
Abstract
We present the case of a 73-year-old woman with a 3-month history of non-traumatic thoracic myelopathy. Initial MRI showed a T6-conus T2 signal hyperintensity. Based on this presentation, and given a personal and family history of autoimmune disease, our patient was first managed as an inflammatory transverse myelitis. Subsequent worsening after lumbar puncture and steroids prompted re-evaluation, ultimately identifying the cause as a thoracic spinal dural AV fistula. Both investigation of possible transverse myelitis with lumbar puncture and empiric treatment with steroids may not only result in diagnostic delays but also precipitate venous infarction and irreversible harm. While the MRI often provides the initial diagnosis, clinical suspicion for this under-diagnosed cause of myelopathy should be raised in older patients with a more progressive thoracic myelopathy with worsening after lumbar puncture and/or steroids. Definitive and time-sensitive treatment by interventional neuroradiology or neurosurgery results in stabilization or improvement of disability in most cases.
Section 1
A 73-year-old previously independent woman presented to the emergency department (ED) with a 3-month history of progressive lower limb weakness and sensory loss. She first developed bilateral lower limb numbness and tingling with mild weakness requiring a cane. Her symptoms then progressed such that at the time of presentation she had reduced sensation to the groin and was barely able to stand with a four-wheel walker. There was no bowel or bladder disturbance. There was no history of trauma, and no constitutional features such as fever or weight loss. Her past medical history was significant for chronic low back pain due to an injury and lumbar degenerative disk disease. She also had ulcerative colitis (in remission on Ustekinumab), right breast invasive ductal carcinoma (curative lumpectomy 2 years prior) and medically managed coronary artery disease, type II diabetes, hypertension, and dyslipidemia. Family history was significant for a daughter with multiple sclerosis. Outpatient electrodiagnostic testing 1-month prior had shown a mild length-dependent symmetrical axonal sensorimotor polyneuropathy.
On examination in the ED, cognition and cranial nerves were normal. Motor exam was normal in the upper limbs. In the lower limbs, hypotonia was noted with 4/5 power bilaterally on hip and knee flexion and extension and ankle dorsiflexion with normal foot plantarflexion. Bilateral patellar reflexes were 2+, Achilles reflexes were 1+ on the left and absent on the right, plantar responses were extensor bilaterally, and she had a crossed adductor reflexes. Sensory examination revealed diminished of pinprick/light touch sensation to the upper thigh (L1/L2 dermatome), absent vibration sensation below the knees, and proprioceptive errors at the great toes. On the abdomen and back, she had normal small fiber sensation with no sensory level and had no saddle anesthesia. Her gait was wide-based and she could only ambulate short distances.
Questions for Consideration
What is the localization of the above presentation?
What differential diagnoses would you consider?
Section 2
The presentation with isolated lower limb weakness, sensory loss, and some upper motor neuron findings raised suspicion for an incomplete myelopathy, with examination findings exclusively below the L1 level. The lower motor neuron features were thought to represent the superimposed axonal sensorimotor polyneuropathy that had recently been demonstrated on nerve conduction testing related to her diabetes.
Demyelinating or systemic inflammatory transverse myelitis (TM) was felt to be the most likely diagnosis given the subacute, non-traumatic, and incomplete presentation with a personal history of ulcerative colitis and a family history of MS. Thoracic degenerative disk disease was to be urgently excluded given her history of chronic back pain but felt to be less likely given the subacute progression changes without recent trauma. Alternative considerations included infection (given the prolonged immunosuppression), malignancy or paraneoplastic process (noting the breast cancer history from 2 years prior), nutritional causes (ulcerative colitis possibly causing malabsorption in the terminal ileum), or vascular causes.
An overnight MRI scan without contrast was obtained, suboptimal due to movement artefact, and reported as showing a T2 sequence hyperintensity extending from T6–T7 level to the conus medullaris at L1–L2 level (Figure 1), favored to represent acute TM. MRI with contrast and MRI angiogram had also been initially requested but were deferred due to the difficulty obtaining a contrast enhanced study after hours. Bloodwork was significant for a mild neutrophil-predominant lymphocytosis. Recent results as part of ulcerative colitis follow-up included a normal ESR and CRP but positive ANA (1:320, homogenous), ANCA (cANCA high positive). Testing 6 months prior for TB, HIV, and hepatitis B and C had been negative. Longitudinally extensive spinal cord lesion on MRI. Sagittal T2 weighted MRI of the patient’s spine shows spinal cord hyperintensity from the T6 vertebral level to the conus medullaris (A) and encompassing the majority of the cross-section of the spinal cord in axial view (B).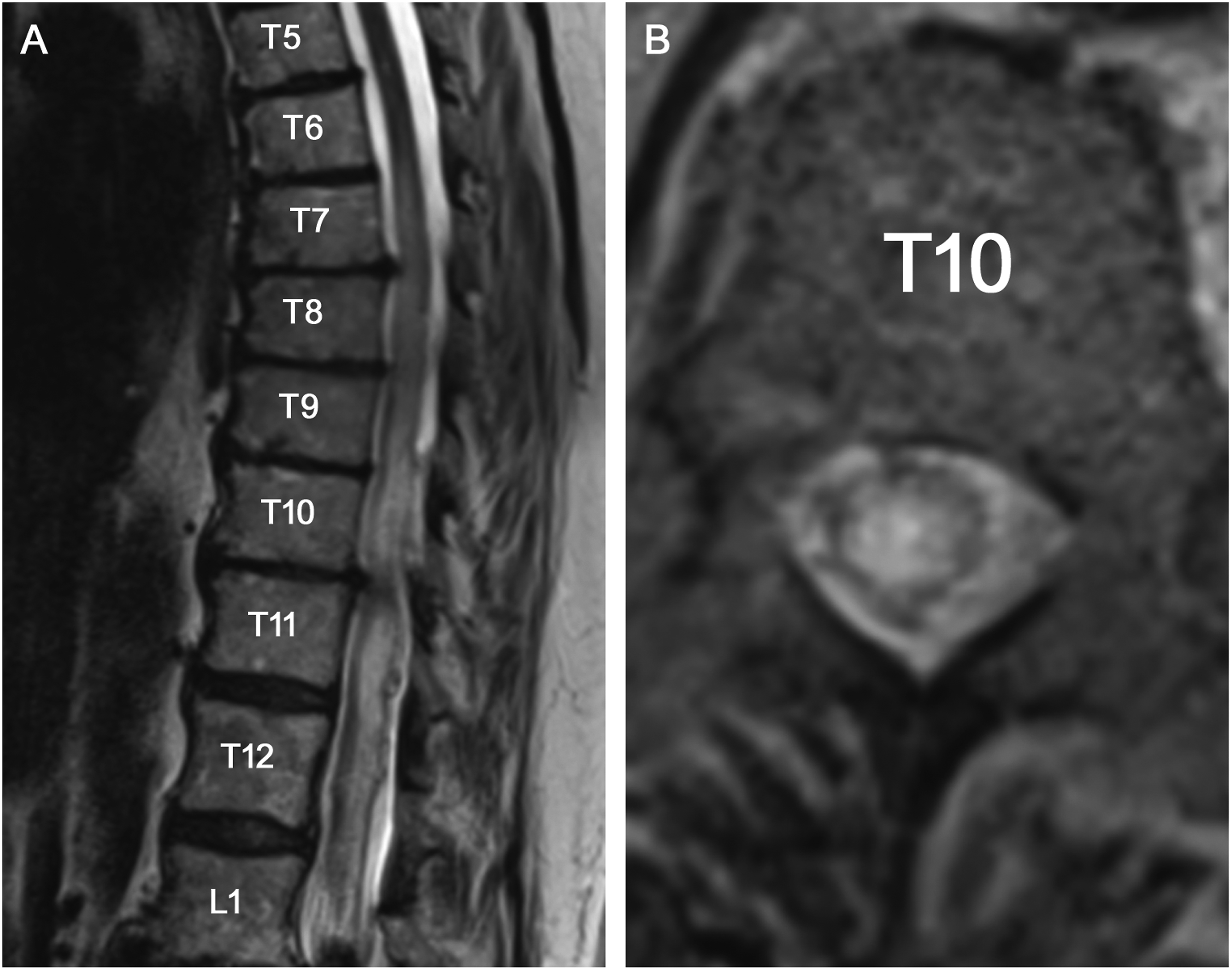
Questions for Consideration
What additional testing would you pursue?
What empiric treatments would you consider?
Section 3
A lumbar puncture was undertaken. Preliminary CSF testing was unremarkable with protein concentration of 41 mg/dL, nucleated cell count of 3 and negative gram stain. With a low risk of occult infection, the patient was started on IV methylprednisolone 1 g/day for a planned course of 5 days. Subsequent CSF testing included oligoclonal bands (mirror pattern), cytology (occasional white cells), bacterial culture, PCR for VZV, VDRL, and flow cytometry (all negative). Additional blood testing included serologies for VDRL, Lyme, HSV, VZV, CMV, and HTLV-1/2 (all negative). Inflammatory serologies included anti-aquaporin-4 and MOG and paraneoplastic antibodies (all negative). Nutritional studies revealed normal B12, copper zinc, and vitamin E.
Within hours of the lumbar puncture and steroid initiation, the patient’s status deteriorated acutely. The on-call team was asked to assess her as she could no longer ambulate to the washroom and could barely move her legs. On exam, she was found to have flaccid paraplegia with absent reflexes.
Question for Consideration
Given the precipitous deterioration despite steroid therapy, what additional testing would you arrange to explore alternative diagnostic considerations?
Section 4
A repeat MRI with angiogram (MRA) was ordered due to the concern of a vascular etiology of such a precipitous worsening of her neurological function. MRA revealed a dilated radicular artery at T11/T12 terminating in a hyperintense pocket (Figure 2(A)), also seen on axial imaging (Figure 2(B)). This finding was consistent with a left spinal dural arteriovenous fistula (SDAVF) at T12. The repeat MRI also revealed the presence of dilated perimedullary vessels seen as flow voids on the MRI not appreciable on the initial scan. Dural arteriovenous fistula visualized on MRI and angiogram. Magnetic resonance angiography with maximal intensity projection (MIP) reconstruction (A) shows the dilated T12 radicular artery terminating in the fistulous pouch (arrow). The fistulous pouch is also shown in axial view with T1 VIBE sequence (B). Digital subtraction angiography (DSA) of the T12 vertebral artery showing filling of the fistulous veins (C).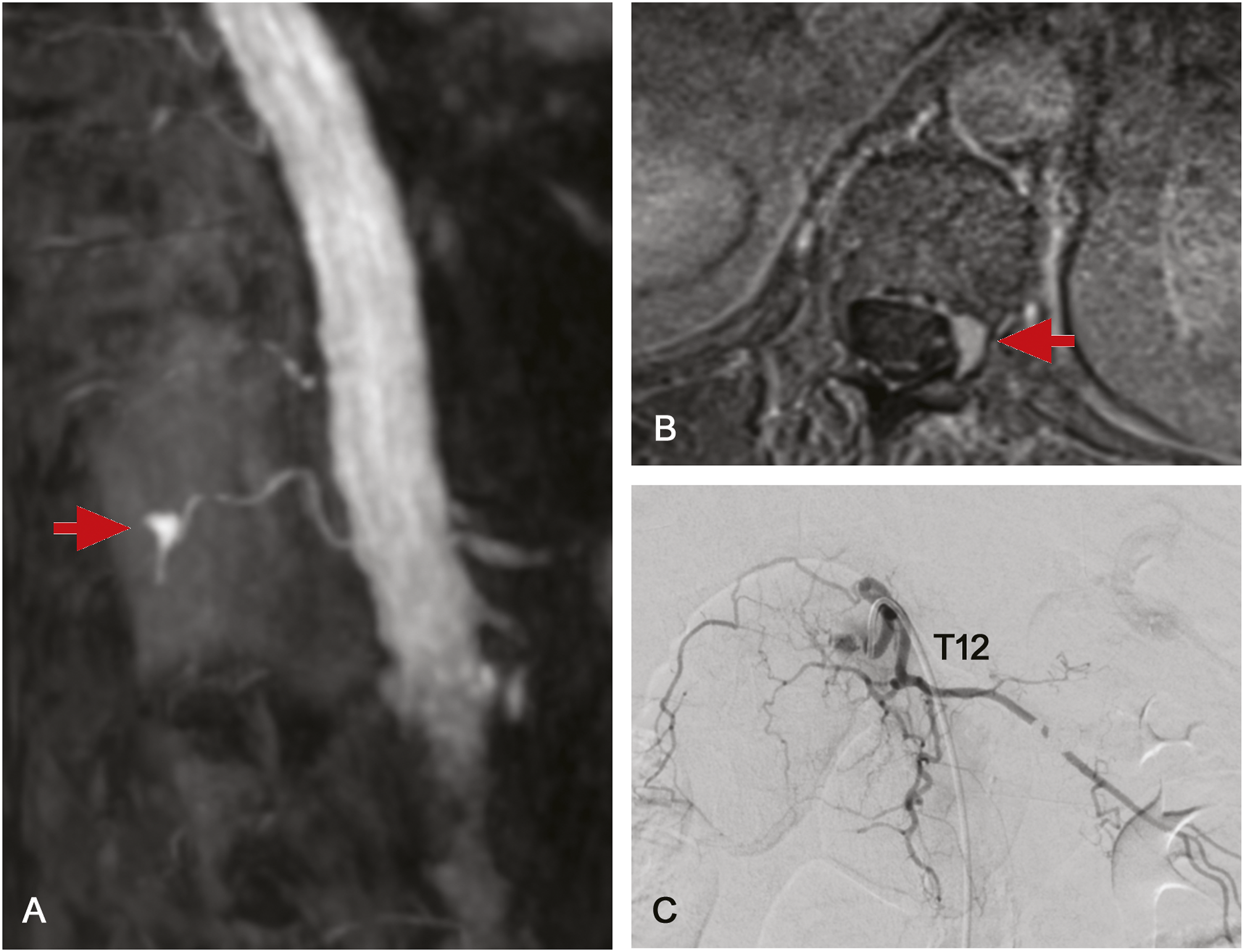
Questions for Consideration
How is this condition managed?
Section 5
Neurosurgery was immediately involved given the sudden worsening of her lower limb weakness in the context of the SDAVF. The patient was taken to the angiography suite to confirm the diagnosis and attempt embolization. On digital subtraction angiography (DSA), the pathologized arterial branch of the left T12 radicular artery was identified (Figure 2(C)). However, endovascular embolization was contraindicated as the artery of Adamkiewicz and its possible anastomotic contributions could not be visualized, the embolization of which could precipitate a large spinal stroke. To facilitate efficient intra-operative identification of the lesion, a coil was deployed into the left T12 radicular artery. The patient was then taken for T11 and T12 bilateral laminectomy and disconnection of the SDAVF. The surgery was uncomplicated. After 2 months of inpatient rehabilitation, she was able to ambulate with a 4-wheel walker. At this point, repeat MRI of the spine with contrast revealed persistent stable extensive cord signal abnormality and enhancement.
Discussion
Spinal dural AV fistula (SDAVF) is the most common vascular malformation of the spinal cord and is an under-appreciated cause of myelopathy. 1 Abnormal connections form between the radicular arteries and veins, typically in the neural foramina. 2 Venous arterialization subsequently results in venous hypertension, and ultimately venous infarction, classically in the thoraco-lumbar region. Initial misdiagnosis of SDAVF as inflammatory transverse myelitis (TM) is common, and neuroradiologists are often the first clinicians to raise the possibility of SDAVF. In one case series of patients referred to a specialist clinic for management of idiopathic TM, 2% were ultimately diagnosed with SDAVF as the cause. 3 This not only leads to delays in time-sensitive treatment, but presumptive TM investigation with lumbar puncture and empiric management with steroids may directly precipitate venous infarction and cause irreversible harm. Our case highlights pertinent clinical and MRI findings and the importance of rapid clinical and MRI recognition.
In our case, clinical clues of SDAVF rather than TM at first presentation included progressive deterioration over months of an incomplete thoracic myelopathy (rather than days-weeks), superimposed sensorimotor axonal neuropathy, older age of onset (40’s–80’s), recent worsening of back pain with distant back trauma, 4 and atypically bland CSF. In most patients, additional early history features often include gait disturbance, asymmetric/ascending sensory disturbance (including radicular symptoms and patchy sensory loss), and later bowel/bladder involvement. 5 Diagnostic delay was caused by the lack of high-quality MRI images. Episodic worsening is an important diagnostic clue, presumably due to transient exacerbations in venous hypertension. Triggers include Valsalva, and as highlighted by our case, IV steroids 6 and lumbar puncture. 7 Corticosteroid worsening may be mediated though mineralocorticoid and saline-induced fluid retention; elevation in venous hydrostatic pressures may further compromise the already fragile venous return into the dural sack, contributing to infarction. Exam can reveal a mixed picture of asymmetric upper and lower motor neuron features 8 and sacral involvement due to involvement of the conus.
With a reader-dependant sensitivity of 80–100%, a high-quality MRI of the whole spine accurately interpreted in the clinical context is the most important initial investion. 9 Inclusion of angiographic sequences does not improve sensitivity but assists in determining the level of involvement. 9 As highlighted by our case, T2 signal hyperintensity is reported in 78–85%,10,11 with additional MRI features including hazy, longitudinally extensive, central signal with cord edema and enhancement, often seen extending from the thoracic region to the conus.11,12 These features noted in isolation could be associated with inflammatory or demyelinating causes. However, the presence of engorged perimedullary veins either as T2-sequence flow voids or, as in our case, better visualized on contrast-enhanced T1 sequences, is more specific, reported in 88% of cases. 11 Due to the risk of venous hypertension, lumbar puncture should be avoided, although as in our case usually reveals a non-inflammatory picture. 13 While nerve conduction studies are not indicated, a polyradiculopathy has been reported. 8 Although digital subtraction angiography is the gold standard diagnostic test, MRI angiogram still has an excellent sensitivity and specificity for both diagnosis and localization of the lesion prior to operative intervention.
While traditional surgical disconnection remains the most successful approach, embolization by DSA is often preferred as a first line approach as it enables treatment at the time of diagnosis in 70–80% of cases and reduces the need for open surgery with associated morbidity. 14 As demonstrated here, if, during spinal angiography, endovascular embolization is felt to be unfavorable, a coil is often deployed endovascularly to help the surgeon locate the spinal level using intra-operative fluoroscopy, minimizing resection and duration of surgery. Prognosis is associated with pre-operative weakness severity, and more than two-thirds of cases either improve or stabilize following treatment. 15 T2 hyperintensity is commonly seen on initial follow-up, resolving in a majority of treated patients. Any recurrence of flow voids should raise concern for treatment failure.
Footnotes
Author contribution
ST, WK and JH collected and synthesized data; drafted the manuscript for intellectual content. GBW, BD and TAF revised the manuscript for intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.