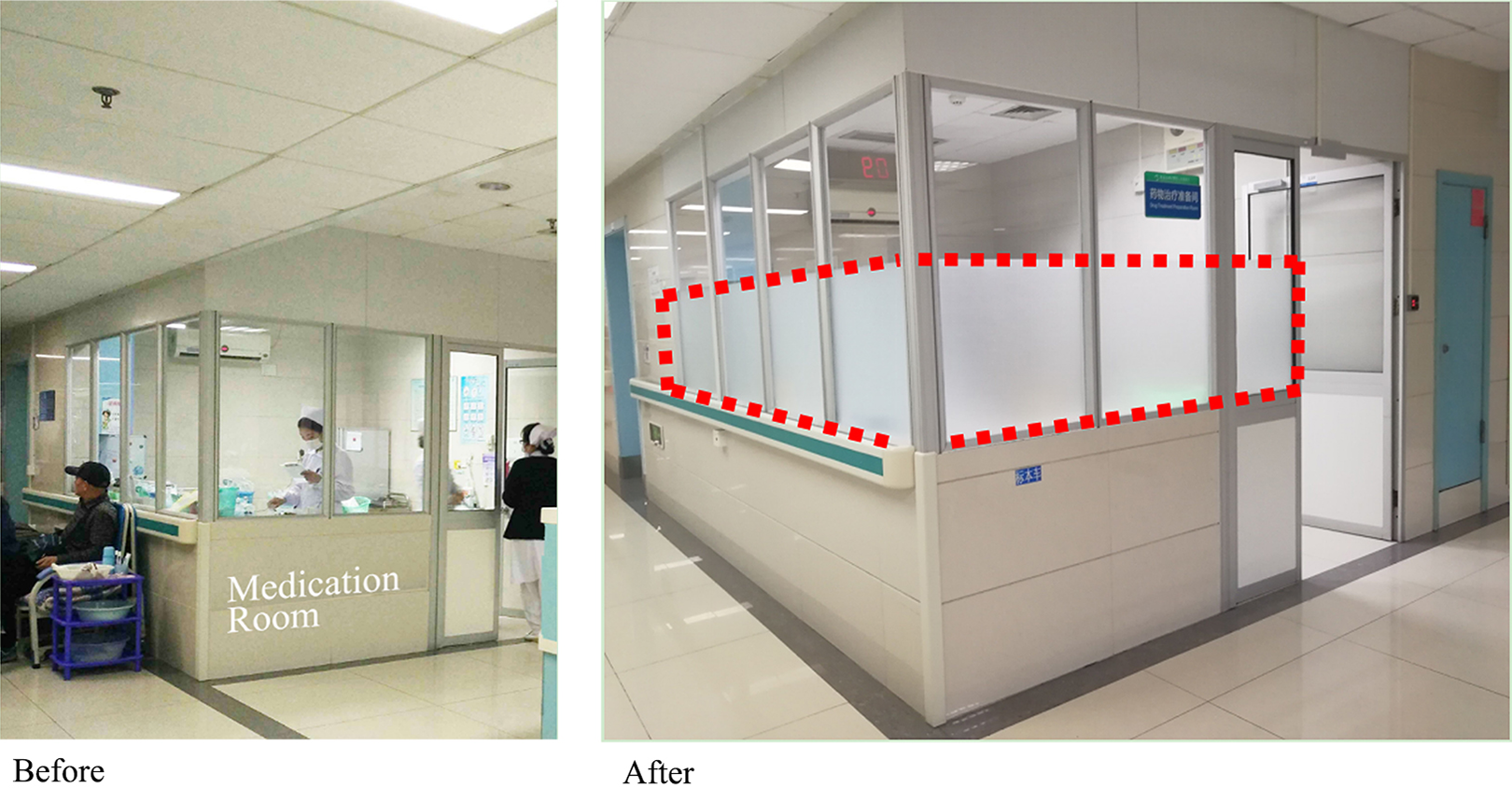
Modification of medication room wall.
Visibility on Communication
This study found that physical barriers, such as solid partition, should not be installed at the rear of the NS to block nurses’ views to doctors. Both the observation and further comments in the questionnaire survey showed that visibility could impact communication patterns between nurses and doctors.
According to the observation, the total frequency of nurses speaking loudly to doctors and nurses going to doctors’ office was 39.3% at Hospital E and 41.0% at Hospital S (Figure 6). The total percentages were similar. However, at Hospital S, the solid partition between the NS and doctors’ office prevents nurses from locating doctors; therefore, nurses must go to doctors’ office to communicate with doctors, which could increase nurses’ walking distance and decrease communication efficiency. The presence and locations of space boundaries, such as walls and partitions, impact the degree of visibility (Johanes & Atmodiwirjo, 2015), which is an important factor that influences communication between nurses and doctors (Becker, 2007; Trzpuc & Martin, 2010).
Limited physical accessibility might result in less communication between nurses (Trzpuc & Martin, 2010; Zborowsky et al., 2010). In this study, the frequency of communication between nurses in the medication room at Hospital S was much higher than the frequency of communication occurred in Hospital E. The medication room at Hospital S was conveniently accessible to the NS, which could enhance communication between nurses and nurses.
Communication between nurses and doctors plays an important role in improving the effectiveness and efficiency of medical care (Seneviratne, Mather, & Then, 2009). In healthcare settings, nurses spend considerable time walking to locate other staff members (Burgio, Engel, Hawkins, McCormick, & Scheve, 1990; Tucker & Spear, 2006) and doctors to deliver healthcare to patients (Hendrich & Chow, 2008). High visibility could increase communication and reduce travel time for nurses (Lu & Zimring, 2012). Through a systematic literature review, Gharaveis, Hamilton, and Pati (2018) claimed that the spatial layout that isolated nurses and doctors would obstruct visibility between nurses and doctors, which could hinder effective teamwork. Therefore, to improve teamwork, an enclosed layout that might impede visibility between team members should be avoided.
Conclusions
The study explored the influence of visibility and proximity on communication, perception of privacy, and efficiency. The findings could be used to improve the design of nursing units that enhance nurses’ communication and efficiency. The visibility would be improved by removing physical barriers between the NS and DO. This finding is congruent with the research conducted in Western hospitals. Isolated layout might impede visibility between team members and have a negative effect on the level of communication and teamwork in healthcare facilities (Gharaveis, Hamilton, & Pati, 2018). The type of wall in the medication room could impact nurses’ perception of privacy and efficiency. The partial glass wall of the medication room could achieve a balance between privacy and visibility. With this type of wall, nurses could not only focus on their work but also be able to see the patients and team members outside the medication room. The close proximity of the medication room to the NS could improve the frequency of communication and efficiency. Previous studies conducted in Western hospitals also found that enclosed spatial layouts were beneficial to improving privacy (Calleja & Forrest, 2011; Zamani, 2019), and when nurses work in close proximity, the likelihood of communication could be increased (Cai & Zimring, 2011; Fay et al., 2017; Zborowsky et al., 2010).
The ideal length of the corridor is approximately 50 m (164 ft), which is far less than the actual length of the corridor. The ideal location for WoWs is at the midpoint between the NS and the end of the corridor. By simulating the flow of the medication administration task, the relative position and spatial layout of the NS, medication room, patient room, and disposal room could influence the walking distance needed to perform medication administration tasks. Due to national differences, the nursing shortage and hospital bed shortage in China are more serious than in Western countries. The differences reflected in the design are that the nursing units are decentralized in the United States, while the nursing units in China are centralized. In contrast to the single patient room in the United States, a multiple patient room (usually two or three patients) design is implemented in Chinese nursing units. The main cultural difference is that China is a society of collectivism that values the harmony of society. This cultural value impacts the needs team members have for proximity and better visual communication within the team to strengthen their collective identity and for a staff area to avoid conflict in public (Cai et al., 2019; Cai & Zimring, 2019). The type of selected double-corridor nursing unit is unique to China and is conducive to team collaboration (Cai et al., 2019). If a physical barrier was installed between the NS and the doctor’s office, the effectiveness of the typology could be tempered.
The primary limitation of this study was that the results were only generated from medical double-corridor nursing units, and the results limit the broad generalizability to other types of nursing units. Another limitation was that only the medication administration task was simulated. In the nursing units observed, the medication administration task was the most time-consuming task. However, in other departments of nursing units, the medication administration task might not be the most important job for nurses. Future research is necessary in triangle, radial, and single-corridor nursing units and in other departments of nursing units such as surgical, gynecological, and intensive care units.
In addition, the study was not based on observations of actual medication procedures. In this study, one bedside nurse took care of several patients, and the main task for the nurses was medication administration. When a patient rang the bell for assistance, the nurses should finish the medical administration process as soon as possible. The frequency of deviation from the efficient route should be very low, and the effect of deviation on walking distance should also be low. Therefore, simulation was used in this study. However, in a real scenario, the actual walking distance might differ from that in the simulation, as nurses often combine tasks to allow maximum work efficiency, and unexpected events might happen during administration of the nursing care task. Moreover, Lu and Seo (2012) discovered that nurses might deviate from efficient routes in the ICU. Therefore, the results of the simulation should be interpreted carefully. In the future, more empirical studies are needed to examine the mechanism of the physical environments based on actual nursing care activities or behaviors demonstrating the differences in efficiency influenced by spatially related differences.
Implications for Practice
The partial glass wall of the medication room could not only limit outside interference but also provide visibility to the patients and maintain nurses’ perception of privacy.
There should be no physical barrier that blocks the visibility between the NS and the doctor’s office. High visibility enhances communication and reduces the time needed to locate team members.
Shortening corridor length and placing the WoW at the midpoint between the NS and the end of the corridor could increase visibility and proximity.
The relative position of the NS, medication room, and disposal room could influence the flow of medication administration tasks, and a geographically contiguous layout could enhance work efficiency.
Having decentralized disposal rooms on both sides of the NS and hand-washing stations conveniently accessible to the NS, medication room, and disposal room could improve work efficiency.
Supplemental Material
Supplemental Material, sj-pdf-1-her-10.1177_1937586719881443 - Impacts of Nursing Unit Design on Visibility and Proximity and Its Influences on Communication, Privacy, and Efficiency
Supplemental Material, sj-pdf-1-her-10.1177_1937586719881443 for Impacts of Nursing Unit Design on Visibility and Proximity and Its Influences on Communication, Privacy, and Efficiency by Xiaodong Xuan, Xixi Chen and Zongfei Li in HERD: Health Environments Research & Design Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Natural Science Foundation of China (No. 51508142).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.