
Abstract
Background and Purpose:
Risk of 30-day stroke readmission has been attributed to medical comorbidities, stroke severity, and hospitalization metrics. The leading etiologies appear to vary across institutions and remain a moving target. We hypothesized that patients with increased medical complexity have higher odds of 30-day readmission and the immediate time after discharge may be most vulnerable. We aimed to characterize patients with 30-day readmission after acute ischemic stroke (IS) and identify predictors of post-IS readmission.
Methods:
We performed a retrospective case-control study analyzing post-IS 30-day readmission between January 2016-December 2019 using data from Mount Sinai Hospital’s Get With The Guidelines database. We performed chi square analyses and multivariate adjusted logistic regression model including age, sex, coronary artery disease (CAD), renal insufficiency (RI), history of prior stroke or TIA, length of stay (LOS) > 7, and NIHSS ≥ 5.
Results:
6.7% (n = 115) of 1,706 IS encounters had 30-day readmission. The 115 cases were compared to 1,591 controls without 30-day readmission. In our adjusted model, CAD (OR = 1.7, p = 0.01), history of prior stroke or TIA (OR = 1.6, p = 0.01), LOS >7 (OR = 1.7, p = 0.02), and NIHSS ≥ 5 (OR = 4.5, p < 0.001) predicted 30-day readmission. 65% (n = 75) of readmitted patients had readmission within 14 days post-discharge.
Conclusions:
Patients with post-IS 30-day readmission were more likely to have complex medical comorbidities and history of stroke or TIA compared to controls. Patients with more severe stroke and longer LOS may benefit from individualized transition of care plans and closer follow up during the vulnerable 30-day post-stroke period.
Introduction
The first 30 days following stroke are of great importance for recovery and rehabilitation, yet more than one-third of patients may be readmitted during this critical period.1-9 Beyond adversely impacting recovery, stroke readmissions are of great cost to patients and hospitals. In the first year following ischemic stroke (IS), all-cause costs can total over $60,000, 9 and unplanned rehospitalizations account for almost a fifth of total Medicare hospital payments. 10 The Centers for Medicare and Medicaid Services (CMS) tracks 30-day readmission for stroke as an indicator of hospital quality, and financially penalizes those with higher than expected 30-day readmissions. 11 In order to develop quality improvement initiatives targeted at reducing 30-day readmissions, research has focused on predicting risk factors for 30-day readmission. Much of the research pre-dates the modern thrombectomy era of care, and, although findings vary, it suggests that patient age, medical comorbidities, and length of stay (LOS) predict 30-day readmission.
The aim of our study is to characterize our large urban stroke population, and present updated data on potential predictors and patterns of 30-day readmission at a major metropolitan hospital providing the latest standard of stroke treatment. We hypothesized that older patients with complex medical histories and more severe strokes will be at greater risk for readmission within 30 days. We further hypothesized that the first 2 weeks post-discharge following stroke represent the highest-risk period for readmission and should be the target for readmission reducing initiatives.
Methods
The Mount Sinai Hospital (MSH), a large, urban academic hospital in New York City with a Comprehensive Stroke Center that treats approximately 450 ischemic stroke patients per year participates in the Get with the Guidelines (GWTG)-Stroke Program. Our local GWTG database includes all patients with a diagnosis of stroke, based on International Classification of Disease-10 codes for the hospitalization, and is organized by anonymous identification numbers where each identifier is a new hospital admission. As part of hospital quality improvement efforts, all patients readmitted within 30-days are tracked in the hospital’s 30-Day Readmissions Dashboard based on stroke diagnosis-related group codes. We conducted a retrospective case-control study analyzing predictors of 30-day post-stroke readmission at our institution. The study included all patients ages 18 years and older at MSH with a diagnosis of IS admitted from January 1st 2016-December 31st, 2019. Patients with all-cause 30-day readmission were identified from the 30-Day Readmissions Dashboard and confirmed by chart review. The control group comprised all IS patients without 30-day readmission during the same time frame. Patients who expired during index admission were excluded from the study and included only in an analysis to test for difference in mortality. This study protocol was reviewed and the need for individual patient consent was waived by the Mount Sinai Institutional Review Board.
Data collection occurred in 2 work streams: the first involved collecting patient and index admission information from the GWTG database, and the second required chart review for details related to the readmission. All information related to patient characteristics (eg., age, sex, medical comorbidities) and index admission metrics (eg., length of stay, treatment interventions, National Institute of Health Stroke Scale) were obtained from the GWTG database, which is maintained by an abstractor outside the study team. Data related to the readmission were gathered from the electronic chart record by 3 trained study abstractors. Time to readmission (defined as the number of days from index discharge to readmission), readmission LOS, and treating service were recorded. Treatment on the neurology service included our institution’s dedicated stroke team. Treatment in the intensive care unit included any intensive care specialty units, such as the neurosurgical intensive care unit and the medical intensive care unit. The primary reason for readmission was identified from the admission note and discharge summary and organized by our study team’s vascular neurologist. Readmission with infection was identified by documentation by the treating team and confirmed by documentation in the readmission discharge summary. Presentations to the emergency department that did not result in admission were not included in the analysis. If patients were hospitalized with a subsequent IS (not within 30 days) over the study time period, they were analyzed as a new case.
Data Analysis
Continuous variables were dichotomized for analysis: age at 65 years, LOS of index admission at 7 days (average of the median LOS for the control, 6 days, and readmitted, 8 days), and the National Institute of Health Stroke Scale (NIHSS) at 5 (median score of the total population combined). Any missing NIHSS score (n = 131) was coded with the median value of the group (4 for controls and 8 for cases). No other data point had missing values. For normally distributed variables, we performed t-tests; comparisons of nominal data were done with chi square tests between the readmitted and non-readmitted groups.
We performed logistic regression modeling of risk factors of 30-day readmission, comparing those with 30-day readmission to those without. Risk factors tested included age, sex, coronary artery disease (CAD), renal insufficiency (RI), history of prior stroke (i.e., ischemic, hemorrhagic, subarachnoid hemorrhage) or transient ischemic attack (TIA), LOS > 7, and NIHSS ≥ 5. First, we ran an unadjusted model and then we adjusted for age (dichotomized at 65) sex, CAD, RI, history of prior stroke or TIA, LOS > 7, and NIHSS ≥ 5. We report odds ratios (and 95% confidence intervals) for 30-day readmission.
An investigator not involved in chart abstraction assessed inter-rater reliability of the readmission chart review by reviewing medical records for the key variables analyzed and calculating the Kappa statistic. The Kappa inter-reliability ranged from 0.7-1.0 for the key variables abstracted from chart review. All data analysis was performed on IBM SPSS Statistics (Version 26).
Results
Among 1,706 IS encounters from January 1st 2016-December 31st 2019, 6.7% (n = 115) were readmitted within 30 days. 1,591 patients without 30-day readmission served as controls. 112 patients who expired at index admission were excluded. Baseline characteristics of the readmitted and control groups are shown in Table 1. Average age was 68 years and 46% (n = 53) were female in the readmitted group, and these demographics were similar in the control group.
Baseline Characteristics and Index Hospitalization Metrics.
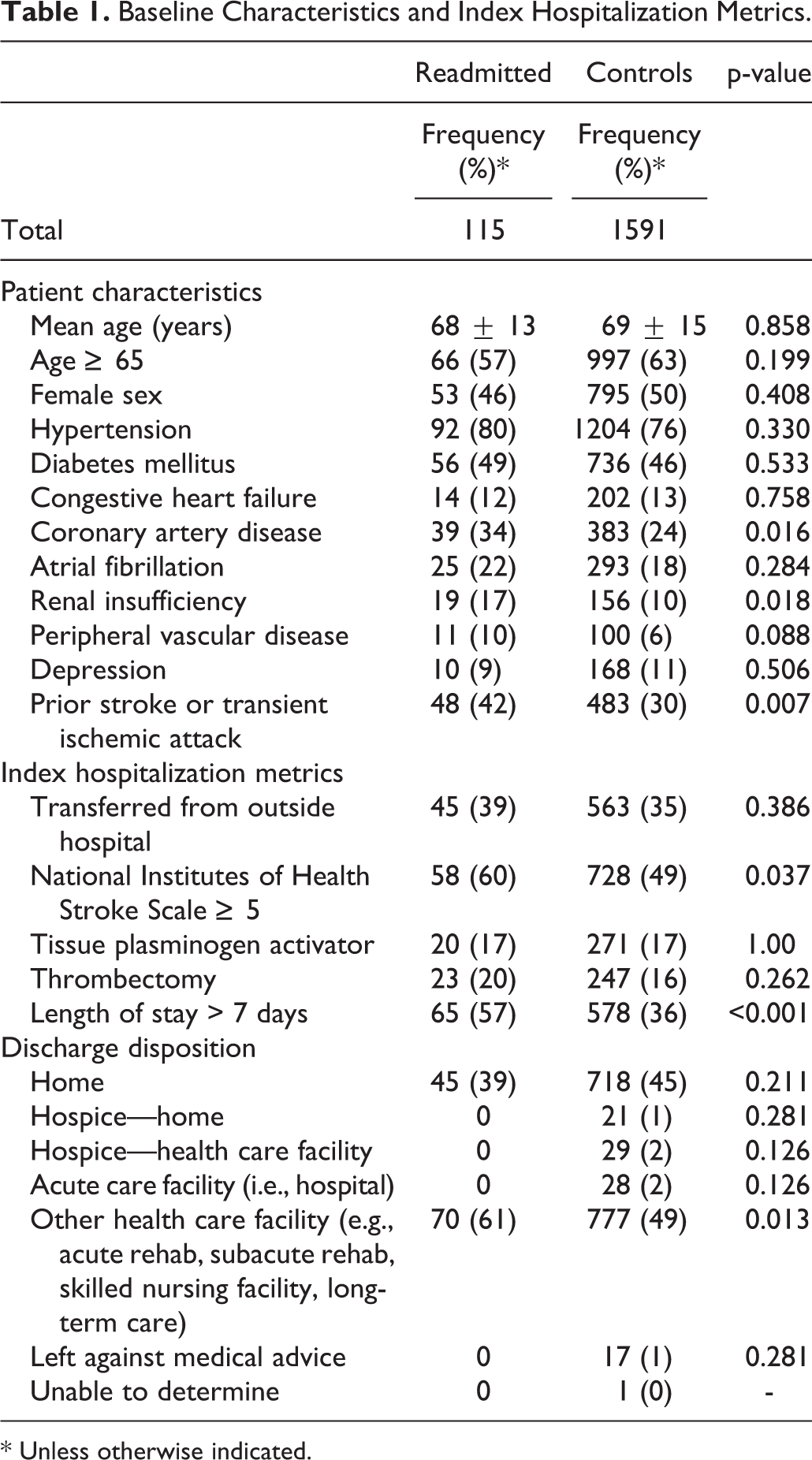
* Unless otherwise indicated.
Although no significant differences existed for the majority of vascular risk factors, the readmitted group had a higher prevalence of CAD (34% vs 24%, p = 0.016), RI (17% vs 10%, p = 0.018), and prior stroke or TIA (42% vs 30%, p = 0.007). Readmitted patients were more likely to have an initial NIHSS ≥ 5 upon presentation at index admission (60% vs 49%, p = 0.037), and those readmitted were more likely to stay greater than 7 days at index hospitalization (57% vs 36%, p < 0.001). There was no significant difference in transfer status at index admission between the 2 groups (39% vs 35%, p = 0.386). The proportion of patients receiving treatment with Tissue Plasminogen Activator (tPA) (17% vs 17%) and thrombectomy (20% vs 16%) were similar across the readmitted and control groups. The majority of patients were discharged either to home or to a health care facility (e.g., acute rehab, subacute rehab). The number of patients discharged to each location was similar between readmitted vs not except for discharge to other healthcare facility (61% vs 49%, p = 0.013).
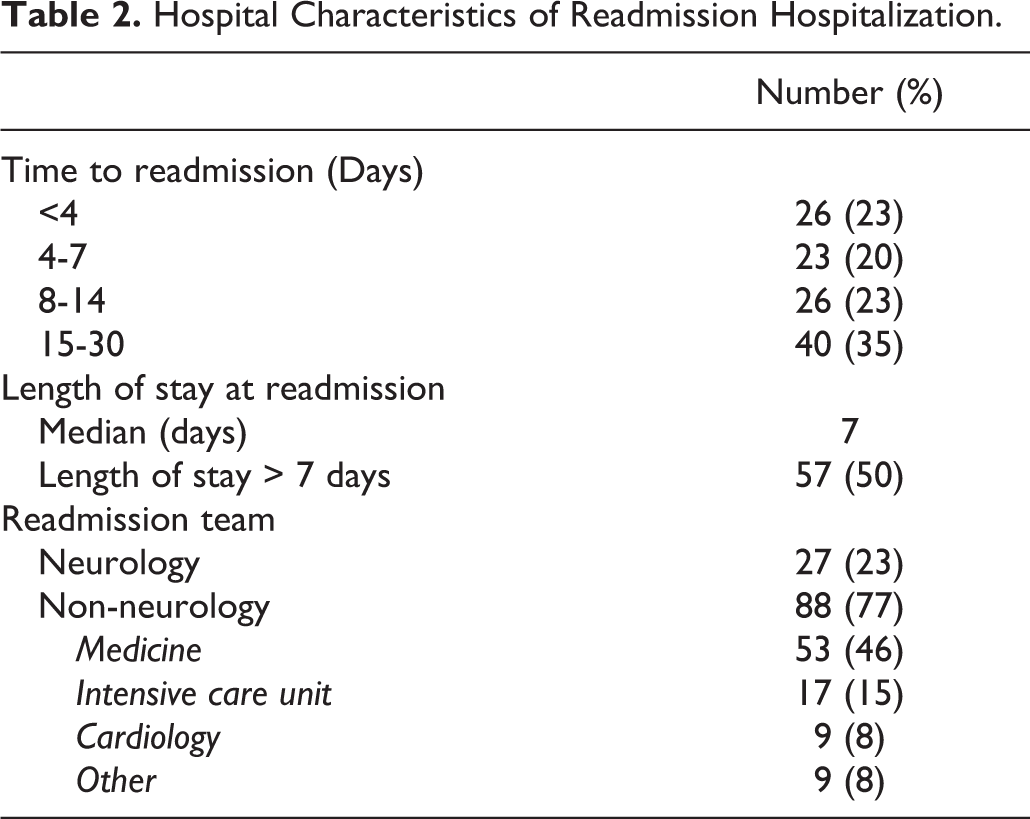
While 24% (n = 27) of patients were readmitted to the neurology service, more patients were readmitted to the medicine service (46%, n = 53) (Table 2). A total of 43% (n = 49) of readmitted patients returned to the hospital within a week, 23% (n = 26) within 1 to 2 weeks, and 35% (n = 40) after 2 weeks. Half of the readmitted patients were hospitalized for more than 1 week. There was no significant difference in mortality during readmission vs. index admission (8.7% vs 7.0%, p = 0.49).
Hospital Characteristics of Readmission Hospitalization.
Most common reasons for 30-day readmission were stroke concerns in 28% (n = 32) and infection in 19% (n = 22) (Table 3). Of those with stroke, 22% (n = 7) were hemorrhagic including subarachnoid hemorrhage (n = 3). The time period with the greatest frequency of stroke contributing to readmission was within the first 3 days post-discharge (Figure 1). Leading etiologies of infection were the urinary tract (36%, [n = 13]) and the respiratory tract (34%, [n = 12]). Notably, 10% (n = 12) returned with a systemic bleeding complication and 4% (n = 5) a pulmonary embolism.
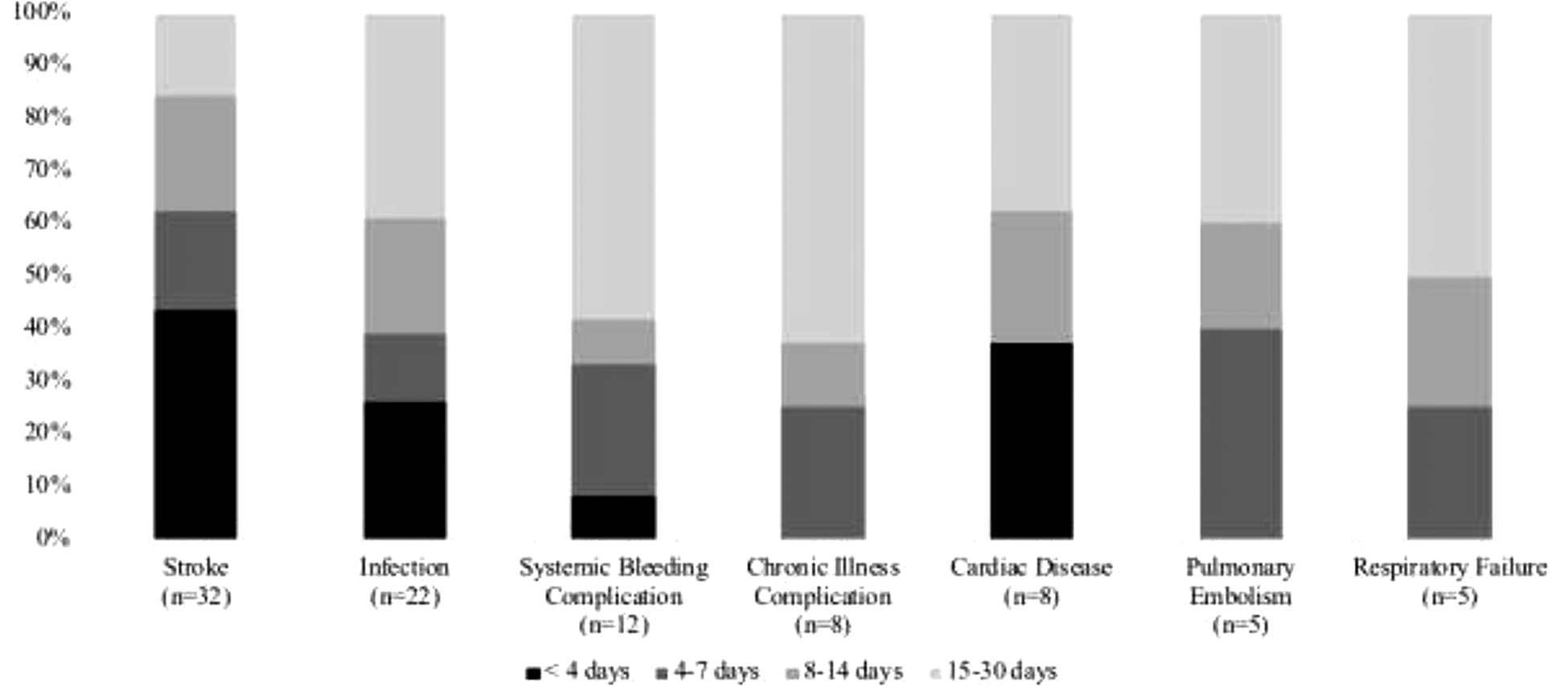
Leading causes of readmission and days to readmission.
Clinical Characteristics of Readmission Hospitalization.
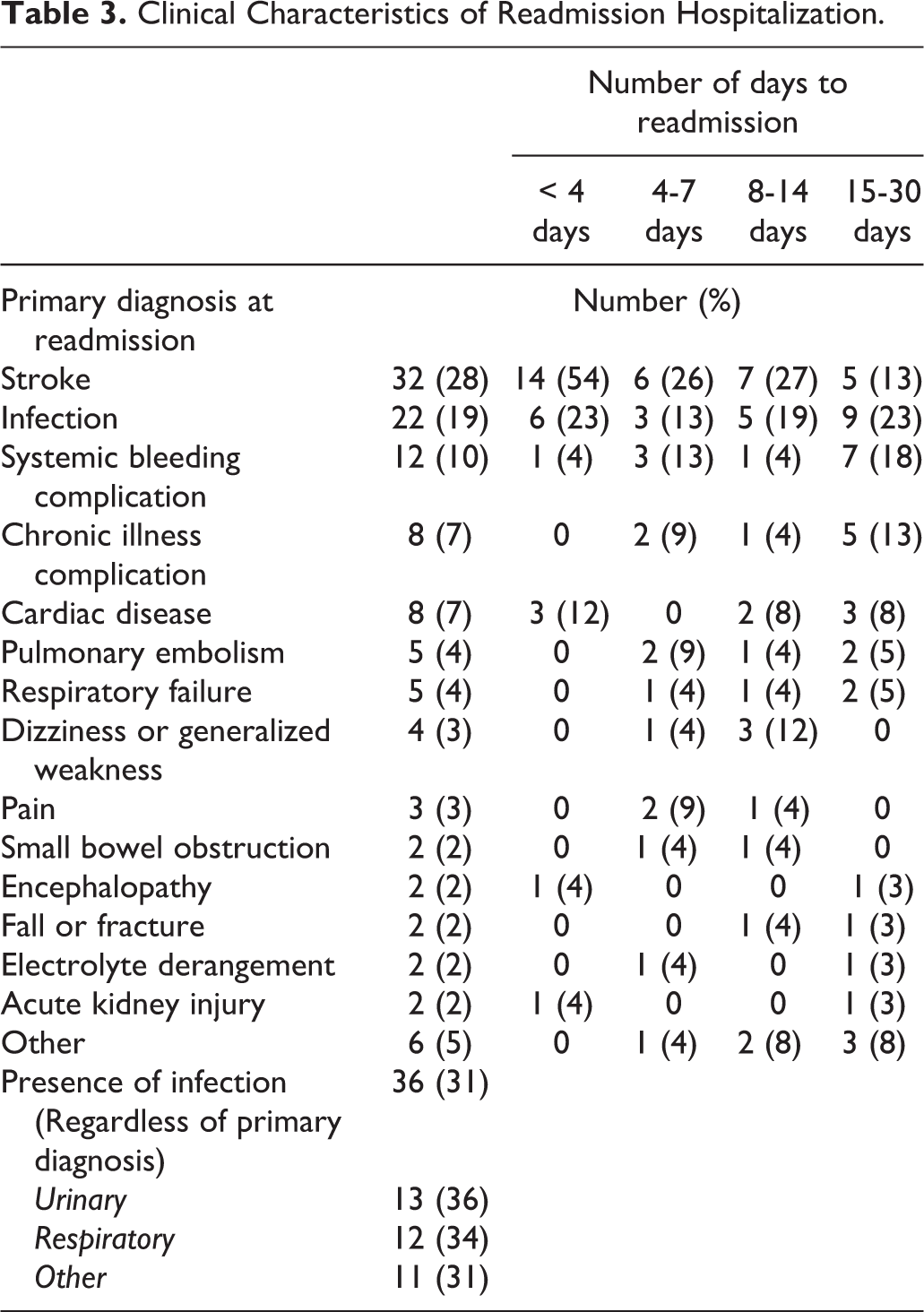
Table 4 shows the unadjusted odds for each 30-day readmission risk factor. In unadjusted modeling, NIHSS ≥ 5 was associated with the greatest odds for readmission (OR 5.0, p < 0.001) followed by LOS > 7 (OR = 2.3, p < 0.001). Prior stroke or TIA (OR = 1.6, p = 0.012), CAD (OR = 1.7, p = 0.007) and RI (OR = 1.8, p = 0.024) also increased odds of readmission in unadjusted models.
Risk Factors for 30-Day Readmission: Unadjusted Odds.
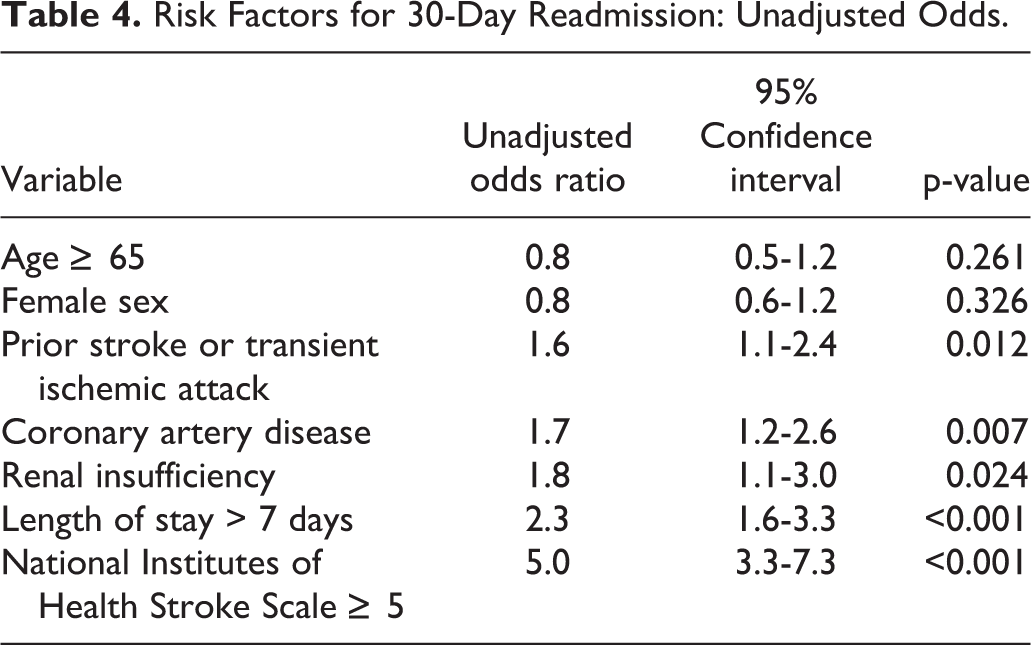
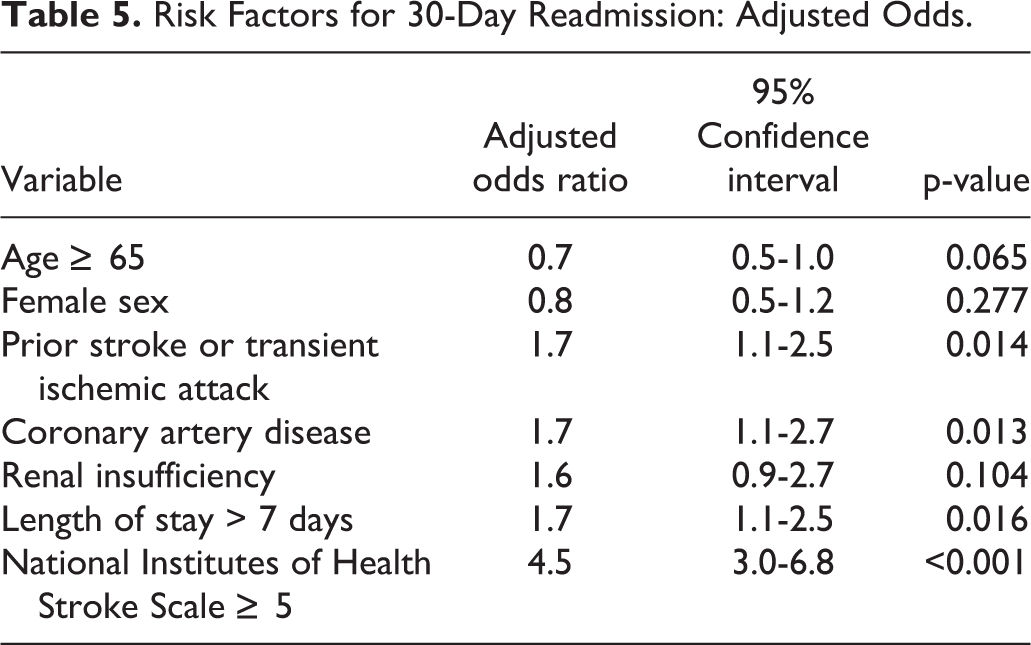
Table 5 shows fully adjusted odds for 30-day readmission. CAD (OR = 1.7, p = 0.013), history of prior stroke or TIA (OR = 1.7, p = 0.014), LOS > 7 (OR = 1.7, p = 0.016), and NIHSS ≥ 5 (OR = 4.5, p < 0.001) were associated with greater odds of 30-day readmission.
Risk Factors for 30-Day Readmission: Adjusted Odds.
Discussion
In this retrospective case-control study, 6.7% of patients were readmitted within 30-days and presence of CAD, history of stroke or TIA, LOS >7 days and NIHSS ≥ 5 predicted 30-day readmission in multivariate analysis. Patients were most often readmitted for stroke and infection, 65% were readmitted within 14 days post-discharge, and readmission LOS was > 7 days in half. Our study provides a thorough analysis of our metropolitan comprehensive stroke center’s contemporary population. It highlights the burden of stroke readmissions in the modern thrombectomy era and emphasizes the continued need for quality improvement initiatives.
The readmission rate of 6.7% over the 4 year study period is on the lower end of the range (6.4%-38.8%) reported in the literature.1-9 This rate may be lower than other institutions in part due to our institution’s dedicated stroke team, consistent with existing evidence that discharge of neurologic patients from a neurology service may lower odds of readmission.2,5 Furthermore, our study includes adults of all ages, instead of only Medicare beneficiaries, and although our data shows no significant relationship between age and readmission, older age has previously been shown to predict readmission.1,2,4,6,12
Medical comorbidity burden has been extensively examined in post-stroke readmission, yet risk factors for readmission vary across studies. Well-established stroke risk factors, such as HTN, DM, and AF, do not show consistent results. While our study and a 2016 meta-analysis with over 250,000 ischemic and hemorrhagic stroke and TIA patients show no significant relationship between these diseases and 30-day readmission, 3 some works suggest otherwise. A prospective cohort study found that DM and AF predict readmission while controlling for age and sex, and AF still predicted readmission in multivariate analysis at 1 year post-discharge 12 ; our study focuses on 30-day readmission so it is difficult to make direct comparisons. A retrospective case control study at a large tertiary care hospital, which included ischemic, hemorrhagic stroke and TIA patients also suggested that DM and AF predict 30-day readmission, yet found no significant effect of HTN. 2
As seen previously,1,3,12 we observe higher odds of 30-day readmission in patients with CAD. The 2016 meta-analysis noted that CAD was the second most common reason for 30-day readmission behind infection at both 30 days. 3 Recognizing that CAD, a key cause of cardiac disease, predicted readmission in our study, it may be interesting to further scrutinize the role of cardiac disease in post-stroke readmission and provide heightened attention to this population in the vulnerable acute post-stroke period. It is possible that a common risk factor profile across the 2 disease states can explain the association between IS and CAD. In addition to cardiac disease, renal disease may increase odds of 30-day readmission,4,13,14 although in our study RI was no longer a predictor after full adjustment.
Lack of early outpatient follow up, notably for renal disease and liver disease has been shown to increase risk of readmission after acute stroke. 5 Evidence suggests that outpatient follow up may be powerful in reducing 30-day readmission, and those who are readmitted are more likely to have missed follow up appointments.5,15 History of prior stroke or TIA has reliably been found as a risk factor for readmission when evaluated.2,12,15,16 Severity of comorbid chronic illnesses likely negatively impacts neurologic recovery from the burden of stroke. The presence of several chronic conditions, and prior stroke or TIA has been shown to increase risk of readmission as seen in our study.8,15
In addition to medical history, we identify LOS and stroke severity as important contributors to readmission. The 2016 meta-analysis found that patients with increased LOS and NIHSS were more likely to experience 30-day readmission. 3 It is possible that those with high comorbidity burden suffer more severe strokes, have higher NIHSS on admission, therefore requiring longer LOS, 17 and may ultimately have increased risk of returning to the hospital for reasons such as infection; stroke burden the immune system and the severity of stroke may correlate with the infectious risk.18,19 A single center study saw in multivariate analysis that only LOS > 10 days predicted 30-day readmission in patients with stroke and other cerebrovascular disease. 5 The burden of hospitalization is relevant, as patients with longer LOS appear more likely to have 30-day readmission.
Two nationwide studies, one with just Medicare beneficiaries 4 and one with all US hospitalizations 1 identified longer LOS among the variables that increase risk of 30-day readmission. Both of these studies were limited by lack of data on stroke severity, while our study controls for NIHSS in multivariate analysis. Considering that NIHSS may act as a strong predictor of LOS, 17 it is important to consider these factors together and adjust for stroke severity when evaluating this hospital-level factor. While we did not assess the impact of the index modified Rankin scale (mRs), baseline functional status certainly impacts outcomes. It is possible that those with higher mRs at baseline may experience a hindered recovery and experience longer LOS and/or greater risk of readmission. In our study significantly more patients with 30-day readmission were discharged to another healthcare facility such as acute rehab, subacute rehab, skilled nursing facility, and long-term care facility. Baseline level of functioning, stroke severity, and treatment outcome may all play a role, and those needing more assistance in the recovery period are often discharged to healthcare facilities.
The chief reasons for 30-day readmission in our study support previous work, namely stroke-related symptoms and infection primarily of the respiratory and urinary tracts.2,3,6,20 Some data suggests that up to 2% of 30-day stroke readmissions are preventable as classified by Agency for Healthcare Research and Quality Prevention Quality Indicators. 4 After stroke and infection, the next most frequent reasons for readmission were systemic bleeding complications, chronic illness complications, and cardiac disease. The reasons for infection in post-stroke patients are multifactorial yet the higher possibility of healthcare-associated infections after lengthier hospital stay should be recognized.19,20 We did not examine the impact of the presence of a Foley catheter or PEG tube, yet prior work has suggested these medical interventions may increase risk of infection and thus readmission.13,20 Generally, patients with more severe stroke and residual dysfunction may require catheters and tubes, and our study indicates that patients with greater stroke severity have higher odds of readmission. Readmissions with systemic bleeding complications, as well as thrombotic events, should always be examined closely to ensure patients were discharged on optimal antithrombotic medications.
Most patients were readmitted to a non-neurology service, which aligns with previous work, 2 and brings into question any potential benefits of continued involvement of the neurology team, considering that patients discharged from neurology services have been shown to have lower odds of readmission.2,5 Length of stay at readmission was >7 days in half. Previous literature looking at this topic demonstrated a median LOS at readmission of 4 days. 2 This may suggest a sicker population at our institution, but also emphasizes the significant burden of readmission to both patients and the healthcare system. To this end, 1 study with over 50,000 IS patients found that the average readmission related to stroke was 10.8 days, which was 3 times longer than index LOS. 9
The time period to readmission may present a critical time for interventions such as outpatient follow up and discharge phone calls to reduce risk of hospitalization. Median time to readmission at our institution was 9 days and comparable to other studies.5,8 Although stratifying by time to readmission leads to small sample sizes, systemic bleeding and chronic illness complications are 2 and 3 times more common, respectively, after 1 week compared to within the first week post-discharge. A retrospective cohort study of patients discharged home after IS showed that primary care follow up shortly after discharge was associated with fewer 30-day readmissions. 8 Despite recommending outpatient follow up, 1 study showed that only 14% of patients with 30-day readmission had 1 scheduled before discharge and inadequate outpatient care coordination was a leading cause of avoidable readmission. 5 Follow up with nurse practitioners in a prospective quality improvement study reduced 30-day readmissions in patients discharged home by almost half, although had no impact at 90 days. 15 Other evidence suggests that the positive impact of follow up on chronic and stroke-related issues may persist, with lower rates of readmission even after 6 months. 21 While not all readmissions are preventable, outpatient follow up may help reduce the number of readmissions resulting from preventable complications.
Much of the existing literature on stroke readmissions predates the modern endovascular era. However, stroke systems of care have evolved dramatically to expand access to life-changing thrombectomy care. The greater complexity in stroke care delivery potentially impacts characteristics of the acute hospitalization and post-hospitalization transition of care that alter risk of readmission. Data from the early thrombectomy era has suggested that those patients treated with thrombectomy who require transfer have greater length of stay, cost, and mortality than those who do not require transfer. 22 Data on the impact of transfer status on readmission specifically are lacking. Our study includes strong representation of patients treated with thrombectomy and transferred to the index hospitalization, reflecting the complexity of the modern endovascular era. As stroke systems of care continue to evolve to expand access to extended-window thrombectomy care, further research on the impact of treatment with thrombectomy and transfer status are needed.
Our study strengths include its thorough review of the contemporary stroke population at a metropolitan comprehensive stroke center. Updated data from the modern thrombectomy era are important to disseminate in order to evaluate whether factors contributing to readmission are evolving in the setting of this recent practice-changing treatment approach. Our study provides data on a substantial number of patients for a single center study, not limited to the Medicare population, including all adults over 18 years old. We include an extensive list of medical comorbidities and hospitalization factors, and important covariates such as LOS and NIHSS to control for potential confounders in our multivariate model. We focus on and provide details elucidating patterns of 30-day readmission in the immediate post-stroke time period by primary diagnosis, which represents a vulnerable, important time to intervene with readmission prevention strategies.
Limitations include its single center nature, although as a major metropolitan hospital, annual stroke volume is high and our study population is sizable. We did not capture readmissions to a different institution and it is possible patients were readmitted elsewhere or died after index admission. Our variables for analysis of patient characteristics and index admission were restricted to the components included on GWTG, and while this is a comprehensive database, certain variables that may be of interest are not included such as outpatient follow up. However, we performed chart review for the readmitted cases in order to gain more detail for reasons of return. Chart review has its own inherent limitations, and we aimed to reduce these by assessing inter-rater reliability and review data with our team’s vascular neurologist.
Our analysis of the contemporary stroke population at a metropolitan comprehensive stroke center highlights the significant burden of stroke readmissions and need for targeted quality improvement initiatives. Patients with complex medical comorbidities including CAD and history of stroke or TIA, severe stroke, and longer hospital stay would likely benefit most from such readmission reduction efforts. Prior work has suggested that 30-day readmission can be significantly reduced with targeted interdisciplinary efforts.5,8,13-15,21,23 and the prevalence of readmission with infection, stroke, and thrombotic and bleeding complications suggest that some of these readmissions may be preventable. Next steps will require the development of timely interventions in the 2 weeks post-discharge to target the most high-risk patients, and assess the impact of such interventions on patient and hospital outcomes.
Footnotes
Authors’ Note
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.