
Abstract
Introduction
Autologous conditioned plasma (ACP) is a single-spin, leukocyte-poor platelet-rich plasma (PRP) that provides a plasma with a platelet concentration 2 to 3 times the blood platelet concentration. The objective of this study was to investigate the clinical effectiveness of ACP intra-articular injection in patients with knee osteoarthritis (OA) and to identify any demographic, disease-associated, or biological predictors of outcome.
Methods
A prospective cohort study was conducted between 2022 and 2023 in a single high-volume tertiary center, including 42 patients (54 knees) who consented to be enrolled. Patients underwent a series of 3 injections of ACP at weekly intervals, prepared using the Arthrex ACP Double-Syringe System. Lysholm scores were collected at baseline, 3-months, and 6-months post-injection.
Results
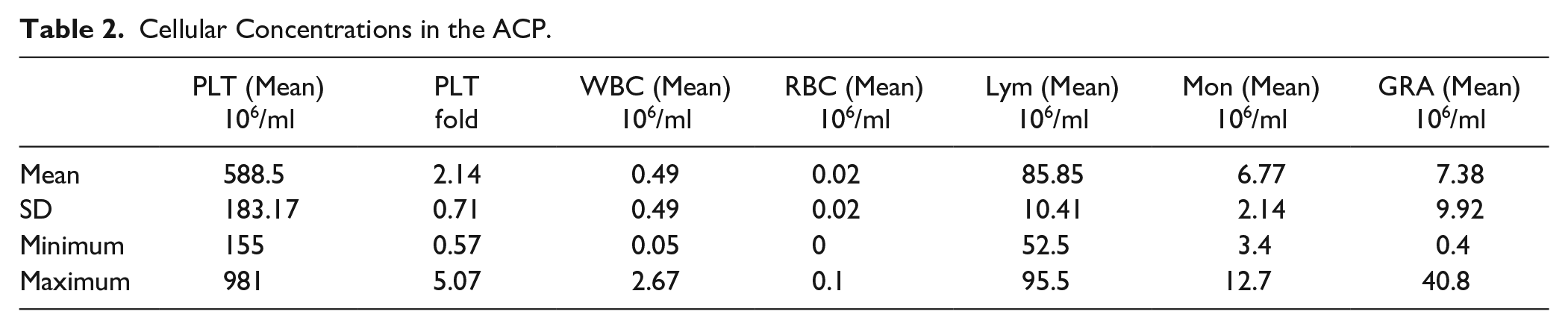
Forty patients (49 knees) completed the follow-up and were included in the final analysis. The mean age was 53.8 ± 10.16 years (range 35-76 years), and the median body mass index (BMI) was 29 (interquartile range [IQR]: 27-34). There were 22 females and 18 males. Treatment failure occurred in 12 out of 49 cases (24.49%). The mean platelet concentration in the ACP was 588.5 ± 183.2 × 106/ml, with a mean platelet fold increase of 2.14 ± 0.71 compared to the baseline. Multi-linear regression modeling showed that older age and higher mean platelet concentration were predictors of higher post-injection Lysholm scores, with beta coefficients of 0.34 and 0.28, respectively, and p values of 0.013 and 0.036, respectively.
Conclusion
Autologous conditioned plasma provided clinical benefits in this cohort study of knee OA patients for at least 6 months post-injection. Older age and a higher mean platelet concentration in the ACP were identified as predictors of a higher Lysholm score.
Keywords
Introduction
The National Institute for Health and Care Excellence (NICE) guidelines for the non-surgical treatment of knee osteoarthritis (OA) include therapeutic exercises, weight management, and corticosteroid intra-articular injections. 1 The use of platelet-rich plasma (PRP) or its derivatives for knee intra-articular injections in the UK is permitted only within the context of research trials. 1 This aligns with the guidelines of the American Academy of Orthopedic Surgeons (AAOS). 2
Platelet-rich plasma contains a high concentration of platelets, which release growth factors and cytokines from α granules upon activation, such as platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and transforming growth factor-β (TGF-β). 3 Cytokines and growth factors released from platelets have beneficial effects on wound healing, cell migration, proliferation, differentiation, and extracellular matrix synthesis. 4 Besides platelets, other cell types such as leukocytes and red blood cells may be found in PRP. 3 PRP preparation methods vary by manufacturer, leading to differences in cellular compositions between products; for example, PRP may be leukocyte-rich or leukocyte-poor. 5 Recent research proposed that the main effect of PRP is to slow down tissue degeneration and reduce inflammation in the joint environment; however, the mechanisms of PRP efficacy still remain unclear. 6 Early generations of PRP had controversial clinical benefits.5,7 This was partly attributed to their high leukocyte content, which was found to release pro-inflammatory cytokines that activate the nuclear factor (NF)-κB pathway, ultimately inhibiting tissue healing. 8 The current trend in PRP preparations is to favor leukocyte-poor preparations. However, no strong clinical evidence exists to support this.9,10
Autologous conditioned plasma (ACP) has emerged as a potential advancement of PRP, aimed at improving clinical outcomes. It is a single-spin, leukocyte-poor PRP (LP-PRP).5,11 The advantages proposed include a quicker procedural time for its preparation, more efficient concentration of platelets, and safer handling, allowing for easy application and use in the clinical setting. 11 The platelet concentration in the single-spin ACP is estimated to be 2 to 3 times the blood platelet concentration.5,11 Few studies have examined the effect of ACP, with outcomes ranging from excellent to poor.12-16 The variance in results could be due to a lack of in-depth investigation into patient demographics, disease characteristics, and biological characterisation of the injected ACP product.
The objective of this preliminary prospective study was to investigate the clinical effectiveness of ACP intra-articular injection in patients with OA and to identify any demographic, disease-associated, or biological predictors of outcome.
Methods
A prospective cohort study was conducted between 2022 and 2023 in a single high-volume tertiary center, including 42 patients (54 knees) who consented to be enrolled. Inclusion criteria were adult patients >18 years old with knee pain attributed to OA and mild to moderate osteoarthritis (Kellgren-Lawrence grade I to III). Patients with severe OA (Kellgren-Lawrence grade IV), rheumatoid arthritis, and inflammatory arthropathies were excluded.
Ethical approval was obtained for this study with a reference number 11/NW/0875. The trial was explained to patients during their routine clinic appointment if deemed eligible. Patients were invited to participate in the trial by the surgeon, and if they agreed, a member of the research team discussed the trial in detail, including the collection of biological samples for analysis. Patients were provided with information leaflets to take home to consider their participation. Those who agreed were scheduled for 3 appointments at weekly intervals for the ACP injections.
Patients underwent a series of 3 ACP injections at weekly intervals, prepared using the Arthrex ACP Double-Syringe System (Arthrex, Naples, USA) following the manufacturer’s instructions. 11 Briefly, 15 ml of autologous blood was drawn into the system and centrifuged for 5 minutes at 300 g. A volume of 4 to 7 ml of ACP was obtained in the top layer of the preparation syringe and injected into patients. Figure 1 illustrates the sequence of events in forming the ACP. During the same session, just before the ACP injection, the knee joint was aspirated. A needle was inserted into the intra-articular space through the superolateral aspect of the knee joint with the knee extended, while the patient lay supine on the couch. The plunger was drawn back to aspirate synovial fluid until the knee was dry. Subsequently, the ACP syringe was attached to the same needle, and the ACP was injected into the knee. In parallel, 4 ml of baseline blood was collected from each patient in EDTA blood tubes. Baseline blood and ACP were both sent for hematological analysis. The concentrations of white blood cells (WBC), red blood cells (RBC), and platelets, as well as the proportions of lymphocytes, granulocytes, and monocytes, were assessed via a hematology analyzer (ABX Micros ES 60; Horiba UK Ltd, Northampton, UK). Mean WBC, RBC, and platelet concentrations for each patient were calculated by averaging values obtained from all the injections.
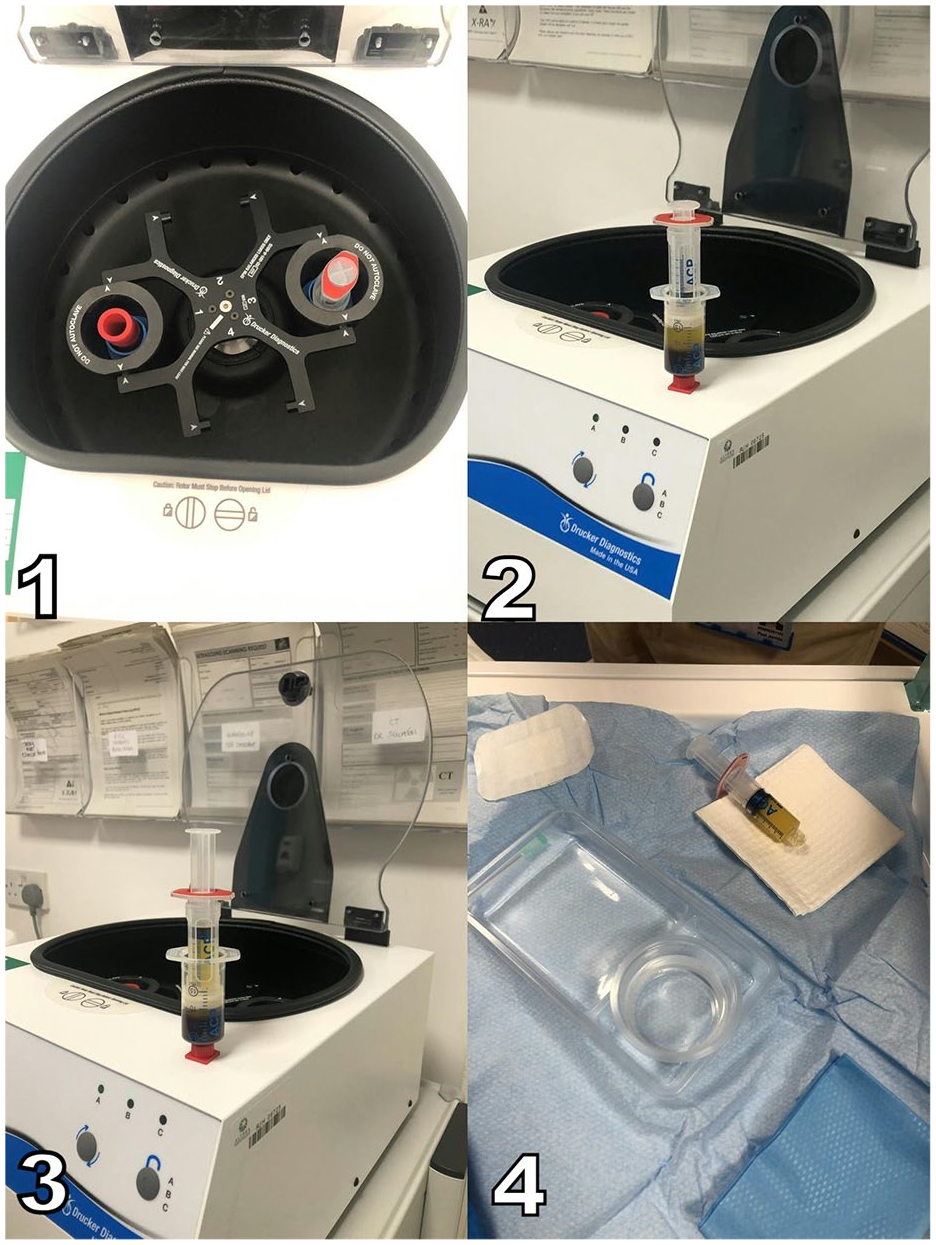
Demonstration of the sequence of events in forming ACP: (1) placing the syringe containing the patient’s blood in the centrifuge, (2) the centrifuged sample, (3) extracting the ACP from the sample, and (4) the final ACP sample.
Demographics, including age, sex, body mass index (BMI), and smoking status, were collected. The pattern of OA was classified as tri-compartmental, uni-compartmental (medial or lateral), or patellofemoral (PFJ). Data on previous knee surgery, history of old fracture around the knee, and Kellgren-Lawrence (KL) classification before injection were also collected.
Treatment failure was defined as a failure of improvement in the 3 or 6-month Lysholm Score below the MCID point. 17 An event was defined as requiring knee surgery within a year attributed to the same condition. Event time was calculated from the moment the decision was made to put the patient on the waiting list, not the actual surgical time, to mitigate any bias related to variability in waiting list times. Lysholm scores as patient-reported outcome measures (PROMs) were collected at baseline, 3 months, and 6 months post-injection. Follow-up for requiring ipsilateral knee surgery attributed to the same condition was conducted up to 1-year post-injection.
The Lysholm score consists of 8 factors: limp, support, locking, instability, pain, swelling, stair climbing, and squatting, each scored individually. 18 The total score ranges from 0 to 100, with higher scores indicating better knee function and fewer symptoms. 18 It was chosen for this study as the primary outcome measure because it effectively assesses knee function, relevant to patients with mild to moderate arthritis included in this study. Unlike Knee Injury and Osteoarthritis Outcome Score (KOOS) or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), which are broader and often used in populations with advanced arthritis or older demographics, the Lysholm score provides a straightforward and targeted assessment of the knee functional outcome. In addition, the mean age of the patients in this study (53.8 ± 10.16 years) represents a relatively younger and active cohort, making the Lysholm score particularly appropriate as it emphasizes mobility and function rather than the broader quality-of-life aspects captured by KOOS or WOMAC.
Statistical Analysis
SPSS was used for statistical analysis (IBM Corp. Released 2023. IBM SPSS Statistics for Macintosh, Version 29.0.2.0. Armonk, NY: IBM Corp). Continuous data are summarized as mean ± Standard Deviation (SD) if normally distributed and median ± interquartile range (IQR) when not normally distributed. Data were tested for normality using frequency histograms, Quantile-Quantile (Q-Q) plots and the Shapiro-Wilk test. Categorical data are summarized as rate and frequency.
A mixed linear model was used to compare Lysholm scores at baseline with those at 3 and 6 months. The model was fitted using the restricted maximum likelihood (REML) estimation method, and t-tests were conducted using Satterthwaite’s method.
A multilinear regression model was utilized to examine the effect of age, KL stage, pattern of arthritis, and mean platelet concentration in the ACP on the 3-month Lysholm scores. Due to sample size limitations, other potential predictors could not be included in the model. Kaplan-Meier survival analysis was performed to assess the survival probability of ACP at different time points until the end of the follow-up at 12 months. A logistic regression model was used to evaluate the effect of age, KL stage, pattern of arthritis, and mean platelet concentration in the ACP on treatment failure. Pearson correlation analysis was conducted to examine the effect of the different cell types on the Lysholm score at 3 months.
Results
Forty patients (49 knees) completed the follow-up and were included in the final analysis. The mean age was 53.8 ± 10.16 years, and the median BMI was 29 (IQR 27-34). There were 22 females and 18 males. Table 1 summarizes the patient demographics and baseline characteristics. Treatment failure occurred in 12 out of 49 cases (24.49%), and 7 out of 49 cases (14.29%) experienced an event, defined as requiring knee surgery within a year. All patients who had an event were also in the treatment failure group.
Patient Demographics and Baseline Characteristics.

Data are presented as mean (SD) for continuous variables and frequency (rate) for categorical variables.
BMI; body mass index, OA; osteoarthritis.
The mean platelet concentration in the ACP was 588.5 ± 183.2 × 106/ml, with a mean platelet fold increase of 2.1 ± 0.7. Table 2 shows the different cellular concentrations in the ACP. The mean Lysholm scores at baseline, 3 months, and 6 months were 46.04 ± 19.21, 68.43 ± 22.63, and 67.7 ± 21.45, respectively ( Fig. 2 ). The mixed linear model showed a significant difference between Lysholm scores at baseline, 3 months, and 6 months (p < 0.001). Post-hoc analysis revealed a statistically significant improvement in Lysholm between baseline scores and those recorded at 3 months and 6 months (p < 0.001 for both). The estimated differences between Lysholm scores at 3 months and 6 months compared to baseline were 22.07 and 19.07, respectively, surpassing the reported minimally clinically important difference (MCID) of the Lysholm scores. However, there was no significant difference between Lysholm scores at 3 months and 6 months (p = 0.7) ( Table 3 ).
Cellular Concentrations in the ACP.
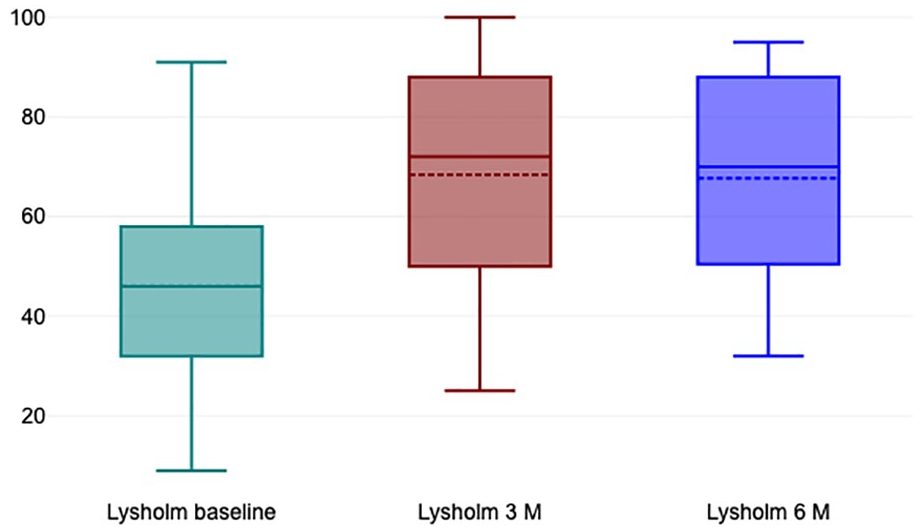
Box plots comparing Lysholm scores at different time points.
Results of a Mixed Linear Model Comparing Lysholm Scores at Different Time Points.

Nine patients received bilateral knee injections, with a mean age of 53 ± 9 years; 5 were female and 4 males. One patient experienced treatment failure in both knees, which both had tri-compartmental OA; however, an event occurred in only one knee. Another patient had treatment failure and an event in one knee with PFJ arthritis, while the other knee, with tri-compartmental OA, responded to treatment. The remaining 7 patients did not experience treatment failure or event in either knee.
Pearson correlation analysis showed a significant correlation between mean platelet count and Lysholm scores at 3 months (p = 0.014, r = 0.32). There was no significant correlation between Lysholm scores at 3 months and red blood cells (RBCs), white blood cells (WBCs), lymphocytes, granulocytes, or monocytes, with p values of 0.90, 0.78, 0.95, 0.94, and 0.55, respectively.
The Multiple Linear Regression (MLR) model included 3 months Lysholm scores as the dependent variable and age at injection, K-L classification, previous knee operation, and mean Platelet (PLT) concentration as independent variables. The model was statistically significant in predicting the post-injection Lysholm score (F = 4.88, p = 0.002, R² = 0.32) (
Table 4
). Age and mean platelet concentration had the highest beta coefficients, 0.34 and 0.28, respectively, with p values of 0.013 and 0.036, respectively. This indicated that older age in our cohort and higher mean PLT concentration were associated with higher Lysholm scores (
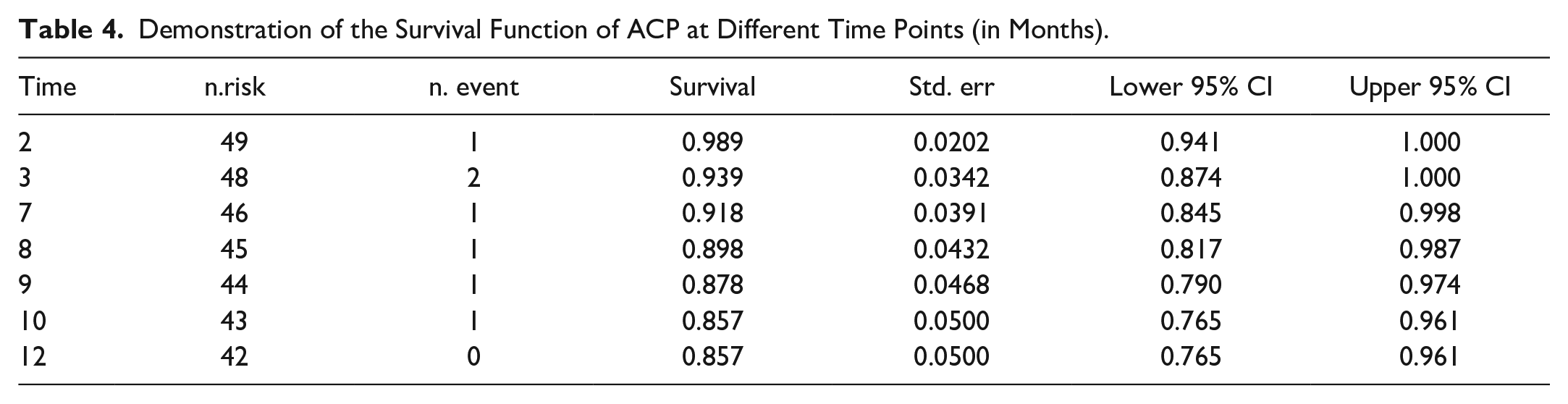
Demonstration of the Survival Function of ACP at Different Time Points (in Months).
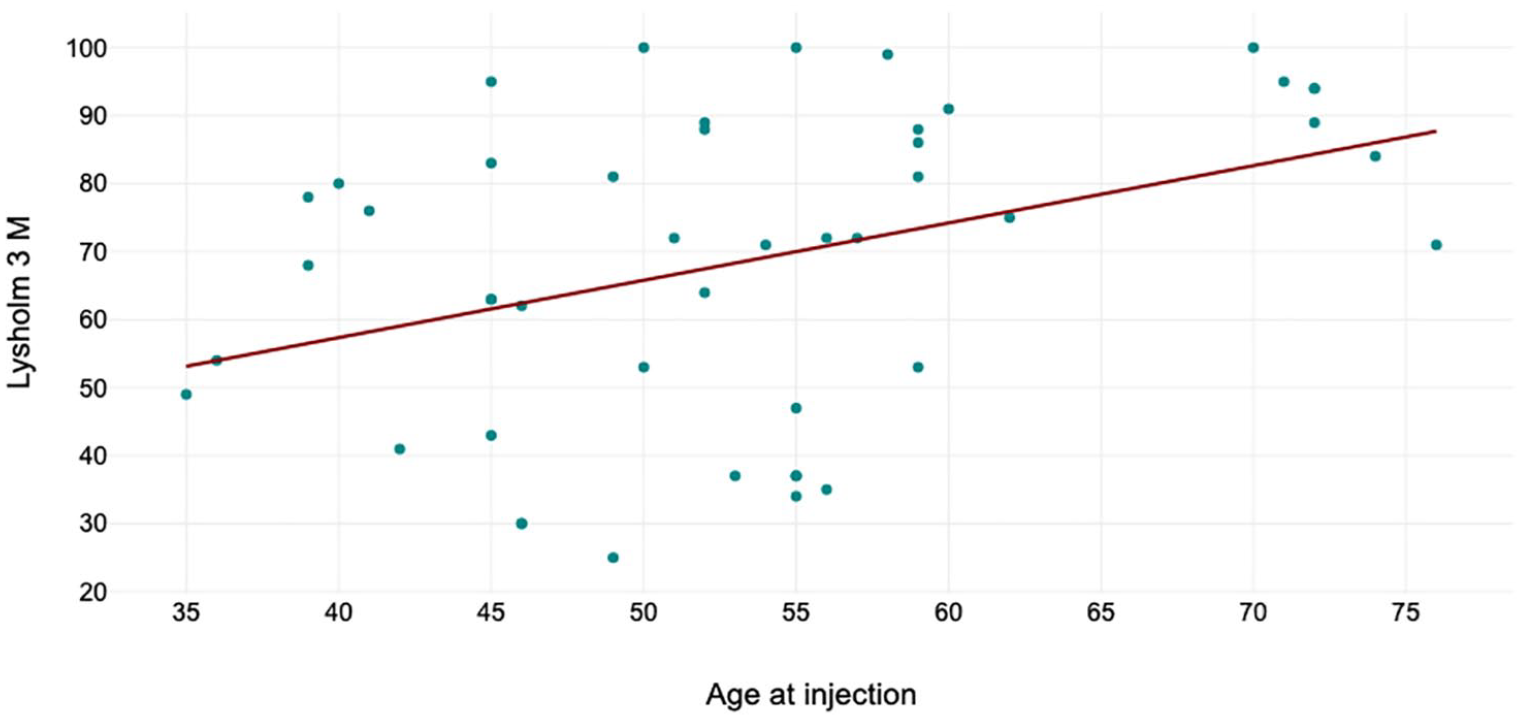
Scatter plot demonstrating relation between age and Lysholm scores at 3 months.
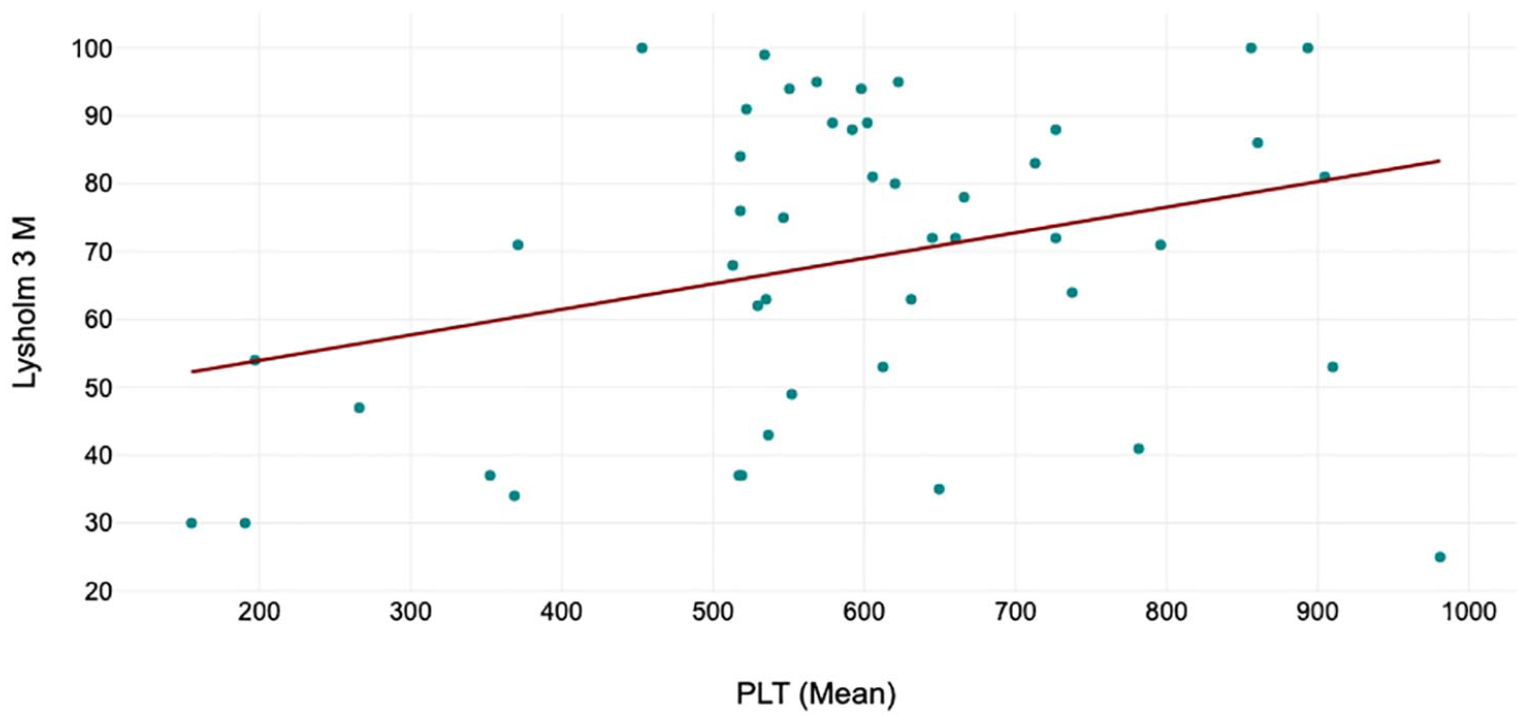
Scatter plot demonstrating the relation between platelet concentration in the ACP and Lysholm scores at 3 months.
The logistic regression model included age, K-L classification, previous knee operation, and mean PLT concentration as independent variables, and treatment failure as the dependent variable. The regression model was not statistically significant in predicting treatment failure (p = 0.106, Cox & Snell R² = 0.14). None of the independent variables were significant in predicting treatment failure. Kaplan-Meier survival analysis of ACP showed a survival probability of 91.8% (95% CI 84.5%-99%) at 7 months and 85.7% (95% CI 76.5%-96.1%) at 12 months ( Table 4 ).
Sensitivity Analysis
The sensitivity analysis evaluated the robustness of the results by excluding certain subgroups, including patients with bilateral cases, patients with KL stage 3, and those with a high BMI (≥35). Mixed linear models showed a significant improvement in Lysholm scores from baseline to 3 months and baseline to 6 months, regardless of subgroup exclusions, with p-values consistently <0.001. However, no significant differences were observed between the 3-month and 6-month scores (p > 0.05), consistent with the results for the whole group. Linear regression models showed that age at injection and mean platelet concentration in the ACP consistently had a significant impact on outcomes, with p-values ranging from 0.013 to 0.029 for age and from 0.023 to 0.035 for mean platelet concentration. Logistic regression demonstrated moderate predictive accuracy for treatment failure (74%-79%) across all subgroups, with none of the independent variables significantly predicting treatment failure.
Subgroup Analysis
Subgroup analysis revealed that patients aged ≤50 (n = 19) showed less improvement in Lysholm scores at 3 and 6 months, with differences not reaching statistical significance (p = 0.097 and p = 0.362, respectively). Logistic regression demonstrated moderate classification accuracy (78.95%), with K-L Grade 3 significantly increasing the odds of treatment failure (odds ratio [OR] = 25.1, p = 0.03), while linear regression identified no significant predictors for Lysholm score improvement. In contrast, patients aged >50 (n = 30) exhibited more substantial improvements in Lysholm scores at 3 and 6 months (p < 0.001), surpassing those observed in the whole group. Logistic regression accuracy for predicting treatment failure was high (86.67%), though no significant predictors were identified; however, linear regression revealed age (p = 0.004) and PLT (p = 0.006) as significant predictors. Among patients without prior knee operations or fractures (n = 25), the greatest improvements in Lysholm at 3 and 6 months (p < 0.001) were observed compared to both the whole group and other subgroups. Logistic regression accuracy for predicting treatment failure was 84%, with linear regression again identifying age (p = 0.013) and PLT (p = 0.025) as significant predictors.
Discussion
Autologous conditioned plasma provided clinical benefits in this small prospective cohort of knee OA patients for at least 6 months post-injection. Older age and higher mean platelet concentration in the ACP were identified as significant predictors of a higher Lysholm score. This is the first study evaluating ACP intra-articular injection in patients with knee OA in the United Kingdom, and the first to comprehensively associate the biological characteristics of the ACP product with outcome.
Overall, the observed improvement in Lysholm scores up to 6 months post-injection highlights ACP’s potential as an effective treatment for patients with mild-to-moderate OA. This could serve as a viable alternative to other conventional treatments, such as hyaluronic acid or corticosteroid injections, given its proven safety, absence of complications, and lower failure rates. The ease of use and quick procedural time in the clinic setting further enhances its appeal for the knee surgeons and acceptance by the patients. Stratified analyses suggest that ACP may be particularly beneficial for certain age groups and those without prior knee surgery which underlies the importance of patient selection. In addition, identifying predictors of treatment failure, such as higher K-L grades, particularly in younger patients, can help refine patient selection criteria. These findings support the potential integration of ACP into clinical practice, either as a primary treatment option or as a bridging therapy for patients on the waiting list for knee replacement. This integration should be guided by well-designed, multicentre trials evaluating ACP’s long-term efficacy, safety, and cost-effectiveness.
Previous studies have reported contradictory outcomes on ACP used for the treatment of knee OA; 7 however, the variability in the number of ACP injections, methods of preparation, primary outcome measures, and follow-up durations may have contributed to these observed differences.
In this study, an increased platelet concentration in the ACP was associated with improved outcomes, consistent with other studies investigating other PRP products and the findings of a recent systematic review by Berrigan et al.19,20 The mean platelet concentration in the injected ACP was 2.14 times the baseline per injection. A platelet concentration in the PRP 5 to 7 times the baseline has been found to promote cell proliferation, bone marrow derived mesenchymal stromal cell (MSC) recruitment, and wound healing.20,21 This paves the way for developing ACP formulations with higher platelet concentrations, which could provide greater clinical benefits with fewer injections. Interestingly, Arthrex Inc. has designed a new Arthrex Max™ PRP system, which is proposed to provide platelet concentrations in the ACP 7 times the baseline with a single injection. 22
The finding that higher platelet concentrations are associated with better outcomes also highlights the importance of standardizing preparation techniques to ensure consistency in clinical practice. This is supported by the biological evaluation of the ACP samples in our study; however, it is important to note that ACP sample evaluation was not consistently performed across all studies assessing ACP outcomes. In addition, as highlighted, patient demographics and clinical characteristics, such as the severity of arthritis, history of previous knee surgery, soft tissue injury, or fracture, may interact together or individually influence the therapeutic response to ACP injections. Variability in these factors across studies could account for some of the observed differences in outcomes. Future research should aim to investigate how these variables interact with platelet concentration by conducting a well-powered subgroup analysis to provide a more comprehensive understanding of the factors that contribute to the success of ACP therapy.
It is important to note that among orthobiologics, PRP consistently provides the best clinical outcomes for mild to moderate knee OA compared to other injectables. Belk et al. 23 demonstrated that PRP treatment improves clinical outcomes compared to HA, with some evidence suggesting LP-PRP may be superior to LR-PRP. Similarly, Qiao et al. 24 found that PRP, both alone and combined with HA, was more effective than HA, placebo, or corticosteroids in improving function and alleviating pain over follow-up periods of up to 12 months. Pelluri et al. 25 reinforced these findings, reporting that PRP outperformed placebo and corticosteroids in reducing pain and enhancing function, with LR-PRP showing greater efficacy than LP-PRP. McLarnon et al. 26 highlighted the superior outcomes of PRP compared to corticosteroid injections, including improved pain management, reduced joint stiffness, and better participation in physical activities at 12 months. They also noted that administering 3 intra-articular PRP injections at weekly intervals may provide greater benefits than a single injection. 26 Collectively, these results underline the potential of PRP, across various preparation methods and regimens, to effectively address symptomatic knee OA. Our study builds on these findings by providing additional clinical and biological insights and emphasizes the need for further randomized controlled trials (RCTs) to refine PRP protocols, preparation methods, and patient selection. There is still debate on whether LP-PRP contributes to better clinical outcomes compared to leukocyte-rich PRP (LR-PRP).9,10,27-29 Xu et al. 8 conducted a comparative study between LR-PRP and LP-PRP to assess their impact on cartilage healing and activation of inflammatory pathways. This study found an improved response to the LP-PRP product in terms of cartilage healing, with reduced activation (or perhaps inhibition) of the NF-κB pro-inflammatory pathway. 8 However, Jayaram et al. 29 found a more anti-inflammatory effect of LR-PRP through the expression of interleukin (IL)-1Ra, IL-4, and IL-8. However, in the same study MMP 9, which has a chondrotoxic effect, was also found in higher concentrations in LR-PRP. 29 The chondro-regenerative effect of LP-PRP was also reported by Su et al. 30 Although some of these biological differences between the PRP preparations are of interest and warrant further study, it is important to remember that in a recent double-blinded clinical trial, Di Martino et al. 10 showed that there is no clinically significant difference between LR-PRP and LP-PRP for the treatment of knee OA. Similarly, Romandini et al. 31 found, in double-blinded RCT, no differences in safety, efficacy, or clinical outcomes between LR-PRP and LP-PRP for knee OA at all follow-up points. Furthermore, Abbas et al. 9 conducted a network meta-analysis and found no difference between LP-PRP and LR-PRP in PROMs for knee OA. Although, LP-PRP had higher Surface Under the Cumulative Ranking (SUCRA) scores for all PROMs at all follow-up times. 9
The lack of a clinically significant difference between LR-PRP and LP-PRP in treating knee OA, as demonstrated in RCTs and meta-analyses, may be attributed to several factors. First, while LP-PRP is designed to minimize inflammatory responses due to reduced leukocyte content, LR-PRP’s higher concentration of growth factors may counterbalance its pro-inflammatory effects, leading to comparable overall clinical outcomes. 23 Second, knee OA is a multifactorial disease influenced by a range of patient-specific factors, such as age, OA severity, and comorbidities, which may overshadow the biological differences between these PRP formulations. Third, variations in PRP preparation methods, injection protocols, and patient populations across studies could dilute the impact of leukocyte content on clinical outcomes. In addition, both LR-PRP and LP-PRP appear to exert beneficial effects on cartilage repair and inflammation modulation, albeit through different mechanisms, which may converge to produce similar PROMs.26,31 Future research should address these limitations by standardizing PRP preparation and injection protocols, stratifying patients by relevant clinical and biological variables, and incorporating biomarkers and imaging studies to better evaluate the differential effects of LR-PRP and LP-PRP on OA progression and symptom relief.
Interestingly, an older age in our cohort was also associated with improved outcomes. Korpershoek et al. 16 reported a similar finding in a larger cohort of ACP treated knee OA patients with a similar age range and mean. However, in other studies with an older age range and mean, no association was seen, 32 or on occasion, the opposite relationship was observed. 33 Together these findings could indicate that some younger patients may be unsuitable for ACP. Several factors could explain these differences: older patients may have lower activity levels and less expectations, which could influence their response to treatment. In addition, younger patients may have underlying knee issues, such as primary soft tissue injuries, traumatic meniscal or ligamentous pathology that could be contributing to their early-onset OA. These factors may affect their response to ACP treatment and could partly account for the observed variation. In our cohort, we found that patients who had undergone prior knee surgeries tended to be younger (median age 51 years) compared to those without previous operations (median age 55.6 years), although this difference was not statistically significant (p = 0.088). Further research is necessary to fully understand this relationship.
It is noteworthy that the overall treatment failure rate, as indicated by the failure to achieve MCID in our cohort, was 25% at 6 months. This is lower than the rate reported by Korpershoek et al. 16 where only 40% achieved MCID at 6 months. However, the outcome measures were different, with the Lysholm score used in our study and the Knee Injury and Osteoarthritis Outcome Score (KOOS) used in the other. In addition, although the demographics between the 2 studies were similar, Korpershoek et al. 16 included patients with a wider range of knee osteoarthritis grades (KL 0-4), whereas 90% of our patients were classified as KL 2 and 3. This variation in patient selection may partly explain the differences in outcomes and highlights the critical role that patient selection plays in achieving successful results. Furthermore, the product and its application differed across these studies, with the mean platelet count in the study by Korpershoek et al. 16 being higher than the current study (626.9 ± 165.7 vs. 588.5 ± 183.2 × 106/mL, respectively). However, baseline blood tests, including platelet counts, were not measured in the Korpershoek et al. 16 study, so the platelet fold increase in the ACP could not be determined. Conversely, the mean WBC and RBC counts were lower in our study (0.02 ± 0.02 vs. 0.06 ± 0.02 × 106/mL for WBC, and 0.49 ± 0.49 vs. 1.93 ± 3.1 × 106/mL for RBC). 16 These cellular differences may also have influenced the outcomes.
In Korpershoek et al.’s 16 study, we have also been informed that they performed the injection of ACP without prior aspiration of synovial fluid, whereas in our cohort, synovial fluid aspiration was conducted before the administration of ACP. This different way of administration of ACP may potentially influence the outcome observed. Further analysis of the aspirated synovial fluid could provide additional insights into its influence on the treatment.
We appreciate that this study has several limitations. The relatively small sample size may limit the generalizability of our findings. A larger, well-powered RCT could facilitate more detailed subgroup analyses, potentially explaining differences in ACP outcomes across studies and improving patient selection. The absence of a control group in this study represents a key limitation. Without a control group, it is difficult to distinguish the effects of the intervention from natural disease progression, placebo effects, or other confounding factors. In addition, this study includes only a single cohort which has the potential for placebo effect bias. However, the findings of this study provide a solid foundation for designing future RCTs to validate the efficacy of ACP for knee OA. The observed mean improvement in Lysholm scores (22.07 ± 22.63 points at 3 months) offers critical data for calculating the effect size and determining the required sample size. Future RCTs should include active comparators or placebo groups, such as hyaluronic acid, corticosteroids, or saline placebo, to establish ACP’s relative benefits and identify scenarios where it offers unique advantages. Subgroup stratification based on age (<50, 50–65, >65 years) and radiographic severity (KL grade I–III) will help identify patient populations most likely to benefit. Additional outcome measures such as WOMAC, KOOS, and EQ-5D should complement Lysholm scores. Extended follow-up (up to 24 months) is also recommended to assess the durability of ACP’s effects. Biomarkers, such as general inflammatory markers (C-reactive protein [CRP], interleukin [IL]-6, tumor necrosis factor [TNF]-α) or cartilage specific markers (COMP), could provide mechanistic insights and refine patient selection. The knee alignment axis, which was not recorded in this study, should also be documented in future research, as varus or valgus malalignment may influence outcomes. Future trials should also evaluate the cost-effectiveness of ACP compared to other treatments and involve multiple centers to enhance generalizability and account for variations in patient demographics, clinical characteristics, and socioeconomic factors. A proposed design could include a multicentre, double-blinded, placebo-controlled RCT with adults aged >18 years (KL grade I–III), comparing ACP, hyaluronic acid, and placebo, with follow-up at 3, 6, 12, and 24 months. Primary outcomes could include changes in Lysholm, WOMAC, and KOOS scores at 12 months, while secondary outcomes could evaluate quality of life, biomarkers, structural changes via magnetic resonance imaging (MRI), and cost-effectiveness.
Conclusion
Autologous conditioned plasma provided clinical benefits in this cohort study of knee OA patients for at least 6 months post-injection. Older age and a higher mean platelet concentration in the ACP were identified as predictors of a higher Lysholm score.
Footnotes
Abbreviations
ACP, autologous conditioned plasma; BMI, body mass index; IL, interleukin; IQR, interquartile range; K-L, Kellgren-Lawrence; KOOS, Knee Injury and Osteoarthritis Outcome Score; LR-PRP, leukocyte-rich platelet rich plasma; LP-PRP, leukocyte-poor platelet rich plasma; MCAR, missing completely at random; MCID, minimal clinically important difference; MMP, Matrix Metalo-proteinase; MI, multiple imputation; MSC, mesenchymal stromal cell; NICE, National Institute for Health and Care Excellence; OA, osteoarthritis; PDGF, platelet-derived growth factor; PRP, platelet rich plasma; PROMs, patient-reported outcome measures; Q-Q, quantile-quantile; RBCs, red blood cells; RCT, randomized controlled trial; REML, restricted maximum likelihood; SD, standard deviation; SUCRA, surface under the cumulative ranking; TGF-β, transforming growth factor-β; VEGF, vascular endothelial growth factor; and WBCs, white blood cells.
Acknowledgment and Funding
Not applicable.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Orthopedic Institute Limited, UK.