
Abstract
Background:
The purpose of this study was to examine the effect of oral versus intravenous (IV) rehydration during exercise in the heat on exercise performance and physiological responses.
Hypothesis:
Oral rehydration will lead to better performance and physiological outcomes.
Study Design:
Cross-over study.
Level of Evidence:
Level 2.
Methods:
A total of recreational active men (age, 29 ± 12 years; peak oxygen consumption [VO2peak], 49.8 ± 6.6 ml kg−1 min−1) performed 90 minutes of cycling exercise at 55% watts at VO2peak (WVO2peak) followed by a 12-km time trial in the heat (34.9 ± 0.6°C; 30.3 ± 0.9%; wind speed, 3.4 m sec−1). Two experimental trials were performed in random order: (1) drank 25 ml of water every 5 minutes (ORAL) and (2) 25 ml of isotonic saline infused intravenously every 5 minutes (IV). Rectal temperature (Trec) and thirst sensation were measured every 5 minutes. Urine specific gravity (USG) and body mass loss were measured before and after trials. Changes (Δ) were calculated based on the resting value for each trial.
Results:
Participants started both trials euhydrated (USG < 1.020), and no differences were found in hydration status between ORAL and IV after trials (USG:ORAL, 1.012 ± 0.006; P = 0.14; IV, 1.013 ± 0.007; body mass loss: ORAL, 2.4 ± 0.8%; IV, 2.3 ± 0.5%, P = 0.68). Thirst levels were higher in IV than ORAL from 20 to 50 minutes (P = 0.03 to 0.05) and after 65 minutes throughout 90 minutes of cycling exercise and the 12-km time trial (P < 0.001 to 0.04). ΔTrec was also significantly higher in IV after 20 minutes throughout 90 minutes of cycling exercise and a 12-km time trial (P = 0.003 to 0.04). The time trial was significantly faster in ORAL (17.7 ± 4.6 minutes) compared with IV (19.6 ± 6.2 minutes, P = 0.05).
Conclusion:
Oral rehydration enhances exercise performance and decreases Trec and heartrate compared with IV rehydration.
Clinical Relevance:
Oral rehydration might have more benefits than IV in exercise performance and physiological response.
Dehydration increases cardiovascular and thermoregulatory strain and impairs exercise performance, and these negative effects are exaggerated during exercise in the heat.1,10 Proper fluid intake is important to maintain optimal fluid balance and prevent the negative impact of dehydration. 18 Thirst is a vital signal to maintain homeostasis and regulate total fluid volume in response to dehydration, increased plasma osmolality, decreased plasma volume, and decreased blood pressure. 2 The osmoreceptors that control thirst also regulate the secretion of arginine vasopressin (AVP)—a key hormone to maintain fluid balance. 17 However, thirst sensation and AVP concentration can be suppressed after fluid intake before dehydration is recovered and plasma osmolality and plasma volume return to normal levels, by activating the oropharyngeal receptors. 9
The oropharyngeal region plays an important role in drinking behaviors. When dehydrated, it provides a signal for drinking by activating the thirst drive. 9 During drinking, the act of swallowing activates the oropharyngeal receptors, causing suppression of thirst sensation and AVP. 9 Based on those responses, the oropharyngeal region acts as the oropharyngeal metering to limit fluid intake and prevent overdrinking. 9 A previous study showed that time trial performance in the heat was improved when a small amount of water was ingested compared with the control group and mouth rinse. 4 Therefore, it is suggested that the oral fluid replacement, due potentially to the oropharyngeal reflex and lowering thirst sensation, might hold benefits. 5
A few studies investigated the effect of oral versus intravenous (IV) rehydration on exercise performance and/or physiological responses.6,8,13 Casa et al 6 indicated that there were no differences in the time to exhaustion test after the oral versus IV rehydration (0.45% NaCl) from 4% dehydration. Furthermore, Kenefick et al 13 demonstrated that physiological and thermoregulatory strain (i.e., heartrate [HR], core temperature) and time to exhaustion performance were similar between the oral versus IV (0.45% saline). These 2 studies implemented 2 different rehydration methods (oral vs IV) during the recovery period after exercise-induced dehydration.6,13 On the contrary, Cheung et al 8 investigated the effect of 2 rehydration methods during exercise and found no differences in 20-km cycling time trial performance in the heat while thirst was manipulated by providing or withholding mouth rinse in both euhydrated and dehydrated states. However, due to the purpose of this previous study, Cheung et al 8 did not control the amount of fluid intake in the same mouth rinse group, and, therefore, the effect of oral versus IV rehydration during exercise remains unclear. While the oral rehydration could be the practical method during exercise, this provides an insight to understand how thirst levels and/or oropharyngeal activation could impact exercise due to different rehydration methods, as suggested previously. 5
While the impact of dehydration on exercise performance, especially in the heat, is well documented, the roles of oral versus IV rehydration and subsequent thirst sensation remain unclear, especially when matching fluid intake and hydration status. This is an important consideration as frequent oral fluid intake to suppress thirst, which induces oropharyngeal reflexes, could be critical, along with the total amount of fluid replacement to prevent excessive dehydration. Therefore, the purpose of this study was to examine the effect of oral versus IV rehydration during exercise in the heat on exercise performance and physiological responses when matching hydration status. We hypothesized that oral rehydration holds benefits as time trial performance would be better using oral rehydration, possibly due to factors related to drinking behavior.
Methods
A total of 12 recreational active male participants (mean ± SD: age, 29 ± 12 years; body mass, 74.7 ± 7.9 kg; height, 179.4 ± 7.0 cm; peak oxygen consumption [VO2peak], 49.8 ± 6.6 ml kg−1 min−1) took part in this study. A power analysis with G*Power Version 3.1.9.6 (Heinrich Heine University Düsseldorf) was conducted to determine the sample size from a previous study looking at the effect of IV versus oral rehydration on subsequent exercise in the heat. 7 Exercise time was used as the parameter (77.4 ± 5.4 minutes vs 84.2 ± 2.3 minutes), and a minimum of 6 participants was needed for an alpha level of 0.05, a power level of 0.8, and an effect size of 1.6 based on the previous study. 7 Exclusion criteria included having a current musculoskeletal injury, chronic health problems affecting the ability to thermoregulate, a history of heat illness, cardiovascular and metabolic, or respiratory disease, and currently taking a medication that influences body temperature. After an explanation of study procedures, which was approved by the institutional review board (IRB), participants provided written and informed consent to take part in this study; the ethical approval number is IRB2021-642, and the study was conducted according to the Declaration of Helsinki. This study was conducted at Texas Tech University and recreational active men were recruited from the local community for the participants.
First, participants performed a VO2peak test on an electronically braked cycle ergometer (Excalibur Sport). On arrival, participants provided urine samples for assessment of their hydration status to ensure they began the VO2peak test in a euhydrated state (urine specific gravity [USG] < 1.020). Then, participants performed a 5-minute self-selected pace warm-up. After the warm-up, participants completed a graded cycling exercise. Power was set at 150 W and increased by 50 W every 2 minutes until volitional exhaustion (TrueOne Metabolic Measurement System, Parvo Medics Inc). Oxygen consumption, respiratory exchange ratio, HR, and rating of perceived exertion (RPE) were collected every 2 minutes. VO2peak and watts at VO2peak (WVO2peak) were determined to calculate exercise intensity for exercise trials.
All participants completed 2 experimental trials on 2 separate visits. Participants were instructed to consume fluid throughout the day (e.g., 500 ml extra water intake) to be euhydrated, and not to perform exercise on the day of the trials and intense exercise the day before the trials. Upon arrival at the laboratory, a urine sample was collected to assess hydration status, and trials were performed when USG (digital urine specific gravity refractometer, Atago) was <1.020. Urine color and urine osmolality (Osmo Pro, Advance Instruments Inc) were also analyzed. 3 After urine collection, nude body mass was measured before the exercise trial (PRE). Participants inserted a rectal thermistor (YSI probe, MP160; Biopac Systems Inc) 10 cm past the anal sphincter to measure core temperature (Trec). Wireless skin temperature sensors were attached to the chest, upper arm, thigh, and calf to calculate mean skin temperature (Tsk) (iButton, iButton Link LLC). 15 HR (H10, Polar Electro) was recorded by wireless HR monitor. Before entering the environmentally controlled heat chamber, blood was drawn by a cannula for the IV rehydration trial and venipuncture for the oral rehydration trial from an antecubital vein while participants were seated to assess serum osmolality. For the IV rehydration trial, after the blood was drawn from the cannula, the IV was inserted and the infusion pump was set to infuse isotonic saline during exercise. Two experimental trials were performed in random order: (1) participants drank 25 ml of water every 5 minutes (ORAL), and (2) participants were infused intravenously with 25 ml of isotonic saline (NaCl 0.9%) every 5 minutes (IV). The IV cannula was inserted only in the IV trial; however, participants understood that the amount of fluid intake was the same between the 2 interventions. Water and saline temperatures were thermoneutral at room temperature (20°C to 22°C) with the total amount ingested or infused being 625 ml. ORAL and IV trials were performed at 13:17 (±0.1 minute) and 12:55 (±0.1 minute), respectively.
After participants entered the heat chamber, they completed a 15-minute equilibrium period. After equilibrium, participants performed a steady-state cycling exercise at 55% WVO2peak for 90 minutes in the heat (ambient temperature, 34.9 ± 0.6°C; relative humidity, 30.3 ± 0.9%; wind speed, 3.4 m sec–1). During exercise, Trec, HR, and Tsk were measured every 5 minutes, and RPE, thermal sensation, fatigue level, and perceived recovery were collected every 15 minutes using a Likert scale. Thirst sensation was measured every 5 minutes using visual analog scales comprising a 180-mm line with an anchor on the left side (0 mm, “not at all”) and a second anchor on the 125-mm mark with the label “extremely.” The assessment of thirst sensation was done before drinking water to avoid the acute impact of drinking. Thirst levels are presented as percent of maximum values (100%) based on the extremely thirsty at the 125-mm value. This procedure was based on the previous study. 1 After 90 minutes of exercise, nude body mass was collected, and a blood draw was performed (MID) in the seated position while participants were still in the artificial heat chamber. Then, participants performed a 12-km cycling time trial (wind speed, 3.4 m sec–1). Participants were instructed to complete 12 km of cycling as fast as possible, and performance incentives (money) were provided as part of subject compensation. During the time trial, participants could see power output, revolutions per minute, and time, and the remaining distance was informed every 4 km while they changed in cadence to control load and Watts. After the time trial, nude body mass measurement, blood draw with the seated position and urine collection were completed (POST). The sweat rate was calculated from the following equation: (PRE body mass – MID body mass + fluid intake – urine) *60 *90 min–1 (L* h–1). However, no participants urinated during the exercise trials.
Data are reported as means and standard deviations; Δ was calculated as the change from the resting value for each trial for Trec, HR, and Tsk for physiological responses, as well as serum osmolality compared with PRE values. Two-way repeated measures analysis of variance with least significant difference post hoc test examined differences in urine osmolality, USG, urine color, serum osmolality, Trec, Tsk, HR, thirst level, RPE, thermal sensation, fatigue level, and perceived recovery between ORAL versus IV throughout each trial. 19 A paired t test was used to assess the difference in time trial measurements, sweat rate, and baseline raw physiological measures (i.e., Trec, HR, and Tsk) between ORAL and IV. All statistical analyses were completed using SPSS Statistics (Version 29.0; IBM Corp) with a significance set at P < 0.05.
Results
Table 1 shows urine and blood measurements. There are no interactions between trials and timepoints, and the main effect of trials in urine osmolality (interaction, P = 0.58; main effect, P = 0.86), USG (interaction, P = 0.14; main effect, P = 0.87), and urine color (interaction, P = 0.10; main effect, P = 0.58). There are significant interactions between trials and timepoints in serum osmolality (P = 0.03). Serum osmolality at PRE was higher in ORAL compared with IV (P = 0.03); however, both ORAL and IV values indicate euhydration (<290 mmol kg–1). 18 There were no differences in serum osmolality at MID (P = 0.45) and POST (P = 0.22) between ORAL and IV; Δ serum osmolality did not have the significant interactions between trials and timepoints (P = 0.10), while there was the main effect of trials (P = 0.04), with the IV being 1.3% greater than the ORAL. The sweat rate during 90 minutes of cycling exercise in ORAL (1.2 ± 0.4 l h–1) and IV (1.2 ± 0.4 l h–1; P = 0.28) was not different. In addition, there are no interactions (P = 0.68) between trials and timepoints, and the main effect of trial (P = 0.57) in relative body mass loss (MID:ORAL, 1.7 ± 0.7%; IV, 1.6 ± 0.7%; POST:ORAL, 2.4 ± 0.8%; IV, 2.3 ± 0.5%).
Urine and blood markers a
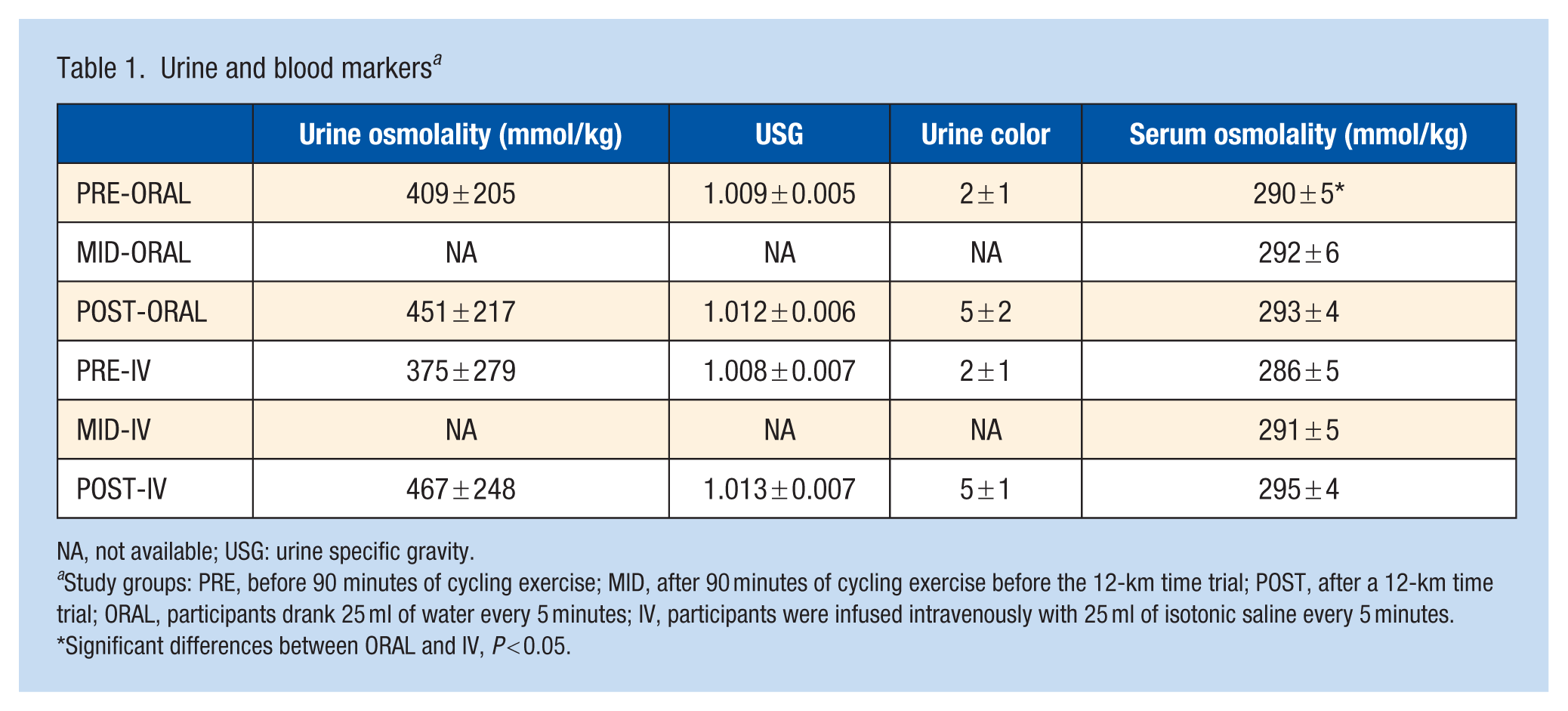
NA, not available; USG: urine specific gravity.
Study groups: PRE, before 90 minutes of cycling exercise; MID, after 90 minutes of cycling exercise before the 12-km time trial; POST, after a 12-km time trial; ORAL, participants drank 25 ml of water every 5 minutes; IV, participants were infused intravenously with 25 ml of isotonic saline every 5 minutes.
Significant differences between ORAL and IV, P < 0.05.
There were significant interactions between trials and timepoints in thirst levels (P = 0.05), ΔTrec (P = 0.05), and ΔHR (P = 0.04). Thirst levels were significantly higher in IV than ORAL from 20 to 50 minutes (P = 0.03 to 0.05), and after 65 minutes throughout 90 minutes of cycling exercise and the 12-km time trial (P < 0.001 to 0.04) (Figure 1). ΔTrec was also significantly higher in IV than ORAL after 20 minutes throughout 90 minutes of cycling exercise and a 12-km time trial (P = 0.003 to 0.04) (Figure 2). ΔHR was significantly higher in IV compared with ORAL at 55 to 65 minutes (P = 0.02 to 0.05) and before the 12-km time trial started (P = 0.006) (Figure 3). However, there were no interactions between trials and timepoints in Δ Tsk (P = 0.24). At baseline, Trec was greater in ORAL (37.3 ± 0.2°C) compared with IV (37.2 ± 0.2°C; P = 0.009) while Tsk (ORAL, 35.4 ± 0.2°C; IV, 35.4 ± 0.3°C, P = 0.19) and HR (ORAL, 93 ± 12 bpm; IV, 98 ± 16 bpm, P = 0.11) were not different. There were no significant interactions between trials and timepoints, and the main effect of trials in RPE (interaction, P = 0.59; main effect, P = 0.40), thermal sensation (interaction, P = 0.26; main effect, P = 0.41), fatigue level (interaction, P = 0.09; main effect, P = 0.18), and perceived recovery (interaction, P = 0.93; main effect, P = 0.13). Finally, the time trial was significantly faster in ORAL (17.7 ± 4.6 minutes) compared with IV (19.6 ± 6.2 minutes, P = 0.05) (Figure 4).
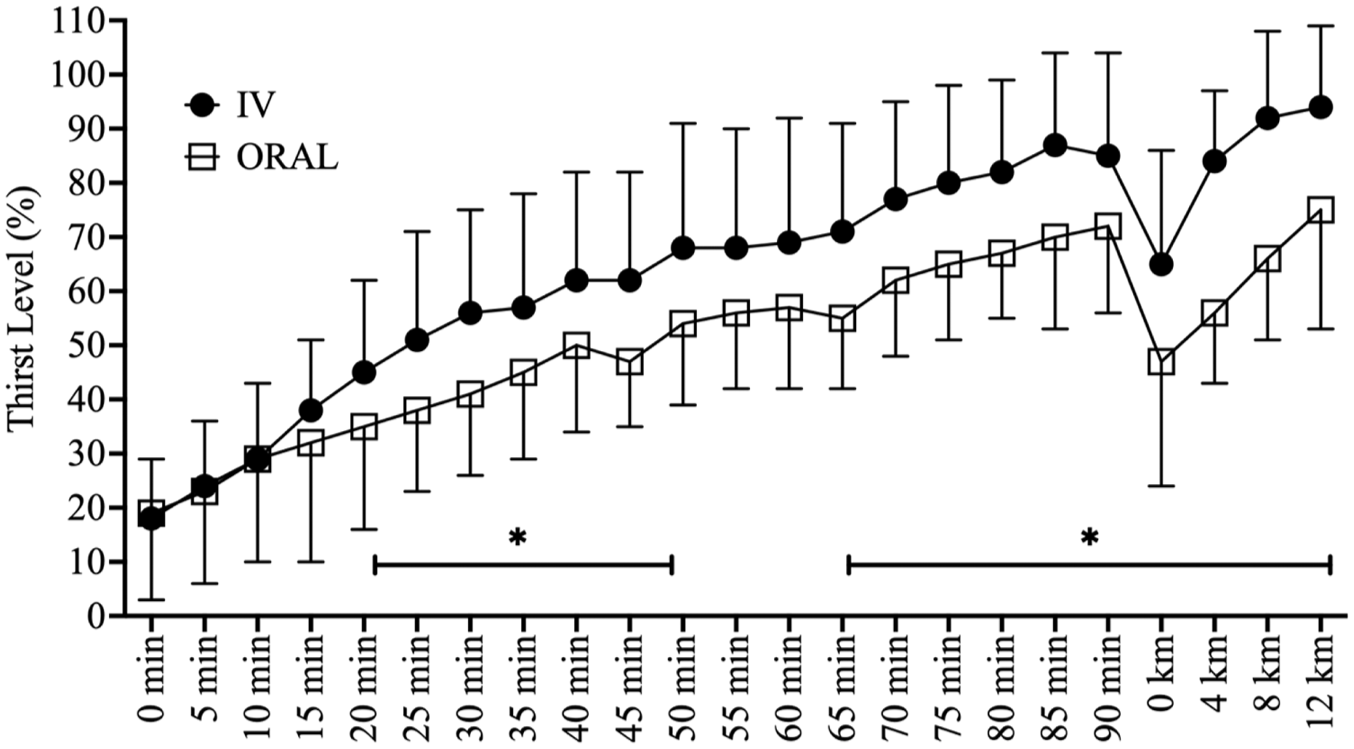
Thirst level for 90 minutes of cycling exercise and 12-km time trial. ORAL, participants drank 25 ml of water every 5 minutes. IV, participants were infused intravenously with 25 ml of isotonic saline every 5 minutes. *Significant differences between ORAL and IV (P < 0.05).
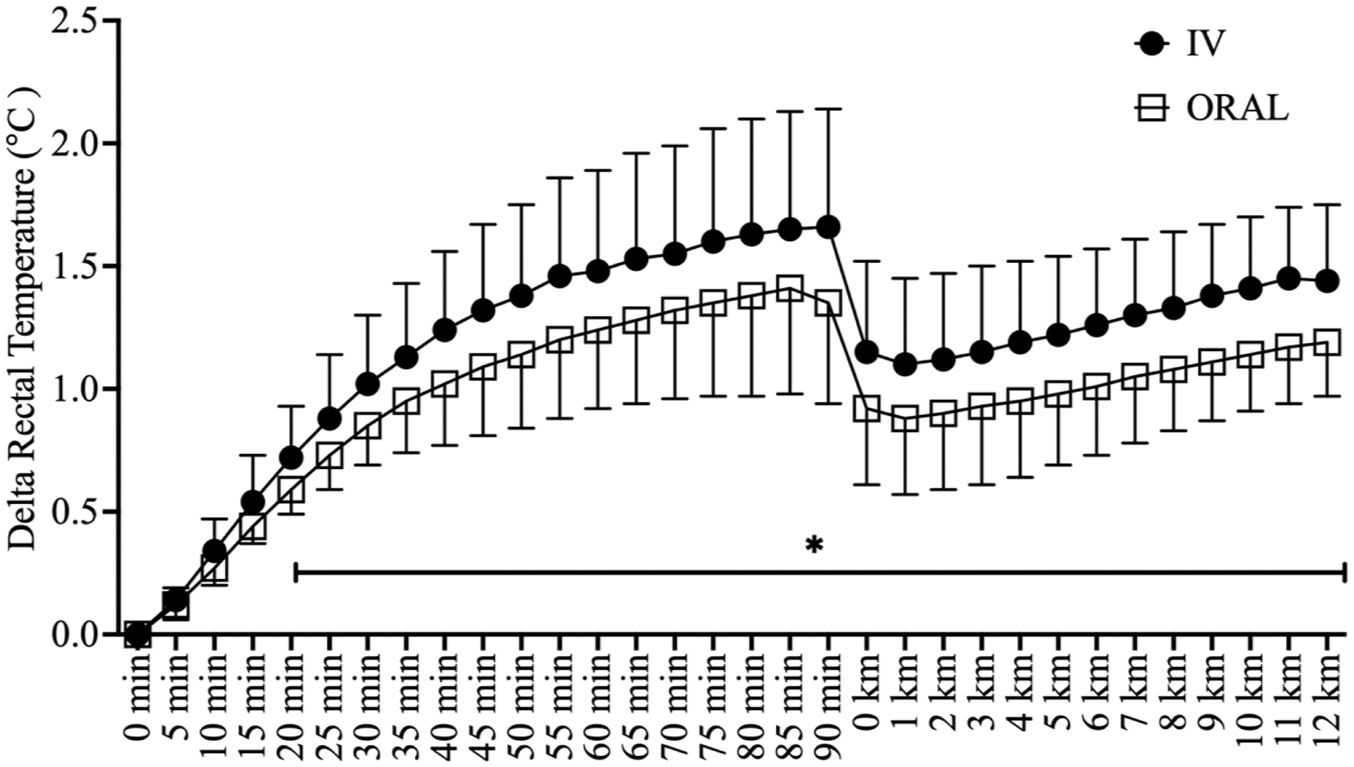
ΔTrec for 90 minutes of cycling exercise and 12-km time trial. ORAL, participants drank 25 ml of water every 5 minutes. IV, participants were infused intravenously with 25 ml of isotonic saline every 5 minutes. *Significant differences between ORAL and IV (P < 0.05). ΔTrec, changes in rectal temperature.
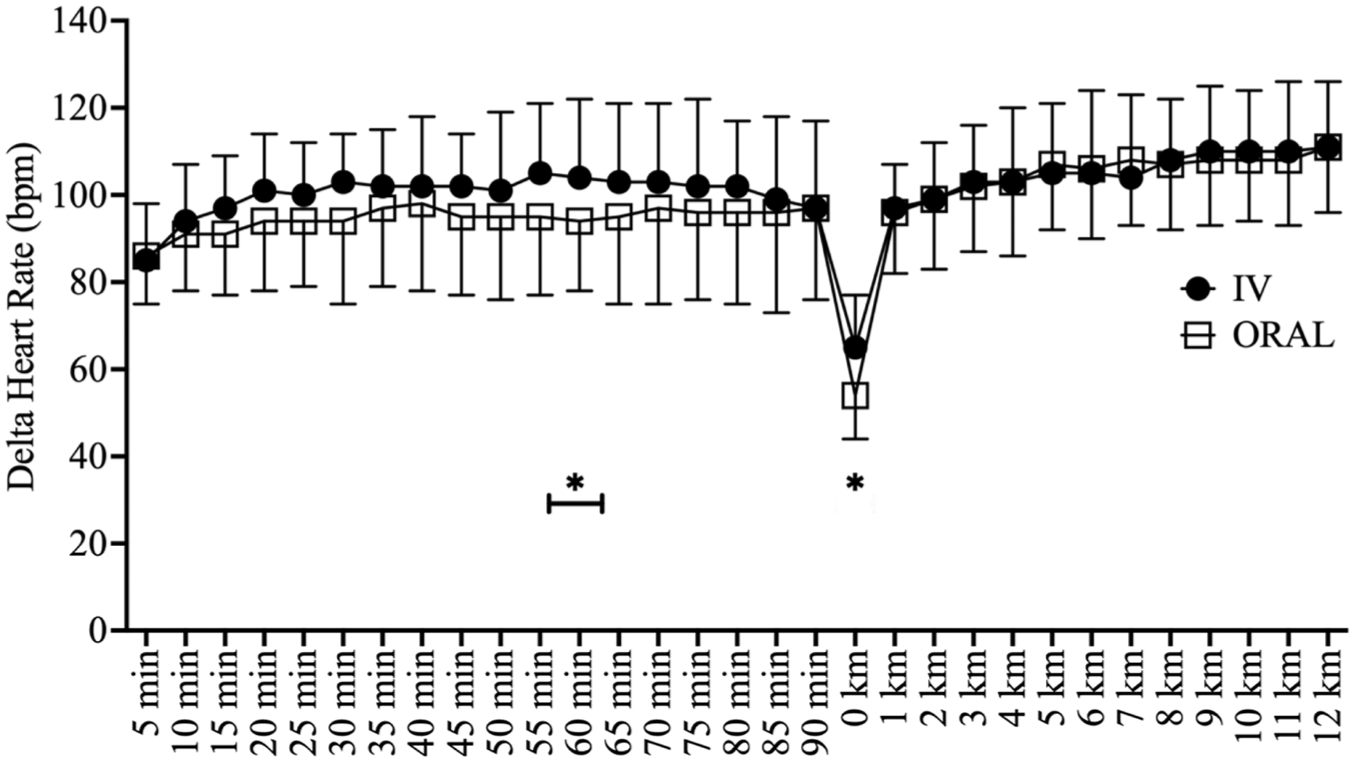
HR for 90 minutes of cycling exercise and 12-km time trial. ORAL, participants drank 25 ml of water every 5 minutes. IV, participants were infused intravenously with 25 ml of isotonic saline every 5 minutes. *Significant differences between ORAL and IV (P < 0.05). HR, heartrate.
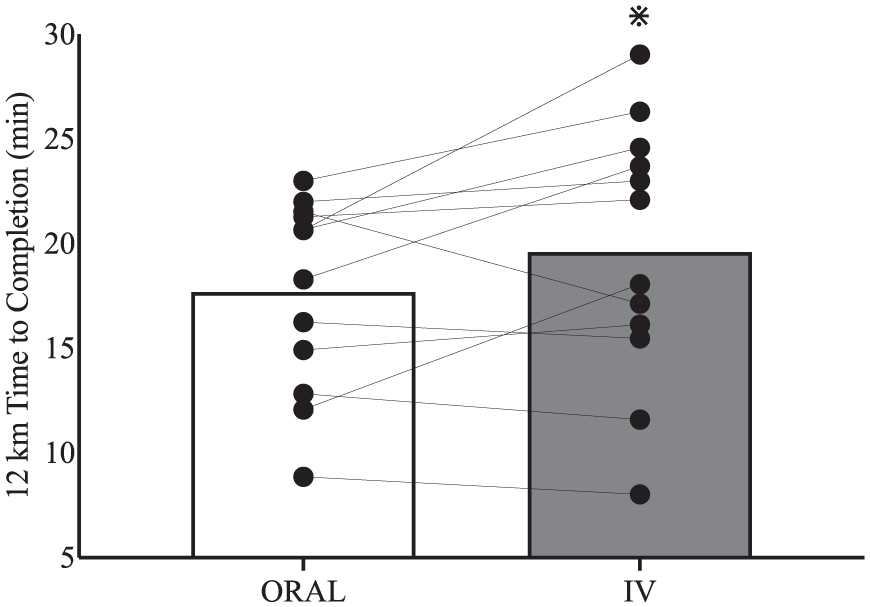
Performance in 12-km cycling time trial. ORAL, participants drank 25 ml of water every 5 minutes. IV, participants were infused intravenously with 25 ml of isotonic saline every 5 minutes. *Significant differences between ORAL and IV (P = 0.05).
Discussion
The purpose of this study was to examine the effect of oral versus IV rehydration during exercise on performance and physiological responses in the heat. This study found that when matching hydration status (urine indices, serum osmolality, and body mass loss between trials were classified in the same hydration status), oral rehydration increased exercise performance and decreased Trec and HR. In addition, IV rehydration induced a higher thirst sensation compared with oral rehydration. These results suggest that oral rehydration might have additional benefits compared with IV rehydration.
Oral rehydration decreased Trec and HR compared with IV rehydration during exercise. Casa et al 6 examined the effect of oral versus IV rehydration in dehydrated people and found that oral rehydration during rest led to lower Trec, HR, plasma glucose, and lactate, and higher stroke volume and sodium concentration in blood during subsequent exercise. While rehydration was not performed during exercise in this previous study, Casa et al 6 reported advantages of oral fluid intake similar to the current findings. However, Riebe et al 16 found conflicting results that there were no differences in Trec and HR during the subsequent exercise after oral or IV rehydration after dehydration. These findings were also similar to what Kenefick et al 12 presented, that Trec and HR were not different after the oral versus IV rehydration. In addition, Castellani et al 7 indicated that HR was higher during exercise in the heat after 2 hours of oral rehydration and rest compared with IV rehydration. Interestingly, Montain and Coyle 14 compared the effect of oral versus IV rehydration during exercise when controlling the blood volume, while the oral rehydration (1.1%) had a lower body mass change than the IV (3.4%). This previous study indicated that core body temperature was lower in the oral rehydration, and the change in blood volume was not responsible for this result. 14 They suggested that the oral ingestion maintained a higher skin blood flow, which reduced hyperthermia, by attenuating increased serum osmolality. 14 In the present study, while urine indices, serum osmolality, and body mass loss indicated the same hydration status between trials, the IV group increased 1.3% more in serum osmolality, probably due to the saline infusion compared with water ingestion in the ORAL group. While the current study did not measure metabolic heat production, skin blood flow might play a role in lower Trec, as sweat rate was similar between groups. Although Montain and Coyle 14 demonstrated that IV rehydration led to 3.6% greater serum osmolality than oral rehydration, IV rehydration achieved a dehydrated state while oral rehydration induced a euhydrated state. Therefore, a change in the serum osmolality could explain the difference in physiological responses; however, the reason for the difference is still unclear, as both ORAL and IV indicated the same hydration status in the current study. Regardless of the mechanisms leading to lower core body temperature with oral rehydration, it is well known that higher core temperature induces higher fatigue and lower exercise performance. 11 Consequently, this likely contributed to better time trial performance in ORAL compared with IV.
Greater exercise performance in the oral rehydration group from the current study was a finding similar to that of Arnaoutis et al, 4 investigating the effect of mouth rinse and a small amount of water ingestion during exercise on time to exhaustion performance. This previous study indicated that, even in small amounts, fluid ingestion enhanced performance compared with mouth rinse, possibly through the activation of oropharyngeal receptors, as mouth rinse did not activate them. 4 While this previous study did not control the amount of fluid intake, this possible mechanism might also explain why the oral rehydration improved time trial performance compared with IV in the current study. The findings by Cheung et al. also support this concept further. 8 This previous study investigated the effect of mouth rinse vs. no month rinse to control thirst sensation in both euhydrated and dehydrated states, which was managed by IV rehydration. 8 This study found that mouth rinse to lower thirst sensation does not change 20km time trial performance, Trec, and HR in the heat for both hydration status. 8 These studies emphasize that mouth rinse did not improve exercise performance and the importance of drinking.4,8 In addition, while the current study demonstrated that thirst levels were lower with the oral rehydration compared with the IV rehydration, the results of Cheung et al 8 support that differences in time trial performance, Trec, and HR between ORAL and IV observed in this study were not due to the differences in thirst levels. Moreover, the oral versus IV rehydration did not impact other subjective measurements, such as RPE, thermal sensation, fatigue level, and perceived recovery. This is a conflicting result to that of Riebe et al, 16 indicating RPE was lower during exercise after oral rehydration compared with IV. While Riebe et al 16 performed rehydration during resting, our results indicated that subjective effort and fatigue level did not impact time trial performance. Taken together, oropharyngeal activations might be one of the other potential factors that lead to superior performance in oral rehydration compared with IV rehydration, but not due to drinking-induced lower thirst sensation. 5
There were limitations in this study. First, the IV sham was not used in the ORAL group to minimize the discomfort for the participants; therefore, this might impact the current findings. In addition, due to the study design, participants knew the same amount of fluid intake was received for both interventions, and the amount of fluid intake was not blinded. Second, it was not clear whether thirst sensation and/or oropharyngeal stimulation impacted exercise performance and thermoregulatory and cardiovascular strain during exercise in the heat, as it was difficult to isolate the effects of thirst sensation and oropharyngeal reflexes due to the study design. Future study needs to investigate the independent effect of thirst sensation and oropharyngeal reflexes. Furthermore, thirst sensation was measured every 5 minutes, and there might be a carryover effect while the visual analogue scale was used instead of Likert scales to prevent this as much as possible. Next, isotonic saline was infused intravenously while water was ingested orally. Serum osmolality indicated the same hydration status between ORAL and IV throughout the study, but the change in serum osmolality was 1.3% greater in the IV compared with the ORAL group. This was probably because IV infused saline and ORAL ingested water, which is also a limitation of the study. In addition, other factors related to the methodological differences, such as gastric emptying and absorption, could impact the results. Furthermore, diet was not controlled, and this might impact energy balance, resulting in an exercise response. However, the 2 trials were performed at 13:17 (±0.1 minute) and 12:55 (±0.1 minute), respectively. Finally, there was no familiarization trial, but a random trial order was used to minimize this effect. There were also no differences between the first and second trials on time trial performance (P = 0.19), which indicated a minimal learning effect was found.
Conclusion
Independent of hydration status, oral rehydration increased exercise performance and decreased Trec and HR during exercise in the heat. These findings provided critical information on how oral rehydration changes physiological and performance markers while the amount of rehydration is the same between IV and oral fluid intake. In addition to determining the amount of fluid to consume to minimize dehydration and maintain optimal fluid balance, drinking itself might be an important factor, while mechanisms behind the current study, such as drinking-induced change in body heat exchange or oropharyngeal activations, need to be investigated in the future.
Footnotes
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Yahama Sport Challenge Grant.The following author declared potential conflicts of interest: S.A.K. is a lead research aerospace physiologist at Luke Air Force base and a member of the science advisory board for Hyduro Inc, Zico rising, and Rockley Photonics. He has served as an occasional scientific consultant for Danone Research and Kraft Heinz. S.A.K. has active grants with Danone Research and Standard Process.