
Abstract
Because of the complex anatomy of the foot, rarity of fractures of the foot, and subtle radiographic cues, foot injuries are commonly overlooked and mis/undiagnosed. This study seeks to investigate a patient population whose peritalar injuries, including fractures and dislocations, were missed on initial examination, in order to analyze factors of known, missed injuries and provide insight into methods for reducing the incidence of missed diagnoses. Surgical cases between January 1999 and May 2011 were queried and retrospectively reviewed to identify missed peritalar injuries. Of 1682 surgical cases reviewed, 27 patients with missed peritalar injury(ies), which were subsequently confirmed by imaging studies, were identified. Using the Orthopaedic Trauma Association classification, fracture and dislocation subtypes were classified. A medical record review was performed to assess demographic and surgical data elements. In this study population, 7 types of peritalar injuries (talus, calcaneal, navicular, and cuboid fractures as well as subtalar, calcaneocuboid, and talonavicular joint dislocations) were diagnosed in 27 patients. All patients required surgical intervention. Talus fractures were the most commonly missed injury. In patients with multiple peritalar injuries, there was a strong correlation between talus and navicular fractures (r = −0.60; P < .01) as well as a moderate correlation between talus fractures and calcaneocuboid dislocations (r = −0.46; P = .02). The presence of a calcaneal fracture significantly decreased the time to definitive diagnosis (P = .01). Male patients’ diagnoses were delayed an average of 324 days and females 105 days (P = .04). A moderate correlation was found between patient age at injury and time to diagnosis (r = −0.47; P = .04), with a decreased time to diagnosis as patient age increased. Significant factors were identified in this patient population, including patient sex and age, which may contribute to missed or delayed diagnosis in the clinical setting. Prompt and accurate diagnosis of peritalar injuries may improve long-term outcomes.
Introduction
Fractures of the foot have been reported as the most commonly missed extremity fracture. 1 Missed dislocations have also been reported. 2 Abundant literature exists both describing missed foot and ankle injuries (ie, fractures and dislocations)3,4 as well as presenting imaging techniques and tutorials for appropriately evaluating and diagnosing peritalar injuries.5-7 The reasons for missed foot injuries are multifactorial. The foot has complex 3-dimensional anatomy that may be difficult to fully assess on conventional 2-dimensional radiographs. Also, although the vast majority of foot and ankle injuries result in innocuous sprains, a small percentage of foot ankle injuries result in significant injuries with subtle radiographic findings. However, Wei et al reported in their study population that only 33% of initially missed fractures were attributable to radiographically imperceptible lesions. 1 Ultimately, the rarity of these injuries limits physician familiarity and increases the frequency of misdiagnosis.
Despite an overall decrease in motor vehicle fatalities, the number of motor vehicle accident victims with foot and ankle injuries has increased, which is likely due to automotive design improvements. These design improvements, such as the airbag, have improved survival rates but have not diminished the incidence of lower extremity injury. Firewall intrusion and propulsion of the foot against the brake pedal are typical high energy mechanisms leading to foot and ankle trauma. The midfoot often experiences the greatest force at impact leading to tarsometatarsal and midtarsal injuries. Richter et al described a biomechanical model inducing midfoot fractures, where peak pressures were measured in the ankle, talonavicular, and calcaneocuboid. 8 Similarly, in a vehicle braking simulation, Jeng et al showed the center of force was distributed between the forefoot (81%) and midfoot (19%) in normal subjects (ie, no ankle fusion). 9 Midfoot injuries may also result from twisting events, with a low energy mechanism. Although contemporary literature has emphasized the importance of Lisfranc injury, little information is available regarding the incidence and natural history of peritalar injury. The overall morbidity of polytraumatized victims with foot injury is greater than polytraumatized victims without foot injury, which underscores the importance of proper recognition of these injuries. 10 Kou et al defined several commonly missed peritalar injuries and described the radiographic clues to diagnosis to increase awareness in the medical community, discuss each injury, and provide physical examination and imaging methods for successful diagnosis. 11
The definition of peritalar may vary according to anatomic versus kinematic principles. For instance, Ledoux et al described the peritalar joint as the articulations between the talus and calcaneus as well as between the talus and navicular, which then form 2 joint capsules, the subtalar and talocalcaneonavicular joints. These joints are anatomically separate but function interdependently. Further, instead of defining the joint only by these capsules, the peritalar joint can instead be defined as the talocalcaneal joint (all articulations between talus and calcaneus) and talonavicular joint (some articulations between talus and navicular). 12 Huson advised that differentiation between anatomic/structural and kinematic/functional definitions was necessary to describe the joint. 13
This paper defined the peritalar joint by anatomic structures (ie, talus, navicular, calcaneus, cuboid) and 3 joint capsules (ie, subtalar, calcaneocuboid, talonavicular). 11 Peritalar injuries are defined as fractures or ligamentous disruption resulting in instability of 1 or more peritalar joints. The subtalar joint plays a key role in converting the foot from a mobile structure as it is in heel strike to a rigid structure as it is at toe off. The talonavicular and subtalar joint, as well as the tibiotalar joint, have been described as essential joints, meaning that the proper functioning is necessary for the normal function of the foot and ankle. Because of the effect on hindfoot kinematics, missed or delayed diagnosis of peritalar injuries often results in permanent functional impairment. This study defines and analyzes a patient population diagnosed with peritalar injuries, excluding the tibiotalar joint, which were initially missed, in order to evaluate the factors leading to delayed diagnoses and additional methods for improving diagnoses. The purpose of this study is to determine the types of peritalar injuries most commonly missed, define diagnostic parameters when encountering these injuries in the acute setting, and increase awareness among orthopaedic surgeons, which may decrease the incidence of misdiagnosis.
Methods
Following Institutional Review Board approval, the medical record database maintained by our institution was queried for delayed or missed peritalar injuries using 14 International Classification of Diseases codes (ICD-9-CM; World Health Organization, Geneva, Switzerland) for operative procedures (Table 1).
List of ICD-9-CM Codes for Query Input.
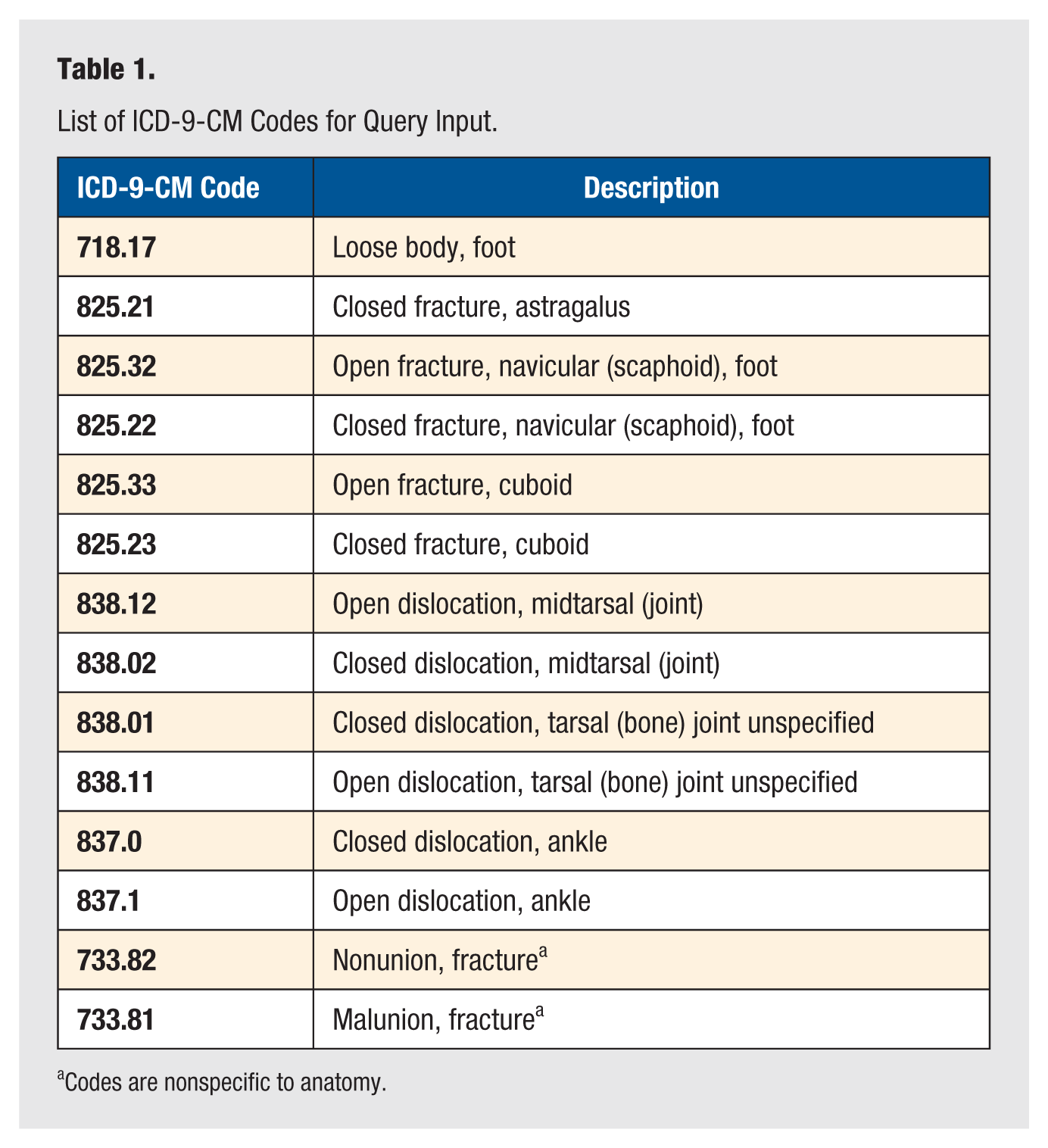
Codes are nonspecific to anatomy.
All coded cases were searched in our institution’s surgical database from January 1999 to May 2011. Calcaneus fractures, while not directly queried, were captured through the malunion and nonunion codes. Through query design, results were restricted to cases of the 2 attending orthopaedic foot and ankle surgeons and 4 attending orthopaedic trauma surgeons practicing at our institution. The query returned 1682 potential cases of missed peritalar injuries that required surgical intervention, as access was only available to surgical cases. Chart reviews were performed on each case by research personnel to establish cases of missed or delayed diagnosis of peritalar injury (defined as a case where a patient experienced a delay from initial examination and/or treatment of foot/ankle injury to definitive diagnosis of peritalar injury) through dictated reports and imaging documentation for inclusion in the study.
Patients who were skeletally immature were excluded. Additionally, patients who received nonoperative management were excluded, as only surgical cases were available for query by our institution’s database. ICD-9 codes 733.81 and 733.82 are nonspecific to foot and ankle, so the body site was first confirmed before review was performed.
Of the 1682 cases returned by the query, 27 patients were confirmed cases of missed/delayed diagnosis of peritalar injury and included in the study population. Medical records, radiographs, bone, and computed tomography (CT) scans, if available, from the confirmed cases were retrospectively reviewed and analyzed.
For confirmed cases, multiple data points were collected, including patient body mass index (BMI), patient sex, patient age at injury, patient age at definitive diagnosis, time to definitive diagnosis (number of days from missed diagnosis at initial examination to definitive diagnosis), ICD-9 code, formal definitive diagnosis, missed injury(ies), associated injuries (ie, peritalar and nonperitalar; missed and diagnosed), mechanism of injury, reason injury missed, physical examination findings at definitive diagnosis, technique (eg, imaging) used at the time of definitive diagnosis to confirm injury diagnosis, and operative fixation method. For missed injuries, the Orthopaedic Trauma Association (OTA) fracture classification was also defined.
Statistical analysis was performed to identify significant factors and relationships between factors (SigmaPlot 11.0, Systat Software, Inc, Chicago, Illinois). Analysis of variance models were used to assess relationships between patient factors, injuries, mechanisms of injury, and operative management. The relationships between occurrence of injury type and time to definitive diagnosis as well as between occurrence of missed diagnosis in cases of isolated injury versus polytrauma were analyzed using a Mann-Whitney rank sum model. Using a Pearson product moment model, patient factors (ie, patient age at injury, patient age at definitive diagnosis, patient sex, BMI) and time to definitive diagnosis were correlated. As many patients in the population encountered multiple peritalar injuries, a Pearson product moment analysis was also performed to determine any relationship(s) between particular combination(s) of injuries. All analyses used α ≤ 0.05 to determine significance. Correlation coefficients of 0.20 to 0.40, 0.40 to 0.60, 0.60 to 0.80, and 0.80 to 1.00 were considered weak, moderate, strong, and very strong, respectively.14,15
Results
Review of Medical Records
The patient population diagnosed with a peritalar injury, which was missed at initial examination, included 16 males and 11 females. The average patient age at injury and definitive diagnosis were 37.3 years (range, 13.8-67.1) and 38.4 years (range, 15.4-67.2), respectively, with an average delay in diagnosis of 217 days (range, 12-571). Patient BMI averaged 30.3 (range, 21.0-42.4).
The mechanisms of injury included 6 high and 17 low energy trauma episodes as well as 4 cases of unknown mechanism. The injury origins included motor vehicle crash (n = 6), twisting and crushing during athletic activities (n = 7), falls (n = 3), and twisting/misstep during activities of daily living (n = 7). Within the 27-patient population, there were a total of 42 injuries: 17 talus fractures, 8 calcaneal fractures, 7 navicular fractures, 3 cuboid fractures, and 7 dislocations (3 subtalar, 3 calcaneocuboid, 1 talonavicular). OTA classification is listed for each patient in Table 2.
Fracture and Dislocation Subtypes According to Orthopaedic Trauma Association Classification System.
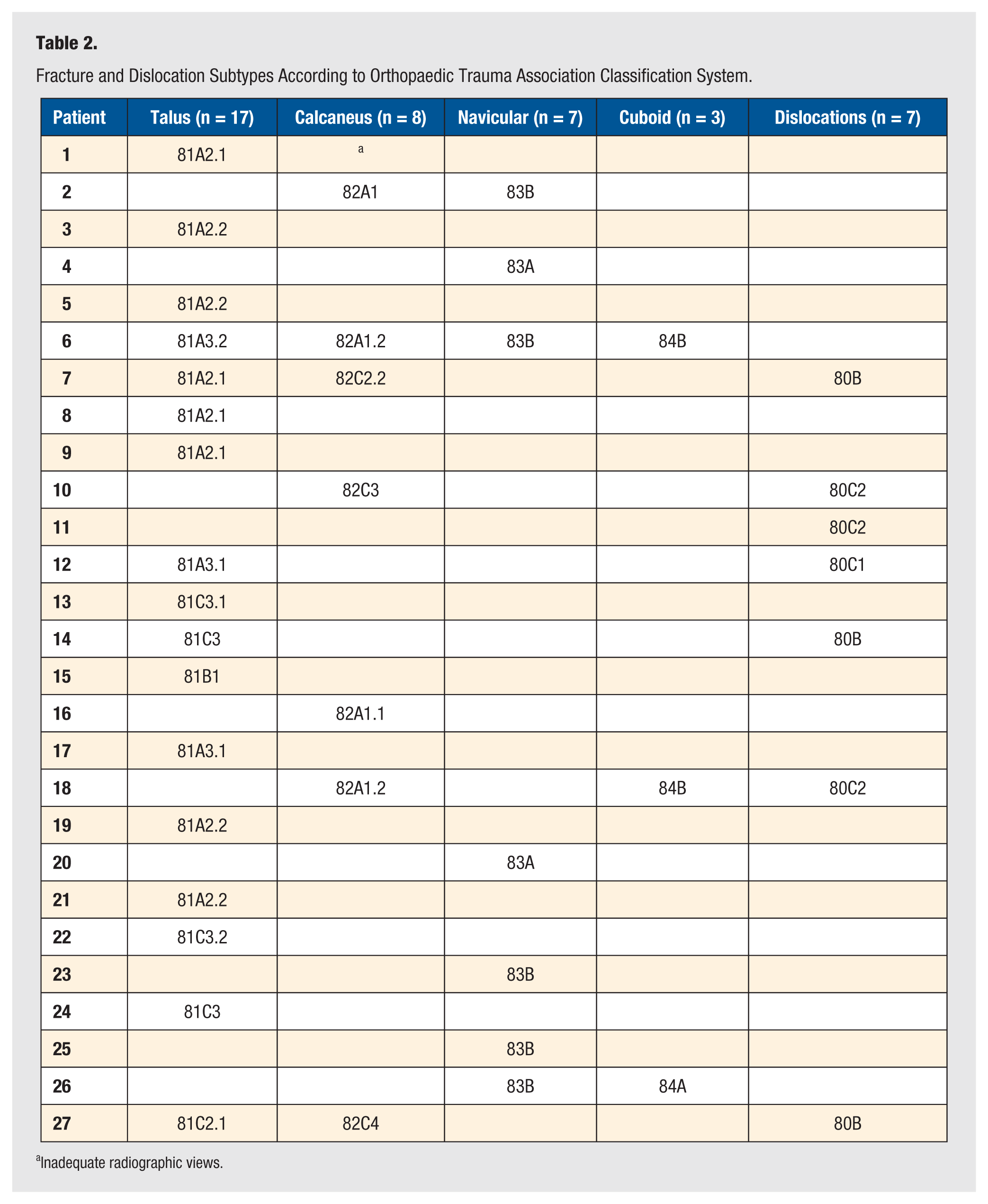
Inadequate radiographic views.
Associated injuries included fibula fracture (n = 3), talus fracture (n = 1), calcaneal fracture (n = 1), compressive neuropathy of deep peroneal nerve (n = 1), lateral ankle ligament tear (n = 1), posterior tibial tendon tear (n = 1), tibia fracture (n = 1), lumbar compression fracture (n = 1), humerus fracture (n = 1), closed head injury (n = 1), and fifth metatarsal tuberosity fracture (n = 1). All associated injuries were accurately diagnosed at the initial examination, except for the tibia fracture and posterior tibial tendon tear. In total, there were 7 polytrauma (peritalar injury with additional nonperitalar injury) and 20 isolated injury (peritalar injury/injuries only) events. Thus, our study population experienced significantly greater isolated peritalar injury than polytrauma events (P < .001). Within the study population of peritalar injuries, there were 10 cases of single peritalar injury and 17 cases of multiple peritalar injuries, which was not statistically significant.
A review of available records confirmed 7 patients received foot (n = 6) or foot and ankle (n = 1) plain films at the time of initial presentation, and these films were provided to the diagnosing orthopaedic surgeons’ offices. Most patients stated that films were obtained, but we were unable to confirm these reports due to 77% of patients initially presenting at outside hospitals or clinics. On average, patients presented at an average of 2.6 known locations (range, 2-4) before being definitively diagnosed. These locations included emergency centers (EC), urgent care (UC) centers, primary care physician (PCP) offices, and orthopaedic surgeon private offices. Patients generally presented to orthopaedic surgeons specializing in sports medicine or general surgery, perhaps due to initial diagnoses of “sprain” or after a period of “persistent pain,” following an EC, UC, or PCP visit. Besides “sprain,” other diagnoses after initial presentation were: “normal” presentation; osteoarthritis; os trigonum or unusual ossification of joint; ossicle, but no fracture; and lucency. Prior to referral to the diagnosing orthopaedic surgeons’ offices, only 3 patients received advanced imaging studies, including magnetic resonance imaging (MRI) (n = 2) and CT (n = 1).
Twenty-five of the patients were definitively diagnosed and managed by 2 orthopaedic foot and ankle surgeons and 2 by 1 orthopaedic traumatologist. Upon examination by the 3 staff surgeons, the missed injuries were confirmed using radiographs at multiple views (ie, lateral, anteroposterior, oblique) (n = 21), CT (n = 21), 2 with 3-dimensional reconstruction, and/or bone scan (n = 1) (Figure 1).
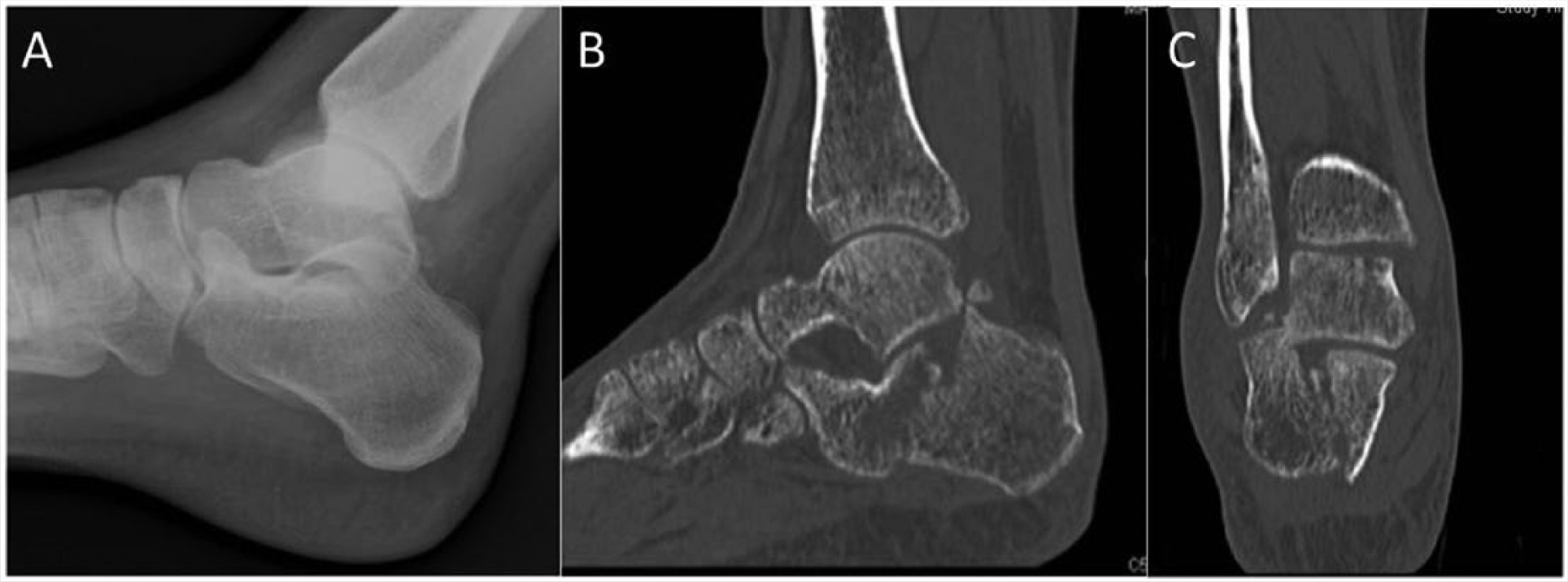
Lateral radiograph and CT of a calcaneal fracture dislocation following a low energy injury. Initial radiographs were interpreted as normal and the patient was allowed to weightbear as tolerated. (A) Lateral radiograph depicts a double density where the posterior facet articular surface is superimposed on the body of the talus. (B, C) CT obtained several weeks after injury confirms the fracture dislocation.
All injuries presented in this study were operatively managed through several techniques, including open reduction internal fixation (ORIF) with plate and/or screw(s) (n = 12), subtalar fusion (n = 7), excision of fragment (n = 4), and calcaneocuboid fusion (n = 1). Surgical records of 3 patients were inaccessible.
Analysis of Factors
Patient Ages at Injury and Definitive Diagnosis
Patient ages at injury and definitive diagnosis were compared with each injury type to assess any associations between age and injury type; however, there were no significant results.
Patient Body Mass Index
Each injury type was also compared with patient BMI and no significant relationships were found.
Patient Sex
The time to definitive diagnosis was compared between female and male patients. There was a significant relationship between time to definitive diagnosis and patient sex, with male patients’ definitive diagnoses delayed by an average of 219 days more than female patients’ (P = .04). Male patients experienced an average delay of 324 days (standard deviation, 258 days) until definitive diagnosis, while female patients remained “delayed in diagnosis” for 105 days (standard deviation, 139 days) (Figure 2).
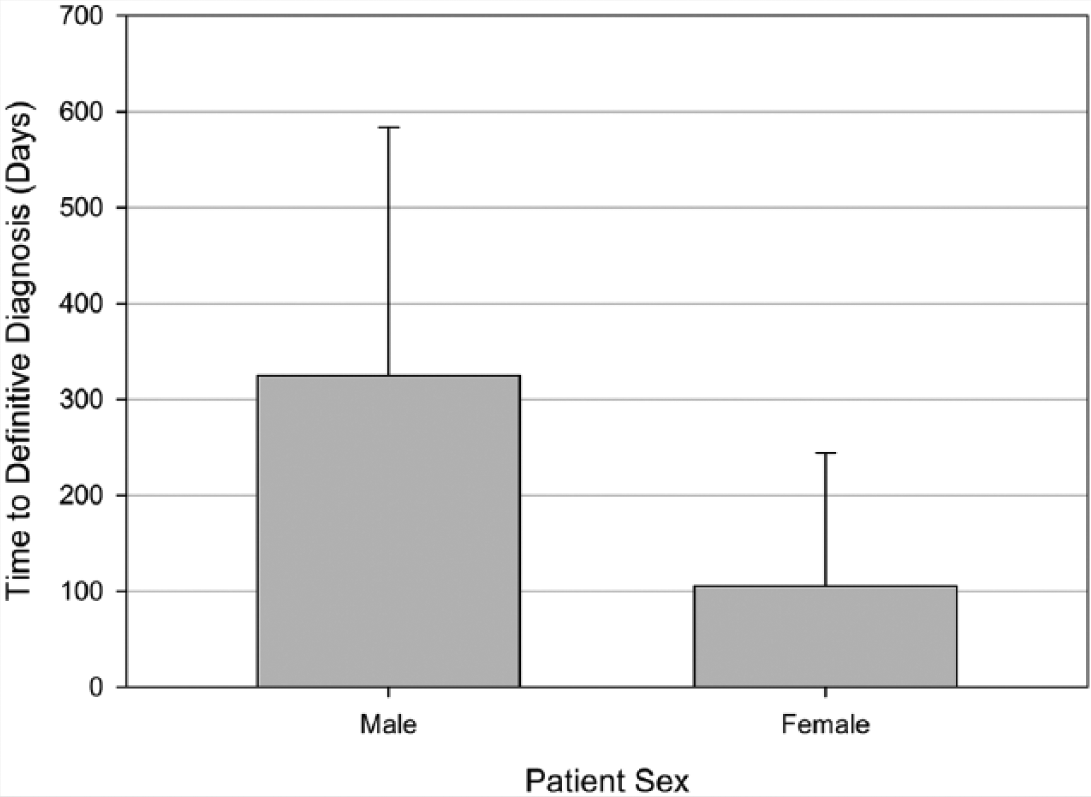
Average time to definitive diagnosis of missed peritalar injury is significantly greater for male patients than female patients.
Mechanism of Injury
Each injury was classified as a high or low energy mechanism event. The average delays in definitive diagnosis resulting from low, high, and unknown mechanisms averaged 214, 268, and 177 days, respectively. Average time to definitive diagnosis of missed peritalar injury was greatest for patients experiencing a high energy mechanism event, followed by low energy injury processes; however, there was no significant relationship between mechanism of injury and time to definitive diagnosis. Within each injury mechanism cohort, the frequency of peritalar injuries was plotted (Figure 3).
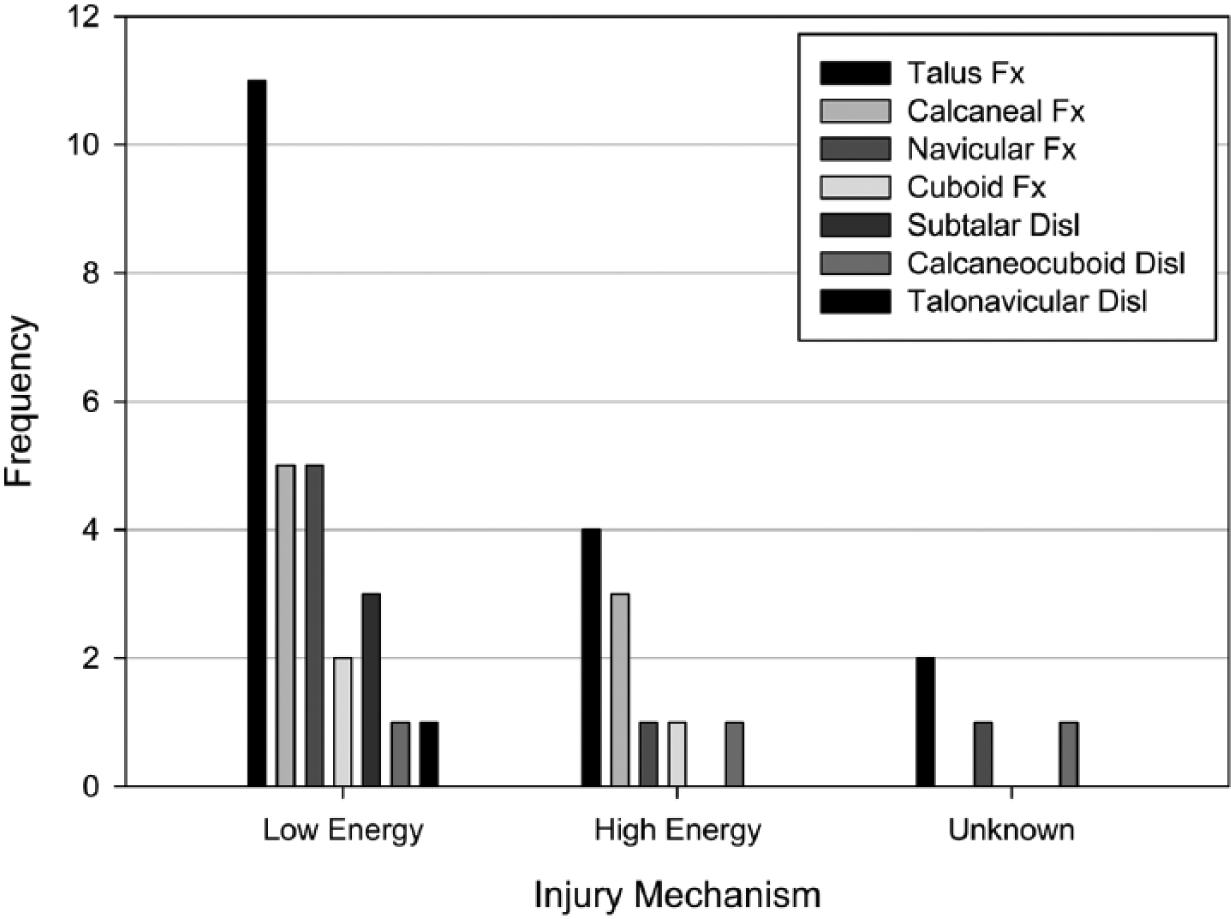
Frequency plot showing number of each injury resulting from low, high, and unknown energy mechanisms.
Talus fractures were the most common missed injury in all mechanism categories, followed by calcaneal, navicular, and cuboid fractures, respectively, in both the low and high energy groups. Talus, calcaneal, and navicular fractures comprised 75% of the peritalar injuries missed after a low energy event. Similarly, 70% of all missed peritalar injuries in the high energy cohort were talus and calcaneal fractures. Cuboid fractures and dislocations, with the exception of subtalar dislocations, were the least common injuries.
Operative Management
When comparing patients who were operatively managed with fusion versus ORIF, fusion patients had an average time to definitive diagnosis of 413 days (standard deviation, 177 days), while patients managed with ORIF had an average delay in diagnosis of 110 days (standard deviation, 131 days) (P < .01). Additionally, the fusion group included 4 high, 2 low, and 2 unknown energy mechanism events, while the ORIF patients experienced 10 low and 2 unknown energy mechanism occurrences leading to injury (P < .01). Patient factors and injury type were not significant between the treatment cohorts.
Correlation of Factors
A Pearson product moment correlation of patient sex, BMI, ages at definitive diagnosis and injury, mechanism of injury, and time to definitive diagnosis was performed. Patient sex and time to definitive diagnosis (delay) was moderately correlated (r = −0.51; P = .02), analogous to the ANOVA test showing male patients experienced longer delays in diagnosis than female patients. In addition, the correlation between patient age at injury and time to definitive diagnosis was also moderate (r = −0.47; P = .04). This correlation indicated that younger patients experience longer delays in diagnosis (Figure 4). Expectedly, patient age at injury and diagnosis are strongly correlated (r = 0.99; P < .01), as the pair of variables increase together.
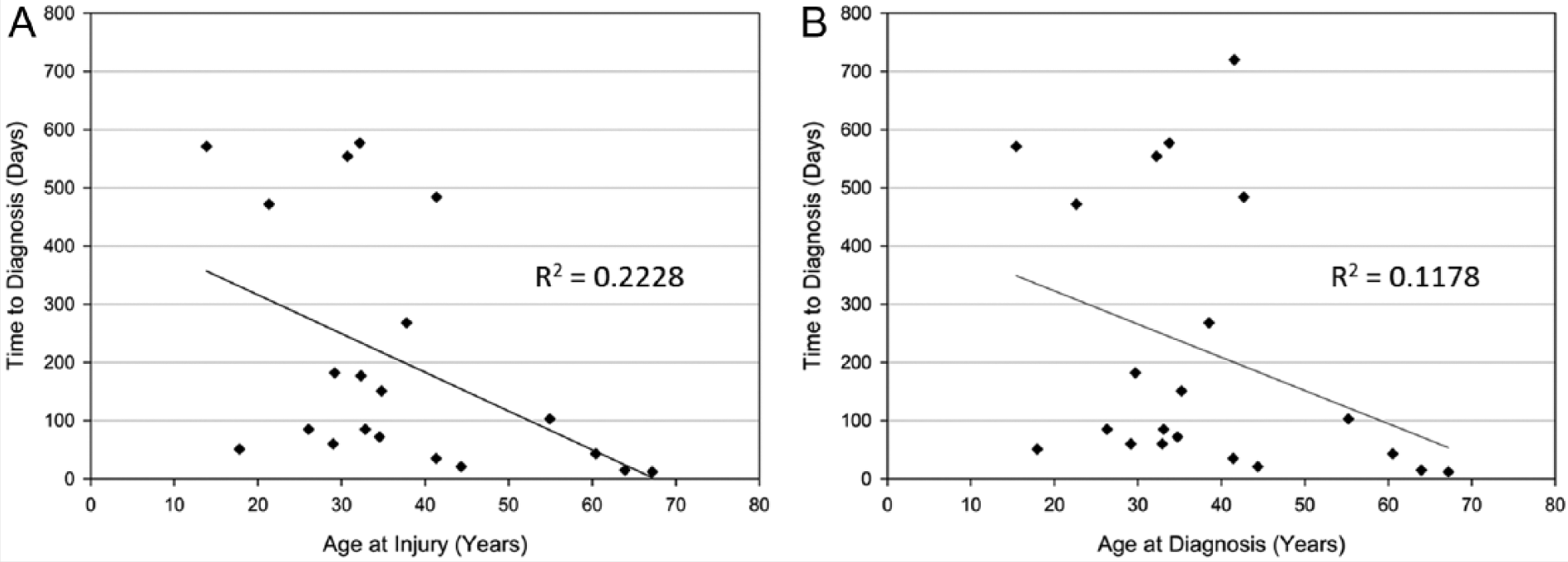
The relationship between patient ages at (A) injury and (B) diagnosis and time to definitive diagnosis of missed peritalar injury are plotted.
The 7 types of injuries defined in our patient population were analyzed using Mann-Whitney rank sum tests to interpret any relationship between type of injury and time to definitive diagnosis, and, specifically, if the presence of one type of injury affected the time period of delayed diagnosis. One relationship was significant in this analysis. The presence of a calcaneal fracture decreases the amount of time a patient was delayed between initial examination and definitive diagnosis (P = .01).
Ten of the 27 patients (37%) were diagnosed with multiple peritalar injuries. A Pearson product moment analysis was performed to evaluate if relationships existed between certain injuries or time to definitive diagnosis. In this study population, the relationship between talus and navicular fractures (r = −0.60; P < .01) was strongly correlated; and, as demonstrated by the negative correlation statistic, these injuries were less likely to occur concurrently, with only 1 case in the study population exhibiting both fractures. Talus fractures and calcaneocuboid dislocations (r = −0.46; P = .02) showed a moderate correlation and were also negatively correlated. This combination did not occur in this study population.
Discussion
Previous reviews of missed injuries and more specifically missed foot and ankle injuries, have begun to define the frequency and scope to which peritalar injuries are missed. 1 , 7 , 11 However, to date, the frequency and factors of missed peritalar injuries (ie, fractures, dislocations, and ligamentous injuries that occur in and/or around the peritalar joints) have not been analyzed. Through a query using 14 ICD-9 codes, we identified 27 cases of missed or delayed diagnosis of peritalar injuries, ultimately treated with operative management, over an 11-year period at our institution.
Several findings attained through our analysis may be practically applied in the clinical setting. First, 79% of our patient population was less than 45 years of age at the time of injury, and these younger patients averaged significantly longer times to definitive diagnosis. Male patients experienced significantly greater delays, on average 219 additional days, in time to definitive diagnosis than female patients. Patient BMI had no effect on times to definitive diagnosis. Patients with high energy mechanism injuries averaged longer times to definitive diagnosis than injuries sustained during low energy events, however, there was no significant relationship.
The most commonly missed injuries identified were fractures of the talus, approximately 40% of the total number of injuries in this population. The most common subtypes were lateral process (n = 4), posterior process (n = 4), head (n = 3) and body, with ankle and subtalar joint involvement (n = 4). The high incidence of missed talus fractures in this study population is, at least in part, due to the study design of querying injury of the talus. We also found talus fractures and calcaneocuboid dislocations were significantly negatively, moderately correlated, with no combinatory cases in our population. This finding has uncertain clinical significance and may be attributed to the difference in the mechanism of injury for these 2 entities.
Missed diagnoses of talus fractures may be due to many factors. First, the shape of the talus is complex in that its 3-dimensional anatomy is poorly identified on plain radiographs. Often, conventional radiographs do not clearly identify the bony landmarks of the talus, or more importantly, fracture lines may be subtle and hidden by other bony projections. Lateral talar process (LTP) fractures comprise 24% of all fractures to the talar body but make up less than 1% of all ankle injuries. 16 Multiple studies describe LTP fractures initially misdiagnosed as ankle sprains, due to characteristic similarities to an anterior talofibular ligament sprain.11,16-19 McCrory et al reported a 15% rate of misdiagnosis for LTP. 16 Kou et al and Noble et al recommended ankle mortise views and CT to definitively diagnose this injury and assess intra-articular involvement and comminution.11,18 Posterior talar process (PTP) fractures, which present with tenderness over the posterolateral ankle with pain during forced plantar flexion and flexor halluces longus tendon motion, are commonly misdiagnosed as os trigonum. Kou et al advocated CT scans, versus radiographs, as PTP fractures are difficult to distinguish on plain films, due to adjacent anatomy and possibility of small fragments. 11 Talar head fractures, which comprise less than 10% of all talus fractures, 20 present at examination with tenderness over the talonavicular joint with ecchymosis. Radiographically, a Canale view may increase perceptibility; CT can further assist with diagnosis. 11
Talus fractures and navicular fractures, in our study population, had a negative correlation, indicating that the presence of 1 injury determined the absence of the associated injury. This relationship was the most significant correlation in this study population, with only 1 talus-navicular fracture occurrence (injury also included calcaneal and cuboid fractures; patient 6). Radiographically, a double-density sign on the lateral view or subtle dorsal subluxation, which may not be apparent in the acute period, may be the only radiographic clue seen on plain films. 11
In our population, 1 injury type, calcaneal fractures, was significantly related to time to definitive diagnosis. The presence of a calcaneal fracture was linked to a significantly reduced time to definitive diagnosis, which may indicate that the overall higher incidence of calcaneal fractures in the general population allows clinicians more familiarity with this injury as compared to the other injuries in the series; however, 8 calcaneal fractures were still initially missed in this population. Anterior process fractures were the most common subtype (n = 4); 3 articular fractures involving the posterior facet were also recorded (specifically, one 2-part, one 3-part, and one 4-part). Two-part fractures have been identified as a rare calcaneal fracture subtype, which is also difficult to diagnose radiographically. 21 Kou et al describe recognizing a double-density sign on the lateral view of the ankle, which reveals the displaced lateral portion of the posterior facet beneath the fibula. 11 On the mortise view, the lateral portion of the posterior facet impacts the fibula and can cause a fibular fracture that can be a distracting injury.
Although not shown to be significant in our series, this example of a distracting injury occurs as the calcaneal tuberosity dislocates, impacting the distal end of the fibula, often resulting in fracture that is more clearly visible than the calcaneal fracture itself.11,22 Our study population included 2 missed calcaneal fractures with associated fibula fractures, which were diagnosed on initial presentation.
Cuboid fractures were the least common fracture in our study population, which is consistent with existing literature describing these fractures as rare, typically capsular avulsion injuries. 23
Available imaging modalities appear to be adequate in accurately diagnosing peritalar injuries at the time of initial examination. Radiographs were ordered at the time of initial presentation in most cases; however, appropriate radiographs (ie, specific views) and accurate interpretation are essential to diagnose these rare injuries. Radiographs were used, at our institution, to definitively diagnose the injuries in approximately 77% of the cases; however, because many of the injuries are subtle on plain films, CT is often indicated for confirmation of these imperceptible, yet complex, fractures. In this study population, CT scans were eventually obtained in 21 of 27 cases. In addition to fractures, dislocations may also be identified by CT.11,24
There were several limitations of our study. Because our institution’s database was limited to operative procedure codes, the missed peritalar injuries treated nonoperatively were not captured. Likewise, we have not captured patients who were not coded with 1 of the 14 queried ICD-9 codes. Due to these limitations, we cannot define the true incidence of missed peritalar injuries at our institution. Examination of this patient population was an attempt to analyze a cross-section of the patients who were diagnosed with a missed peritalar injury requiring surgery as a means for assessing common factors associated with missed peritalar injuries. Effectively, because this cohort of patients ultimately required surgery, these injuries are likely of the greatest clinical significance and morbidity. Additionally, data and imaging studies, from visits prior to presentation at diagnosing orthopaedic surgeons’ offices, were difficult to obtain and/or confirm.
We presented an analysis of rare, yet commonly missed peritalar injuries. This patient population showed that age at injury, patient sex (ie, male patients), and specific combinations of peritalar injuries are significantly correlated to increased times to definitive diagnosis. When clinical features, such as pain and/or swelling in the peritalar region and/or inability to bear weight persist, and candidate causes are excluded, additional imaging may be useful differential diagnostic tools to confirm or exclude peritalar injuries. Radiographic features, including joint space asymmetry and subtle subluxation, can distinguish peritalar injury, while advanced imaging modalities, such as CT, can confirm and assess characteristics of peritalar injury. An awareness of the factors and interactions in this study population may contribute to the surgeons’ algorithm for assessing peritalar injuries, thereby reducing rates of missed diagnoses.
Footnotes
Acknowledgements
This paper is dedicated in memory of Harry N. Herkowitz, MD.
Authors’ Note
This study did not receive any funding from an outside entity. The authors have no conflicts of interest to report regarding the research presented in this manuscript.