
Abstract
Patients with fixed and dilated pupils (FDPs) due to rising intracranial pressure (ICP) typically experience a deterioration in consciousness. We describe an exceptional case of a patient with bifrontal contusions who developed worsening edema and a unilaterally FDP while maintaining consciousness and the ability to communicate. A 58-year-old man with history of hypertension and diabetes mellitus type II presented after being assaulted, with bifrontal contusions and right frontal intraparenchymal hemorrhage. On hospital day 8, his right pupil became fixed (NPi 0) and dilated (4.8 mm). The patient was drowsy, arousable to tactile stimuli, answering questions, oriented to place and time, following commands on his right side, maintaining Glasgow Coma Scale of 14 (E4, V5, M6). He described complete loss of vision and could not identify objects or count fingers. His gaze was dysconjugate with impaired vertical excursion and inability to fully abduct to the right side. Corneal reflexes were intact bilaterally. Hypertonic saline and mannitol produced no improvement in his pupillary exam. Head computed tomography showed worsening midline shift and interval increase in subfalcine herniation related to increased peri-hematoma edema. We performed an emergent right-sided decompressive hemicraniectomy with durotomy and duraplasty. His pupil became reactive 5 hours after surgery. While FDP without deterioration of consciousness has been described due to traumatic subdural and epidural hematomas, we report this unusual constellation as a sign of rising ICP and impeding herniation due to intraparenchymal contusions, highlighting that any pupillary change warrants prompt work-up and intervention.
Introduction
A fixed and dilated pupil (FDP) is considered a grave sign in neurosurgical patients1-3 and correlated with poor neurological prognosis and high mortality. 4 In a patient with deteriorating consciousness, FDP is a recognized indicator of acute brainstem compression. 5 Here, we describe an exceptional case of a patient with bifrontal contusions who developed worsening edema and brainstem compression, manifesting with FDP while remaining conscious and conversant, and review the pertinent literature on this topic.
Case Description
Our institutional review board did not require approval or consent for this case report, including deidentified information appropriately compliant with institutional requirements.
A 58-year-old man with a prior history of hypertension and diabetes mellitus type II presented after hitting the back of his head during an altercation. On initial examination, Glasgow Coma Scale (GCS) was 14; he was drowsy but able to answer orientation questions appropriately, followed commands with his right side, and had a left hemiparesis. Pupils were equal, round, and reactive to light. Non-contrast head computed tomography (CT) demonstrated bifrontal contusions, including a right frontal intraparenchymal hemorrhage (ICH) measuring 4.5 × 3.0 × 3.5 cm (Figure 1A), with 4 mm midline shift and minimal subfalcine herniation (Figure 1B). Head computed tomography at the time of presentation showing bifrontal contusions and no midline shift (A and B). Repeat head computed tomography obtained due to decreased mental status showing worsening bifrontal edema with 7 mm of right-to-left midline shift (C and D). Head computed tomography obtained after right NPi became 0 showing increasing edema around his right frontal contusion, now with 9 mm of right-to-left midline shift, with mildly increased right-to-left subfalcine herniation and similar effacement of the right perimesencephalic cistern compared to prior (E and F).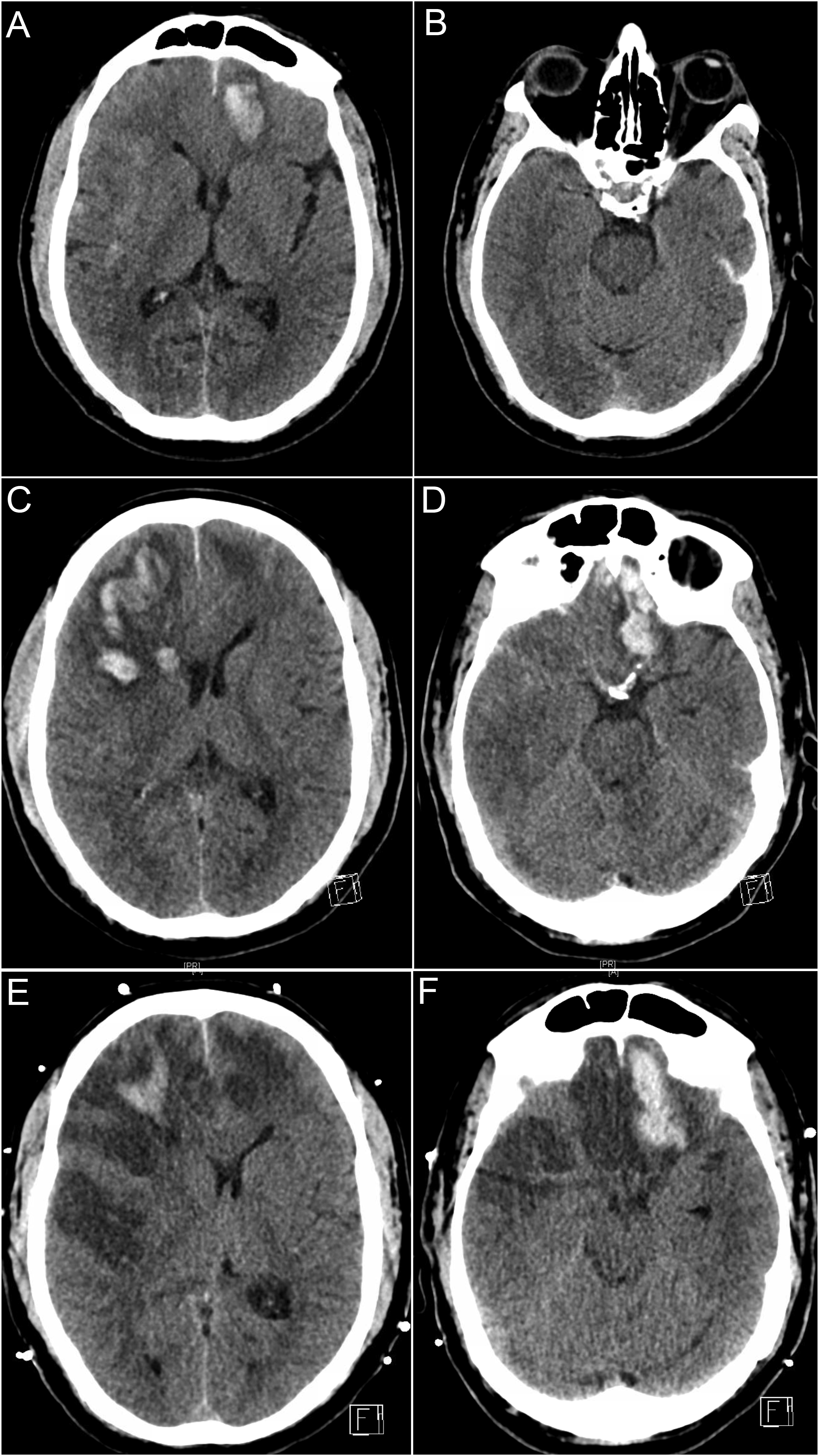
For the next 5 days, the patient’s neurologic exam remained stable, although head CT on hospital day (HD) 4 demonstrated blossoming of contusions and worsening edema with increased right-to-left midline shift from 4 to 7 mm (Figure 1C) and right uncal herniation (Figure 1D). On HD 7, he became drowsier but followed commands and remained easily arousable. Repeat head CT was stable. Continuous electroencephalographic monitoring showed no evidence of seizures.
On HD 8, his right pupil became dilated and unreactive. Pupillometer (NeurOptics, Irvine CA, USA) exam demonstrated a decrease in Neurological Pupil index (NPi) on the right from 4.4 to 0 and increased diameter from 2.5 to 4.8 mm (left pupil: NPi 3.6, diameter 2.4 mm). Surprisingly, his mental status exam at the time remained stable (GCS 14: E4, V5, M6). He was able to answer orientation questions, follow commands, and reported bilateral loss of vision with minimal light perception. He did not blink to threat, corneal reflexes remained intact, gaze was dysconjugate with limited vertical excursion, and he had right abducens palsy. Treatment with mannitol (administered 30 min after first noticing the FDP) and 23% hypertonic saline (administered 130 min after detection of the FDP, following the head CT and en route to the OR) did not change his pupillary exam. An emergent head CT (Figure 1E) (completed at 100 min after FDP detection) showed increasing edema around his right frontal contusion, 9 mm right-to-left midline shift, and worsening uncal herniation with effacement of the right perimesencephalic cistern (Figure 1F). An emergent right decompressive hemicraniectomy (started at 150 min after FDP detection) with durotomy and duraplasty was performed.
Postoperatively, his head CT demonstrated adequate decompression. His pupil became reactive to light (NPi: 1.8 mm) 5 hours after surgery, with NPi 4.1 mm at 24 hours.
The patient’s neurological exam remained stable; he was discharged to inpatient rehabilitation on postoperative day 30. Four months following his initial injury, he underwent autologous cranioplasty without complication. At a follow-up visit 8 months after his injury, he continues to have a spastic left hemiparesis requiring a wheelchair; he is able to communicate with brief phrases, exhibiting residual cognitive deficits affecting attention, initiation, short-term memory, and executive functions; and enjoys spending time with his young granddaughter.
Review and Summary of the Literature
Summary of literature describing isolated oculomotor nerve palsy with preserved consciousness.
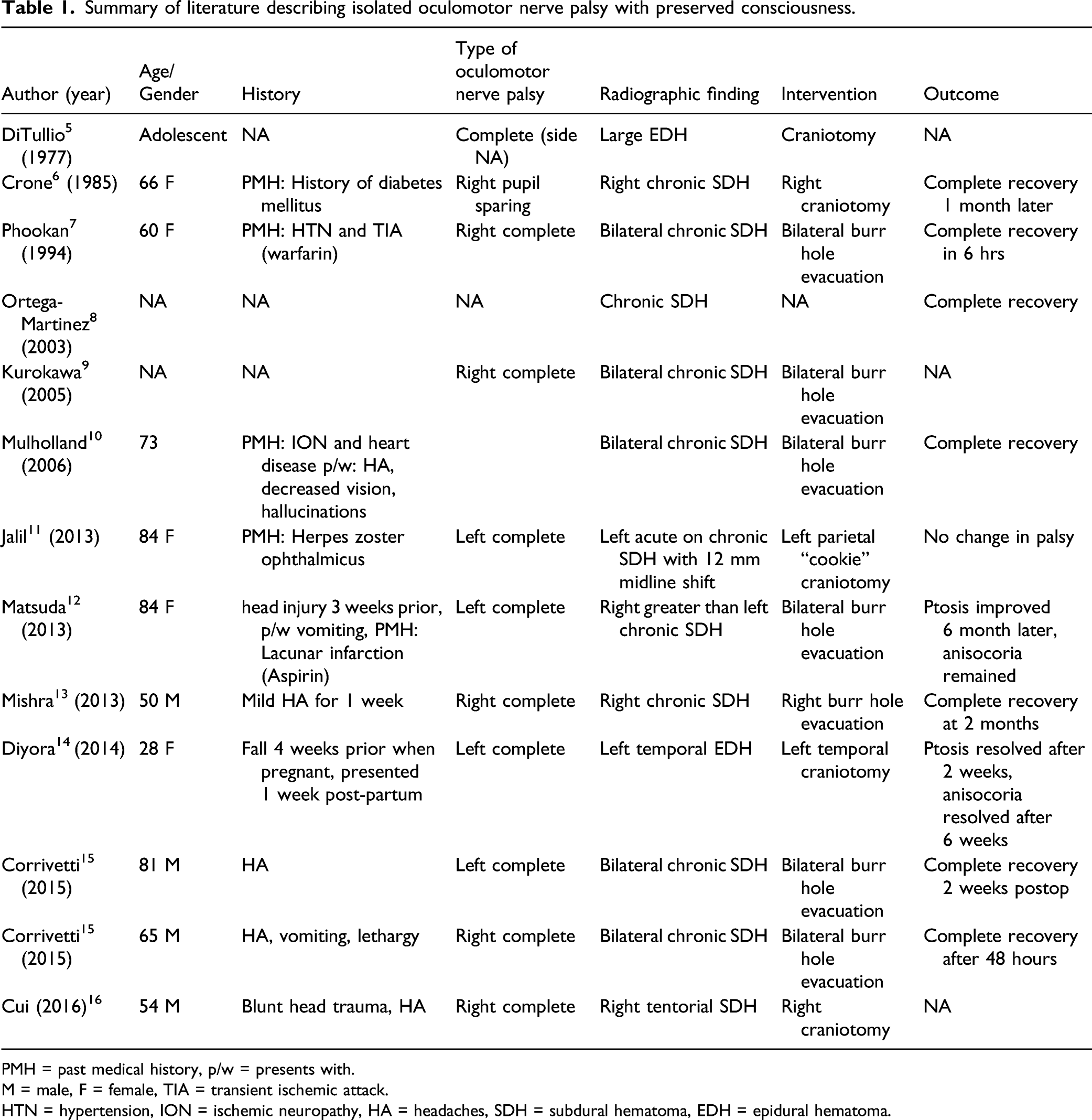
PMH = past medical history, p/w = presents with.
M = male, F = female, TIA = transient ischemic attack.
HTN = hypertension, ION = ischemic neuropathy, HA = headaches, SDH = subdural hematoma, EDH = epidural hematoma.
Discussion
Isolated OMN lesions have been associated with a variety of etiologies and are commonly described in the context of microvascular infarction, compression from a posterior communicating artery aneurysm, neoplasia, and inflammatory conditions, as well as traumatic axonal injury. However, the occurrence of an isolated OMN due to elevated intracranial pressure (ICP) without deterioration of consciousness is extremely unusual. The classic reference, Plum and Posner’s Diagnosis of Stupor and Coma, states, “A pupillary dilation from uncal herniation with preserved level of consciousness is rare enough to be the subject of case reports.” 6 As described above, only few cases of isolated OMN in the context of traumatic ICH have been reported, all of which were due to chronic SDH or EDH. To the best of our knowledge, this is the first case reporting complete loss of pupillary reflex (NPi: 0) with preserved consciousness due to an intraparenchymal traumatic contusion resulting in increasing ICP and impeding herniation.
Historically, German internist Ernst Von Leyden was the first to experimentally demonstrate a relationship between FDPs and increased ICPs by injecting protein solutions intracranially (1866). He noted the phenomenon was associated with coma and deduced that in the absence of impaired consciousness, the pupillary dilation could be attributed to a peripheral OMN lesion. 5 To this day, we differentiate between pupillary dilation due to increased ICP and brainstem compression vs an isolated peripheral OMN lesion based on the neurological exam; pupillary changes in the context of increasing ICP are typically associated with deteriorating mental status. 2 The assumption is that the reticular formation, consisting of fibers immediately dorsal to the OMN within the midbrain, is primarily affected by downward herniation before the OMN, as components of the reticular activating system (RAS) are superior to the path of the OMN.
Our case is remarkable in the peculiarity of the patient’s ability to follow commands, communicate, and even report visual loss despite increased ICP and mass effect on his brainstem. Compression of the dorsal surface of the OMN from the increase in right uncal herniation could explain the unilateral pupil dilation, as could worsening midline shift with stretch of the OMN. The patient’s acute vision loss could be attributed to optic nerve compression or compression of the posterior cerebral arteries against the tentorium, causing ischemia of the occipital lobes and cortical blindness 9 ; in similar scenarios, these symptoms are not reported at the time of the injury due to associated loss of consciousness.
One possible anatomical explanation for preserved consciousness in this case could be the predominant increase in subfalcine herniation and preserved perimesencephalic cisterns, suggesting that the more anterior structures were primarily affected by the worsening edema and shift, rather than by downward herniation, resulting in sparing of the RAS and its prosencephalic projections. Alternatively, the FDP could have been caused by compression of the OMN due to uncal herniation with early superimposed, evolving brainstem compression not yet manifesting in decreased consciousness. Also, in reviewing the literature, several reports of similar cases with isolated FDP had a prior history of microvascular disease (e.g., due to diabetes mellitus) or nerve injury (e.g., prior herpes zoster ophthalmicus), potentially predisposing the patient to OMN injury.17–26 Our patient also had diabetes mellitus type II, and chronic microangiopathic changes might have contributed to the early development of an OMN palsy.
NPi changes without altered consciousness among patients with traumatic brain injury have been described in the context of other mechanisms. Chen et al describe the case of a 67-year-old man who suffered a fall; his only deficit was right-sided decrease in NPi. Head CT showed prepontine hemorrhage with presumed OMN compression by the clot. 7 Joseph et al 8 describe decreases in pupil dilation velocity and percent change in pupil diameter in otherwise asymptomatic high-school football athletes who sustained high-acceleration head impacts, which was attributed to axonal injury. In addition to providing information about OMN function, the NPi has been investigated as a non-invasive tool to measure ICP, along with other modalities such as optic nerve sheath ultrasound and diameter (ONSD), 10 pulsatility index, and transcranial doppler (TCD). 1 With current studies demonstrating mixed results with regards to the association between NPi changes and increased ICP,2-4 further research is needed to establish the prognostic value and utility of NPi in guiding clinical decision making.
In conclusion, any pupillary change in the appropriate clinical context should prompt swift action regardless of level of consciousness. Atypical presentations of an isolated OMN lesion with preserved consciousness might prompt providers to look for other etiologies of FDP and could delay emergent interventions necessary to prevent herniation. In our patient, associated neurological findings, including visual loss and abducens palsy, strongly suggested acute intracranial pathology. Other non-invasive ICP measurements such as ONSD and TCDs can confirm the suspicion of elevated ICP. Recognizing this uncommon presentation is of critical importance, as prompt neurosurgical decompression appears to result in good recovery of the third nerve in most cases.
Supplemental Material
sj-pdf-1-nho-10.1177_19418744211056613 – Supplemental Material for Fixed, Dilated, and Conversing—Unreactive Pupil With Preserved Consciousness Indicating Acutely Rising Intracranial Pressure due to Traumatic Intraparenchymal Contusions: Case Report and Review of the Literature
Supplemental Material, sj-pdf-1-nho-10.1177_19418744211056613 for Fixed, Dilated, and Conversing—Unreactive Pupil With Preserved Consciousness Indicating Acutely Rising Intracranial Pressure due to Traumatic Intraparenchymal Contusions: Case Report and Review of the Literature by Malia McAvoy, Gina Lee, Scott Boop, Madeline E. Greil, Kayla A. Durler, Christopher C. Young, Lindy Craft, Randall M. Chesnut and Sarah Wahlster in The Neurohospitalist
Footnotes
Acknowledgments
The authors appreciate the assistance of Sharon Durfy, PhD, with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.