
Abstract
Background and Purpose:
The transfer of patients with ischemic stroke from the intensive care unit (ICU) to noncritical care inpatient wards involves detailed information sharing between care teams. Our local transfer process was not standardized, leading to potential patient risk. We developed and evaluated an “ICU Transfer Checklist” to standardize communication between the neurocritical care team and the stroke ward team.
Methods:
Retrospective review of consecutive patients with ischemic stroke admitted to the neurocritical care unit who were transferred to the stroke ward was used to characterize transfer documentation. A multidisciplinary team developed and implemented an ICU Transfer Checklist that contained a synthesis of the patient’s clinical course, immediate “to-do” action items, and a system-based review of active medical problems. Postintervention checklist utilization was recorded for 8 months, and quality metrics for the postintervention cohort were compared to the preintervention cohort. Providers were surveyed pre- and postintervention to characterize perceived workflow and quality of care.
Results:
Patients before (n = 52) and after (n = 81) ICU Transfer Checklist implementation had similar demographic and clinical characteristics. In the postchecklist implementation period, the ICU Transfer Checklist was used in over 85% of patients and median hospital length of stay (LOS) decreased (8.6 days vs 5.4 days, P = .003), while ICU readmission rate remained low. The checklist was associated with improved perceptions of safety and decreased time needed to transfer patients.
Conclusions:
Use of the standardized ICU Transfer Checklist was associated with decreased hospital LOS and with improvements in providers’ perceptions of patient safety.
Introduction
The process of safely transferring medically complex patients from the intensive care unit (ICU) to the lower acuity hospital ward is dependent on provider handoffs. In some cases, acute medical problems and management plans may not be clearly described in the medical record or during the verbal transition of care handoff. 1,2 This may contribute to adverse patient events as up to 80% of medical errors occur due to limited communication at the time of transfer of care, either from the ward to the ICU or from the ICU to the ward. 3 -6
Standardized transfer checklists and structured handoffs are an Agency for Healthcare Research Quality and Joint Commission Safety Goal. 7,8 These tools have been associated with reductions in medical errors, more efficient workflow, and improved provider satisfaction in certain patient populations. 9 -11 Standardized handoff tools, such as I-PASS, have been used in the transfer of neurosurgical patients to the ICU and the transfer of general pediatric and adult ICU patients within and to the hospital ward, collectively demonstrating improvements in patient safety. 4,6,12 -14 However, little is known about the value of standardized protocols in the transfer of neurologically ill patients from the ICU to the hospital ward. One previous study examined the impact of a handoff checklist at the time of transfer from the ICU to the hospital ward in the neurocritical care population. 15 The checklist was associated with improved medication reconciliation and discontinuation of urinary catheters and had no effect on ICU or hospital length of stay (LOS).
A standardized written transfer format for communicating active problems for all organ systems and providing anticipatory guidance regarding potential acute changes facilitates synthesis of large amounts of patient data and ensures that key information is shared. For the ICU population specifically, it was felt that a written handoff that was documented in the electronic medical record (EMR) would enhance some strategies that were already in place but inconsistently used at our institution, such as I-PASS.
In this study, we aimed to develop and implement a standardized ICU Transfer Checklist and evaluate the association with hospital LOS, ICU LOS, and ICU readmissions. We also sought to evaluate the impact of the checklist on providers’ perceptions of patient safety and satisfaction with the ICU transfer process. We hypothesized that the ICU Transfer Checklist would be associated with decreased hospital LOS, ICU LOS, and ICU readmissions and with improvements in providers’ perceptions of patient safety and satisfaction with workflow.
Methods
Study Approval
The Stanford University Institutional Review Board Compliance Office reviewed the study and determined that it did not constitute human subject or clinical investigation research (45 Code of Federal Regulations (CFR)-46 and 21 CFR-56). Full review was waived under a quality improvement exemption. All authors complied with Health Insurance Portability and Accountability Act (HIPAA) regulations.
Setting
At our institution, over 300 patients with ischemic stroke are admitted annually. More than 40% of these patients are admitted to the ICU. In the ICU, care is provided by the neurocritical care and medical intensive care teams. The neurocritical care team is distinct from the ward stroke team, which cares for patients after transfer out of the ICU. A separate verbal handoff between the ICU resident on both the medical ICU and neurological ICU teams to the stroke ward resident is expected for all patients transferred out of the ICU to the hospital ward. However, nonstandardized forms of verbal and written handoffs are commonly used.
Intensive Care Unit Transfer Checklist Development
A multidisciplinary team of residents, fellows, attendings, and Advanced Practice Providers (APPs) in neurocritical care and vascular neurology developed the ICU Transfer Checklist. A formal process for checklist structure and development was used. 16,17 Human factors engineering was applied in our process, including placement of the most critical items at the beginning of the checklist, minimizing checklist length, and iterative pilot testing. 18 We next performed a contextual needs assessment, which led to an ICU Transfer Checklist composed of: (1) a concise synthesis of the patient’s medical status and ICU course, (2) “to-do” action items, and (3) a problem list of inpatient medical issues organized by organ system. The concise synthesis component comprised a focused summary of the patient’s overall course including key dates of major events and procedures. The “to-do” items represented action items for the team assuming care of the patient and included pending diagnostic studies, consults, and “if, then” plans for anticipatory guidance. The organ-system based problem list component was intended to help the ICU team cross-check that each organ system was addressed in the current progress note or within the text of the checklist (Figure 1).

Structure of the ICU transfer checklist that was added to the note in the electronic medical record as a template when an patient with ischemic stroke was transferred from the ICU to the stroke ward. ICU indicates intensive care unit.
The usability of the checklist, including time to complete and sequential flow of questions from synthesis to a final cross-check, was evaluated by the authors prior to its implementation. Based on pilot tests, several updates were made. Modifications were consensus-based among the authors and occurred in 4 iterations. The ICU Transfer Checklist development was complete by the time of study initiation and the checklist was not modified during the study. The finalized checklist tool was then imported into a shareable text template for the EMR. It was designed to be added to the end of the daily progress note on the day that the patient was identified by the neurocritical care team to be ready to transfer out of the ICU to the ward.
Before implementation of the standardized transfer checklist, the presence of a Transfer Summary document in the EMR or a transfer checklist in any format was recorded. Following implementation, the ICU Transfer Checklist was evaluated for its inclusion in the EMR progress note on the date of transfer from the ICU to the hospital ward and for completion of each of the 3 checklist components. The study design and use of the ICU Transfer Checklist during each phase of the study is depicted in Figure 2.
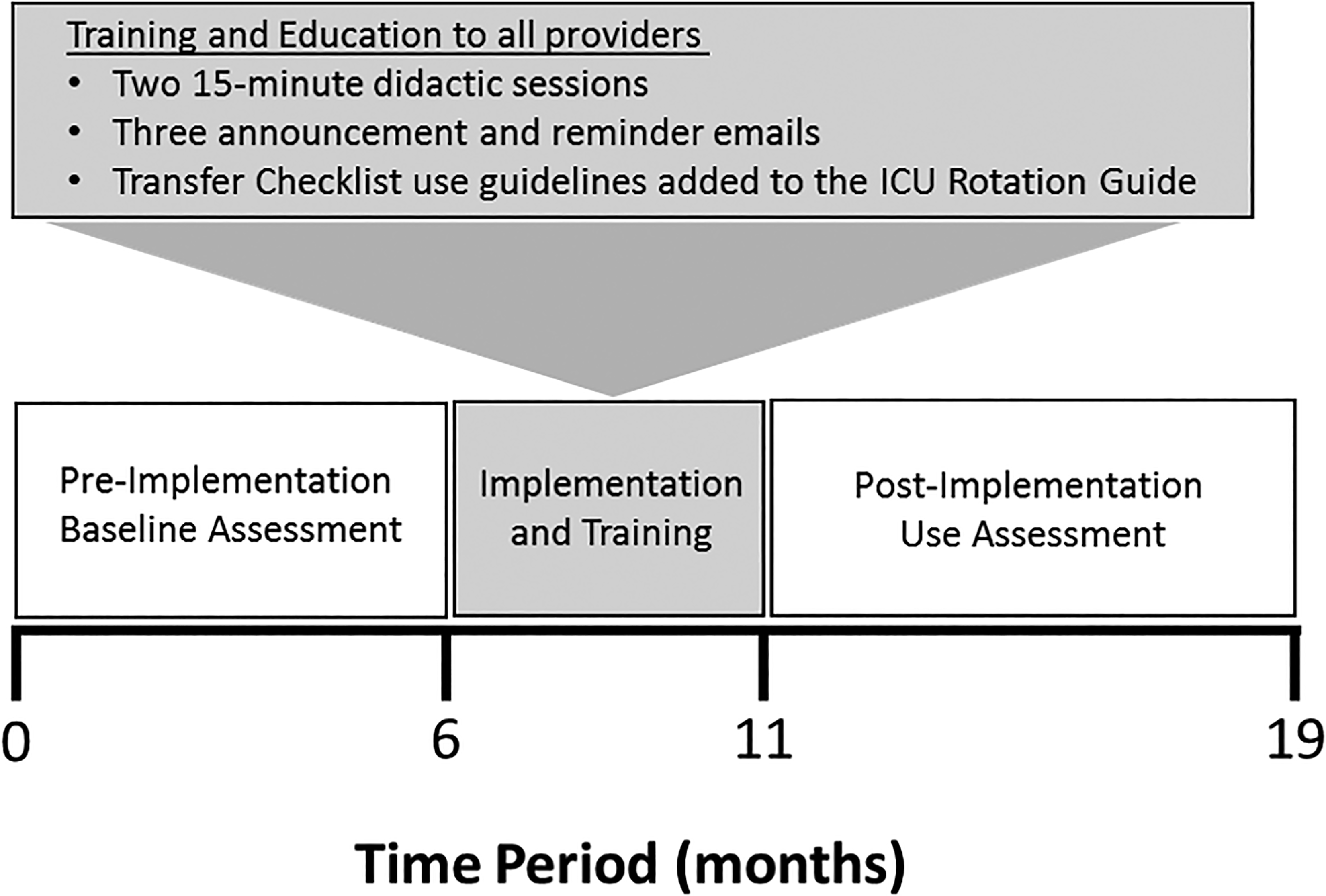
Study design of the ICU transfer checklist development over 18 months with an average of 8 to 10 patients per month who were eligible for its use. The transfer checklist implementation periods are shown. “Before” marks the 6 months of baseline transfer checklist use assessment, “Training and Implementation” marks the 5-month period of roll-out and education on appropriate use, and “After” marks the 8 months of postimplementation use. ICU indicates intensive care unit.
“Appropriate use” of the ICU Transfer Checklist was defined as completion for every neurocritical care patient admitted to the ICU for greater than 48 hours prior to being transferred out of the ICU to the hospital ward. “Appropriate use” was also defined as no checklist utilization if the patient was in the ICU for less than 48 hours, was transferred to a ward service other than the stroke service, or was transferred out of the ICU with comfort-focused care goals. The 48-hour cutoff was chosen to reflect pilot feedback from providers that patients being transferred out of the ICU after a brief ICU admission tended to have a lower illness severity and would thus benefit less from a detailed ICU Transfer Checklist.
Patient Cohort
Patients were included in the study cohort if they were admitted to the neurocritical care unit with a diagnosis of ischemic stroke and subsequently transferred to the stroke ward service. Consecutive patients were identified by International Classification of Diseases, Tenth Revision (ICD-10) code and a stroke program database, and verified by manual chart review. The cohort included patients from a 6-month period prior to checklist implementation and an 8-month period after checklist implementation. The longer time frame for the postimplementation cohort was chosen to evaluate sustainability.
Transfer Checklist Implementation
The implementation of the ICU Transfer Checklist took place over a 5-month period. This duration was selected to ensure adequate training for its use given frequent turnover of rotating residents. During the implementation period, all providers were educated about the checklist. Residents and APPs received 3 comprehensive e-mails regarding the checklist. The first e-mail was sent 5 days before the day of implementation, and the second and third were sent 2 and 4 months after the first, respectively. Two days after the first e-mail, there were separate 15-minute in-person didactic sessions for APPs and residents on how and when the checklist was to be used. These sessions were repeated 3 months later. Finally, the institutional guide for providers rotating in the neurocritical care unit was updated to reflect the guidelines for checklist use, and this guide was e-mailed to all providers before starting the ICU rotation.
Hospital Metrics and Illness Severity
Metrics assessed in all patients pre- and postimplementation included appropriate use of the ICU Transfer Checklist, hospital LOS, ICU LOS, and ICU readmission. Manual chart review was used to evaluate completion of the ICU Transfer Checklist and to confirm the presence or absence of ICU readmission. Hospital LOS, diagnosis related groupings (DRGs), and discharge disposition were identified from an internal MIDAS institutional database (IQVIA, Durham, North Carolina). All hospital metrics were cross-checked for accuracy using manual chart review. Intensive care unit severity scales, such as the Acute Physiology And Chronic Health Evaluation II or Sequential Organ Failure Assessment score, were not available. The quality of checklist utilization, such as the extent and depth of the “if, then” plans or an objective method of volume status measurement, was not characterized.
Two administrative quality and performance databases were used to identify other relevant metrics. From the Vizient Clinical Data Base (Vizient Inc, Irving, Texas), we extracted basic patient demographics, ICU LOS, ICD-10 codes, and severe ICU level complications. Respiratory failure was defined by the need for noninvasive or invasive ventilation. Renal failure was defined as glomerular filtration rate less than 15 mL per minute. Acute heart failure was identified by ICD-10 code. Shock was defined by the use of vasopressors. From the 3M All Patient Refined Diagnosis Related Groupings (APR-DRGs) database (St. Paul, Minnesota) we identified admission severity of illness and risk of mortality at admission. The 3M APR-DRG retrospectively assigns illness severity using a classifier algorithm based off coding features from the EMR. While validation data are proprietary to 3M, these data are widely used by Centers for Medicare & Medicaid Services for value-based reimbursement calculations nationwide.
Provider Perception Surveys
Neurology residents and neurocritical care APPs who cared for patients with stroke during the study period were surveyed twice on their perceptions of the quality of patient transfers from the ICU to the hospital ward, once before and once after implementation of the ICU Transfer Checklist. The timing of pre- and postimplementation surveys were the same for all providers: 1 week immediately prior to its implementation and then 2 days after the end of the 8-month implementation period.
A 4- or 5-point Likert Scale was used to evaluate perceptions of adverse patient events, the quality and safety of the transfer process, effect on transfer workflow time, awareness of pending to-do items, anticipatory guidance plans for neurological deterioration, the documentation of stroke metrics (use of intravenous tissue plasminogen activator, thrombectomy, and Thrombolysis In Cerebral Infarction score if available), and status of goals of care and medication reconciliation (completed, pending, or unknown). 19,20 Survey questions characterized provider perceptions of these items and did not require providers to verify the presence or absence of such items in the EMR. Survey instruction provided explanation of specific question terminology. Near misses were defined as a possible close call of a clinical adverse event that was identified before actually occurring, and unstable issues were defined as medical problems that the provider judged to be acute or prone to rapid clinical change, with or without a next steps plan documented. Goals of care documentation was a perceived measure: survey instructions indicated that it should be marked as completed only if there was provider perception of a goals of care documentation note or a California Physician Orders for Life-Sustaining Treatment (POLST) completed. Residents and APPs were asked to complete the postimplementation survey whether or not they had completed the preimplementation survey. Prechecklist and postchecklist surveys were not paired at the level of individual residents and APPs.
Data Analysis
Continuous variables were analyzed with a Student t test. Likert scale responses were analyzed with a Mann-Whitney U test. Chi square (χ2) tests and Fisher exact tests were used for all categorical data. Differences were considered significant with P < .05 (Graph Pad Prism, La Jolla, California). The Standards for Quality Improvement Reporting Excellence 2.0 guidelines were used. 21
Results
Patient Demographics and Clinical Characteristics
Fifty-two patients were included in the 6-month prechecklist cohort, and 81 patients were included in the 8-month postchecklist cohort (Figure 3). The pre- and postchecklist cohorts had similar demographics and clinical characteristics, including age, sex, race, calculated admit risk of mortality, stroke type, admission National Institutes of Health Stroke Scale score, preadmission medical comorbidities, severe ICU level complications, and hospital discharge disposition (Table 1). Patients in the postimplementation cohort had a greater admission illness severity (extreme illness severity pre- vs postchecklist: 15% vs 25%, P = .03).
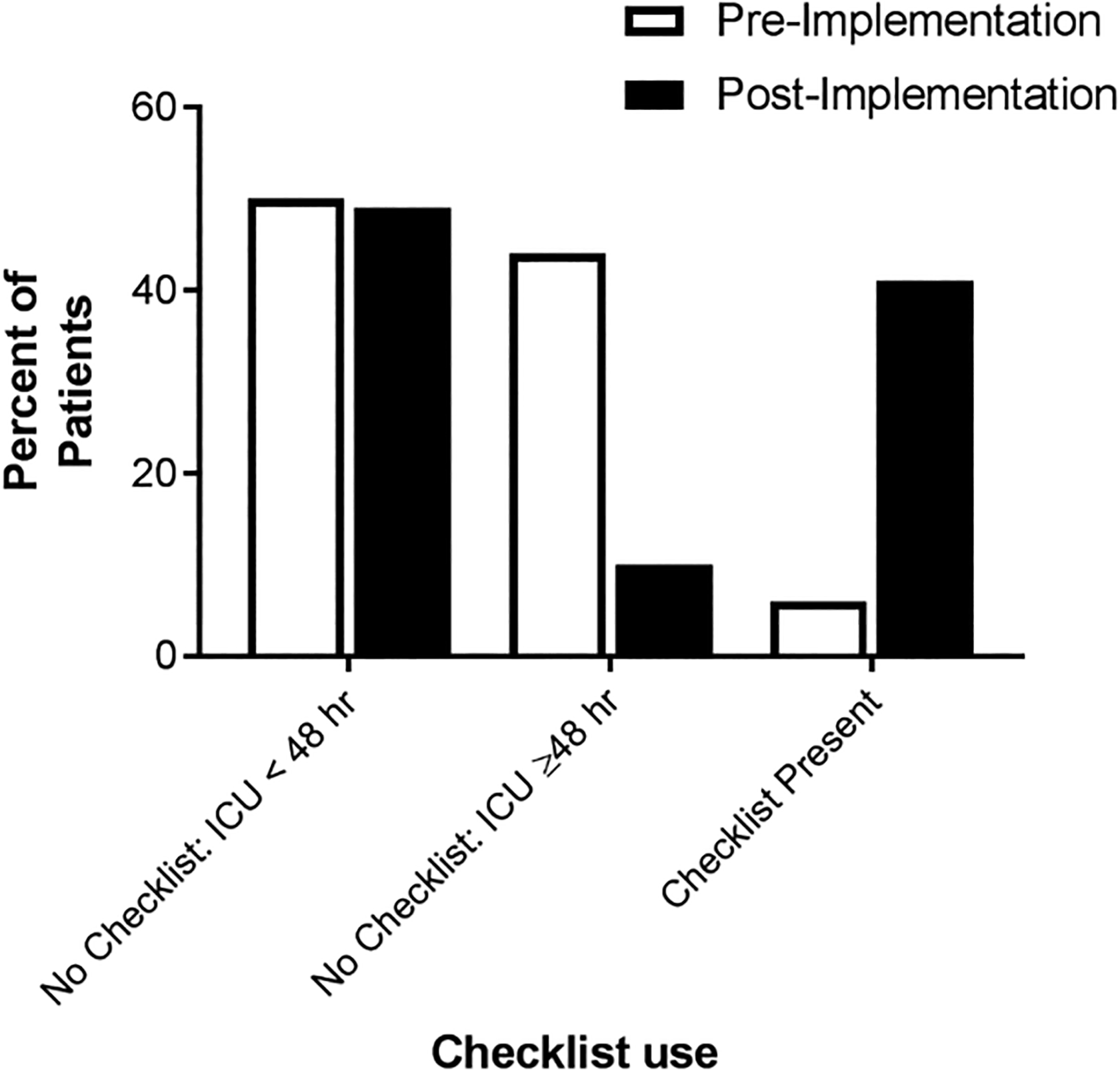
The total patient population for pre- and post-ICU Transfer Checklist implementation phase (6- and 8-month periods, n = 52 and 81, respectively). The shift in use of any transfer checklist (preimplementation) to the standardized ICU Transfer Checklist (postimplementation) is represented by percent of patients in each category. ICU indicates intensive care unit.
Demographic and Clinical Characteristics of the Patients With Ischemic Stroke Transferred From the Neurocritical Care Unit to the Hospital Stroke Ward.a
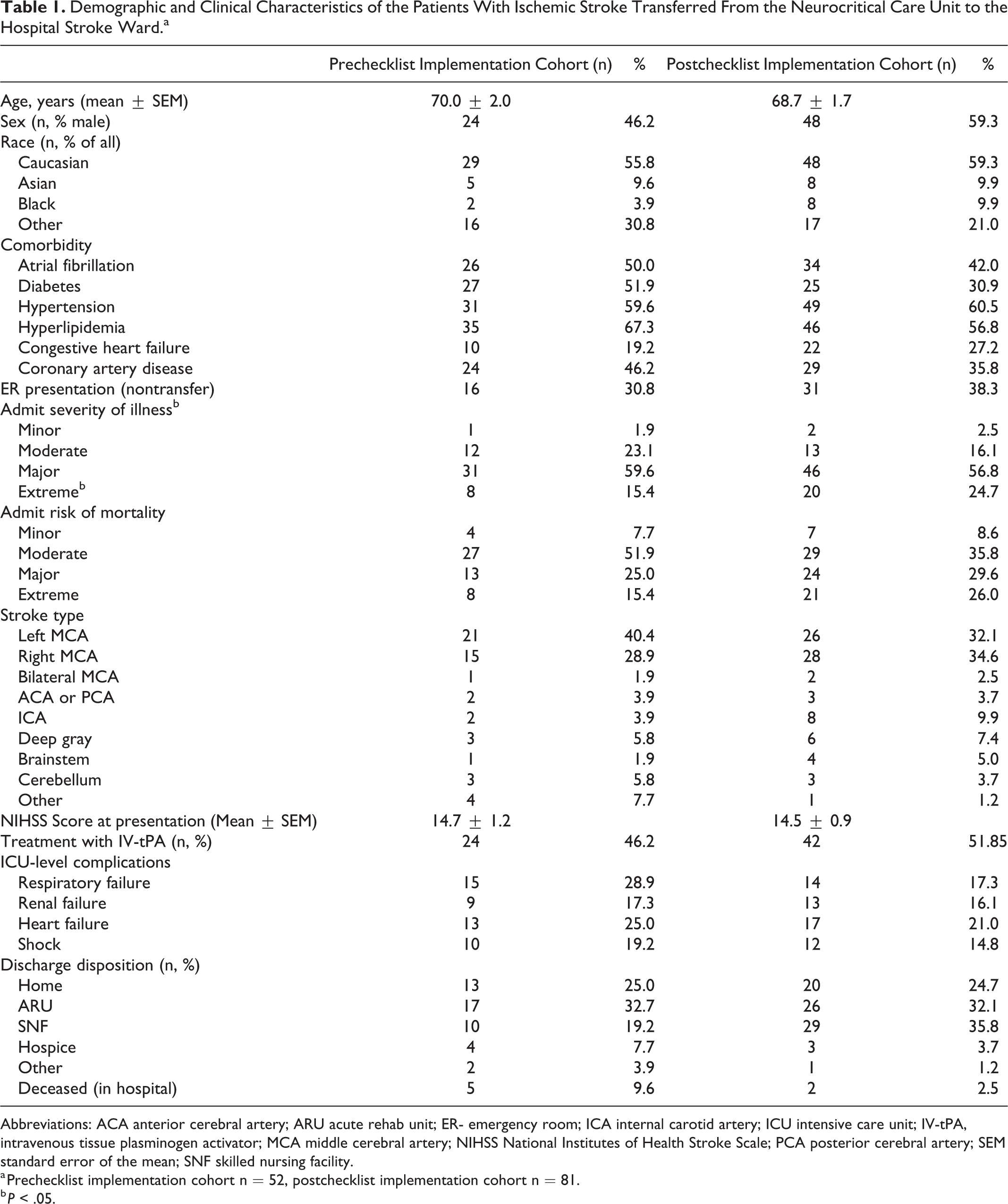
Abbreviations: ACA anterior cerebral artery; ARU acute rehab unit; ER- emergency room; ICA internal carotid artery; ICU intensive care unit; IV-tPA, intravenous tissue plasminogen activator; MCA middle cerebral artery; NIHSS National Institutes of Health Stroke Scale; PCA posterior cerebral artery; SEM standard error of the mean; SNF skilled nursing facility.
a Prechecklist implementation cohort n = 52, postchecklist implementation cohort n = 81.
b P < .05.
Transfer Checklist Utilization
In the 6 months prior to the implementation of the ICU Transfer Checklist, 6% (3/52) of patients had some form of transfer summary in their EMR chart at time of transfer from the ICU to the hospital ward. In the 8 months after implementation of the ICU Transfer Checklist, 93% (75/81) of patients had appropriate transfer checklist utilization, including 86% (38/44) of patients who should have had the checklist used and 37 patients hospitalized in ICU for less than 48 hours who per protocol appropriately did not have checklist used (Figure 3).
Length of Stay and ICU Readmission Metrics
Hospitalization metrics differed between the pre- and postchecklist implementation cohorts. The median hospital LOS decreased (pre- vs postchecklist: 8.6 days, interquartile range (IQR): 3.7-14.2, vs 5.4 days, IQR: 3.1-8.3, P = .003; Figure 4A). Intensive care unit LOS showed a trend to decrease, (median: 2 days, IQR: 1.0-6.0, vs 1 day, IQR: 1.0-2.0, P = .068; Figure 4B) and ICU readmissions remained low (5.8%, n = 3/52 vs 1.2%, n = 1/81; odds ratio [OR]: 0.20, 95% confidence interval [CI]: 0.02-1.4).
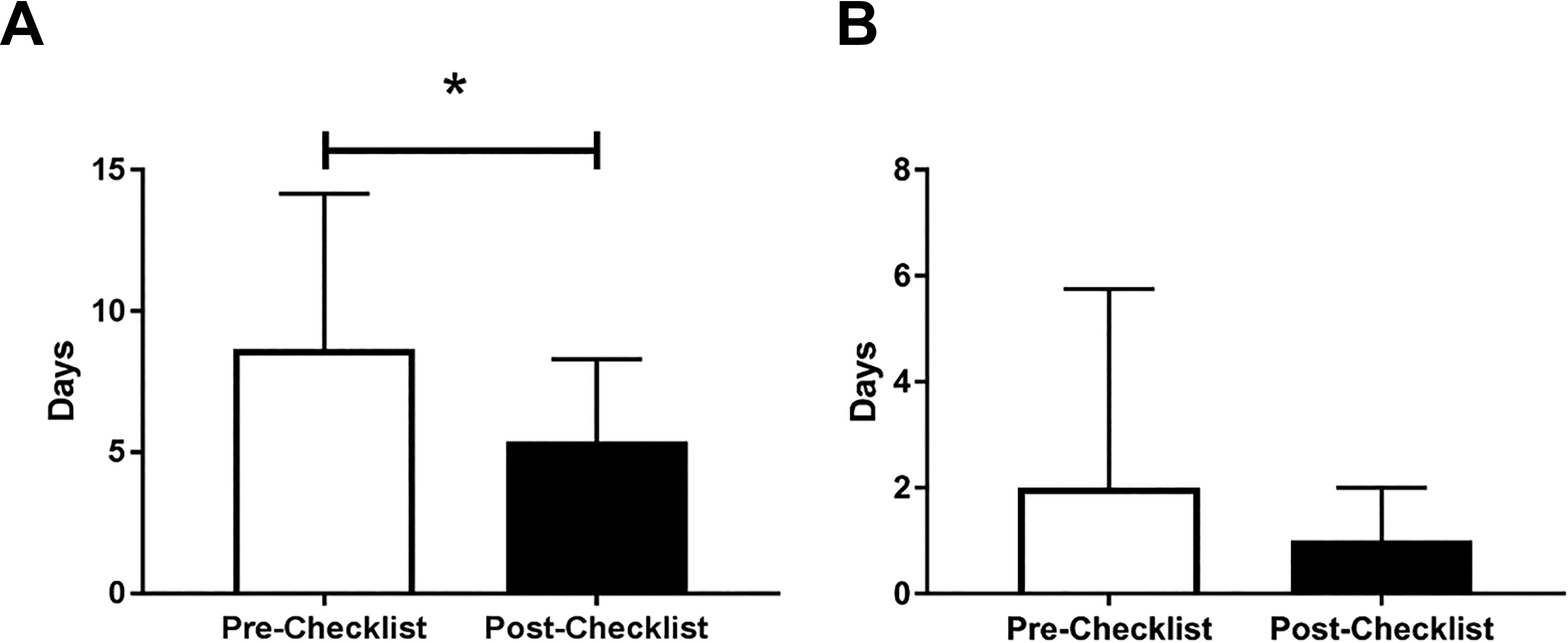
Length of stay (LOS) of patients with ischemic stroke for the 6-month prechecklist implementation cohort compared to the 8-month postchecklist implementation cohort (median ± SD). A, Length of stay for the entire hospital admission, including ICU LOS, * P < .05. B, Length of stay for the ICU admission only, P = .069. ICU indicates intensive care unit; SD, standard deviation.
Provider Perceptions of the Transfer Checklist
Prechecklist provider perception surveys were completed by 59% of eligible providers (17/29) and postchecklist surveys were completed by 41% (12/29). After checklist implementation, responses of frequent near miss events decreased (pre- vs postchecklist: 33% vs 9%, OR: 0.10, 95% CI: 0.01-0.75, P = .02) and provider perception of medication reconciliation being clearly documented as either done, pending, or unknown increased (pre- vs postchecklist: 26% ± 3% vs 46% ± 8%, P = .02). Additionally, the perception of clear goals of care documentation at time of transfer increased in the postimplementation cohort (pre- vs postchecklist: 48% ± 6% to 70% ± 5%, P = .01; Figure 5). Some variables did not change, including documentation of stroke treatment metrics perceived as frequent (pre- vs postchecklist: 65% vs 75%, OR: 1.64, 95% CI: 0.31-7.19, P = .69) and description of unstable issues and associated next steps perceived as frequent (82% vs 92%, OR: 2.36 95% CI: 0.30-33.1, P = .62). Postchecklist, providers perceived that it took less time to complete medical record review at time of transfer (pre- vs postchecklist: 34 ± 3 minutes vs 16 ± 1 minute, P = .0002; Figure 5). In the postimplementation survey, over 80% of providers reported that continuing of the ICU Transfer Checklist would be useful. Notably, 47% would not change the structure, while 30% would make minor modifications.
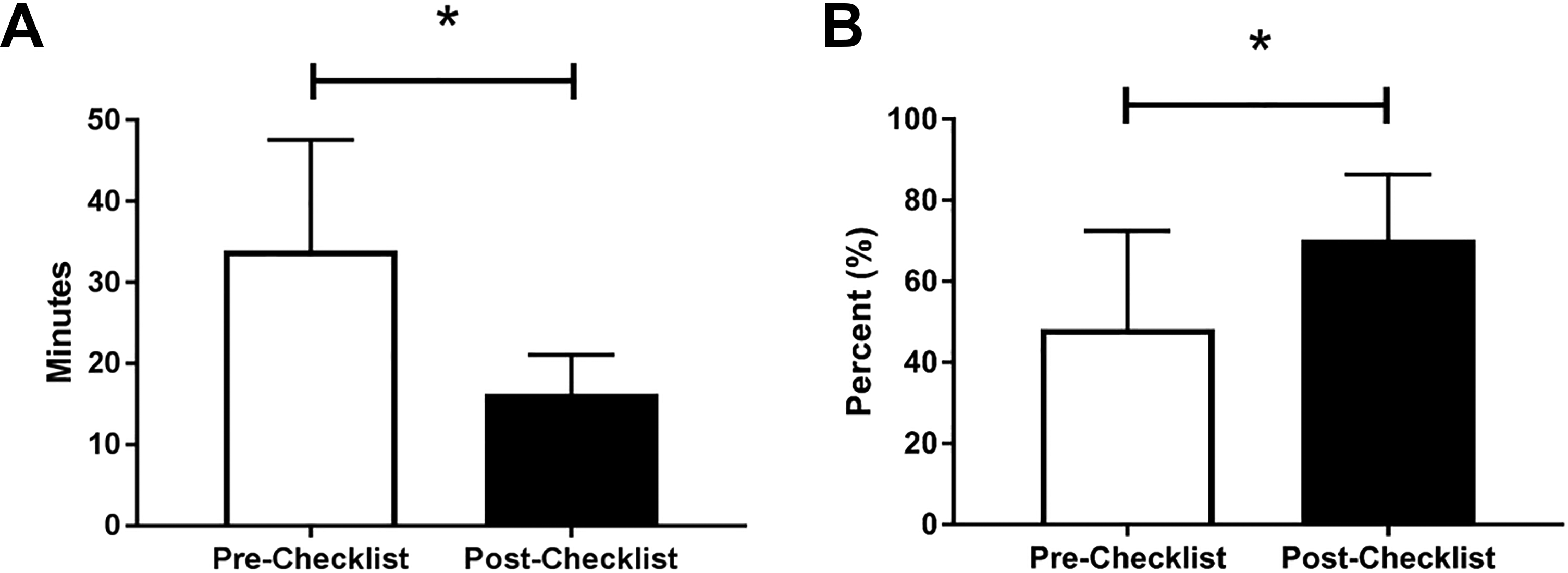
Provider perception survey results before (white bars) and after (black bars) implementation of the standardized ICU Transfer Checklist for patients with ischemic stroke transferring out of ICU to the stroke ward. A, Change in provider responses for minutes required for chart review during the transfer process. B, Perceived percentage of patients with status of goals of care documentation listed. *P < .05. ICU indicates intensive care unit.
Discussion
We developed and implemented a written ICU Transfer Checklist to standardize the workflow for handoff communication of patients with ischemic stroke transferring from the ICU to the hospital ward. The ICU Transfer Checklist was associated with decreased hospital LOS and improved provider perceptions of transfer workflow efficiency and patient safety. This effect was seen despite a significantly greater proportion of patients with Extreme Admission Illness Severity in the postchecklist implementation cohort. While there was only a trend to reduce ICU LOS, it is likely that this effect was a result of the checklist improving the comprehensive care of patients prior to transfer, as providers may have altered care behavior as they were aware of the future need to complete the checklist.
The ICU Transfer Checklist was utilized for nearly 90% of eligible patients. This is among the highest rates of handoff tool utilization reported in studies of transfer optimization (45%-94%). 1,6,15 We hypothesize that the high level of utilization was achieved through engagement of key stakeholders, including residents and APPs, in the development and implementation process and the ease of use of the checklist. The checklist did not create an additional opportunity cost in the form of a new documentation task. Rather the reduction in time required for chart review reflects that the design of the checklist may have aided efficient workflow. Importantly, the high rate of checklist utilization was sustained over 8 months.
To our knowledge, this is the first study to describe an ICU Transfer Checklist for neurocritical care patients with stroke that demonstrated a significant reduction in LOS while also improving provider perceptions of patient safety and workflow. A previous study examining the impact of a primarily “yes or no” answer format transfer checklist in a neurocritical care population over 3 months did not demonstrate significant differences in hospital or ward LOS. 15 We note that our Transfer Checklist is more than a traditional “yes or no” checklist, but rather a format for a framework for the transfer handoff of ICU patients. Specific components of this Transfer Checklist framework (eg, the clinical patient synthesis, “if, then” items, and checklist items) may have had different association strengths to the observed outcomes. We chose to refer to the template used here as a Transfer Checklist to emphasize to the provider that its primary purpose is to prompt systematic and thorough review and handoff of important clinical details of each patient.
The improvements in hospital LOS and provider perception of patient care in the current study likely has multiple drivers. The ICU Transfer Checklist could be a contributor to these favorable changes. It may prepare the ward provider with a clinical synthesis of the complex ICU patient, alert them to the to-do items for active medical problems, and outline clear anticipatory guidance with “if, then” plans for managing an acute change in clinical condition. It may also provide preemptive guidance to the ICU provider. This preparation may also lead to more appropriate timing of ICU discharge and, once out of the ICU, encourage patient stabilization without triggering an ICU readmission, prolonging inpatient stay, or providing inappropriate escalation of care. We hypothesize that the bulleted “to-do” list may be associated with more timely interventions, consultations, or diagnostics, which may reduce the LOS on the hospital ward.
We identified other variables that were not controlled for in this study, but may be associated with our observed improvement in LOS. These include the hiring of a new case manager and the implementation of a quality-focused daily rounding checklist on the stroke ward service. The relative contribution of these interventions compared to our intervention is not easily determined. The existence of these interventions does not invalidate the value of our intervention, as our intervention likely played a significant role in the LOS improvement and providers found the ICU Transfer Checklist to be beneficial.
There were several limitations to this study. First, the present study had a relatively low sample size of patients due to restricting the target population to patients with ischemic stroke. These patients may have shorter LOS than those with other neurological illness and may be less likely to benefit from a Transfer Checklist. The neurocritical care unit cares for a wide variety of patients, such as those with seizures, hemorrhagic stroke, and neuromuscular failure. Patients with these conditions may also benefit from use of a standardized checklist. Second, using a survey design to assess provider perception of the checklist may introduce bias and a survey design does not objectively reflect rates of medical errors, preventable adverse effects, or near misses. Third, there were no long-term outcome functional outcome measures included in our data. Fourth, the written handoff used here may have affected the content and quality of the verbal handoff, which was not measured.
In summary, use of the ICU Transfer Checklist was associated with improvements in the quality of patient care during our measurement periods. A broader effect of the checklist may be achieved by standardizing its use in the verbal patient handoff, as well as adapting it for additional neurological diseases. Further validation with a prospective study involving additional institutions will allow for evaluation of the generalizability of the improvements. Such studies should characterize the timing of transfer, including daytime versus nighttime, nursing handoffs, and effect of transfer on the neurocognitive status, such as anxiety, of the patient and their family members. Use of a standardized ICU transfer process that concisely communicates evaluative data, is reproducible between patients, and reflects salient disease-specific understanding is a critical component of safe, high-quality care for neurocritical care patients.
Footnotes
Authors’ Note
All work was performed at Stanford University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.