
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are the most common knee ligament injuries and ACL reconstruction (ACLR) is often required to restore stability and facilitate return-to-sport. However, kinesiophobia—fear of movement due to risk of reinjury—is prevalent post-ACLR (62% to 78%) and linked to poor return-to-sport outcomes despite good physical recovery.
Hypothesis:
Patient, injury, surgery, and rehabilitation factors can be associated with elevated kinesiophobia in patients undergoing primary ACLR.
Study Design:
Retrospective cohort study.
Level of Evidence:
Level 3.
Methods:
A retrospective review was conducted using data from a tertiary acute hospital’s ACL registry between June 1, 2019 and June 1, 2023. Included were patients aged 18 years to 60 years undergoing primary ACLR. Exclusions were revision ACLR, multiligament injuries, and incomplete 1-year dataset. Demographics, injury/surgery/rehabilitation factors and patient-reported outcomes were measured preoperatively, and at 6 months and 1 year. Tampa Scale of Kinesiophobia-17 (TSK-17, with ≥37 indicating elevated kinesiophobia), was recorded preoperatively and 1 year postoperatively. Multivariate regression was used to identify predictors of elevated 1-year kinesiophobia.
Results:
Data from 200 patients were analyzed (8 excluded due to incomplete data). Baseline TSK-17 was 38.6 ± 5.6, improving to 32.6 ± 7.6 at 1 year (P < 0.001), with 59% showing elevated kinesiophobia at baseline and 29% at 1 year. The average TSK-17 reduction was 6.1 ± 8.6, meeting the minimal clinically important difference (MCID) level. Prehabilitation was attended by 106 patients (55.21%), with a median of 1 session (range 0-10). Elevated 1-year kinesiophobia was associated significantly with higher baseline TSK-17 scores (odds ratio [OR], 2.004; 95% CI, 1.013-3.968; P = 0.05) and inversely associated with attending ≥1 prehabilitation session (OR, 0.513; 95% CI, 0.264-0.997; P = 0.05).
Conclusion:
Prehabilitation before ACLR should be standard-of-care, to reduce risk of elevated kinesiophobia at 1-year.
Clinical Relevance:
High baseline kinesiophobia predicts sustained elevated 1-year kinesiophobia, hence assessment (TSK-17 scores) and early intervention targeting kinesiophobia should be included in preoperative ACLR protocols.
The anterior cruciate ligament (ACL) is the most commonly injured ligament in the knee. 21 An incompetent ACL can result in significant instability and reduced physical function. In particular, patients who suffer ACL injuries may be unable to return to pivoting sports. 52 In these patients, ACL reconstruction (ACLR) surgery can be performed to improve mechanical stability and potential return to sport (RTS). 14
Several well-defined variables, such as symmetry of quadriceps and hamstring strength, restoration of range of motion (ROM), and hop tests have been demonstrated to predict successful RTS. 19 However, it has been noted that some people with adequate physical recovery may still struggle with RTS, potentially due to a lack of psychological readiness. 40 In a cross-sectional study of 164 ACLR patients by Ardern et al, 3 poor psychological readiness (measured with the ACL Return-to-Sport after Injury [ACL-RSI] scale) was shown to be a consistently strong predictor (P < 0.001, odds ratio [OR] = 1.8) for poor RTS outcomes. One key aspect of this psychological readiness is that of kinesiophobia – defined as the fear of movement, often due to the fear of reinjury. 24 This psychological parameter has been studied heavily in several musculoskeletal injuries, including low back pain, knee arthroplasty, rotator cuff tears, and ACL injuries,7,22,28,32,38 and also in patients undergoing ACLR.2,10 The prevalence of kinesiophobia in patients with ACL injuries has been reported to range from 62% to 78%.2,45 Variables such as male sex, 41 or a longer time delay from injury to surgery, 46 have been identified as risk factors for kinesiophobia. The wide variance in kinesiophobia suggests that there may be other factors that influence kinesiophobia. It is important to identify these potentially modifiable factors as studies have shown that elevated kinesiophobia in ACLR patients is associated with poorer RTS rates and self-perceived function,35,40 even in cases where full physical knee function and stability are regained postsurgery. 6
Given its high prevalence and significant impact on ACL outcomes, addressing kinesiophobia and its determinants will be crucial to improving patient outcomes post-ACLR. This study aims to identify patient, injury/surgery, and rehabilitation factors that are associated with elevated kinesiophobia in patients undergoing primary ACLR.
Methods
A retrospective registry review of primary ACLR patients in a single institution (a tertiary acute Southeast Asian hospital with approximately 2000 beds) was performed. Ethics approval was obtained (2024/00278-APP1). The study design was guided by the “STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE)” guidelines checklist to improve reporting of different components of this study (Appendix 1, available in the online version of this article). This registry contains deidentified patient data of all patients undergoing primary ACLR within the institution from June 1, 2019 to June 1, 2023. The inclusion criterion was all patients aged 18 years to 60 years who underwent primary ACLR. Exclusion criteria included revision ACLR, multiligamentous knee injuries, and patients with incomplete data at 1 year postoperation.
Questionnaire responses were entered by patients independently at standardized intervals (preoperatively, and at 6 months and 1 year postoperatively). The completeness of response was ensured by a trained research assistant after patients completed the questionnaires. Transcription of data into the registry was performed by a trained research assistant and accuracy was validated by quarterly random audits. Registry data included patient demographics (age, sex), injury/surgery factors (graft choice/size, concomitant intraoperative meniscal injuries, delay to surgery from injury), rehabilitation factors (attendance of presurgery rehabilitation [“prehabilitation”], total number of prehabilitation sessions, total number of physiotherapy sessions attended) and outcome measures (International Knee Documentation Committee (IKDC) score, Knee Injury and Osteoarthritis Outcome Score [KOOS]). Kinesiophobia was assessed via the Tampa Scale of Kinesiophobia-17 (TSK-17) scores at baseline (preoperatively) and 1-year postoperatively.
Prehabilitation was defined as any guided physiotherapy session performed before surgery. These sessions were conducted by a certified physiotherapist and consisted of preoperative ROM optimization, improving familiarity with hamstring and quadriceps strengthening exercises, and patient education regarding surgery and expectations postsurgery.
The IKDC score and KOOS are patient-reported outcome measures (PROMs) used routinely to assess function in ACLR patients.20,42 The IKDC score comprises components assessing function/symptomology/sports, giving a combined score ranging from 0 (poor function) to 100 (good function). 20 Conversely, the KOOS assesses 5 domains separately: pain, symptoms, activities of daily living (ADL), sports and quality of life (QoL)—also 5 separate scores from 0 (poor function) to 100 (good function). 42
TSK-17 is a patient-reported measure of kinesiophobia with good test-retest reliability (intraclass coefficient correlation, 0.77 to 0.99) and internal consistency (a = 0.68-0.91), 11 and has been validated for use in multiple orthopaedic conditions, including ACL injuries. 34 The TSK-17 is a 17 question self-reported survey that measures a patient’s degree of “activity avoidance” and “somatic focus” - resulting in a composite numerical score from 17 to 68. 30 A higher score indicates a higher degree of kinesiophobia and a cutoff score was developed and validated by Vlaeyen et al, 49 where a TSK-17 score of ≥37 was indicative of having elevated kinesiophobia.
Statistical Method
Statistical analysis was conducted using STATA Version 18.0. Summary statistics were presented for continuous variables while count and percentage were presented for categorical variables. To identify risk factors for 1-year kinesiophobia, all variables collected in the ACLR registry (patient demographics, injury/surgery factors, rehabilitation factors, outcome measures, and baseline kinesiophobia) were considered. Univariate analysis was conducted to test the association between each variable and 1-year kinesiophobia—independent t test was applied for continuous variables and Chi-square test was applied for categorical variables. The variables selected (P ≤ 0.1) were then included in the multivariable logistic regression model. In addition, patient sex and duration of delay to surgery were also included in the model as these variables were shown (in existing literature) to contribute to elevated kinesiophobia in ACLR patients.41,46 The model selection was based on log-likelihood ratio test. All tests were based on a 2-sided type I error of 0.05.
Results
Demographics
A total of 200 patients underwent ACLR within this institution from June 1, 2019 to June 1, 2023. After application of inclusion and exclusion criteria, a total of 192 patients were included (96%), with 8 patients excluded due to incomplete 1-year data. There were 36 women (18.75%) and 156 men (81.25%), and the mean age was 29.6 years (SD = 7.8). There were no professional athletes in this cohort. All patients were ethnically Southeast Asian, comprising of 120 Chinese (62.50%), 46 Malay (23.96%), and 26 Indian (13.54%) patients.
Injury/Surgery Factors
There were more concomitant medial meniscal injuries (83 of 192; 43.23%) as compared with lateral meniscal injuries (76 of 192; 39.60%). Of 192 patients, 137 (71.35%) underwent ACLR with hamstring autograft tendon while 55 (28.65%) underwent ACLR with an allograft tendon. The mean graft diameter was 8.4 mm (SD = 0.84). There was a median delay to surgery of 201 days (0 to 6377).
Rehabilitation Factors
Of the 192 patients, a total of 106 (55.21%) attended ≥1 prehabilitation session before ACLR. Patients attending prehabilitation attended a median of 1 session (0 to 10). Patients attended a median of 15 (1 to 84) physiotherapy sessions within the first 1-year post-ACLR surgery.
Patient-Reported Outcome Measures
The mean baseline IKDC score was 52.3 (SD = 11.7), while 1-year IKDC score was 62.8 (SD = 11.5). Mean baseline KOOS scores were: Symptom score 52.9 (SD = 14.7), Pain score 73.2 (SD = 20.7), ADL score 81.0 (SD = 20.2), Sport score 46.1 (SD = 27.9) and QoL score 34.3 (SD = 22.6). Mean 1-year KOOS scores were: Symptom score 59.4 (SD = 12.8), Pain score 87.8 (SD = 14.3), ADL score 92.8 (SD = 13.9), Sport score 70.7 (SD = 24.5), and QoL score 58.3 (SD = 23.5).
Kinesiophobia
The mean baseline TSK-17 score was 38.6 (SD = 5.6) and improved at 1-year to 32.6 (SD = 7.6). Of the 192 patients, 115 (59.90%) had elevated baseline kinesiophobia (TSK-17 ≥ 37); similarly, this improved at 1 year, with 57 of 192 (29.69%) patients having elevated kinesiophobia. Results of a paired t test showed significant improvement in kinesiophobia from baseline to 1-year (P < 0.001). The mean delta in baseline TSK-17 and 1-year TSK-17 scores was –6.093 (SD = 8.56) - this met the minimally clinically important difference (MCID) for TSK-17, which has previously been established as 6 points. 33
Tables 1 and 2 present a summary of the descriptive statistics and results of univariate analysis with elevated kinesiophobia at 1 year (Table 1) and outcome measures (Table 2) collected with the study methodology.
Summary of descriptive statistics and univariate analysis for elevated 1-year kinesiophobia
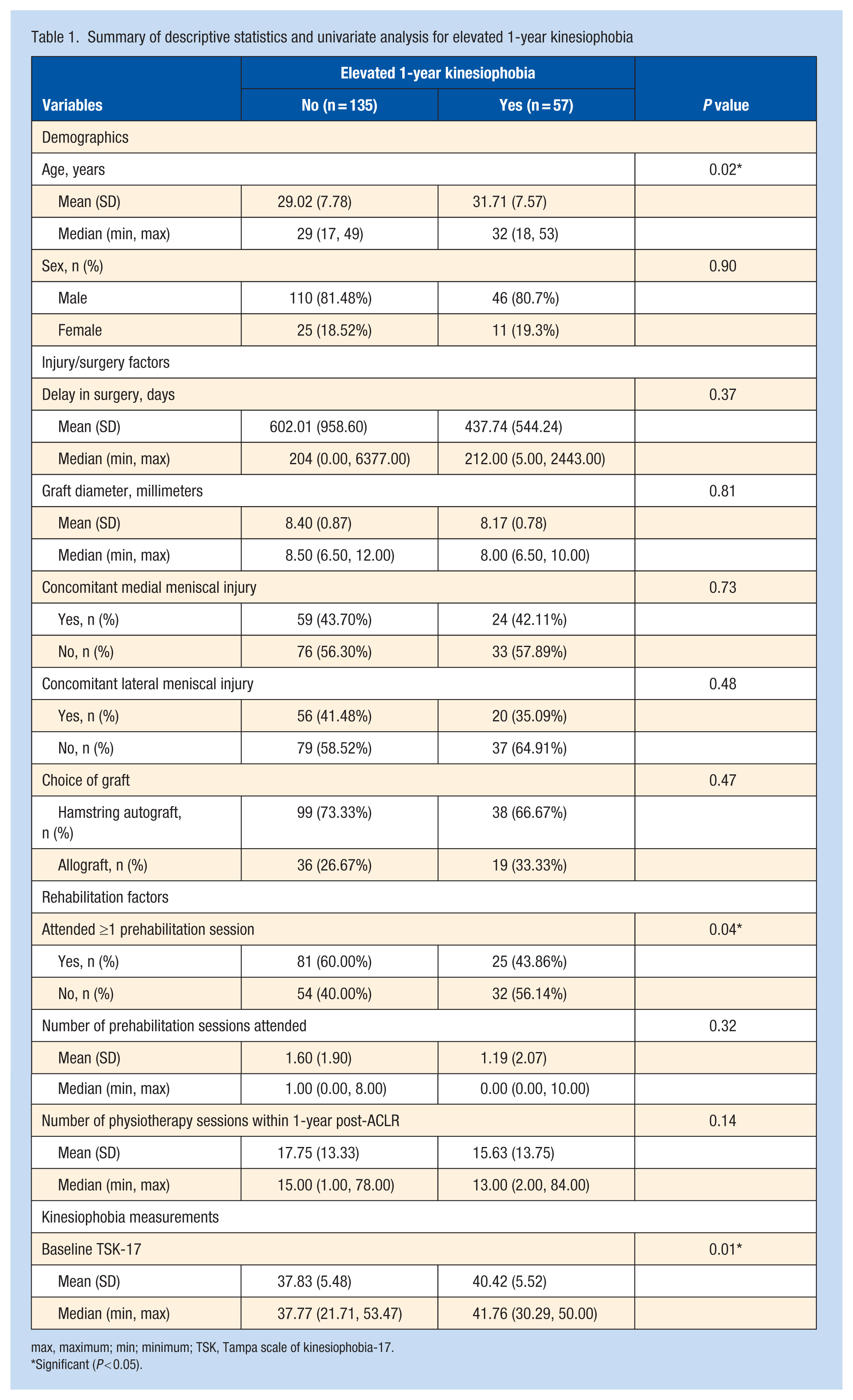
max, maximum; min; minimum; TSK, Tampa scale of kinesiophobia-17.
Significant (P < 0.05).
Summary of baseline/1-year outcome measures and univariate analysis for elevated 1-year kinesiophobia
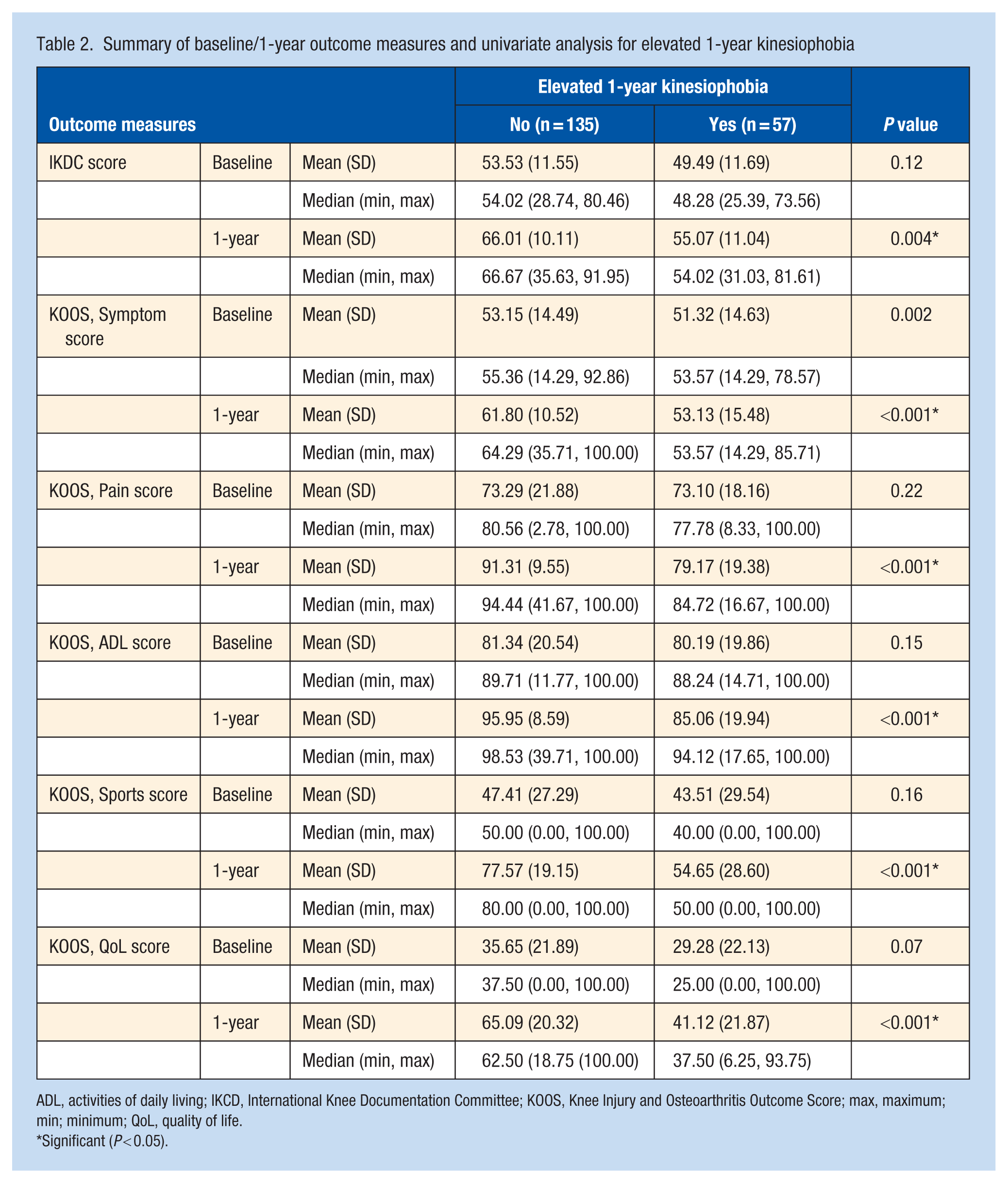
ADL, activities of daily living; IKCD, International Knee Documentation Committee; KOOS, Knee Injury and Osteoarthritis Outcome Score; max, maximum; min; minimum; QoL, quality of life.
Significant (P < 0.05).
Univariate analysis revealed significant association between age, baseline TSK-17 scores, and attendance of ≥1 prehabiliation session with elevated 1-year kinesiophobia (Table 1). The 1-year outcome measures (KOOS and IKDC scores) were also associated significantly with reduced elevated 1-year kinesiophobia (Table 2).
A multivariate logistic regression model was then performed to investigate the preoperative risk factors of elevated 1-year kinesiophobia (Table 3). The results showed significant association of attendance of prehabilitation (OR, 0.513; 95% CI, 0.264, 0.997; P value = 0.05) and baseline TSK-17 score (OR, 2.00; 95% CI, 1.013, 3.968; P value = 0.05) with 1-year kinesiophobia. Higher age tended to have higher risk of having elevated 1-year kinesiophobia, but this was not statistically significant in our data. Sex and delay to surgery also had no statistically significant relationship with elevated 1-year kinesiophobia.
Multivariate logistic regression model for elevated 1-year kinesiophobia
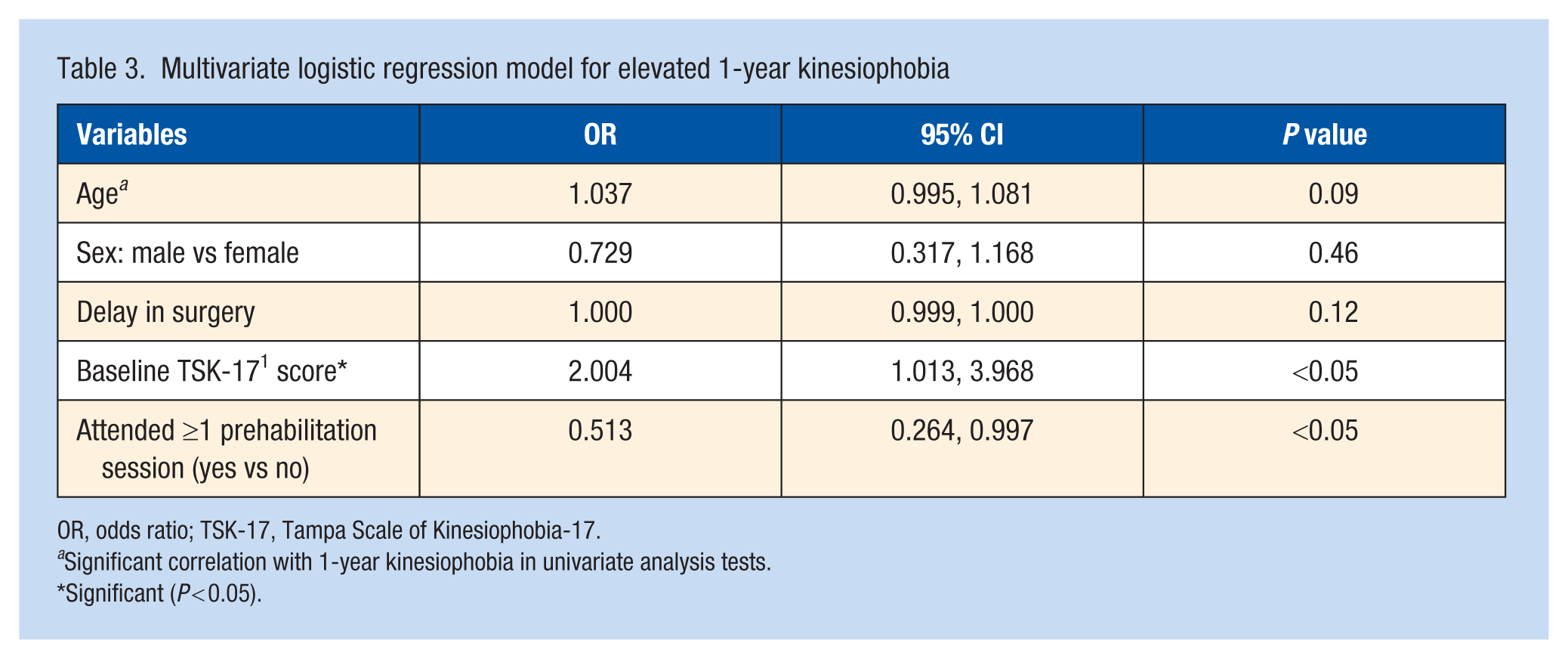
OR, odds ratio; TSK-17, Tampa Scale of Kinesiophobia-17.
Significant correlation with 1-year kinesiophobia in univariate analysis tests.
Significant (P < 0.05).
Discussion
This study demonstrated a significant impact of prehabilitation on the presence of elevated 1-year kinesiophobia levels in patients undergoing ACLR. The attendance of any prehabilitation session(s) before ACLR was associated with significantly reduced risk of elevated kinesiophobia at 1-year post-ACLR. To the authors’ knowledge, this is the first paper to have established a significant association between prehabilitation (as an intervention) and kinesiophobia. Given the negative association between elevated kinesiophobia and RTS rates (as well as 1-year PROMs in our study), minimizing kinesiophobia in ACLR patients should be prioritized. This study highlights a modifiable preoperative factor associated with 1-year kinesiophobia that is relatively easy to implement before ACLR. As such, the authors propose that prehabilitation should be considered as part of the preoperative preparation for patients undergoing ACLR.
This study also demonstrated that elevated 1-year kinesiophobia is associated with poorer patient-reported functional outcomes (IKDC and all KOOS subscores) in ACLR patients. These findings are consistent with the existing literature showing inferior IKDC and KOOS scores are associated with elevated kinesiophobia, in both patients with or without high functional requirements (e.g., athletes). 35 In a cross-sectional study by Van Wyngaarden et al, 47 the authors sought to investigate the impact of multiple physical performance parameters on PROMs, while controlling for potential confounders such as age, delay-to-surgery, and TSK-17 scores, and found that TSK-17 scores were the only confounders that added significant variance to all investigated PROMs (which included KOOS and IKDC). Likewise, the cohort study of 140 ACLR patients by Koovit et al 25 revealed a significant association between kinesiophobia levels and inferior KOOS Symptoms (P = 0.001), QoL (P = 0.001) and Total scores (P = 0.001), although differences in mean patient-reported outcome scores between patients with and without elevated kinesiophobia were not reported. These findings are not surprising given what is currently known about kinesiophobia and its impact on patient outcomes. Elevated kinesiophobia has been shown to contribute to a fear-avoidance model, where high pain catastrophization leads to high pain anxiety and fear of movement.3,27 This repetitive pain-related avoidance of movement can then lead to muscle atrophy and impaired strength/proprioceptive control recovery, eventually amounting to functional deficits.3,8 Minimizing kinesiophobia in ACLR patients is crucial to prevent this vicious cycle from occurring and to help improve patient outcomes after surgery. It is thus vital that the determinants of kinesiophobia be understood so that preventative measures can be adopted to reduce kinesiophobia post-ACLR.
Prehabilitation is a concept that was first popularized with surgical oncology, aiming to improve physical function and reduce length of stay in frail/cachectic oncology patients. 23 Within orthopaedic surgery, prehabilitation has also shown to improve postoperative physical recovery and function via improving preoperative muscle strength, function and health-related QoL scores,5,50 countering any surgery-associated catabolism and decline in physical function.1,17 In this study, the total number of prehabilitation sessions and total number of physiotherapy sessions within 1-year postoperatively had no significant association with elevated 1-year kinesiophobia. One possible explanation is the difference in patient profiles. A large proportion of current literature on prehabilitation is focused on the elderly and frail patients. A 2023 systematic review of 48 unique randomized control trials involving 3570 unique patients by Punnoose et al 39 showed how prehabilitation can improve function, muscle strength, and ROM as well as pain in total knee arthroplasty, total hip arthroplasty, and lumbar surgery patients. 48 In the context of ACLR, however, this physical benefit may not be as significant given that the typical ACLR patient is often younger, more active, and fitter compared with a frailer patient undergoing arthroplasty or spine surgery, 13 and hence may not benefit as much from physical therapy.
When analyzed as a categorical variable, attendance of prehabilitation was significantly associated with reduced incidence of elevated 1-year kinesiophobia (i.e., attending ≥1 prehabilitation session was associated with reduced incidence of elevated 1-year kinesiophobia in ACLR patients). The authors hypothesize that the psychological effects of prehabilitation may be more important than previously thought. Similar findings are also demonstrated in total knee arthroplasty patients, where preoperative education alone has been shown to help improve pain and disability outcomes. 43 Existing literature has already shown that psychological factors should not be underestimated in the ACLR recovery process, with fear of reinjury and overall uncertainty regarding full recovery being 2 barriers often cited as hindering the RTS process. 10 Further, the timing of disease education (about the recovery process and expectations) has also been proven to be important, with interventions before ACLR being shown to be more effective in breaking through these psychological barriers (vs postsurgery). 4 As such, the authors propose that prehabilitation should be included when planning preoperative protocols for ACLR patients. Further studies should be conducted to determine the exact influence of prehabilitation on the psychological and physical improvements in ACLR patients.
Given how important prehabilitation appears to be for ACLR patients, it is concerning that prehabilitation is not currently well defined. There is no current consensus on components of an ideal prehabilitation program, although published programs are consistent in the aims of achieving improvements in knee ROM, quadriceps strengthening, and proprioception in the timespan of 3 to 6 weeks. 9 Psychological prehabilitation is also not well established. Taking reference from surgical oncology (where the concept of prehabilitation first originated), Hirst et al 16 conducted a systematic review and found that psychological prehabiliation was absent in a large proportion (95 of 111; 85.6%) of investigated studies. Even when discussed, there was inadequate intervention descriptions and large heterogeneity of intervention type, duration, and associated outcome measures. Likewise, the lack of high-quality evidence surrounding psychological prehabilitation for ACLR may be limiting its widespread implementation. Further research will be required in this area to show the benefits of psychological prehabilitation in patients undergoing ACLR, and further define its components.
Finally, this paper identified an elevated baseline TSK-17 score as an independent risk factor for elevated 1-year kinesiophobia levels. Although this factor is potentially nonmodifiable, the authors recommend that patients with high baseline scores should be highlighted to the multidisciplinary care team (surgeons, physiotherapists) such that greater care can be taken to institute interventions that have been proven to reduce kinesiophobia. For example, ensuring progressiveness in the increase in intensity of physical therapy, ensuring variation in the physical exercises and consistently timed patient education throughout the rehabilitation process are some interventions highlighted in a 2024 systematic review by Serafim et al 44 that can be effective in reducing kinesiophobia, specifically in the setting of ACLR patients. Conversely, patient factors (age, sex), injury/surgery factors (choice of graft, diameter of graft, concomitant meniscal injuries, delay to surgery), and rehabilitation factors (number of physiotherapy sessions attended), were not significantly related to elevated kinesiophobia. There is no consensus on what a “reliable” predictor for elevated kinesiophobia is, with numerous authors disagreeing about the impact of age or sex on kinesiophiobia levels.29,35,41,45 Studies that have linked longer delay to surgery and concomitant menisci injuries with high postoperative kinesiophobia were also unfortunately low-powered studies with limited follow-up (e.g., 6 months).36,46,51 There is also a gap in literature, with limited studies investigating in-depth the effect of graft choice/diameter or physiotherapy (quantity/duration/components) on kinesiophobia after ACLR.12,31 These findings further highlight the potential importance of baseline TSK-17 scoring as a screening tool for elevated 1-year kinesiophobia in ACLR patients.
Prehabilitation is not part of routine care within the authors’ institution for patients undergoing ACLR but remains an easily implementable intervention that should be considered to reduce the levels of 1-year postoperative kinesiophobia, potentially due to its psychological benefits. Raised baseline TSK-17 scores also potentially highlight patients at risk of persistent elevated kinesiophobia and could be a useful screening tool in preoperative ACLR patients, allowing greater emphasis to be placed on psychological interventions and progressive physical rehabilitation in these patients to minimize kinesiophobia.
Strengths and Limitations
To the author’s knowledge, this is the largest study investigating the effects of prehabilitation on postoperative kinesiophobia in ACLR patients.
There are several limitations in this study. First, there are no formal exclusion of patients with mental health disorders. Although there remains a paucity of literature directly linking established psychiatric diagnoses (e.g., major depression disorder, generalized anxiety disorder) and kinesiophobia incidence in ACLR patients, recent studies have shown that psychiatric conditions such as depression do have influence, specifically on patient-reported outcomes, postoperative analgesia requirements, and subjective knee stiffness in ACLR patients. 15 Given that kinesiophobia is a psychological construct, excluding pre-existing mental health conditions within the analysis could have improved the methodology and strengthened the claims of this study. In addition, another commonly used measure for psychological readiness to RTS is the ACL-RSI scale.18,26,37 It would have been helpful if ACL-RSI was obtained as well, but this variable was not available in the database.
Second, although all patients were prescribed prehabilitation, there was no practical way to enforce attendance. There is a potential for selection bias as patients who attended prehabilitation may have been more motivated. The authors attempted to reduce this confounder by including attendance of prehabilitation within the regression model to minimize the impact of this on the eventual results of this study.
Finally, there is currently no consensus definition for prehabilitation.9,16 In this study, the authors chose to define prehabilitation as “any guided physiotherapy session performed before surgery”. The authors believe that prehabilitation should be defined as any intervention which can contribute to the ACLR patient’s increased preparedness for surgery and postoperative recovery/outcomes. The results of this study show that this can include both physical and psychological components. This is similar to arthroplasty patients, where attendance of a low number (1 or 2) of preoperative pain neuroscience education sessions is associated with reduced postoperative pain intensity and kinesiophobia prevalence. 43
Conclusion
Attendance of prehabiliation before ACLR is an easily modifiable preoperative factor that can reduce the risk for elevated kinesiophobia at 1-year postoperation. Patients with elevated baseline TSK-17 scores are at risk of elevated kinesiophobia at 1-year postoperation. Assessment of baseline TSK-17 scores and implementation of prehabilitation should be included when planning pre-operative ACLR protocols.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261453652 – Supplemental material for Prehabilitation for Patients Undergoing Anterior Cruciate Ligament Reconstruction Reduces Kinesiophobia Levels at 1-Year Postoperation
Supplemental material, sj-docx-1-sph-10.1177_19417381261453652 for Prehabilitation for Patients Undergoing Anterior Cruciate Ligament Reconstruction Reduces Kinesiophobia Levels at 1-Year Postoperation by Sean Wei Loong Ho, Ming Foo Kenneth Nah, Oliver Tze Rong Lim, Xiaoe Zhang, Jegathesan T, Lester Teong Jin Tan and Keng Thiam Lee in Sports Health
Footnotes
The following authors declared potential conflicts of interest: S.W.L.H. has received speaking fees for Smith and Nephew, DePuy Mitek; J.T. received speaking fees for Arthrex; and L.T.J.T. has received speaking fees for Arthrex.
Ethics Statement
Ethical approval for this study was obtained from National Healthcare Group’s domain specific review board (Reference no: 2018/00060).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.