
Abstract
Background
Few studies have investigated return to play after surgical stabilization of syndesmotic injuries without fracture with minimal data on patient-reported outcome measures. The purpose of this study was to evaluate patient-reported outcomes, patient satisfaction, and return to play after surgical repair of syndesmosis injuries in competitive athletes.
Methods
A retrospective review of competitive athletes who underwent surgery for an unstable syndesmosis was performed. Patients were excluded if they were not competitive athletes or had the presence of a concomitant fracture. Patient-reported outcome measures were collected via telephone questionnaires. These included the Foot and Ankle Ability Measure (FAAM) Sports Subscale as well as 7 other questions regarding subjective assessment of function, patient satisfaction, and return to play.
Results
A total of 29 ankles in 28 competitive athletes were included. Twenty-four of 28 (86%) patients were male, and 4 of 28 (14%) patients were female. Average age at surgery was 20.7 ± 2.4 (15-24). Twenty-five of 28 (89.3%) athletes completed the post-operative telephone questionnaire with a mean follow-up of 41 months (minimum 9 months). In total, 100% of patients returned to athletic activity. Nineteen of 20 patients (95%) eligible to do so returned to competition, with 16 of 25 (64%) patients reporting a return to pre-injury level of function. The average FAAM-sports score was 29.6 (max 32) ± 3.5. Twenty-four of 25 patients reported post-operative function as normal or nearly normal. Twenty-four of 25 patients reported that they were either very satisfied or satisfied. Patient-reported time of return to unrestricted play was 19.9 ± 9.8 weeks. Injury grade, repair technique, acuity of injury, and concomitant injuries were not associated with prolonged return to play or decreased FAAM scores.
Conclusion
A high percentage of competitive athletes undergoing surgical treatment of syndesmosis injury were able to return to their previous level of competition, with nearly all achieving good-to-excellent outcome scores and satisfaction. Severity of injury, concomitant injury, or repair technique was not found to have an effect on outcomes.
Level of Evidence
IV, single-arm retrospective case series.
Introduction
“The purpose of this study was to evaluate patient-reported outcomes, patient satisfaction, and return to play after surgical repair of syndesmosis injuries in competitive athletes.”
Syndesmotic ankle injuries, often referred to as high ankle sprains, commonly occur among high-level athletes engaging in contact sports such as football, soccer, and lacrosse. High ankle sprains account for 7% to 25% of total ankle sprains 1 and have been associated with longer recovery than lateral ankle sprains. 2
Management of isolated syndesmotic injuries in athletes is controversial, particularly regarding diagnosis and treatment of intermediate-grade unstable injuries without gross tibiofibular diastasis. 3 There has been recent interest in surgical management of syndesmotic injuries to allow for earlier return to play, 4 and a high rate of return to sport has been demonstrated by multiple systematic reviews.4-6 However, there are few published clinical studies of outcomes after surgical repair of the syndesmosis in athletes,7-11and only 2 of these studies reported any patient-reported outcome measures (PROMs).9,11 Both of these studies were limited to a single scoring questionnaire, and none have reported patient satisfaction, subjective assessment of function, or subjective timing of return to unrestricted play.
The aim of this study was to explore return to play and PROMs, including satisfaction and subjective assessment of function, of competitive athletes who underwent surgical treatment of unstable syndesmotic injury without associated fracture.
Methods
Institutional review board (IRB) approval for the study was obtained. A retrospective chart review using a single institution’s electronic medical record was performed using Current Procedural Terminology (CPT) code 27829, Ankle/Lower leg, and Open Reduction and Internal Fixation (ORIF) distal tibiofibular joint disruption (syndesmosis). Inclusion criteria included competitive athletes (high school, collegiate, or professional level) above age 14 who underwent surgery for acute, primary syndesmosis injuries between January 2017 and April 2024, with minimum a follow-up of 9 months. All patients underwent surgical repair by one of 2 fellowship-trained foot and ankle surgeons, using trans-syndesmotic stabilization with suture button constructs or direct anterior inferior tibiofibular ligament (AITFL) reconstruction, with ankle arthroscopy prior to syndesmotic stabilization/repair. Surgical technique was selected at the surgeon’s discretion based on instability/injury pattern. Exclusion criteria included recreational athletes (those not participating at high school, collegiate, or professional level) and concomitant lateral, medial, or posterior malleolus fracture. Patients undergoing other ligamentous repairs at the time of syndesmotic stabilization (ie, lateral ligament reconstruction, deltoid ligament repair, etc) were included in the study. There was no comparison group utilized.
Syndesmotic injuries were classified as either West Point grade 12 2B (partial syndesmosis injury with instability) or 3 (complete syndesmotic disruption with frank diastasis), as modified by Calder et al 7 based on stress or weight-bearing radiographs, magnetic resonance imaging (MRI), clinical examinations, and findings under arthroscopy. The IRB approval was obtained for the telephone survey process including the questionnaire that was administered. No patients were under 18 years old at the time of the telephone survey. All requirements under the Health Insurance Portability and Accountability Act (HIPAA) were followed. All patients were contacted via telephone to complete a questionnaire at the time of chart review, and informed consent was obtained to participate in a research study. This included the Foot and Ankle Ability Measure (FAAM)-sports subscale-questionnaire 13 with an additional 7 questions regarding return to play and patient satisfaction. Twenty-five of 28 (89.3%) patients completed the survey over the phone; 3 of 28 (11.7%) patients were lost to follow-up.
Surgical Techniques
Rehabilitation Protocol
Statistical Analysis
Statistical analysis was performed using Student’s t-tests to evaluate differences in time to return to play and FAAM-sports subscale scores based on gender, West Point grade, presence of cartilage injury, concomitant lateral ligament reconstruction, or concomitant deltoid ligament repair. One-way analysis of variance (ANOVA) testing was used to evaluate the timing of return to play and FAAM-sports scores based on the surgical technique utilized (trans-syndesmotic suture button fixation vs AITFL reconstruction vs both techniques), as well as the timing of surgery relative to injury (acute, subacute, chronic). For the purposes of analysis, acute was defined as surgery within 4 weeks from injury, subacute as within 4 to 12 weeks from injury and surgery, and chronic as longer than 12 weeks between injury and surgery.
After exclusions, 29 ankles in 28 patients were included for analysis of surgical details, injury classifications, and complications. Twenty-five of 28 patients (89.7%) completed telephone surveys and were included in the PROM analysis. All 25 of these patients were included in the return to athletic activity analysis. Twenty of 25 (80%) patients were eligible to return to competition after surgery and were included in the return to competition analysis. Five of 25 patients (20%) had surgery during their senior season or after their career ended and were not eligible for return to competition analysis.
Results
Demographics
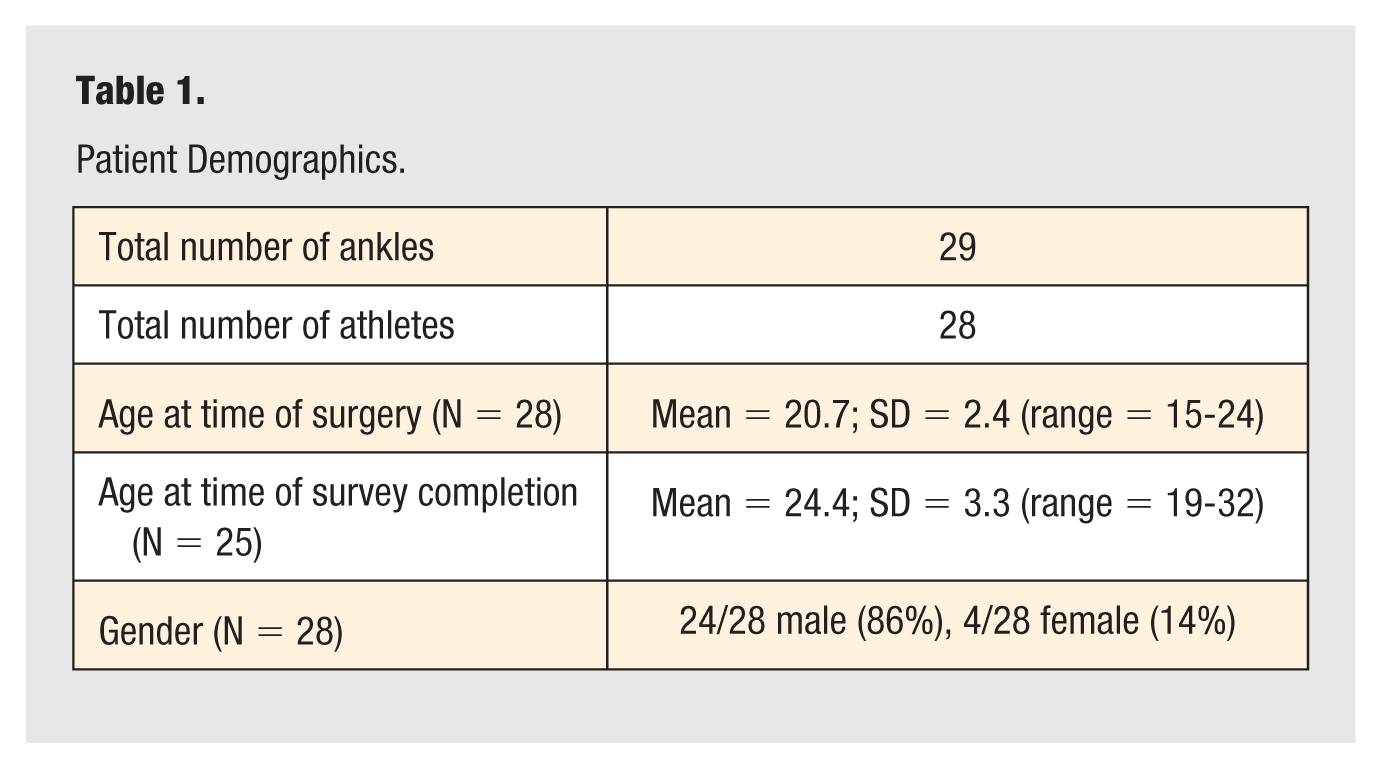
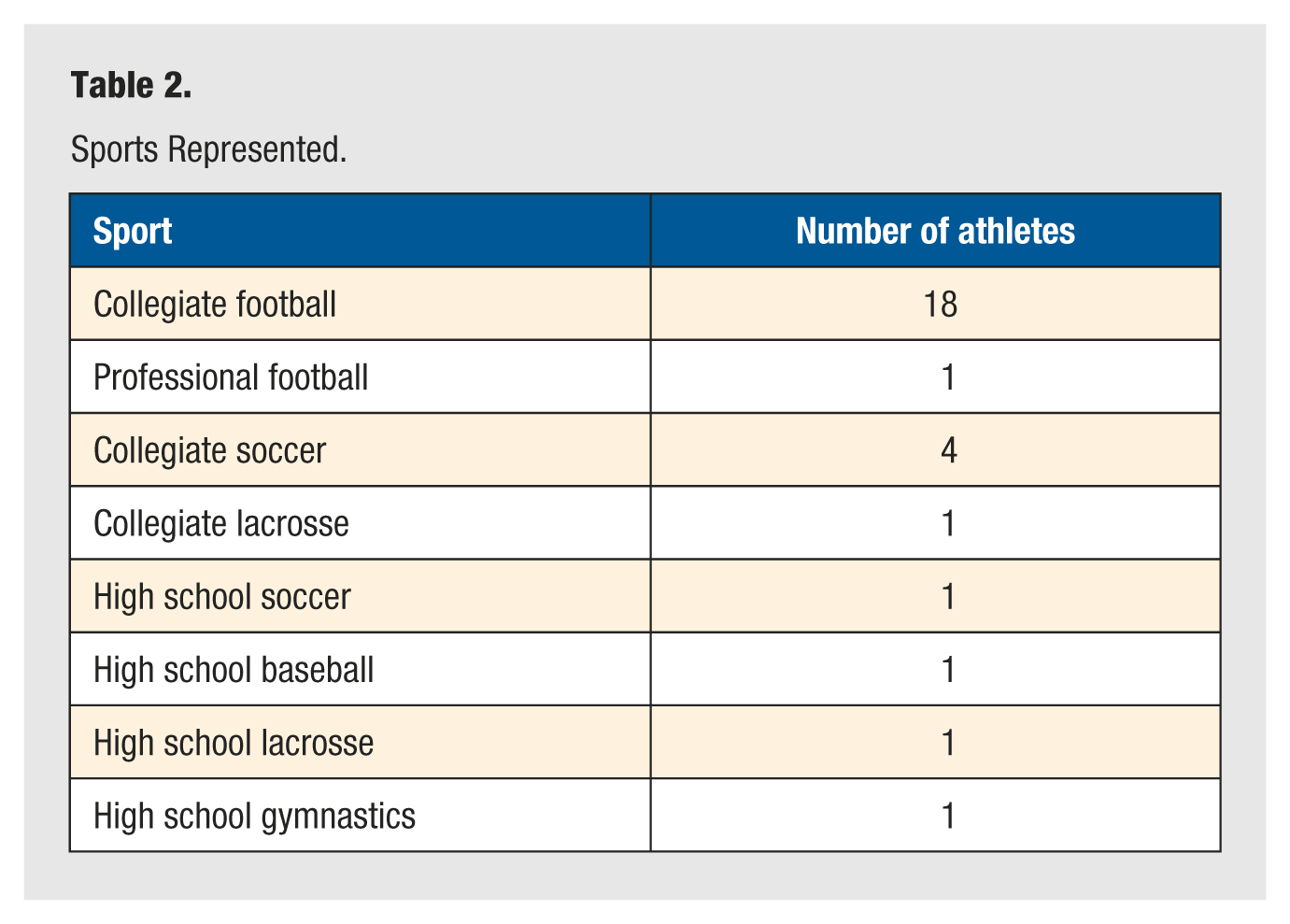
A total of 29 ankles in 28 patients were included in the analysis, as 1 patient had surgery for a contralateral syndesmosis injury 3 years after the index procedure (Table 1). The average age of the athletes at the time of surgery was 20.7 ± 2.4 (range = 15-24). Of the patients who completed telephone surveys (N = 25 patients), the average age at the time of survey completion was 24.4 ± 3.3 (range = 19-32). Twenty-four of 28 (86%) patients were male, and 4 of 28 patients were female (14%). Specific sports at the time of injury (Table 2) included collegiate American football (18), professional American football (1), collegiate soccer (4), collegiate lacrosse (1), high school soccer (1), high school baseball (1), high school lacrosse (1), and high school gymnastics (1). One collegiate football player underwent contralateral surgery for a syndesmosis injury while playing professional football 3 years after the index procedure. Two of 4 high school athletes ultimately progressed to a collegiate career in their respective sports.
Patient Demographics.
Sports Represented.
Injury Classifications, Surgical Details, and Complications
Seven of 29 (24.1%) surgeries were for acute injuries (surgery within 4 weeks of injury), 8 of 29 (27.6%) surgeries were for subacute injuries (surgery 4-12 weeks after injury), and 13 of 29 (44.8%) surgeries were for chronic injuries (surgery greater than 12 weeks from injury) (Table 3). Five of 29 ankles (17.2%) were West Point grade 3 (radiographic tibiofibular diastasis with complete injury of syndesmotic ligaments). Twenty-four of 29 ankles (82.8%) were West Point grade 2B (unstable syndesmosis without radiographic tibiofibular diastasis). Eight ankles underwent concomitant deltoid ligament repair (27.6%), 12 ankles underwent lateral ligament reconstruction (41.4%), and 5 of 29 ankles had evidence of chondral injury on routine arthroscopy (17.2%). Eleven of 29 (38%) ankles were true isolated syndesmosis injuries without lateral or deltoid ligament injuries.
Injury Classifications, Surgical Details, and Complications.
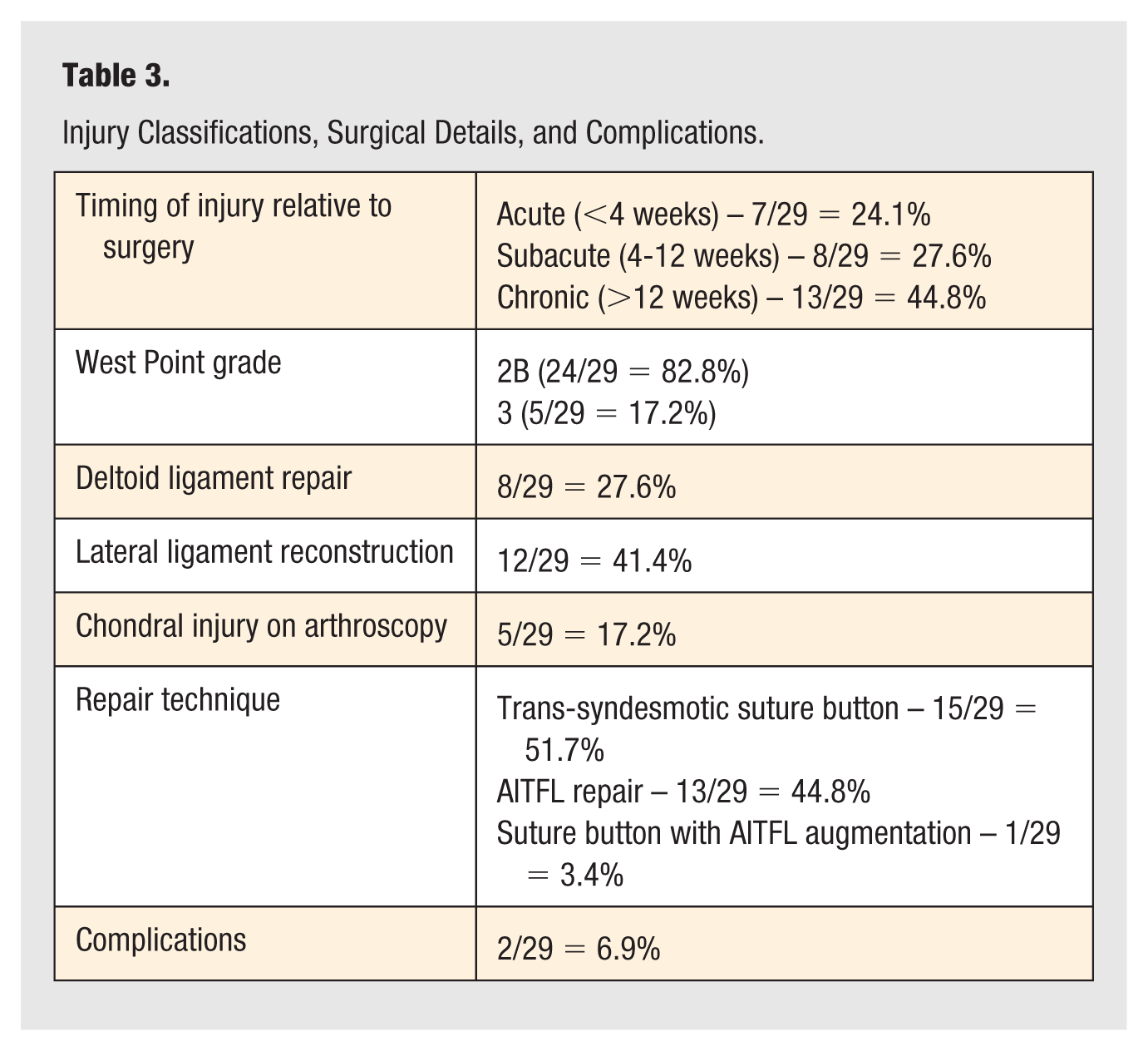
Fifteen of 29 (51.7%) ankles were treated with trans-syndesmotic flexible fixation with a suture button construct. Thirteen of 29 (44.8%) ankles were treated with direct AITFL repair using suture anchors. One ankle was treated with both techniques.
Complications were seen in 2 of 29 surgeries (6.8%). One patient had post-operative peroneal neuropathy and later underwent common peroneal/superficial peroneal nerve decompression with improvement in symptoms. One patient required removal of the suture button construct due to saphenous neuritis from the medial button. The patient’s symptoms resolved with hardware removal.
Survey Results
Twenty-five of 28 (89.3%) athletes completed telephone surveys post-operatively at a mean follow-up of 41 months (3.4 years) post-operatively, with a minimum follow-up of 9 months (range = 9-88 months) (Table 4). Mean FAAM-sports subscale score was 29.6 ± 3.5 out of 32 (range = 21-32). The mean “Percentage Normal” was 86.6% ± 16.5%.
Telephone Survey Results.
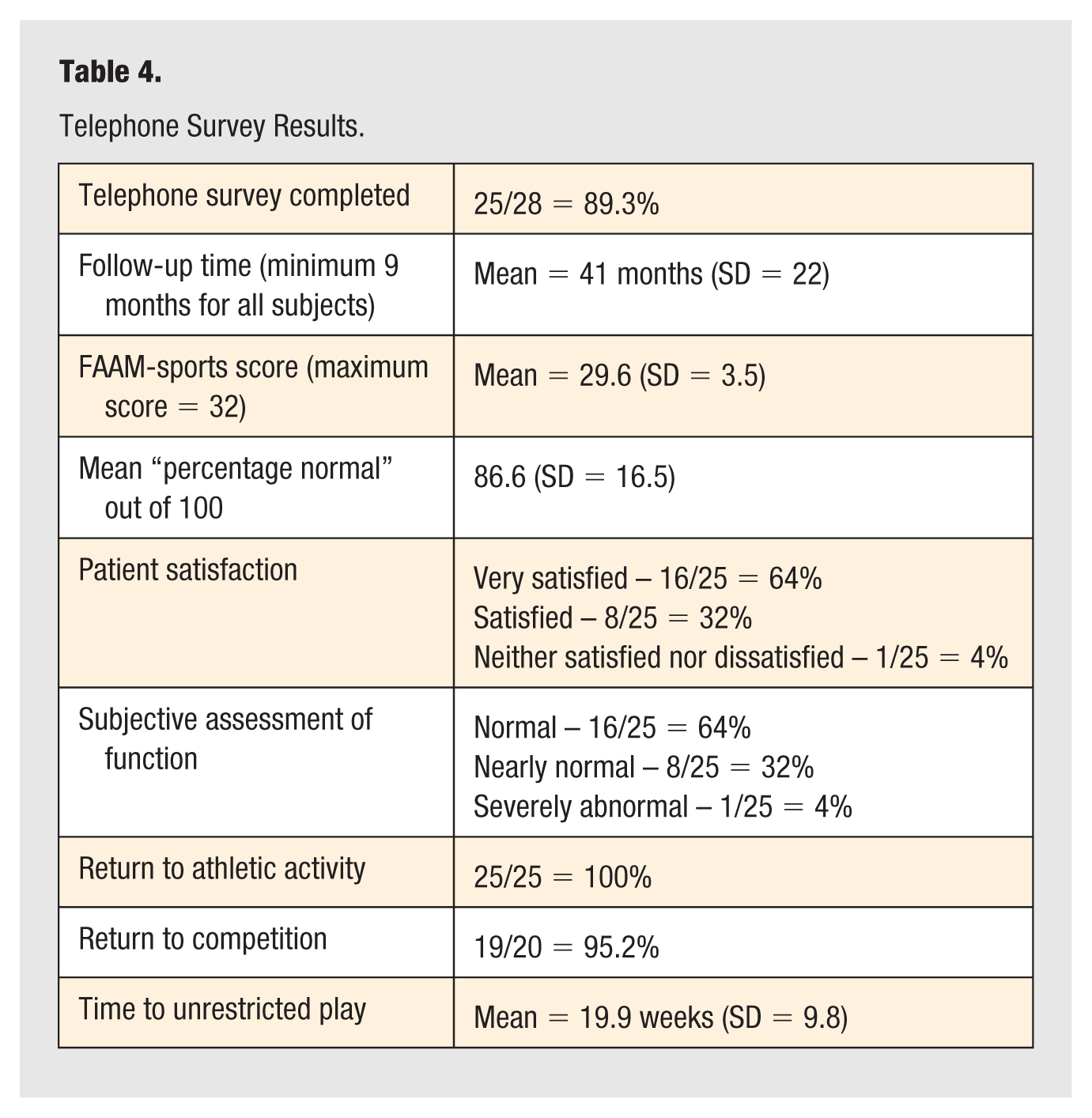
Average reported return to unrestricted play was 19.9 weeks ± 9.8 (range = 2-52 weeks). Twenty-five of 25 (100%) patients returned to athletic activity after surgery. Four of 25 patients had surgery after their competitive athletic careers ended or during their senior seasons. Of the 20 patients who were eligible to do so, 19 of 20 (95%) patients returned to competition level. The 1 athlete who did not return to competition level was a high school athlete.
Twenty-four of 25 (96%) patients rated their current level of ankle function as normal (16/25 = 64%) or nearly normal (8/25 = 42%). One of 25 (4%) patients rated the current level of function as severely abnormal. Sixteen of 25 (64%) patients reported that they returned to the pre-injury level of function. Nine of 25 (36%) patients reported they did not return to the pre-injury level of function. Twenty-four of 25 (96%) patients reported they were either very satisfied (16/25 = 64%) or satisfied (8/25 = 32%) with their surgical outcome. One of 25 (4%) patients reported neither satisfied nor dissatisfied with the outcome. Twenty-three of 25 (92%) patients reported that they would have surgery again, with 2 of 25 (8%) patients reporting that they would not undergo surgery again. Two of 25 (8%) patients had a repeat injury of the operative ankle after return to play; the remaining patients reported no further injuries to their ankle.
Variables Associated With Timing of Return to Unrestricted Athletic Activity and Outcome Scores
The 25 patients who completed telephone surveys were included in the analysis. All patients reported on return to unrestricted athletic activity, even if not eligible to return to competition level. The only variable found to have a significant difference in timing to return to athletic activity was gender, with female patients in the cohort having an average return to play of 25.0 ± 1 weeks compared with male patients, who returned on average at 19.2 ± 10.5 weeks (difference 5.8, P = .02). Of note, only 3 female patients were included in the analysis. There was no significant difference in timing of return to athletic activity associated with West Point grade (P = .283), the presence of cartilage injury on arthroscopy (P = .202), concomitant lateral ligament reconstruction (P = .283), concomitant deltoid ligament repair (P = .608), surgical technique, ie, trans-syndesmotic suture button fixation vs AITFL reconstruction vs both (P = .494), or acuity of injury in relation to surgical timing (P = .327).
On statistical analysis of FAAM-sports subscales, patients with the presence of chondral injury were actually found to have a statistically higher average score than those without (31.75 vs 29.2, P = .006). Otherwise, there was no statistically significant difference detected in FAAM scores based on gender (P = .116), West Point grade (P = .669), concomitant lateral ligament reconstruction (P = .321), concomitant deltoid ligament repair (P = .989), surgical technique (P = .670), or acuity of injury (P = .435).
Discussion
In this cohort of young (age range = 15-24), competitive athletes undergoing surgical repair of the ankle syndesmosis without associated fracture, return to sport was excellent, with 100% of athletes who completed telephone surveys returning to unrestricted athletic activity, and 19 of 20 (95%) athletes eligible to do so returning to collegiate or professional competition level. This is similar to other systematic reviews in the literature. Vancolen et al 6 reported a 93.8% return to pre-injury level for athletes after syndesmotic injury; however, that study included recreational athletes as well as injuries managed non-operatively in the analysis. A more recent systematic review by Bolia et al 5 reported that 100% of 171 elite athletes (collegiate or professional level) undergoing surgical repair of ankle syndesmosis injuries returned to sport. The majority of the studies included in this review focused solely on timing of return to play rather than subjective assessments of function, which is the strength of our study. Our study included 4 high school athletes, 2 of whom did progress to a collegiate career in their respective sport. The 1 patient in our cohort who did not return to competition level despite being eligible to do so was a high school athlete whose sport was gymnastics. Five patients in our cohort were not eligible to return to competition, as their injury ended their senior season; however, all of these patients reported return to athletic activity. Three of the 5 patients reported a 32/32 on the FAAM-sports score, rated their current ankle function as “normal,” and reported that they returned to pre-injury level of function. Two of the 5 patients reported an FAAM-sports score of 21/32 and that they did not return to pre-injury level.
There are minimal data in the existing literature on PROMs after syndesmosis repair in athletes. Of the studies included in the previously mentioned systematic review, which were athlete-specific studies, only 2 included any PROMs, both of which were limited to a single outcome score. Kim and Shin 9 reported on 22 athletes undergoing suture anchor repair of the AITFL and included only the average Foot and Ankle Outcome Scores (FAOS). Taylor et al 11 described a case series of 6 collegiate athletes undergoing screw fixation of syndesmotic injuries and reported scores using the Sports Ankle Rating System. Our study offers a greater breadth of PROMs, including the FAAM-sports subscale, subjective assessment of function, and patient satisfaction, which should assist surgeons who treat athletes in the future with regards to patient counseling. Our cohort was also larger (28 patients) than the previous studies that included any PROMs.
In addition, of the 171 athletes in the Bolia systematic review, 5 only 3 played American football. The highest number of patients in these studies were either soccer or rugby players.7-10 To our knowledge, our study reports return to play and outcomes on the largest cohort of American football players undergoing surgical repair of the syndesmosis in the literature, with 19 patients in our series playing football. This is significant given the prevalence of these injuries in American football as well as recent media attention.
A review of National Football League (NFL) athletes participating in the NFL combine from 2009 to 2015 reported that 1216 of 2285 (53.2%) had a history of ankle injury, with high ankle sprains representing 417 of 1242 (33.6%) ankle sprains. 14 Another study reported 533 high ankle sprains in 498 NFL players between 2009 and 2020. 15 In collegiate football, Hunt et al 16 reported 573 high ankle sprains over a 5-year period, accounting for 24.6% of all ankle sprains; however, only 2.7% required surgical intervention. Our study adds important data to the existing literature on surgical syndesmosis repair in football players, as relatively small numbers of athletes require surgical intervention in comparison with the total number of high ankle sprains sustained. This is particularly true as the indications for surgery in intermediate-grade injuries evolve.
The average patient-reported return to play in our cohort was 19.9 weeks (139 days). The most comprehensive study on return to play after surgical treatment was done by D’Hooghe et al. 8 They followed 110 professional soccer players after surgery for West Point grade 2B and 3 injuries without fracture and found a mean time to return to team training of 72 days post-operatively and a mean time to first official match of 103 days post-operatively. This is a faster return to play than the averages seen in our cohort. It is, however, important to note that all athletes in their study were professional-level athletes and did not include the higher-energy injuries often sustained during American football participation. The majority of athletes in this study were collegiate level; thus, the timing of surgery in relation to in-season or off-season status may have had more influence on return to play. We also based our return-to-play information on patient-reported data, which may contribute to differences.
Eleven of the 29 (38%) ankles in this study were true isolated syndesmosis injuries without lateral or deltoid ligament injuries. Five of the 29 (17.2%) ankles demonstrated chondral injury on arthroscopy. There are growing data to suggest that isolated syndesmosis injuries are rare, and risk factors for prolonged returned to play should be evaluated. A recent analysis of 83 syndesmosis injuries in the NFL found that only 11 of 83 (13%) injuries were isolated to the syndesmosis, with 65 of 83 (78%) associated with other ligamentous injuries. 17 That study found a significantly longer return to play if there was the presence of an associated deltoid injury or fracture. Calder et al 7 similarly found prolonged return to play with associated deltoid ligament injury, and the previously discussed D’Hooghe study 8 found prolonged returned to play with chondral injury. We did not find worse FAAM scores or differences in return to play with concomitant injury in our cohort; however, this could have been limited by sample size. Interestingly, patients with chondral injury had a significantly higher FAAM score in our cohort than those without. While these data are difficult to interpret, it underscores the importance of routine arthroscopy and suggests that even with chondral injury, return to play and outcomes can be predictable. There was no significant impact on the timing of surgery in relation to injury, and this may indicate that even those athletes with delayed presentation may do well once an appropriate diagnosis and treatment plan is established.
This study is not without limitations. This was a retrospective study, which comes with inherent limitations in data collection. This was a single-arm case series without a comparison group. This was also a relatively small sample size with 29 surgeries completed by only 2 surgeons, which may limit generalizability. Return-to-play data are difficult to standardize, as there are different definitions on return to play. This is particularly true in high school and collegiate athletics, as several players had surgery in the off-season or after their careers ended, unrelated to their injury. In addition, there may be differences from when a player is cleared to return to play by their surgeon or athletic trainer compared with when he or she actually felt comfortable to return to sport. We therefore focused on subjective return to unrestricted play data reported by the individual athletes as a PROM; however, timing of return to play was still influenced by whether the athlete was in or out of season at the time of injury. Three patients were lost to follow-up and did not complete telephone surveys. The telephone surveys were also administered at the time of chart review rather than at standardized time post-operative points with variable follow-up. The information included is thus subject to recall bias, in particular for patients with longer follow-up. The study participants were obviously made aware that they were participating in a research study, which could influence responses. We also did not compare non-operative to operative treatment in grade II injuries; thus, we are unable to comment on differences in return to play or outcomes.
Conclusion
In this review of competitive athletes who underwent surgical repair of an unstable ankle syndesmosis injury without associated fracture, nearly all were able to return to their previous level of participation, with high patient satisfaction and outcomes scores, and few complications. Severity of injury, presence of concomitant injury, and repair technique were not found to have an effect on patient-reported outcome scores or timing of return to play.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Institutional review board approval from the University of Virginia Health System (IRB approval number 24455) was obtained for the study, and informed consent was obtained from study participants via telephone.
Data Availability Statement
The data sets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Trial Registration
Not applicable.