
Abstract
Objectives
(1) To describe the existing literature on procalcitonin (PCT) as a biomarker in patients with acute rhinosinusitis (ARS), (2) to analyze outcomes in ARS patients who were treated with PCT-guided therapy versus traditional management, and (3) to compare PCT to other biomarkers used in diagnosis of bacterial ARS.
Results
The 2 RCTs demonstrated a reduction (41.6% in 1 study and 71% in the other) in antibiotic prescription rate in the PCT-guided group versus the control group with no change in the number of days with impaired activity due to illness (9.0 vs 9.0 days [P = .96]; 8.1 vs 8.2 days [95% confidence interval −0.7 to 0.7]), number of days of work missed, and percentage of patients with persistent symptoms at 28 days. In the observational cohort studies, PCT did not consistently correlate with C-reactive protein, body temperature, and/or white blood cell counts.
Conclusions
The limited existing literature on the role of PCT in diagnosis, management, and prediction of clinical outcomes in ARS suggests that PCT-based guidelines for antibiotic prescription are a safe and effective method of minimizing unnecessary antibiotic use.
Introduction
Antibiotics are widely prescribed in a variety of health-care settings for the management of acute rhinosinusitis (ARS).1–2 However, the role of antibiotics in these patient populations is poorly understood, and prediction of who will benefit from antibiotic treatment is difficult.Although antibiotics modify the course of ARS for some patients, the number needed to treat is high and most cases are self-limited. 3 For uncomplicated ARS, recent randomized control trials (RCTs) demonstrated no or minimal benefit with the use of antibiotics.4–6 However, rhinosinusitis (RS) accounts for the most adult outpatient antibiotic in the United States. 7 The vast majority of ARS episodes are viral infections with bacterial infections complicating only 1% to 2% of cases.8–10 Practice guidelines recommend against antibiotics for ARS unless evidence of bacterial infection is present. 11 Nonetheless, antibiotics are prescribed in >80% of ARS visits. 9 ,12–19 Although clinical characteristics such as nasal obstruction, facial pain, purulent rhinorrhea, and prolonged duration of symptoms are commonly used to justify antibiotic treatment, 15 studies have found that these symptoms do not adequately distinguish bacterial from viral ARS. 20 , 21 Middle meatal swab or sinus aspirate cultures are suggested as the gold standard to determine bacterial ARS, but these techniques have low sensitivity and lack practicability.
Procalcitonin (PCT) has emerged as a potential diagnostic marker of bacterial infection and has been studied with regard to outcomes in sepsis, 22 pneumonia, 23 , 24 and endocarditis. 25 PCT release is mediated by cytokines that increase in response to bacterial infection such as tumor necrosis factor α and interleukin 1 beta 26 and suppressed by interferons released in response to viral infections. Although a range of cut-off values for PCT have been defined based on prior observational studies, recent studies have found that PCT levels greater than 0.10 ng/mL 25 or 0.25 ng/mL 24 provide safe and efficacious cut-off values for PCT-guided antibiotics in management of the aforementioned bacterial infections. Thus, postulating that elevated PCT levels (ie, greater than 0.10 ng/mL) can be used with history, physical exam, and nasal endoscopy to identify patients with bacterial ARS is reasonable. As such, PCT levels could be used to stratify patients to appropriate treatment groups and minimize unnecessary antibiotic use. The objective of this study is to systematically evaluate the existing literature with regard to the utility of PCT in diagnosis and management of ARS.
Methods
This review was conducted based on the 2009 Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 27 In this review, we present all studies up to September 2017 that analyze the role of PCT in patients with ARS with regard to (a) prognostic value of PCT levels in predicting clinical outcome, (b) noninferiority in outcomes for patients randomized to observation instead of antibiotic therapy based on PCT levels, and/or (c) correlation of PCT with sinonasal cultures.
Search Strategy
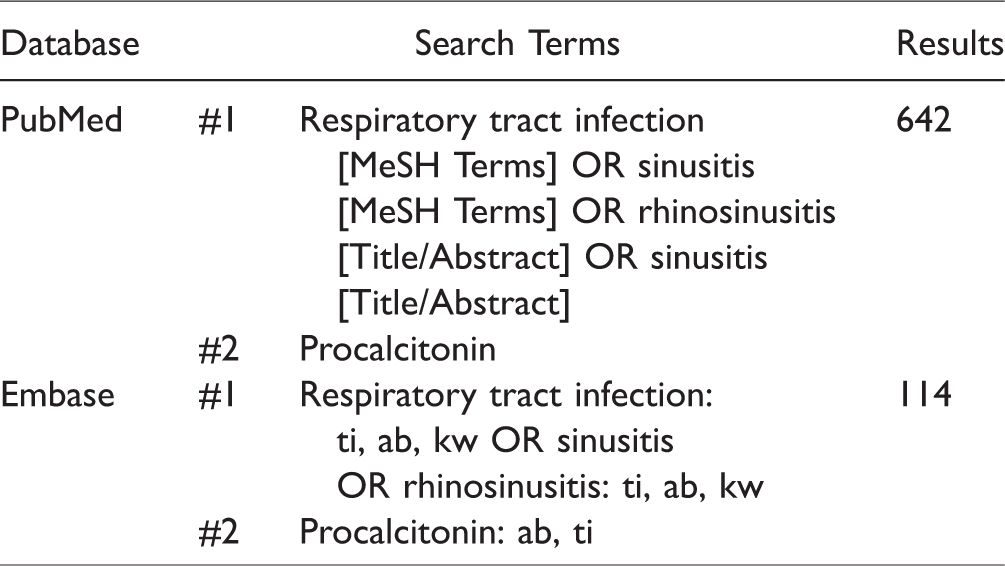
Relevant literature was identified by a systematic search of PubMed and Embase databases using the following terms as detailed in Table 1: RS, upper respiratory infection, and PCT.
Search Databases and Filters.
Study Selection
Articles were identified on September 14, 2017, from the date of database inception using the search strategy noted earlier. Inclusion criteria for this study consisted of RCT or prospective cohort studies that analyzed the role of PCT in patients with acute or chronic sinusitis. Given the small number of studies, we did not exclude studies based on subgroup analysis (ie, no analysis of the sinusitis group alone). We excluded animal studies, case reports, articles written in languages other than English, and duplicates based on review of titles and abstracts. Prior systematic reviews and meta-analyses that included patients with sinusitis were excluded from this analysis but will be addressed in the discussion. In addition, studies that focused exclusively on biomarkers other than PCT or diseases other than sinusitis, lower respiratory tract infections (RTIs), pneumonia, influenza, sepsis, and generalized RTIs without specified inclusion of sinusitis were excluded.
Two authors (S.S.S. and A.E.D.) independently screened the first 250 of 727 (34%) nonduplicate titles and abstracts (in alphabetic order of first author) of the retrieved publications for selection. Interrater reliability was calculated by κ score, and acceptable reliability was confirmed when κ >0.9. A single author (S.S.S. or A.E.D.) screened the remaining titles and abstracts for selection. Subsequently, 2 authors (A.E.D. and S.S.S.) independently assessed the full texts of eligible studies for further selection (Figure 1), data extraction, and analysis. Two authors (A.E.D. and S.S.S.) independently and systematically analyzed the eligible studies and assessed the level of evidence and risk of bias.
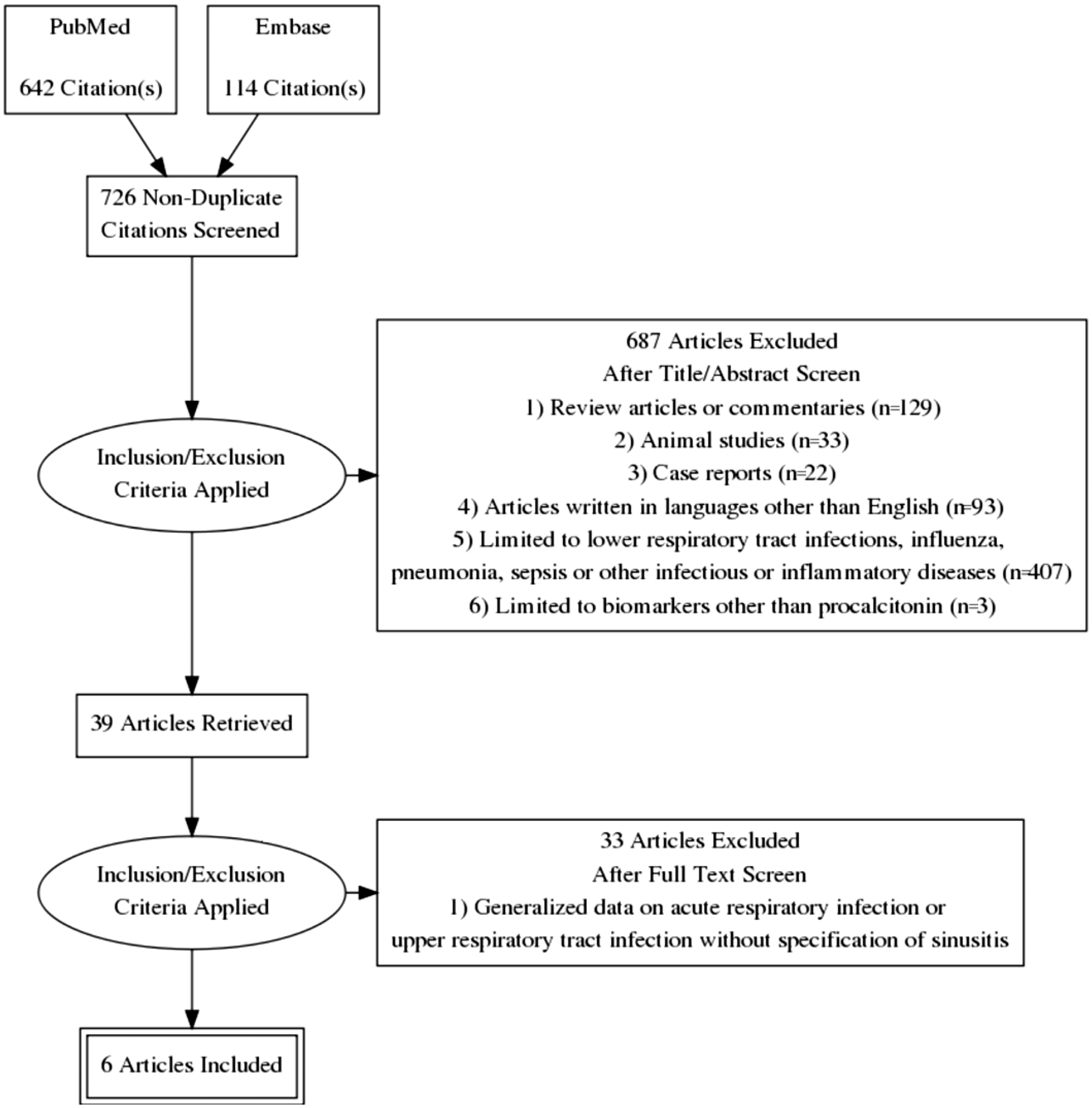
Study selection based on inclusion/exclusion criteria.
Two authors (A.E.D. and S.S.S.) independently assessed the level of evidence to provide an overall estimate of the strength of study design when the study design produced data directly pertaining to our research question. The risk of bias was assessed at the study level and outcome level by examining each study for specific markers of validity. These markers included randomization, concealment of subject allocation, and blinding of subjects or investigators. Disagreement was resolved by discussion.
Results
The search of PubMed and Embase retrieved a total of 726 nonduplicate articles, 6 of which met inclusion criteria and were included in this study (Figure 1). Interrater reliability of the initial screen based on title and abstract was substantial (κ = 0.92 with 95% confidence interval [CI] [0.86–0.98]), and there was 100% agreement on articles for full review following discussion between authors. Two of these studies were conducted as RCT. 28 , 29 Burkhardt et al. included a noninterventional study arm in which PCT levels were measured at time of diagnosis. These data were not included in the analysis, as Burkhardt et al. neither tracked PCT over time nor compared it to other biomarkers.
The location of the studies and patient demographics were carefully examined to avoid duplicated data. One of the prospective noninterventional studies utilized patient groups from RCT. 29 , 30 Given that the aims of these studies were separate from those of the respective RCT from which the patient cohorts were established, the results were analyzed separately.
The percentage of patients reportedly lost to follow-up ranged from 1.12% to 14%, and no studies were excluded based on these figures. All included studies included a sufficiently large patient population and complete data sets and thus were suitable for systematic analysis.
Using the described search strategies, we were unable to identify any studies that specifically assessed the role of PCT levels in chronic rhinosinusitis (CRS). Two studies did not identify a time frame in which the specified symptoms of RS presented; however, given that the other subgroups in these studies included acute tonsillopharyngitis and peritonsillar abscesses, identification of cases of acute upper respiratory infection is likely. As such, analysis could only be completed with regard to ARS at this time.
Risk of Bias in Included Studies
In 3 of the studies,28–30 the diagnosis of acute respiratory illness or sinusitis was not validated by an external source. Although physicians were encouraged to use updated guidelines for diagnostic criteria, it is possible that some of these patients were misclassified, thus creating the potential for selection bias. Three studies31–33 used specified criteria to identify patients with sinusitis (Table 2); however, only Autio et al. included timing of symptom onset in criteria. Whether the other 2 studies distinguished between patients with ARS and CRS is unclear.
Characteristics of Included Studies.
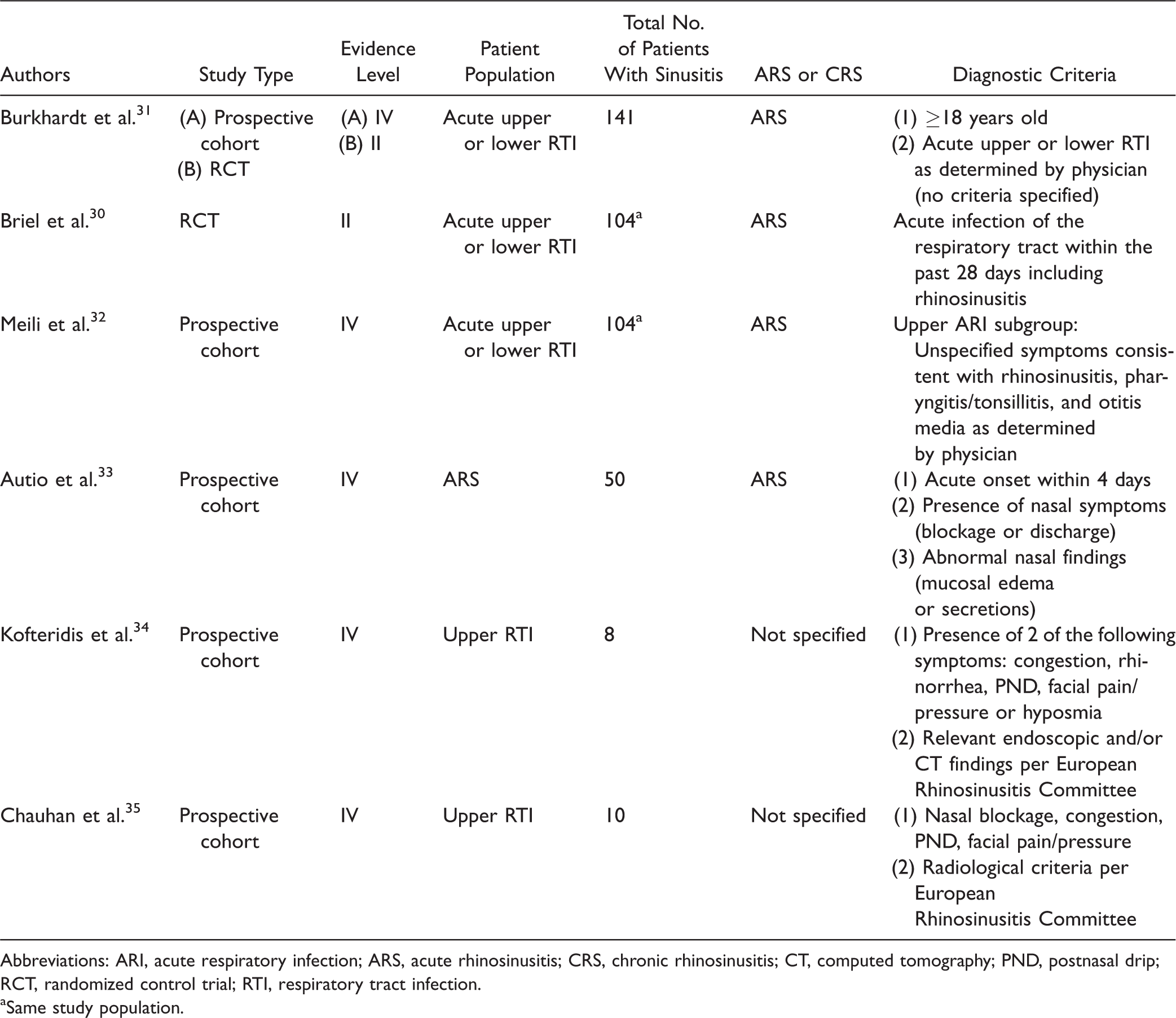
Abbreviations: ARI, acute respiratory infection; ARS, acute rhinosinusitis; CRS, chronic rhinosinusitis; CT, computed tomography; PND, postnasal drip; RCT, randomized control trial; RTI, respiratory tract infection.
aSame study population.
In the RCT that utilized PCT levels as a metric to recommend for or against antibiotic use, the degree to which the participating physicians were blinded from the randomization and PCT level varied. The physicians in the Briel et al. study were informed of the PCT test results for all patients who were randomized to receive PCT-guided therapy. Burkhardt et al., however, faxed a recommendation regarding antibiotic therapy to the prescribing physicians but did not specify randomization status or exact PCT level. In addition, both studies gave physicians the choice to override recommendations, which occurred in 13.1% to 15% of cases for various reasons. In the Burkhardt et al.’s study, patients in this group were analyzed separately in terms of primary and secondary end points to avoid bias due to physician preferences.
For both RCT, outcomes at day 14 and 28 were elicited over the telephone by research personnel blinded to study aims in order to reduce potential for interviewer bias.
Data Extraction
A total of 313 patients with RS were included in these studies. Pooling of data was not possible due to heterogeneity among the studies in terms of diagnostic criteria, stratification of subgroups for data analysis, and outcome measures. Data are summarized in Tables 3 and 4. Data were extracted independently in duplicate. CIs were reported for studies that did not include P values.
Results of Randomized Controlled Trials of PCT-Guided Therapy.
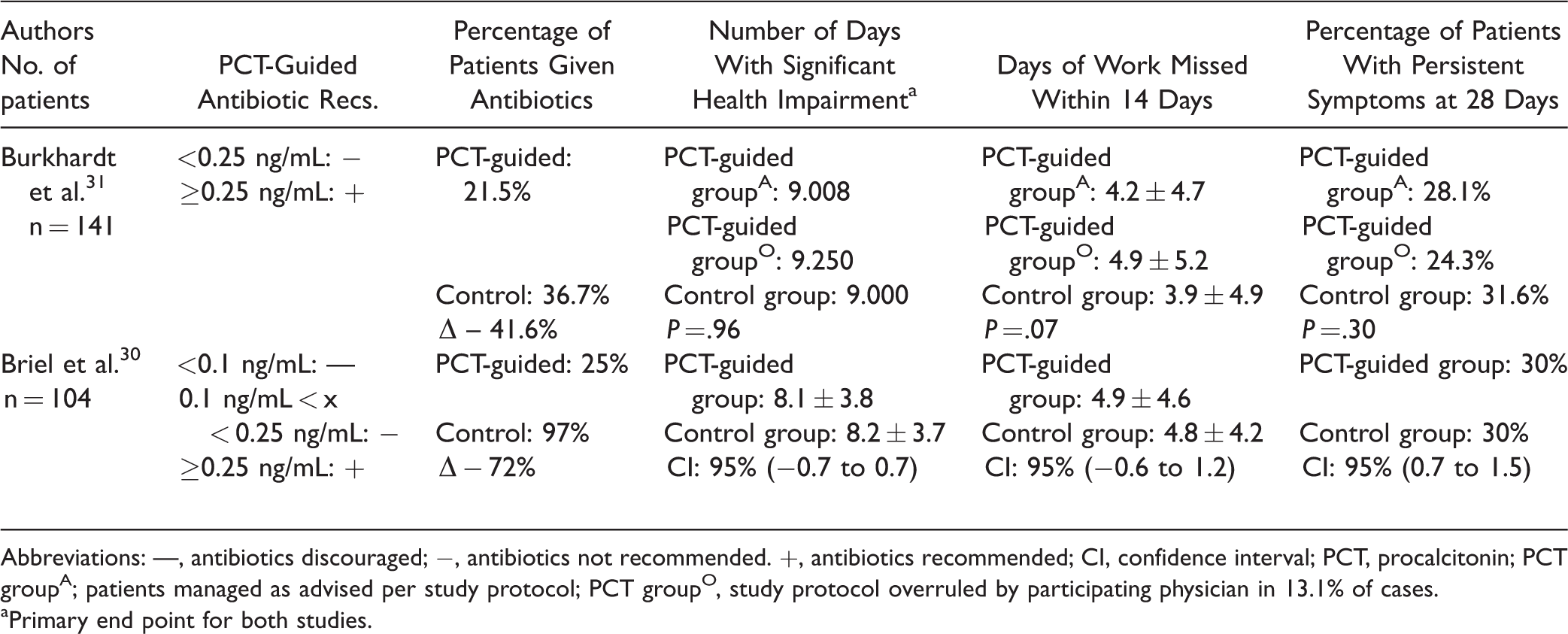
Abbreviations: —, antibiotics discouraged; −, antibiotics not recommended. +, antibiotics recommended; CI, confidence interval; PCT, procalcitonin; PCT groupA; patients managed as advised per study protocol; PCT groupO, study protocol overruled by participating physician in 13.1% of cases.
aPrimary end point for both studies.
Results of Prospective Cohort Studies.
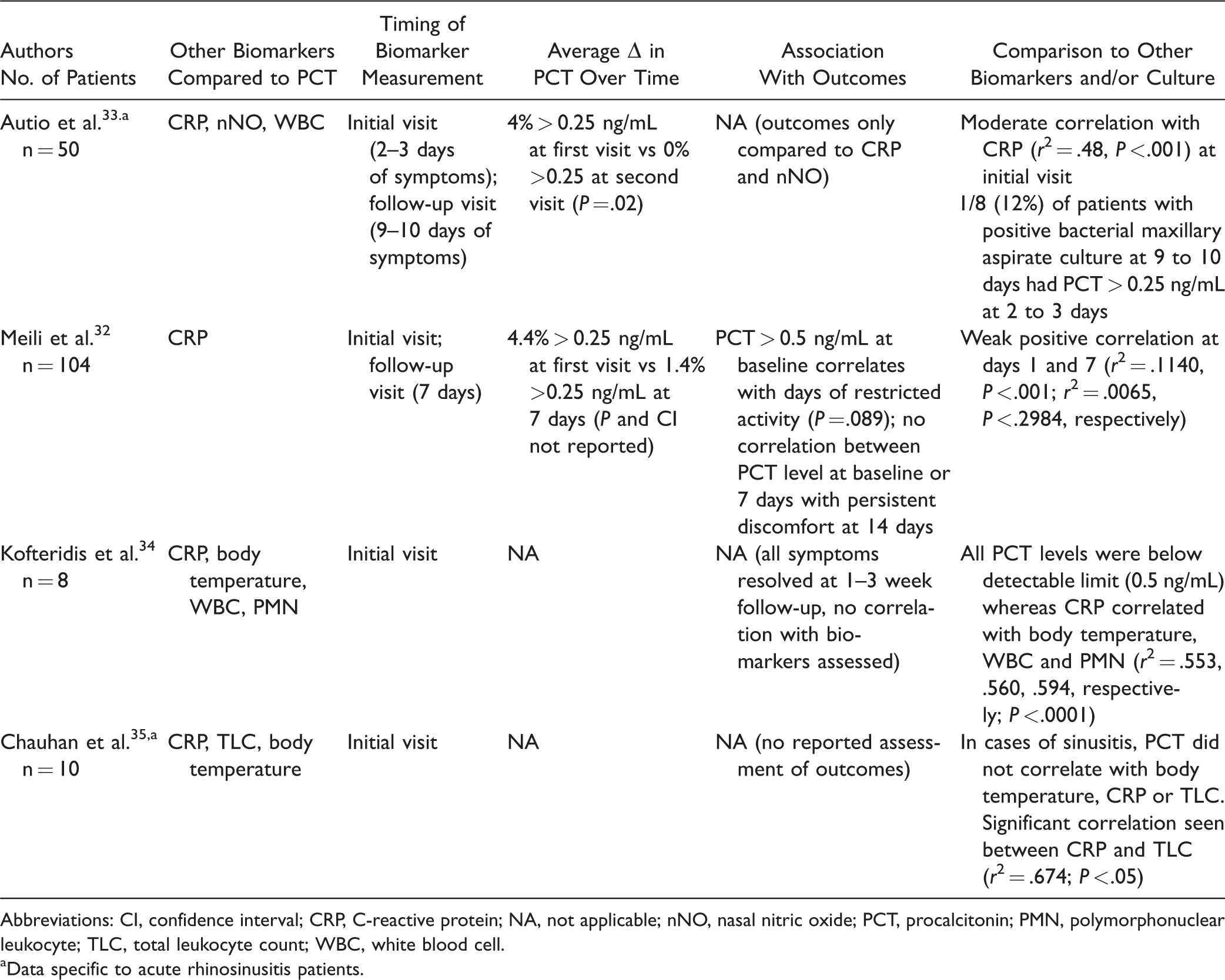
Abbreviations: CI, confidence interval; CRP, C-reactive protein; NA, not applicable; nNO, nasal nitric oxide; PCT, procalcitonin; PMN, polymorphonuclear leukocyte; TLC, total leukocyte count; WBC, white blood cell.
aData specific to acute rhinosinusitis patients.
PCT-Guided Antibiotic Therapy
The 2 RCTs (n = 245) were compared in terms of PCT level-based guidelines, percentage reduction in antibiotic use, number of days with significant health impact, number of days of work missed in 14 days, and percentage of patients with persistent symptoms at 28 days. Both studies recommended antibiotic use in patients with a serum PCT level of greater than 0.25 ng/mL and discouraged antibiotic use when PCT levels were less than 0.25 ng/mL. Briel et al. further subdivided the latter group into PCT < 0.10 ng/mL (antibiotics discouraged) and between 0.10 ng/mL and 0.25 ng/mL (antibiotics not recommended), although it is unclear how this subdivision affected physician adherence to guidelines and antibiotic prescription rate. A significant reduction in antibiotic prescription was found in the PCT-guided group as compared to the control group, ranging from 41.6% to 71%. 28 , 29
Both studies measured days with restricted activity secondary to infection as a primary end point. Briel et al. study analyzed this end point by subtype of RTI, with ARS included in the “upper RTI (URTI) or influenza (excluding tonsillitis or pharyngitis)” group, whereas Burkhardt et al. did not perform subgroup analysis. No significant difference was found between the control group and the PCT-guided group (9.0 vs 9.0 days; 8.2 ± 3.7 vs 8.1 ± 3.8 days, respectively). Similarly, no significant difference was found in the secondary end points of days of work missed within a 14-day period and percentage of patients with persistent symptoms at 28 days (Table 3). As such, both studies concluded that the use of a PCT-based guideline for antibiotic prescription is noninferior to current protocols for antibiotic use in the management of acute RTIs, including ARS.
PCT Compared to Other Biomarkers and Sinus Cultures
Four studies were identified that compared PCT to other biomarkers in patients with URTI with specific inclusion of patients with ARS. The correlation between PCT and C-reactive protein (CRP) in these studies was inconsistent and weak to moderate at best. Two of these studies measured PCT at 2 separate time points and found an overall downtrend in PCT level between 7 and 10 days after the initial visit, although this information is limited in that it was presented generally and not as a paired analysis. 30 , 31 Only Meili et al. assessed the relationship between baseline and 7-day PCT levels and clinical outcomes. This study found that PCT > 0.5 ng/mL at baseline correlated with number of days of restricted activity (P = .089) but not with persistent discomfort at 14 days.
Of the 4 studies, only 1 examined the correlation between PCT levels and positive maxillary sinus aspirate cultures. Autio et al. found that only 1 of the 8 patients with positive bacterial cultures 9 to 10 days after initial presentation had an elevated PCT level (>0.25 ng/mL) at the initial visit. 31
Discussion
Antibiotic overuse in the outpatient setting has contributed significantly to the increasing development of drug-resistant bacteria over the last several decades. 34 , 35 It is estimated that in the United States, 2.5 million patients develop a drug-resistant bacterial infection every year leading to approximately 23 000 deaths. 34 Management of drug-resistant bacterial infections represents a significant source of health-care expenditure due to prolonged hospital stays, increased medical costs, and loss of productivity. In 2008, 1 single-institution cohort study reported a societal cost of $10.7 to $15 million for that hospital alone. 36 In response to this public health issue, the White House released The National Action Plan for Combating Antibiotic-Resistant Bacteria in 2015 with a goal of reducing inappropriate antibiotic use by 50% in outpatient settings and 20% in inpatient settings by 2020. 37
Subsequent to the development of a national agenda to address the increasing medical and societal burden of drug-resistant infections, the Agency for Healthcare Research and Quality (AHRQ) conducted a large systematic review in 2016 focused specifically on antibiotic use in uncomplicated acute RTIs with the intention of providing guidelines for quality improvement in antibiotic prescription. 38 Acute RTIs including bronchitis, otitis media, pharyngitis, tonsillitis, and RS account for a significant number of primary care and emergency room visits annually. Although the majority of acute URTI cases are viral and self-limited, studies have shown that 60% to 73% of patients are prescribed antibiotics. 39 , 40 As such, analyses of the National Ambulatory and National Hospital Ambulatory Medical Care Surveys from 2007 to 2009 have shown that antibiotics are prescribed at approximately 101 million adult ambulatory visits annually. 41
In cases of uncomplicated ARS, antibiotics are prescribed to the majority of patients seen in outpatient settings despite standardized treatment guidelines that aim to reduce unnecessary antibiotic use. This is seen in both primary care and emergency department settings, where rates of antibiotic prescription for children and adults with ARS range from 51.4 to >80%. 16 , 42 A large retrospective chart review at Kaiser Permanente Southern California found that of 152 774 patients with uncomplicated ARS who presented to primary care, urgent care, or the emergency department, 89.2% were prescribed antibiotics at their initial encounter. Furthermore, detailed chart review of 300 randomly selected patients revealed that antibiotics were prescribed according to existing guidelines in only 29% of cases. 43 This suggests that current guidelines based on symptoms, physical exam, nasal endoscopy, and imaging are not sufficient to combat the systemic public health issue of antibiotic overuse in this population. Because differentiation of mild viral infection from bacterial infection is challenging, clinicians often start empiric antibiotic treatment, which increases resistance of common bacteria and causes drug-related side effects. 44
As such, a range of techniques has been studied with the aim of reducing inappropriate antibiotic use, including physician education and communication training, 45 public campaigns, 46 mathematical modeling of symptomatology, 47 and clinical scoring guidelines. 48 Barham et al demonstrated that even in patient with a steadfast belief that their recurrent acute symptoms are “sinus” in origin, computed tomography scans are often normal. 49 Because differentiation of mild viral sinusitis from bacterial ARS is challenging, clinicians often start empiric antibiotic treatment. This in turn leads to increased drug-resistance and drug-related side effects. 44 , 50
More recently, biomarkers has been investigated as a tool for identification of patient subgroups that would benefit from antibiotics. Although very few of these studies address ARS, these protocols have the potential to be applied to any infectious process in which it is difficult to differentiate self-limited viral infections and bacterial infections requiring antibiotic treatment.
CRP has been studied as a serum biomarker for bacterial infection in a wide variety of conditions, including acute RTIs such as ARS. The AHRQ systematic review found that CRP point-of-care testing was associated with an overall reduction in antibiotics prescription in 7 RCTs, although the absolute reduction ranged widely. In addition, some studies demonstrated an increased rate of reconsultation within 4 weeks; and while some studies reported no impact on rates of hospitalization (n = 5), 2 reported higher frequency of hospitalization in the CRP groups. 38 Whether these adverse events were seen in patients with ARS or in a different subgroup of RTI is unclear; however, these results should be taken into consideration when establishing a new diagnostic and treatment algorithm for ARS. Furthermore, data suggest that CRP may have limitations in guiding antibiotic therapy given its latent peak in levels and lower sensitivity and specificity compared to PCT in patients with a variety of bacterial infections and/or sepsis. 51
Our systematic review demonstrates that PCT does not reliably correlate with CRP levels in URTI. A possible explanation is the aforementioned difference in kinetics of CRP and PCT. PCT typically peaks within 8 hours of stimulation, 52 whereas CRP peaks at 36 hours. 53 High PCT levels (>0.50 ng/mL) do, however, correlate with number of days of restricted activity. 30 This suggests there may be a role for PCT in identifying cases of ARS that are not self-limited and would thus benefit from antibiotic treatment.
Although only 2 RCT on PCT-guided management of acute RTI have specifically included patients with ARS, both showed noninferiority in PCT-guided treatment groups at both primary and secondary end points, including number of days with restricted activity due to illness, number of days missed from work, and percentage of patients with persistent symptoms at 28 days. The use of PCT-based guidelines in these studies reduced antibiotic use by 41.6% to 71% 28 , 29 without a change in rate of serious adverse events, namely, hospitalization or death. In addition, Briel et al. also demonstrated that the PCT-guided group experienced a significant reduction in mean number of days with adverse effects from medication including abdominal pain, diarrhea, nausea, vomiting, and/or skin rash (2.3 days vs 3.6 days, adjusted decrease of 1.1 days in PCT group [95% CI, 0.1–2.1 days]). These findings are corroborated by the AHRQ study, which found that PCT-based algorithms significantly reduce antibiotic prescribing in adults with URTI without affecting mortality or treatment failure at 30 days. 38 This suggests that PCT-based guidelines for medical management of ARS are a safe and effective strategy for reducing antibiotic overuse.
Given the relatively small number of studies that have investigated the role of PCT in diagnosing and treating RS, this review has several limitations. Three of the 6 studies analyzed included patients with ARS as diagnosed by participating physicians but did not include specific diagnostic criteria. Furthermore, the subgroup analyses in these studies did not stratify data specifically with regard to sinusitis. Data were either generally reported without regard to diagnostic subgroup 29 or subgroup analysis was performed only at the level of upper respiratory tract versus lower RTIs. 28 , 30 In addition, the inclusion criteria for 4 of the 5 studies25–28 did not include a defined time period of symptoms. Thus, selection bias may be present in that some of the patients included in these studies could meet criteria for CRS as opposed to ARS. The majority of the patients in the trials of PCT-guided antibiotics had resolution of symptoms at 28 days (Table 3). This is inconsistent with a diagnosis of CRS, and thus it can be deduced that the majority of these patients were suffering from acute infections; however, there is no long-term follow-up data available to assess for recurrence or persistence of symptoms at 3 months.
Two of the studies comparing CRP and PCT 32 , 33 included relatively few patients with ARS. This may be why a significant association between CRP and PCT was not appreciated in these studies. Of note, Kofteridis et al. utilized a cutoff of 0.50 ng/mL as a normal value for PCT (as opposed to 0.25 ng/mL in several other studies 28 , 29 ) and did not further analyze the results associated with PCT given that all measurements fell below this value. In addition, the time point in the course of the infection at which serum biomarkers were measured (ie, number of days with symptoms) was not specified in either of these studies. Given that PCT and CRP peak at different points during bacterial infections, measurements that occurred after several days of symptom onset may not capture PCT at its peak. Despite these limitations, the existing literature suggests that there may be a role for PCT in management of ARS, particularly in developing new criteria to reduce antibiotic overuse.
Conclusion
Literature on PCT as a serum biomarker for diagnosis and appropriate antibiotic treatment of ARS is limited, and no studies have addressed the role of PCT in management of CRS. Existing data on PCT-guided antibiotic treatment of acute RTIs, including ARS, have shown noninferior outcomes despite decreased antibiotic use. PCT does not consistently correlate with CRP; however, CRP is not currently used as a biomarker for ARS, thus this lack of correlation does not negate the role for PCT in management of ARS. There is a need for further research, such as a large-scale RCT, to investigate the potential utility of PCT-guided management of ARS.
Footnotes
Authors’ Note
This study was presented at the American Academy of Otolaryngology—Head and Neck Surgery National Meeting, September 10, 2017, in Chicago, IL, USA.
Acknowledgments
The authors would like to thank Amy Yang M.S. of the Northwestern University Biostatistics Collaboration Center for her assistance with statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Northwestern University-Patient-centered Intervention and Engagement Training K12 Faculty Scholars Training Program, Grant Number K12HS023011 from the Agency for Healthcare Research and Quality, the National Institutes of Health’s Chronic Rhinosinusitis Integrative Studies Program, Grant Number U19 AI106683, and the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number UL1TR001422. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality or the National Institutes of Health.