
Abstract
Steroid-induced avascular necrosis (AVN) of the lower extremity is a destructive process of the bone found in patients who have been treated with these medications for a variety of medical conditions. There are several proposed etiologies for development of this condition, however much debate still remains for the exact pathophysiology. The main clinical characteristics include edema, arthralgias, and restricted joint range of motion. Diagnostic imaging is a key aspect in the analysis of this pathologic process. When steroid-induced AVN affects multiple bones, this atypical presentation is difficult to treat due to its diffuse nature, therefore surgical options are limited. In these cases, conservative therapy is targeted toward pain relief and preserving joint range of motion. This review aims to provide an overview on the presentation of steroid-induced AVN in the foot and ankle, outline the pathophysiology of the process, and describe a variety of both conservative and surgical treatment options. A case study is provided to showcase a patient presentation of diffuse steroid-induced AVN of the foot and ankle and their course of treatment.
“Many cases are misdiagnosed as the initial symptoms present as generalized tenderness and arthralgia without radiographic findings.
Avascular necrosis (AVN) of bone induced by steroid use was first described in 1957 and is one of the most debilitating complications of steroid treatment. 1 It is found in patients with medical requirements for immunosuppression, such as those with systemic lupus erythematosus (SLE), asthma, glomerulonephritis, peripheral neuritis, pemphigus, Guillain-Barre syndrome, hematological diseases, prior organ transplantation, and those on combined chemotherapy.1,2 Progressive pain and reduced or restricted joint motion are common symptoms and can precede radiographic changes. By the time this bone destruction does present on imaging, joint surfaces have often collapsed, which results in severe dysfunction and disability.
There is much in the literature showcasing the effects of steroid-induced AVN commonly affecting the femoral heads, humerus, and proximal tibia; however, there are few reports of this process in the bones and joints of the foot and ankle. 1 Many cases are misdiagnosed as the initial symptoms present as generalized tenderness and arthralgia without radiographic findings. It is not until advanced imaging is obtained, demonstrating multiple sites of diffuse bone and joint necrosis, that a definitive diagnosis is made. 3 It can be difficult to predict the continued course and involvement, especially if the patient is required to stay on long-term steroids for their systemic disease. Due to underreporting in the literature, there are limited treatment guidelines for how to manage and support this progressive and debilitating disease. The aim of this study is to review the current literature regarding the presentation, etiology, and treatment options for steroid-induced AVN in the foot and ankle, as well as to present a case of this extensive bone destruction in a patient on chronic steroid treatment.
Case Presentation
A 41-year-old woman with a past medical history of SLE of 6 years with class 5 lupus nephritis, chronic kidney disease IV (CKD), and pulmonary vasculitis was referred to the senior author (CZ) for bilateral foot and ankle pain, worse on the left. Of note, the patient had been taking prednisone 10 mg daily and hydroxychloroquine 400 mg daily for 6 years for treatment of her SLE. The onset of symptoms began 6 months prior to this visit, where she was originally diagnosed and treated for an ankle sprain from suspected trauma and given a controlled ankle motion (CAM) boot for support. The pain persisted and progressively worsened, with new pain developing at the contralateral ankle. She also endorsed dull joint pain to her knees, elbows, and shoulders without noticeable swelling or skin changes. On physical exam, the patient had generalized global tenderness to the foot and ankle with pain throughout ankle joint and hindfoot range of motion. Radiographs were rendered inconclusive as they had been negative for any osseous or soft tissue changes (Figure 1). A magnetic resonance imaging (MRI) of the left foot and ankle was obtained demonstrating extensive AVN within the distal tibia, as well as the tarsal bones (Figures 2 and 3). Given her diffuse arthralgias to multiple joints, the patient was not an optimal surgical candidate. The patient was referred to physical therapy focusing on low resistance activities to preserve range of motion and manage symptoms. She was provided with a lace up ankle brace and eventually a patellar tendon brace to manage pain during gait. She continued close follow-up with her rheumatologist who discontinued steroid use following the diagnosis of AVN and supplemented the patient with rituximab infusions. She showed marked improvement after conservative treatment without any additional medication modifications, with continued pain relief at 13 months from her initial presentation.
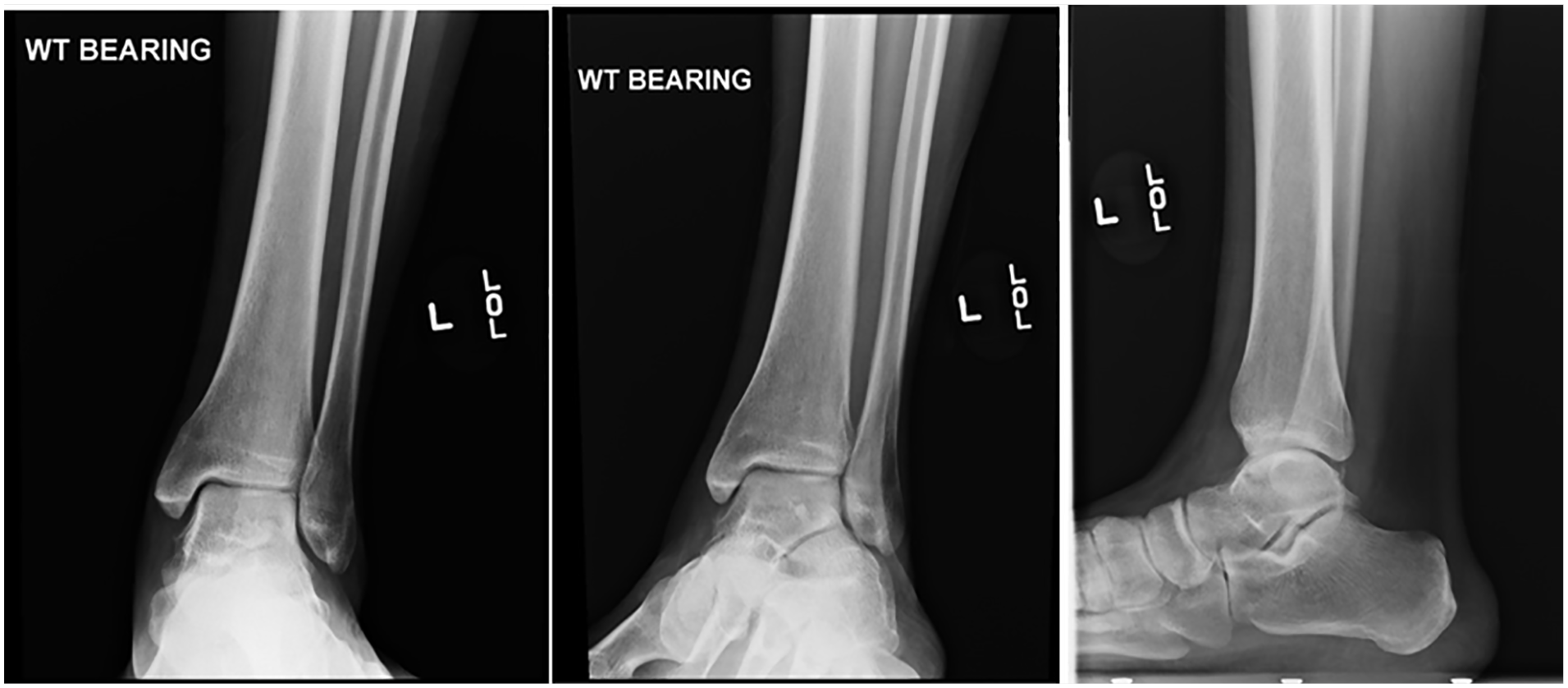
(A) Anteroposterior, (B) oblique, and (C) lateral standard weightbearing ankle radiographs did not demonstrate any soft tissue or osseous abnormalities.
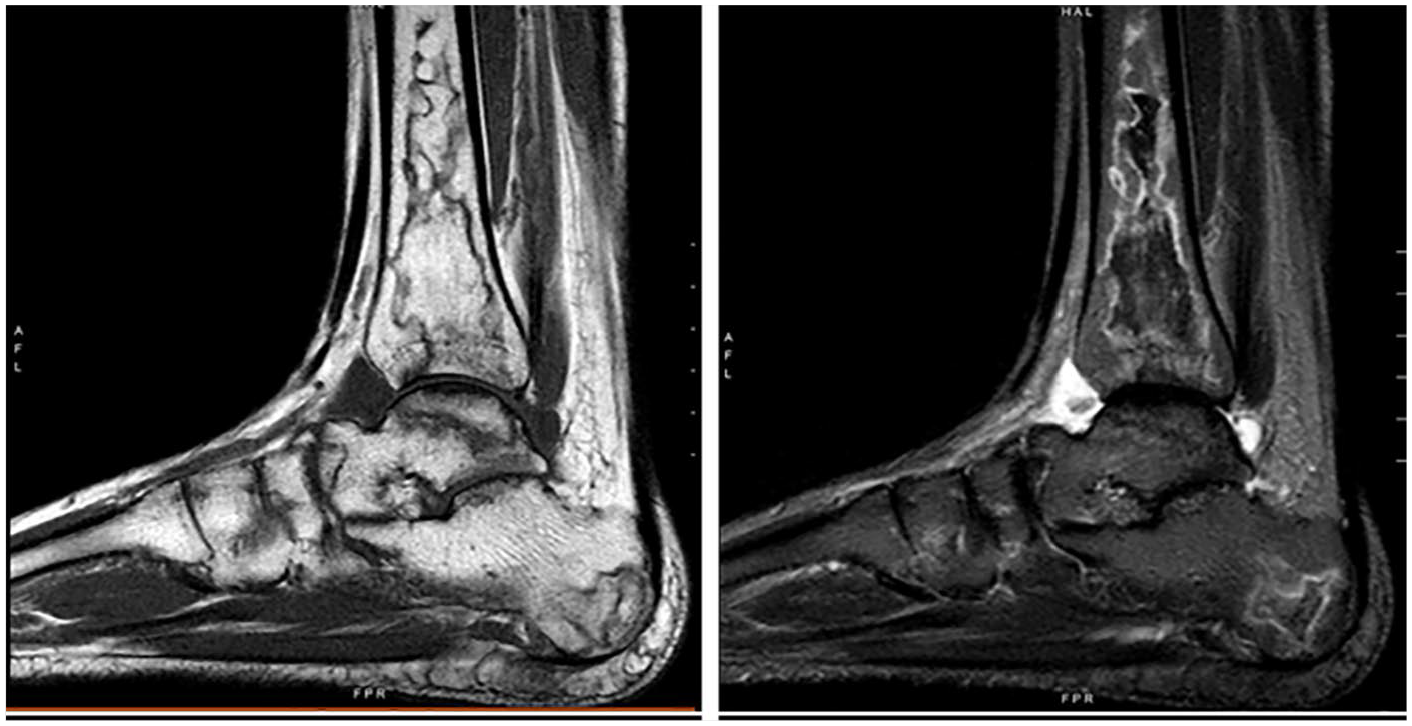
(A) T1-weighted magnetic resonance imaging (MRI) of the ankle, sagittal view. Decreased signal present to tibia, calcaneus, talus, and bones of the midfoot. (B) T2-weighted MRI of ankle, sagittal view. Marked sclerosis and increased signal present in the distal tibia and calcaneus, talo navicular articulation, within the medial cuneiform, and the first metatarsal diaphysis.
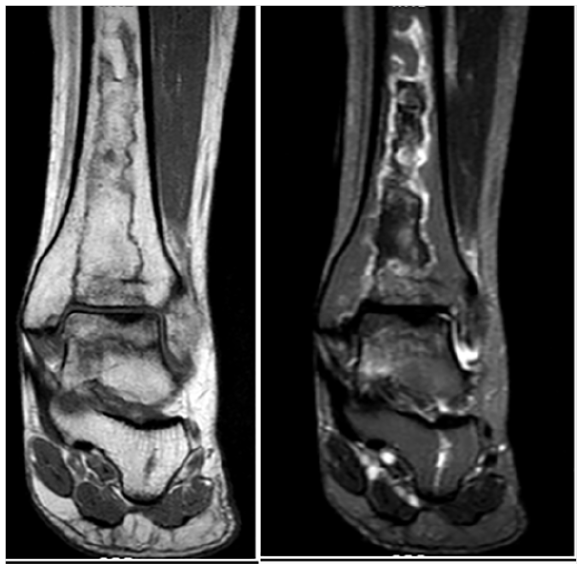
(A) T1-weighted magnetic resonance imaging (MRI) of the ankle, coronal view. Extensive decrease in signal to distal tibia, talus, and calcaneus. (B) T2-weighted MRI of the ankle, coronal view. Extensive signal increase in the calcaneus extending to the posterior subtalar joint, talar body, and within the distal tibial diaphysis.
Steroid-Induced Avascular Necrosis Presentation
Steroid-induced AVN of the bones of the foot and ankle presents with signs and symptoms of diffuse edema with associated tenderness to the affected sites. It often starts as pain with weight bearing in the affected extremity, which is improved with rest, but can eventually lead to an inability to bear weight secondary to severe joint pain. Active range of motion of the affected joints can be limited in more severe cases. Once symptoms increase in severity and duration, they are usually accompanied by radiographic changes.
This type of AVN can occur in any weight bearing bone or joint. It is well documented that the femoral head is the most commonly affected bony location for this condition; however, some other areas of the skeleton that are affected include the humeral head, femoral condyles, tibial plateau, talus, and capitulum of the elbow. 2 Patients who present with an initial site of bony involvement have a high risk of developing additional sites of necrosis. A study by Hungerford and Zizic 4 revealed that 86% of patients with steroid-induced AVN had multi-bone or joint involvement with an average of three sites per patient.
Steroid-induced AVN is associated with a number of medical conditions, including SLE, leukemia, severe acute respiratory syndrome (SARS), malignant tumors, renal failure, inflammatory bowel disease, sickle cell disease, previous organ transplantation, and dermatologic associated diseases such as dermatomyositis. 5 This is likely due to the fact that many of these conditions have an autoimmune-related component and patients are actively taking these steroids for immunosuppression. According to various studies, there is a higher incidence of AVN seen in the SLE population than the non-SLE population, with numbers ranging anywhere from 4% to 40% of patients.2,6,7 Up to 90% of lupus patients with AVN have more than 2 bones or joints involved. 2 It is hypothesized that the diffuse vasculitis of SLE may affect blood vessels in bone, resulting in ischemia and osteonecrosis. 8 Among the non-SLE group, polymyositis and dermatomyositis had the highest incidence of steroid-induced AVN. 6 It has also been reported that the risk of developing this type of AVN increases as the age of initial steroid administration increases, where pediatric patients have a lower risk of developing bone necrosis if started on steroids at an earlier age. 9 Females tend to have an increased risk of developing this AVN compared to males; however, this may be due to the fact that they are more frequently affected by autoimmune disease.10,11
Diagnosis of the condition can initially be suspected by relating clinical exam findings and symptoms with current medical history including steroid use. Differential diagnoses can include: osteoarthritis, osteomyelitis, neoplastic bone conditions, osteoporosis, adjacent soft tissue trauma, inflammatory synovitis, and complex regional pain syndrome. 12 Advanced imaging such as MRI or computed tomography (CT) scans are extremely useful in further evaluating bony changes and leads to a better understanding of what specific regions are affected. 3 Bone biopsy is a less common method of diagnosis, mainly obtained through operative intervention, which allows for histological examination of the affected bone to reveal destructive changes such as empty lacunae, necrosis, and loss of osteocytes.13,14 Bone biopsy can be useful for confirming AVN; however, changes in imaging correlated to clinical suspicion remains to be a reliable and less invasive method of diagnosis.
Pathophysiology
The exact etiology of steroid-induced AVN in bone remains controversial; however, there are a number of hypotheses for this bony process. The first is related to the increase in formation of fatty cells with the use of steroids. These medications cause altered lipid metabolism, leading to an elevation of serum triglycerides, phospholipids, and cholesterol in the body, which put patients in an overall state of hyperlipidemia. 15 This leads to the formation of a fatty liver with the loss of subcutaneous fat, thus increasing liver size. When this hepatic fat is released to form serum lipids, there is subsequent fatty emboli, which can lodge in the microvasculature of subchondral bone, resulting in bony necrosis from arterial occlusion. 2 There has also been evidence of fat cell hypertrophy within bone after steroid use where intramedullary fat cells enlarge causing a compartment syndrome effect that leads to cell death. 16 A similar destructive process with the use of steroids has demonstrated an increase in intraosseous pressure of the bone marrow that can also lead to cell death. 2 A second theory for steroid-induced AVN involves the mechanism that these drugs create a hypercoagulable state in the body. Vasculitis provoked by cortisone use and underlying autoimmune disease can also lead to intravascular thrombus formation, causing a blockage of arteries as well as venous outflow obstruction, which then leads to bony death. 17 The last hypothesis is that steroids have a negative effect on bone cells directly. There is evidence to indicate they impede osteogenesis, leading to microfractures and eventual sequestering of the involved bone area.10,18 Steroids may also induce osteocyte apoptosis, causing accumulation of cell products in bone and disruption of the osteocyte-lacunar-canicular system with eventual bony collapse. 19
Daily corticosteroid dose, dose per weight, cumulative dose, and pulse dose are all levels to assess when suspicious of a steroid-induced AVN. 5 The initiation of this process depends on the body’s response to a high dose of corticosteroid therapy with subsequent decrease in bone mineral density. As the steroid dosage increases, as seen with dosages over 40 mg/d, patients have an significantly increased risk of developing osteonecrosis. 6 A study by Mont et al 20 suggested that there is a 3.6% increase in incidence of AVN for every 10mg/d increase in steroid dose. While high doses of steroids alone can induce AVN, chronicity of use has also been found to increase the risk of this destructive process. 21 It has been studied that cumulative doses from 480 to 4320 mg of dexamethasone or an equivalent steroid can cause osteonecrosis. 22 The exact timing for onset of symptoms after the initiation of steroid therapy is difficult to predict. Some reports in the literature demonstrate gradual symptom onset 6 months after starting steroid therapy to as long as 5 years after initial administration. 18 Definitive radiographic changes with evidence of AVN may not be found until as late as 1 year after the onset of symptoms. 10
Diagnostic Imaging
As stated earlier, clinical symptoms of pain and reduced joint range of motion may precede any findings on diagnostic imaging; however, determining the degree of bony destruction remains key for proper diagnosis and treatment planning for AVN. Radiographs are the first line of imaging for initial evaluation. Sclerotic bands, cystic changes, and a crescent sign in the subchondral bone are indicative of AVN. Due to loss of bone substance resulting in thin cortices and subchondral osteopenia, there is noted radiological resorption of this subchondral bone. These radiographic lesions enlarge, coalesce, and result in the collapse of this region of bone. 10 The Ficat and Arlet classification for AVN is the most widely used system for staging the level of bone necrosis based on the radiographic appearance. 23 Unfortunately, this imaging modality lacks the ability to evaluate early bony changes when compared with more advanced imaging.
MRI provides the highest sensitivity and specificity for diagnosis and remains the gold standard for detecting these pathologic changes. 3 T1-weighted images will demonstrate a single density line that represents the separation of the nonpathologic and necrotic bone, whereas T2-weighted images will demonstrate a high signal line representing the granulation tissue with an increased vascularity. Evidence of bone marrow edema indicates progression to advanced osteonecrosis. 5 Other forms of advanced imaging such as CT or bone scans may highlight subchondral fractures and joint depression. 1 On CT, resorption of healthy bone results in decreased Hounsfield units, reflecting osteopenia. During reossification, new bone is laid down over necrotic trabeculae, increasing Hounsfield units, which appears as sclerosis. 3 Bone scan is a less popular method of evaluation for this destructive bony process. In the early stages of AVN, there is increased osteoblastic activity, which leads to more blood flow to the bone, demonstrated as increased uptake. In the later stages, the necrotic center of the bone shows decreased radioisotope uptake, with an increased uptake noted in the surrounding subchondral bone adjacent to the necrotic segment. 2
Treatment
In the early stages of AVN, with little evidence of bony changes, conservative treatment methods may suffice. Once harrowing radiographic destruction occurs, the result of medical management alone may be unsatisfactory, and a combination of surgical or supportive therapies are required depending on the extent of the pathology. 4 Steroid-induced AVN has been shown to globally affect multiple joints and bones of the foot and ankle and has been demonstrated to be a progressively deteriorating process with continued use of steroid therapy. Therefore, it is not always feasible or effective to surgically intervene with typical invasive treatments of isolated bony AVN such as subchondroplasties, core decompressions, bone transplants, joint replacements, or arthrodeses, when it affects such diffuse areas.2,5 Therefore, these more drastic cases are best managed conservatively to support the systemic disease as well as to prevent the affected areas from further collapse, stress, and continued pain.
Conservative Therapies
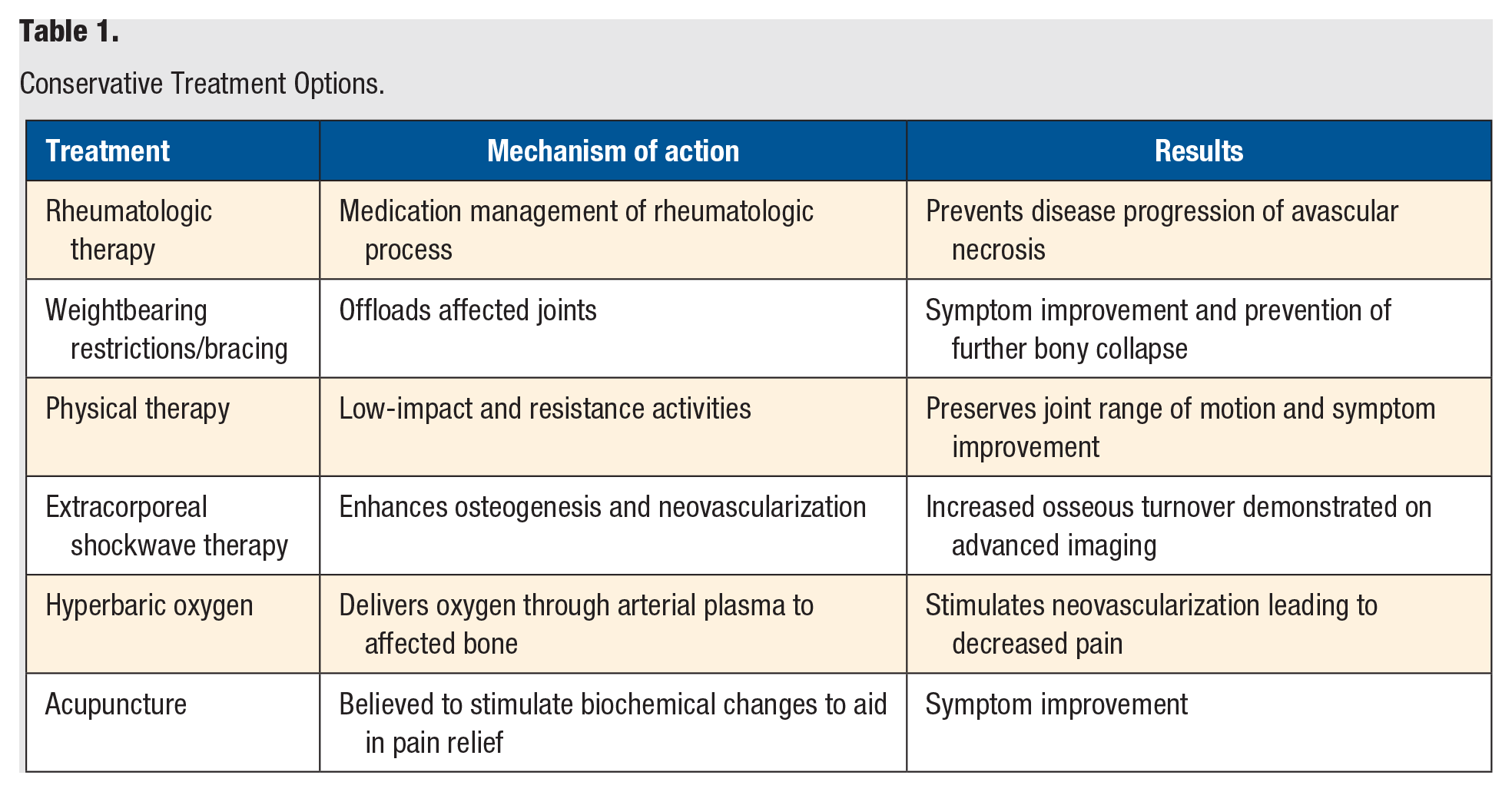
Table 1 lists the conservative therapies for steroid-induced AVN.
Conservative Treatment Options.
Rheumatologic Therapy
Proper management of the underlying systemic disease is key for the management of the AVN itself. Ensuring steroid limitation, as well as exploration of alternative medication options for treatment in order to down titrate steroid use will prevent further collapse and progression of the disease. 2 As SLE is the most prevalent cause for reported cases of steroid-induced AVN, a rheumatologist is often closely involved in treatment and plays a vital role in medication management and monitoring of the clinical course. Close management of medication usage and disease progression with routine labs is imperative to successful treatment of AVN.
Weightbearing Restrictions/Bracing
With the acute diagnosis of AVN, weightbearing restrictions may be aimed to protect the joint from all forces until the affected bone has been revascularized and regained its original strength. Protecting the joint can prevent further collapse or disintegration of the bone. Nonweightbearing is more beneficial in earlier cases or those with evidence of subchondral atrophy or revascularization. The role of weightbearing restrictions becomes more controversial in patients with sclerotic zones and late presentation of the disease. 24 This treatment course may be trialed for up to 6 months of nonweightbearing followed by a period of limited or partial weight bearing 1 . Patellar tendon bracing has been proven to be an effective method of limiting forces for lower extremity AVN of both nontraumatic and traumatic origin. There was noted to be better clinical outcomes in the posttraumatic group; however, radiographic outcomes were found to be comparable in a group of 21 patients (10 nontraumatic vs 11 traumatic). 25 This is an added modality for stability and protection of the joints during the partial weightbearing phase as patients transition into progressively further weightbearing.
Physical Therapy
The role of physical therapy in management of AVN of the foot and ankle although not curative, is imperative to slowing down progression of the disease as well as associated pain. Physical therapy should be targeted toward low-resistance and -impact activities such as swimming, as well as range of motion exercises to preserve joint function. This can be supplemented with the use of a continuous passive motion machine. High-impact and -resistance activities should be avoided by activity modification to prevent further stressors and degenerative changes across the affected bone and joints to maintain functional gait and activity. 26 Adjunctive physical therapy modalities have demonstrated success in management of pain and slowing down the progression of the debilitating disease. Most modalities have been trialed on a case-by-case basis of personal successes without significant literature- or study-based evidentiary support.
Extracorporeal Shockwave Therapy
Electrical stimulation has been shown to experimentally enhance osteogenesis and neovascularization as well as increase osseous turnover. 27 Extracorporeal shockwave therapy (ESWT) sends pulsed electromagnetic fields through soft tissue and the subsequent change of impedance between the soft tissue and bone interface results in energy deposition, which attributes to the therapeutic effect. 28 One hypothesis is that ESWT, through the pulsed fields, can induce microfracturing of the bone to accelerate osteogenesis and angiogenesis. When comparing an ESWT group with a control group, there was a noted increase in expression of bone morphogenic protein (BMP)-2, vessel endothelial growth factor (VEGF), alkaline phosphatase, runt-related transcription factor 2 (RUNX2), and osteocalcin mRNA in marrow stromal cells that all have roles in bone production. 29 Although this therapy shows promising results, electrical stimulation still remains experimental for AVN. Additional studies are needed that define the optimum dosage, application, and duration of this treatment option. Gao et al 30 reported that 83.9% of patients with early-stage osteonecrosis of the femoral head with treatment of ESWT showed significant improvements in the function of affected hips and MRI changes.
Hyperbaric Oxygen
Hyperbaric oxygen therapy (HBOT) is an efficient way of delivering oxygen to hypoxic, blood-deprived areas making it a reasonable treatment modality for AVN. This method delivers a high content of dissolved oxygen into the arterial plasma which diffuses into the tissue areas where red blood cells containing hemoglobin are deprived. Restoring the optimal tissue oxygen level through this will restore cell function. In addition, this state of hyperoxia causes vasoconstriction which reduces edema and intraosseous pressure, leading to improved microcirculation and eventual neovascularization. This principle is similar to the operative effect of core decompression.2,31 A randomized control trial of 20 patients with Ficat stage II femoral head AVN who underwent 30 sessions of HBOT in 6 weeks demonstrated significant improvement in pain and range of motion as well as substantial radiographic healing of AVN. 32 Follow-up after 7 years of HBOT showed clinical improvement and no patients required surgical intervention of total joint arthroplasty. A study by Reis et al 33 demonstrated regression of MRI changes in 12 out of 16 Steinberg stage I AVNs. Even with some preliminary studies, the use of HBOT is still considered controversial in both early and diffuse stages of AVN due to limited data available.
Acupuncture
Acupuncture has been supported in the Eastern medicine literature in the past for treatment and management of chronic pain in many debilitating conditions. As diffuse AVN can be extremely painful across many joints, it is difficult to achieve adequate pain relief conservatively and without experiencing side effects of traditional analgesics. Acupuncture provides patients a method of symptom management of chronic and diffuse pain. There is no medical evidence that acupuncture points exist; however, numerous studies suggest that the stimulation from acupuncture increases blood flow as well as triggers the activity of the body’s natural painkillers. Wang et al 34 compared the efficacy of traditional acupuncture and acupotomy for the treatment of AVN at early and middle stages and noted significant increase in Harris Hip Score for both groups. Jafarian et al 35 also described a case report utilizing laser acupuncture, which uses laser light in place of needles to stimulate acupuncture points, showing progressive regeneration of femoral head AVN on MRI findings. The addition of acupuncture can be used as an effective tool for management of pain symptoms to aid during rehabilitation, physical therapy, and pharmacologic treatments.
Medications
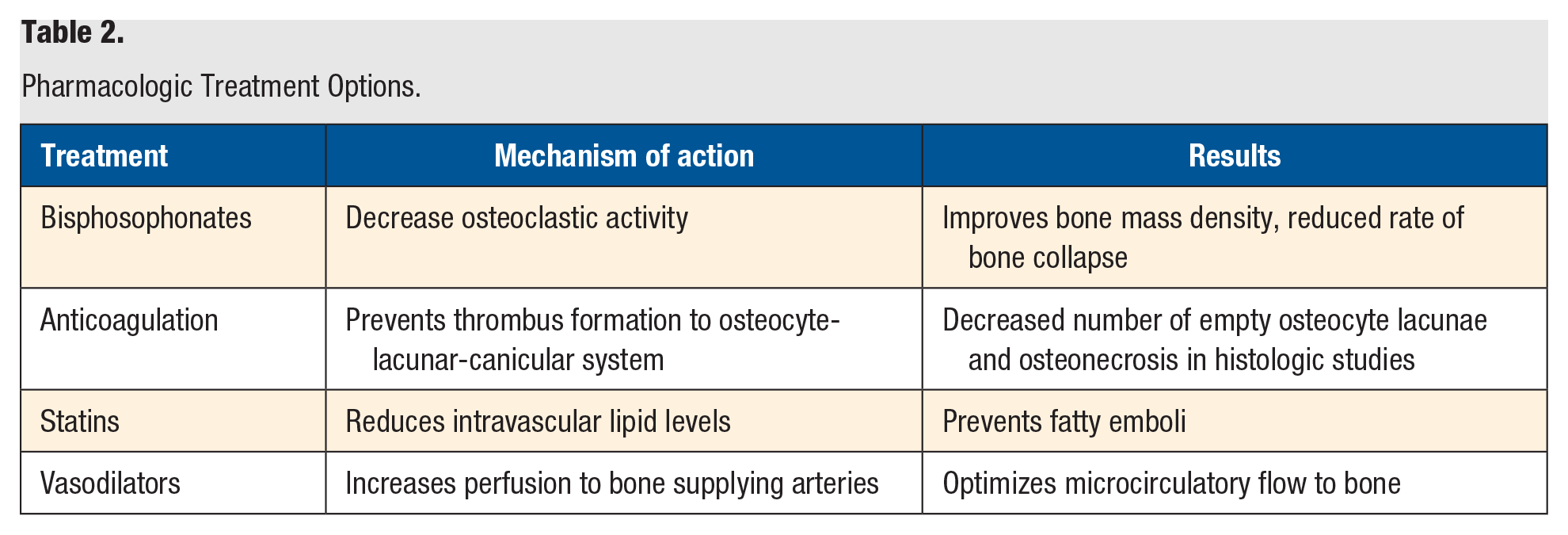
Table 2 lists the pharmacologic therapies for steroid-induced AVN.
Pharmacologic Treatment Options.
Bisphosphonates
Bisphosphonates have been occasionally used to treat and supplement AVN. Bisphosphonates are effective through their ability to decrease osteoclastic activity and improve bone mass density. 5 The nature of the drug includes anti-resorptive and anti-inflammatory actions that prevent structural bone weakening from reparative osteocytic necrosis and apoptosis. There are some studies that demonstrate clinical improvement with use of bisphosphonates for progressive AVN; however, there is no consensus on the duration of therapy. Studies in the femoral head suggest alendronate use led to a significant improvement in pain and disability score, reduction in the rate of collapse, and decreased requirement for surgery with the efficacy lasting up to 10 years. 36
Anticoagulation
In recent literature, scholars have investigated the effects of anticoagulants on relieving or reversing venous occlusion as well as preventing thrombus formation. Osseous venous outflow obstruction and intravascular coagulation caused by venous thrombosis leads to reduced arterial flow, ischemia, bone death, and subsequent collapse of the articular surface. 37 Given the positive effect of anticoagulants such as enoxaparin in the inhibition of the progression of osteonecrosis, further investigations have been done for the use of enoxaparin as therapeutic treatment during high-dose glucocorticoid therapies. In animal studies where high doses of glucocorticoid methylprednisolone were administered, the experimental group with additional co-treatment of enoxaparin resulted in a decrease in the number of necrotic changed osteocytes and empty lacunae under histologic examination when compared with the control group. The control group without dual therapy of enoxaparin demonstrated pathologic histological features of osteonecrosis including an increased number of empty osteocyte lacunae and osteonecrotic changed osteocytes, suggesting that the co-treatment of anticoagulation may have a preventative effect to the progression of steroid associated AVN. 38 A study by Glueck et al 39 demonstrated that enoxaparin therapy in 19 of 20 patients with thrombophilic-hypofibrinoloytic disorders could arrest progression of osteonecrosis in patients exhibiting Ficat stages I and II bony changes. 39 Further clinical studies with larger patient volumes are still needed to assess dosage and treatment duration of supplementation of anticoagulation to prevent formation or further progression of AVN.
Statins
This group of medications are traditionally used to lower cholesterol levels by reducing intravascular lipid levels. As stated, patients with steroid-induced AVN often exhibit hyperlipidemia which leads to the formation of fat emboli. 15 Statins may assist in the disease progression by decreasing lipids, therefore preventing the fatty emboli that lead to bone cell death and increasing vascularization to reverse osteonecrosis. In an animal study with rabbits, it was demonstrated that simvastatin and pravastatin significantly reduced the incidence of steroid-induced AVN. 40
Vasodilators
As the pathomechanism of steroid-induced AVN is thought to impair blood flow to the bone, vasodilating agents can therefore decrease the perfusion pressure and increase blood flow to the microcirculatory system, including those arteries supplying bone. Drescher et al 41 conducted a study in a rabbit model receiving methylprednisolone injections to investigate nitric oxide and nitrate patches as a preventative effect on a steroid-related AVN. Histological observation demonstrated decrease of empty osteocyte lacunae and adipose sites in the nitrate patch–treated animal groups compared with the control animals, suggesting a preventative effect of nitrate as co-treatment for steroid-induced AVN. 41 The positive effects of the prostacyclin derivative iloprost as a dilator were studied by Claßen et al, where 108 patients with 136 osteonecrosis sites with differing etiology and severity were treated with iloprost. There was significant improvement of subjective complaints with administration of iloprost over a 6-hour period daily for 5 days in 74.8% of patients. The medication overall proved to be an effective therapeutic option of AVN involving different locations in the body. 42
Surgical Treatments
In the cases of isolated bone or joint AVN, surgical intervention has proven to be successful. In the setting of systemic steroid-induced AVN; however, there is limited literature to suggest that treating every affected joint is a viable option. There is an increased burden to the patient, rate of complications, and rehabilitation required from multiple surgeries. There are, however, some circumstances in which surgical intervention may be of interest in the setting of less severe scenarios, where there are either fewer bone and joint sites affected, or a location that has significantly increased pain compared with others. When there is a select debilitating joint, in which pharmaceutical and physical therapy control of symptoms has failed, a patient may benefit from surgical procedures to assist in revascularization of the affected area or debridement of inadequate bone.2,5 Surgical interventions can include bony resection and accompanied bone grafting to rebuild the structure and provide mechanical support. Core decompression is used to reduce intramedullary pressure and improve blood flow, while joint fusion or replacement are more aggressive options that prevent further pain across the affected joint site.43,44
Conclusion
The exact etiology of steroid-induced AVN is unknown, although several proposed pathophysiological processes have been described. Physical therapy modalities and various pharmacologic agents can provide symptom relief as well as prevention of disease progression. Many of the conservative treatment options are promising and have shown to be effective in smaller scale investigations and animal studies; however, they require further higher level of evidence research for the specific population of global steroid-induced AVN. The recommendation for treatment of this disease process is trialing conservative options to prevent progression of the osteonecrosis in the acute stage, as well as symptom management in the chronic stage as surgical intervention for diffuse AVN is often not feasible and impractical. Surgical interventions should be reserved for an isolated debilitating joint and paired with medication supplementation or modification. Further investigation of this disease process caused by steroid use will be necessary for the development of optimized treatment options.
Footnotes
Author Contributions
Shirley S. Chen, DPM; Amber M. Kavanagh, DPM; Caitlin Zarick, DPM, FACFAS: provided substantial contributions to conception and design, acquisition of data, drafting the article and revising it critically for important intellectual content, and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.