
Abstract
Purpose. This study investigated whether the Wide-Awake Local Anesthesia No Tourniquet (WALANT) technique, widely used in hand surgery, is safe and acceptable in elective hallux valgus (HV) surgery. Methods. A total of 83 patients were included in this cross-sectional retrospective study, 38 of whom underwent surgery with WALANT and 45 of whom underwent surgery with spinal anesthesia (SA). The 2 groups were compared regarding demographic data, clinical results, and radiological outcomes. Results. Preoperative preparation time and hospital stay were shorter in the WALANT group compared to the SA group. Visual analogue scale (VAS) values at the first, sixth, and 72nd hours after surgery were lower in the WALANT group. Intraoperative VAS-Anxiety (VAS-A) values were higher in the WALANT group, while postoperative VAS-A values at the sixth hour were lower. In the WALANT group, American Orthopaedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal Rating System (AOFAS Hallux MT-IP) postoperative second-week values were found to be higher and the time to return to work was shorter than in the SA group. The groups had no significant difference regarding other variables. Conclusion. The WALANT technique in HV surgery is a method that can be easily applied, is safe, and is not inferior to SA in terms of clinical results. The WALANT shortens preoperative patient-preparation time, hospital stay, operating room usage, and return-to-work time after HV surgery. It improves functional and clinical results with low postoperative complication rates.
“The walant technique in hv surgery is a method that can be easily applied, is safe, and is not inferior to sa in terms of clinical results.”
Introduction
Hallux valgus (HV) is a disease characterized by hypermobility and pronation of the first metatarsal bone, which eventually leads to subluxation and pain in the first metatarsophalangeal (MTP) joint. 1 When conservative treatment methods fail, surgical proximal/distal osteotomies, joint arthrodesis, and soft tissue procedures are performed. In these surgical procedures, spinal anesthesia (SA), other locoregional anesthesia methods (local anesthesia, knee and ankle nerve block), and general anesthesia are most commonly used. 2 Although the Wide-Awake Local Anesthesia No Tourniquet (WALANT) technique has shown high efficacy, safety, patient satisfaction, and cost-effectiveness in hand surgery, data on its use in HV surgery are limited. 3 This technique provides advantages for the patient and the surgeon regarding comfort, time, and cost savings and reduced admission to intensive care. 4 In addition, general and locoregional anesthesia has many complications, and local anesthesia (LA) reduces these complications. Although there are a few studies using WALANT in foot and ankle surgeries such as trauma and HV surgery, the number of patients and the parameters investigated in these publications are limited.5,6
This study aimed to investigate whether the WALANT technique, which is widely used in hand surgery, is safe and acceptable in elective HV surgery. For this purpose, we investigated the difference in clinical significance and patient satisfaction between WALANT and SA, the most commonly used technique in HV surgery present.
Materials and Methods
The institution’s ethics committee approval is obtained for the study by the Declaration of Helsinki. Patients who underwent HV surgery under WALANT and SA were retrospectively analyzed. In total, 97 patients were identified. Patients who had inflammatory arthritis, hallux rigidus in addition to HV, hallux valgus angle (HVA) over 40 degrees, intermetatarsal angle (IMA) over 15 degrees, and who were operated under general anesthesia were excluded from the study. In total, 14 patients who met the exclusion criteria were not included in the study. At last, 83 patients are included in the study. In all, 38 of them were operated under WALANT and 45 of them were operated under SA between 2020 and 2024. Scarf osteotomy was done to 6 patients in the WALANT group and 5 patients in the SA group, while chevron osteotomy was done to the other patients. In addition to osteotomies, HV soft tissue procedures were done to all 83 patients in the study. Informed consent was obtained from all included patients.
Preoperative patient-preparation time, hospital stay length, intraoperative visual analog score (VAS), and visual analog scale for anxiety (VAS-A) score at first, sixth, and 72nd hours, operation time, preoperative and postoperative IMA and HVA, wound healing problems, return-to-work time, and AOFAS Hallux MT-IP (American Orthopaedic Foot and Ankle Society [AOFAS] Hallux Metatarsophalangeal-Interphalangeal Rating System) were evaluated. This scoring system was evaluated with patients in the preoperative period, early postoperative period (second week), and mid-postoperative period (second month). Preoperative patient “preparation time” was evaluated as the time from the patient’s arrival in the operating room until the skin incision. “The operation time” was calculated in minutes as the difference between skin incision and skin closure.
Postoperatively, all patients were followed up with HV shoes for 4 weeks. Then, full weight bearing without HV shoe was allowed. Patients in the WALANT group were discharged on the same postoperative day, and patients in the SA group were discharged the day after surgery. The decision on the time to return to work was left to the patient’s discretion, provided that it was not earlier than 10 days.
Preparation of Wide-Awake Local Anesthesia No Tourniquet
The WALANT solution was prepared as 50 mL (1 mL 0.5 mg/mL epinephrine, 25 mL 2% lidocaine, 5 mL 8.4% sodium bicarbonate, and 19 mL 0.9% isotonic sodium chloride), and a total of 30 mL was applied to each patient. In total, 4 mL was applied subcutaneously to the incision line. Three points were determined at equal intervals along the incision line (Figure 1).

Four regions where WALANT was applied (the midpoint of the incision was demarcated when determining the red injection dots, the proximal and distal dots were marked at 2 cm intervals from this midpoint, and additionally, the first web space was marked).
The first metatarsal medial proximal injection point was entered vertically with a 27-gauge needle, the first metatarsal cortex was felt, the needle was slightly withdrawn, and 2 mL of solution was administered to this area. Then, the needle was moved to the plantar and dorsal parts of the first metatarsal, targeting the subperiosteal area, and 3 mL of solution was administered to these areas (Figure 2). The same procedure was applied to the 3 designated points. Subsequently, 2 mL was applied between the first and second metatarsal heads for adductor tenotomy. The primary surgeon performed the WALANT in the waiting room, without the anesthesia team, approximately 30 minutes before the incision, starting from the most proximal area and moving toward the distal. Spinal anesthesia was performed by the anesthesia team using hyperbaric bupivacaine according to standard institutional protocols.
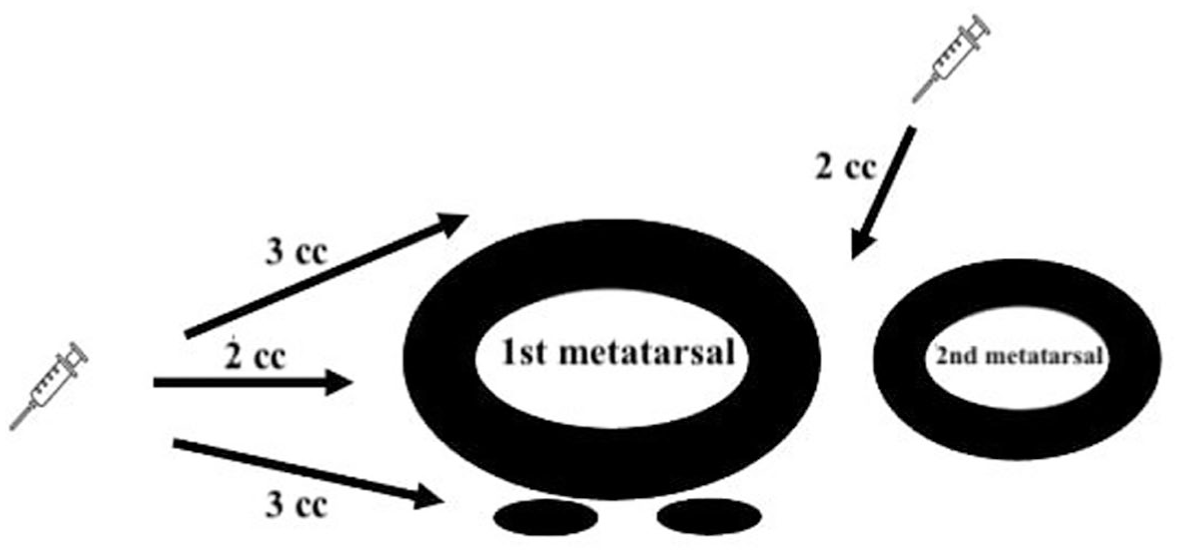
Schematic illustration of WALANT application (4 cc is applied to the subcutaneous incision area, 2 cc to the first metatarsal medial, 3 cc each to the first metatarsal dorsal and plantar, and 2 cc to the first web space).
Statistical Analysis
Data analysis was performed using IBM SPSS 25.0 (Armonk, New York: IBM Corp) and MedCalc 15.8 (MedCalc Software bvba, Ostend, Belgium) statistical package programs. While evaluating the study data, descriptive statistical methods (frequency, percentage, mean, standard deviation, median, min-max) and chi-square (χ2) test were used for comparing qualitative data. The conformity of the data to normal distribution was assessed using the Kolmogorov-Smirnov test, skewness-kurtosis, and graphical methods (histogram, Q-Q Plot, Stem and Leaf, Boxplot). In the study, an independent samples t-test was used for comparing normally distributed quantitative data between groups, a paired samples t-test for comparing within groups, a Mann-Whitney U test for comparing data that did not show normal distribution between groups, and Friedman’s test for comparing within groups. The Bonferroni correction was applied in cases where differences were found in multiple comparisons. The statistical significance level was accepted as P = .05.
Results
In total, 66.3% (n = 55) of the patients were female. The mean age was 36.4 ± 7.7, and the mean body mass index was 23.8 ± 2.2. The left side was affected in 50.6% (n = 42) of the patients. The mean follow-up time was 16.8 ± 4.3 months. The detailed properties were given in Table 1.
The Preoperative and Postoperative Properties of the Patients.
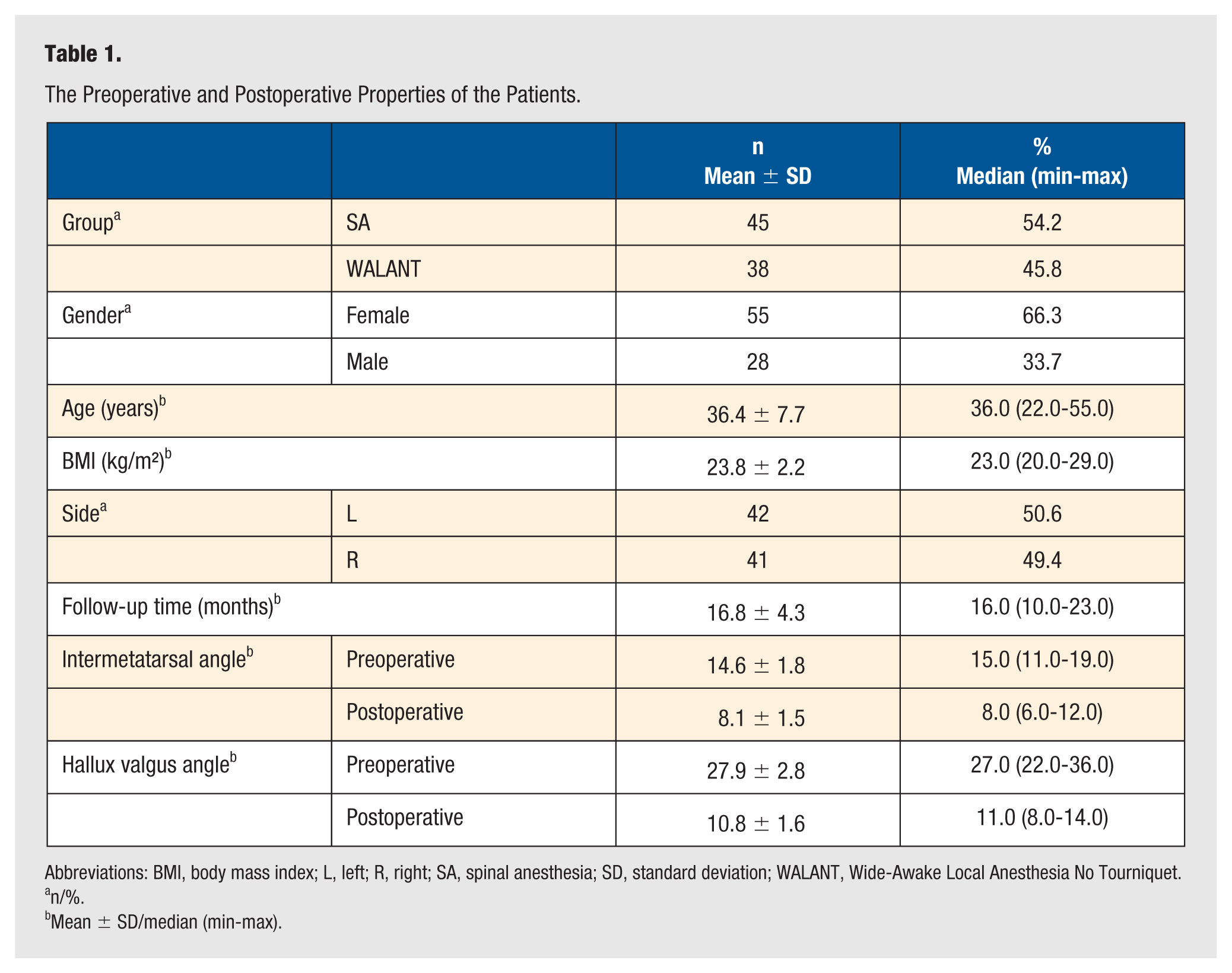
Abbreviations: BMI, body mass index; L, left; R, right; SA, spinal anesthesia; SD, standard deviation; WALANT, Wide-Awake Local Anesthesia No Tourniquet.
n/%.
Mean ± SD/median (min-max).
The mean age in the WALANT group was younger, and the preoperative preparation time and hospital stay were shorter than in the SA group (P < .001). While consultations were needed to evaluate anesthesia and other comorbid diseases in the SA group, routine preoperative laboratory values were generally sufficient in the WALANT group. The VAS values at the first, sixth, and 72nd hours after surgery were lower in the WALANT group (respectively, P < .001, P = .001, P < .005). Intraoperative VAS-A values were higher in the WALANT group (P < .001), while postoperative VAS-A values at the sixth hour were lower compared to the SA group (P < .001) (Figure 3).
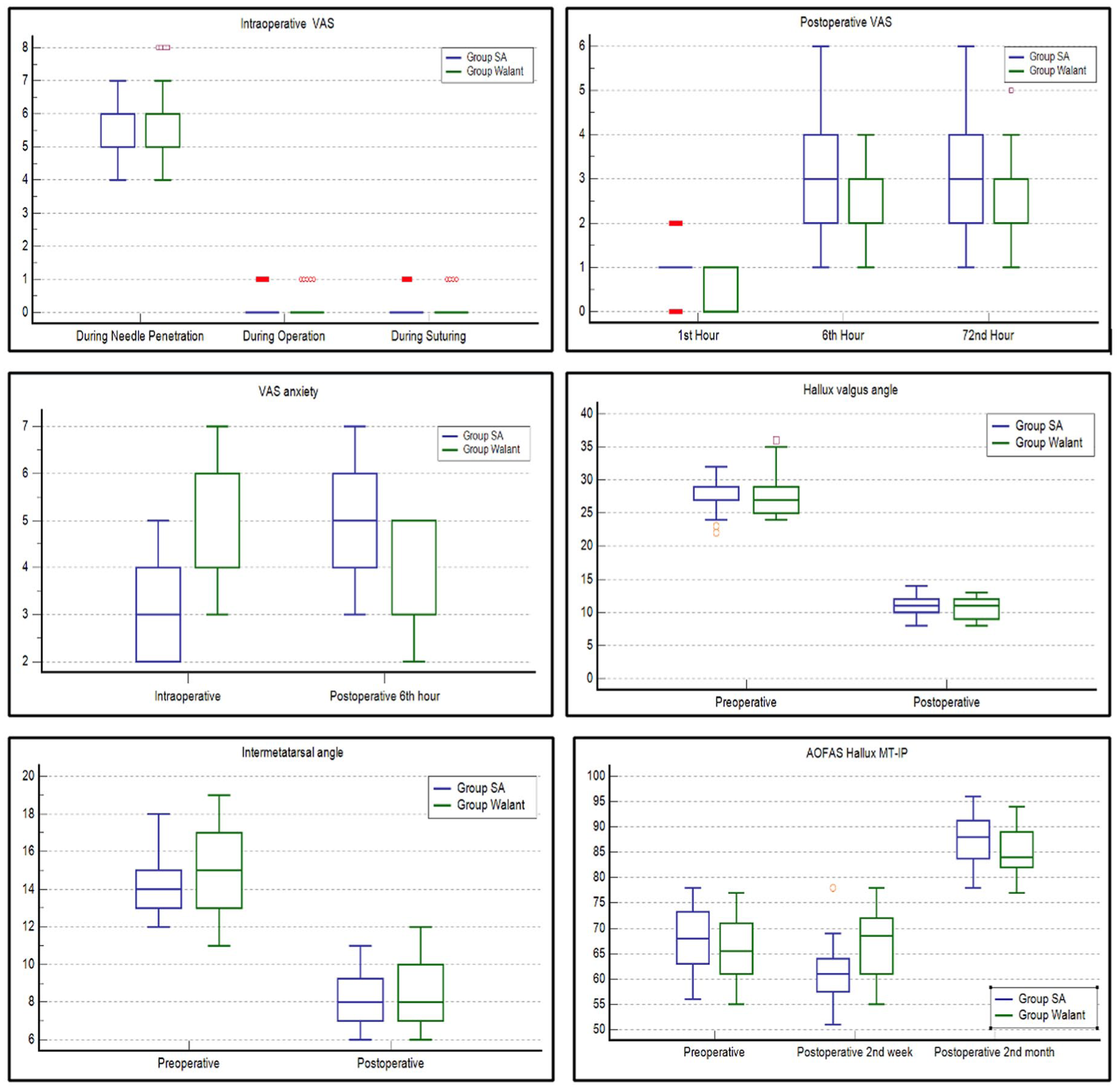
Comparison between groups.
Preoperative patient-preparation time was shorter in the WALANT group than in the SA group (P < .001) (Figure 3). No difference was observed between the 2 groups in terms of surgery time (P = .226).
In the SA group, 8 patients had transient thigh pain due to the tourniquet, 1 patient had swelling in the surgical area, and 1 patient had headache (for 12 days) due to SA. In the WALANT group, 2 patients had swelling in the surgical area and were discharged on the first postoperative day. Vasovagal problems due to WALANT were not observed in any patient.
There were 28 active working patients in the SA group and 26 in the WALANT group. In the WALANT group, AOFAS Hallux MT-IP postoperative second-week values were found to be higher (P = .000), and the time to return to work was shorter than in the SA group (P < .001). There was no significant difference between the groups in terms of other variables (P > .05) (Table 2 and Figure 3).
The Comparisons Between Groups.
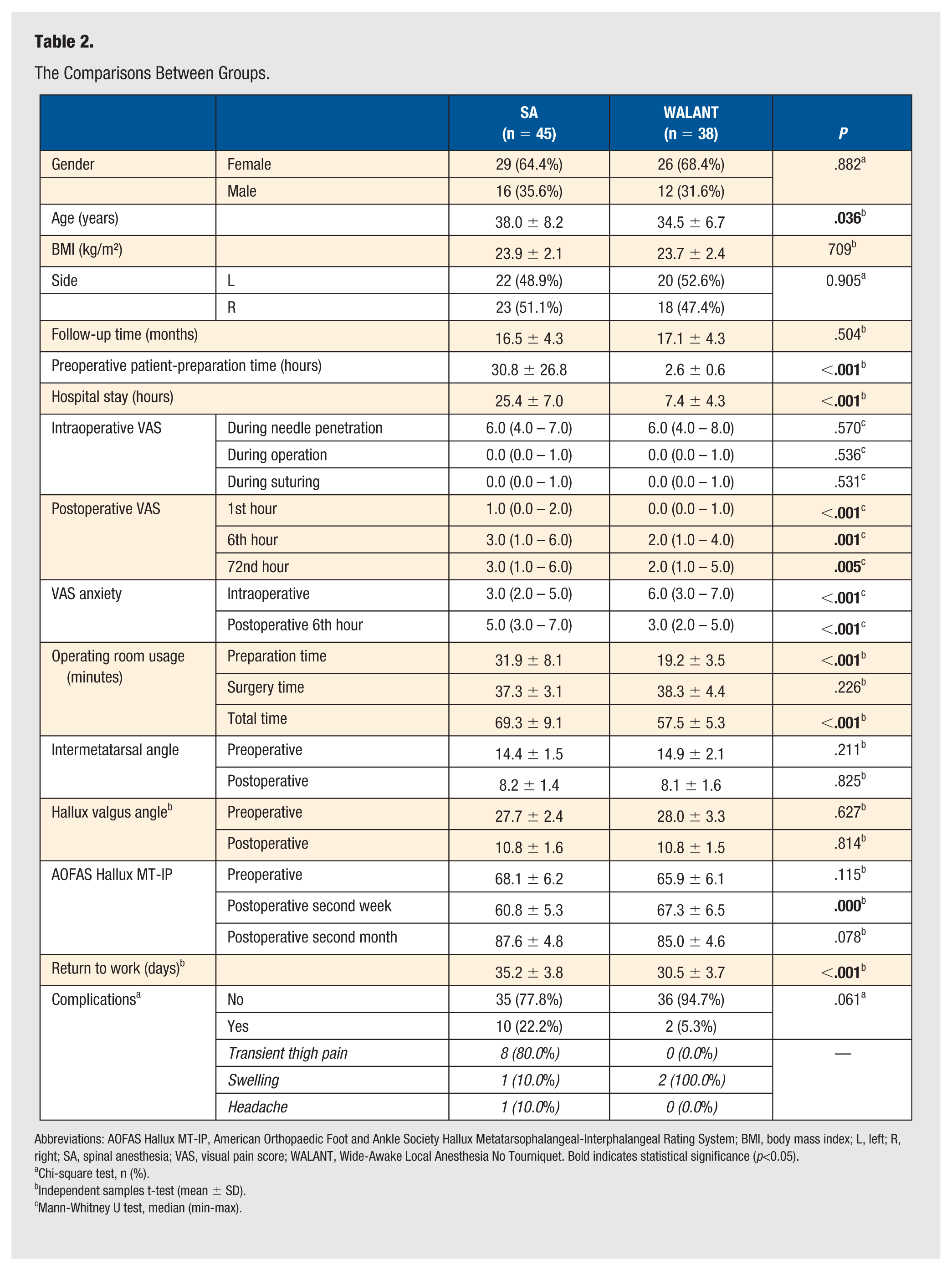
Abbreviations: AOFAS Hallux MT-IP, American Orthopaedic Foot and Ankle Society Hallux Metatarsophalangeal-Interphalangeal Rating System; BMI, body mass index; L, left; R, right; SA, spinal anesthesia; VAS, visual pain score; WALANT, Wide-Awake Local Anesthesia No Tourniquet. Bold indicates statistical significance (p<0.05).
Chi-square test, n (%).
Independent samples t-test (mean ± SD).
Mann-Whitney U test, median (min-max).
There was no difference in preoperative and postoperative IMA and HVA between the 2 groups (P > .05). There was also no difference in complications between the 2 groups (P > .05).
Discussion
This study showed that the WALANT technique might be more advantageous than SA as an anesthesia method in HV surgery. Preoperative preparation time, hospital stay, total operation time, and return to work time were shorter in the WALANT group than in SA. In addition, postoperative VAS and VAS-A values and postoperative complications were lower in the WALANT group than in SA. In this study, the application technique of WALANT in HV surgery was defined, and various advantages of this technique compared to SA were demonstrated. This study has the largest sample compared to the limited examples in the literature and has shown the reliability of the WALANT technique in lower extremity surgeries.
In contemporary hand and extremity surgery, regional anesthesia remains widely accepted as the standard anesthetic technique due to its predictable analgesic efficacy and surgeon familiarity. 7 However, the WALANT technique has gained increasing attention as a safe and effective alternative in selected procedures. Compared with regional anesthesia, WALANT eliminates the need for sedation, reduces anesthesia-related systemic risks, shortens recovery time, and allows real-time intraoperative functional assessment, which may improve surgical precision in tendon and ligament procedures. Several recent studies have demonstrated comparable pain control, complication rates, and patient satisfaction between WALANT and regional anesthesia, while highlighting potential advantages such as lower cost, avoidance of tourniquet discomfort, and feasibility in outpatient settings.8-12 Nevertheless, regional anesthesia continues to be preferred in longer and more complex procedures, and careful patient selection remains essential when considering WALANT. Therefore, WALANT should not be viewed as a replacement for regional anesthesia but rather as a complementary technique with specific clinical advantages in appropriately selected cases. In the context of lower extremity surgery, the findings of the present study should be interpreted specifically for elective HV surgery, which represents a relatively limited soft tissue procedure and osteotomies with moderate operative duration. Therefore, WALANT may not be generalizable to all lower extremity operations, particularly more complex reconstructive procedures requiring extensive dissection or prolonged operative time. In appropriately selected cases, WALANT may provide important advantages compared with spinal or regional anesthesia. Such cases may include cooperative patients undergoing elective forefoot procedures with limited surgical exposure, lower expected postoperative pain burden, and a desire for shorter hospitalization or avoidance of systemic anesthetic risks. Conversely, regional or SA may remain preferable in patients with severe anxiety, anticipated prolonged surgery, or complex hindfoot and ankle procedures requiring extensive intraoperative manipulation.
It has been reported that surgeries with WALANT reduce hospital stay and treatment costs and facilitate surgical preparations in upper extremity and hand surgery.9,13 In this current study, hospital stay and preoperative patient-preparation time were lower in the WALANT group. Although cost analysis was not performed in this study, it is presumed that the cost would be lower in the WALANT group due to the lack of preoperative consultations from other specialties, no need for an anesthesia team, and the short hospital stay.
There was no difference between the 2 groups regarding pain scores during WALANT and SA applications. MacNeill and Mayich 14 reported mild pain during the first anesthetic injection and little or no pain during subsequent injections during the WALANT application. The present study found no difference between the 2 groups intraoperatively. However, patients in the WALANT group generally reported that they could feel pressure or movement in the surgical area.
It has been shown that patients who underwent WALANT had less pain than SA in the early postoperative period of HV bone surgeries. 15 Again, Wright et al 16 observed less postoperative pain in the WALANT group in a study comparing patients who underwent general anesthesia and WALANT in forefoot surgery. In this current study, pain was also lower in the WALANT group than in the SA group in the first 3 postoperative days.
In forefoot and HV surgeries performed with the WALANT technique, patient anxiety scores were found to be lower in the WALANT method compared to the SA group.15,16 However, the intraoperative anxiety level of the WALANT group was found to be higher than that of the SA group. This was probably due to the fact that the patient was fully awake, heard the sounds resulting from the surgical procedure during surgery, and felt pressure and movement in the surgical area. However, interestingly, in this current study, the postoperative VAS-A score was found to be lower in the WALANT group than in the SA group.
Seretis et al compared the “total operation time” and “operating room usage time” in the WALANT group and the general anesthesia group in frequently performed plastic surgery operations in the upper extremity. Although no difference was found in total operation time, the operating room usage time was higher in the general anesthesia group. 17 In another study comparing axillary block and WALANT in carpal tunnel surgery, no difference was found in total operation time. 18 In this current study, similar to the literature, no difference was found between the 2 groups in operation time. In contrast, the operating room usage time was shorter in the WALANT group than in the SA group. The reason for this difference is that SA was performed in the operating room, whereas the WALANT procedure and its effect were performed in the waiting “preparation room.” Nevertheless, it can be said that the reduction in the operating room usage time of the WALANT application is positive for surgeons.
Torun et al 19 reported that the hospital stay was shorter in patients with distal radius fracture operated under WALANT compared to the infraclavicular block. In this study, the duration of hospital stay was shorter in the WALANT group. Regardless of the type of surgery, patients who underwent SA in our country are usually followed at least 1 day to follow-up for possible complications.
Kir and Kir 20 compared patients with HV who underwent general anesthesia with those who underwent ankle nerve block in addition to general anesthesia, and they could not detect a difference between the AOFAS HV MT-IP scores at different times postoperatively between the 2 groups. In this present study, while the AOFAS value was found to be better in the WALANT group in the second postoperative week than in the SA group, no difference was found between the groups in the second postoperative month.
The return to the work period was shorter in the WALANT group compared to the SA group. In the literature, the average return to work after HV surgery is 45 days. 21 In this current study, the average was found to be 30.5 days in the WALANT group and 35.2 days in the SA group. The fact that the treatment was daily in the WALANT group may have accelerated the patients’ return to their previous daily lives.
The use of tourniquets in lower extremity surgeries has been reported to be associated with muscle pain, loss of joint range of motion, prolonged hospital stay, and nerve damage.22,23 In this current study, more early complications were observed in the SA group compared to the WALANT group. This situation showed that WALANT is also safe in terms of early complications.
Both groups achieved the desired results in terms of IMA and HVA postoperatively, and the surgeons’ intraoperative time was not affected by these 2 types of anesthesia. However, this may be the subject of another study.
This study has some limitations. First, this study is a retrospective study. Although patient data were meticulously collected preoperatively and postoperatively, prospectively designed studies may increase reliability on this subject. Since there is no need for an anesthesia team for WALANT, it is thought to have lower costs; in this study, an objective cost analysis was not performed. The study focused on the suitability of WALANT for HV surgery and its effect on the pain of patients in the early postoperative period. The time to return to work was investigated as a functional outcome, but this is a limitation of the study, as it may vary according to the type of surgical technique.
Conclusion
The WALANT technique in HV surgery is a method that can be easily applied, is safe, and is not inferior to SA in terms of clinical results. The WALANT can be used in upper extremity surgeries and lower extremity surgeries with limited dissection. The WALANT shortens preoperative patient-preparation time, hospital stay, operating room usage, and return to work time after HV surgery. It improves functional and clinical results with low postoperative complication rates. However, there is a need for more extensive prospective randomized controlled studies in the future to determine the optimal anesthesia method.
Footnotes
Acknowledgements
None.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The institution’s ethics committee approval is obtained for the study (approval no.: 2024-704, dated: September 4, 2024) by the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from all included patients.
Data Availability Statement
Data and materials are available from the corresponding author on reasonable request.