
Abstract
Background
Investigation of unjustified computed tomography (CT) scan in patients with minor head injury is lacking in Saudi Arabia. The purpose of the study was to evaluate the compliance and effectiveness of the Canadian computed tomography head rule (CCHR) in our emergency department (ED) and trauma centre and also to reduce the number of unjustified CT studies of the head in the centre.
Methods
A retrospective study of 368 ED patients with minor head injury was conducted. Patients who underwent CT scan between July 2010 and June 2011were selected from the ED head trauma registry by systematic randomisation. The CCHR was retrospectively applied on the patients’ charts to calculate the prevalence of unjustified head CT scans. A separate survey was conducted to evaluate three emergency physicians’ level of awareness about the CCHR and their ability to determine the necessity of CT scans with various clinical scenarios of head injury.
Results
The prevalence of unjustified CT scans as per the CCHR was 61.8% (95% confidence interval (CI) 56.5–66.9%). Approximately 5% of the sample had positive CT findings with 95% CI 2.9–7.6%. The CCHR correctly identified 12 cases with positive CT findings with 66.67% sensitivity. Only 24 (6.7%) had Glasgow coma scale scores less than 15 (13/14). The Glasgow coma scale correctly identified only two cases with positive CT findings with 11.11% sensitivity. The percentage of skull fracture (0.9% vs 5%, P = 0.030) was significantly lower in patients with unjustified CT scans than in patients with clinically justified CT scans. There was fair to substantial agreement between the ED physicians and the CCHR (κ = 35–61%). Two ED physicians identified all cases of justified CT scan with 100% sensitivity (95% CI 71.51–100%).
Conclusion
The level of education regarding the CCHR was found to be optimal among emergency physicians using a case-based scenario survey. The CCHR was found to have a poor compliance potential in the busy ED of our trauma centre and the prevalence of unjustified cranial CT scans remained high.
Introduction
Eighty-four per cent of head traumas are minor head injuries (MHIs). 1 Performing head computed tomography (CT) for every head injury would be time consuming and costly in addition to the radiation hazards. Therefore, the Canadian computed tomography head rule (CCHR) has been established. 2
Canadian computed tomography head rule.
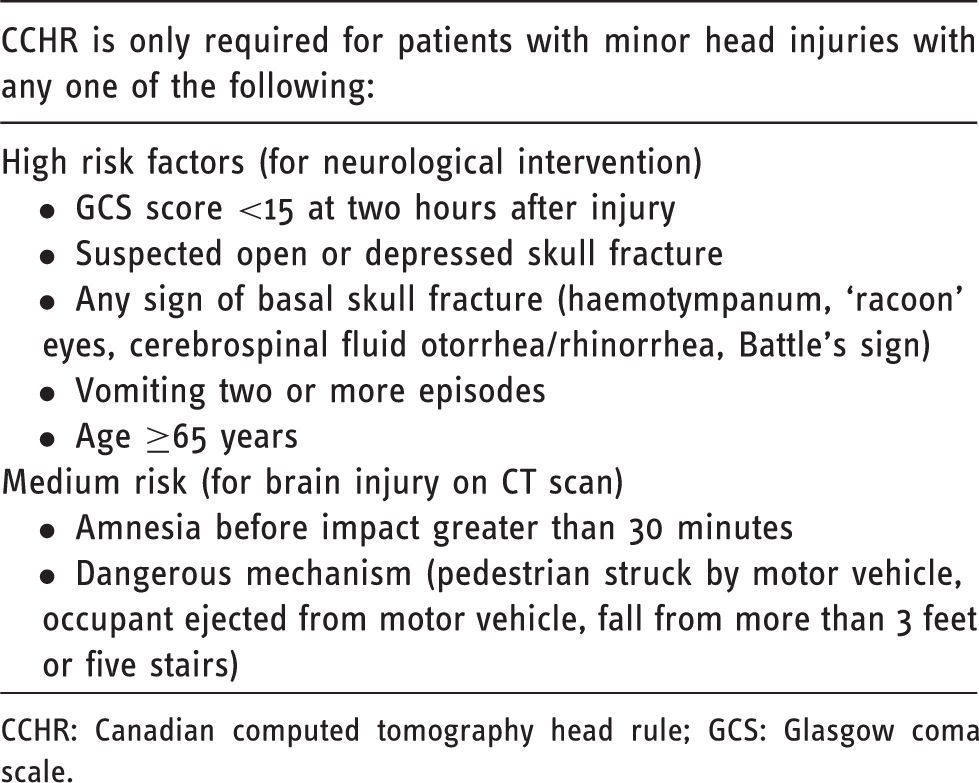
CCHR: Canadian computed tomography head rule; GCS: Glasgow coma scale.
The CCHR has very high sensitivity of 99–100% and a specificity of 48–77% in predicting the need for neurological intervention. 3 Its diagnostic value and superiority has been validated in some studies, along with the potential to decrease inhospital admission with CCHR guided practice. 4 The CCHR has also been shown to be more specific than the New Orleans criteria in predicting the need for neurosurgical intervention based on the results of CT examinations.5,6 Several other studies have commented on the validity of the CCHR; however, none had measured its effect in reducing the number of CT scans in a busy emergency department (ED) setting that applies the CCHR as the standard of care according to our knowledge.
A pilot study that evaluated the impact of the CCHR on British practice found that it would increase the number of CT scans performed for the evaluation of MHI; therefore, its use in optimising the management of MHI was questionable. 7 Furthermore, in a study conducted in Turkey the CCHR was applied retrospectively on patients with MHIs. The number of MHI patients with a significant head injury that required surgical intervention was six of 923 (0.6%) patients. This result was found to justify the ‘liberal’ use of CT scans rather than applying the CCHR. 3
We have tested the practical value of the CCHR by reapplying the guidelines to measure the number of unjustified head CT scans in a single high volume trauma centre, which has officially adopted the CCHR guidelines by policy. Moreover, sensitivity, specificity, positive and negative predictive values have been calculated to determine the accuracy of the CCHR guidelines in our centre.
Methods
This cross-sectional study was held in a tertiary care hospital, which hosts the largest trauma centre in our region. The institutional review board had approved this study without the need for informed consent. We conducted retrospective review of the records of head trauma patients who presented to the ED from June 2010 to July 2011.
The patients were selected from the ED registry of head trauma by systematic randomisation. The systemic randomisation was performed by selecting every other patient using medical record numbers from the ED head trauma registry. MHI patients were defined according to the CCHR including patients with a GCS score of 13–15 on presentation with witnessed loss of consciousness, amnesia, or disorientation. Patients with a GCS score less than 13, aged less than 14 years (as ≥14 years is considered the age of adulthood in our institution), acute neurological deficit, penetrating skull injury, trauma of more than 24 hours, pregnancy, known history of seizures, bleeding disorder, or returned for reassessment were excluded. The data extracted from patients’ charts included, age, gender, mechanism of injury, neurological symptoms, high and medium risk factors, associated injuries and head CT findings. Information on subsequent neuro-surgical intervention and neurological deterioration were recorded.
The primary outcome was the prevalence of unjustified CT scans in MHI as per the CCHR guidelines. The secondary outcome was to determine the prevalence of CT abnormalities among justified and unjustified CT scans. The sensitivity, specificity, positive and negative predictive values have been calculated to detect the CT abnormality and need for surgical intervention.
The prevalence of unjustified CT scans was determined by reapplying the CCHR to patients’ charts retrospectively. The type and prevalence of abnormalities were recorded by two radiologists with at least five years’ experience in reading trauma head CT, who were blinded to the clinical findings when reading the head CT scans. Cases with discrepancies in interpretation were further reviewed by a neuroradiologist for a final opinion. The types of abnormalities included soft tissue swelling, extradural haemorrhage, subdural haemorrhage, subarachnoid haemorrhage, intraparenchymal haemorrhage, intraventricular haemorrhage, cortical contusions, brain oedema, diffuse axonal injury, brain herniation/midline shift, skull fracture and facial bone fracture. A separate survey that was generated to evaluate ED physicians’ knowledge of the CCHR included scenarios of patients who presented to the ED with MHI. The scenarios were selected by systematic randomisation.
Statistical analyses
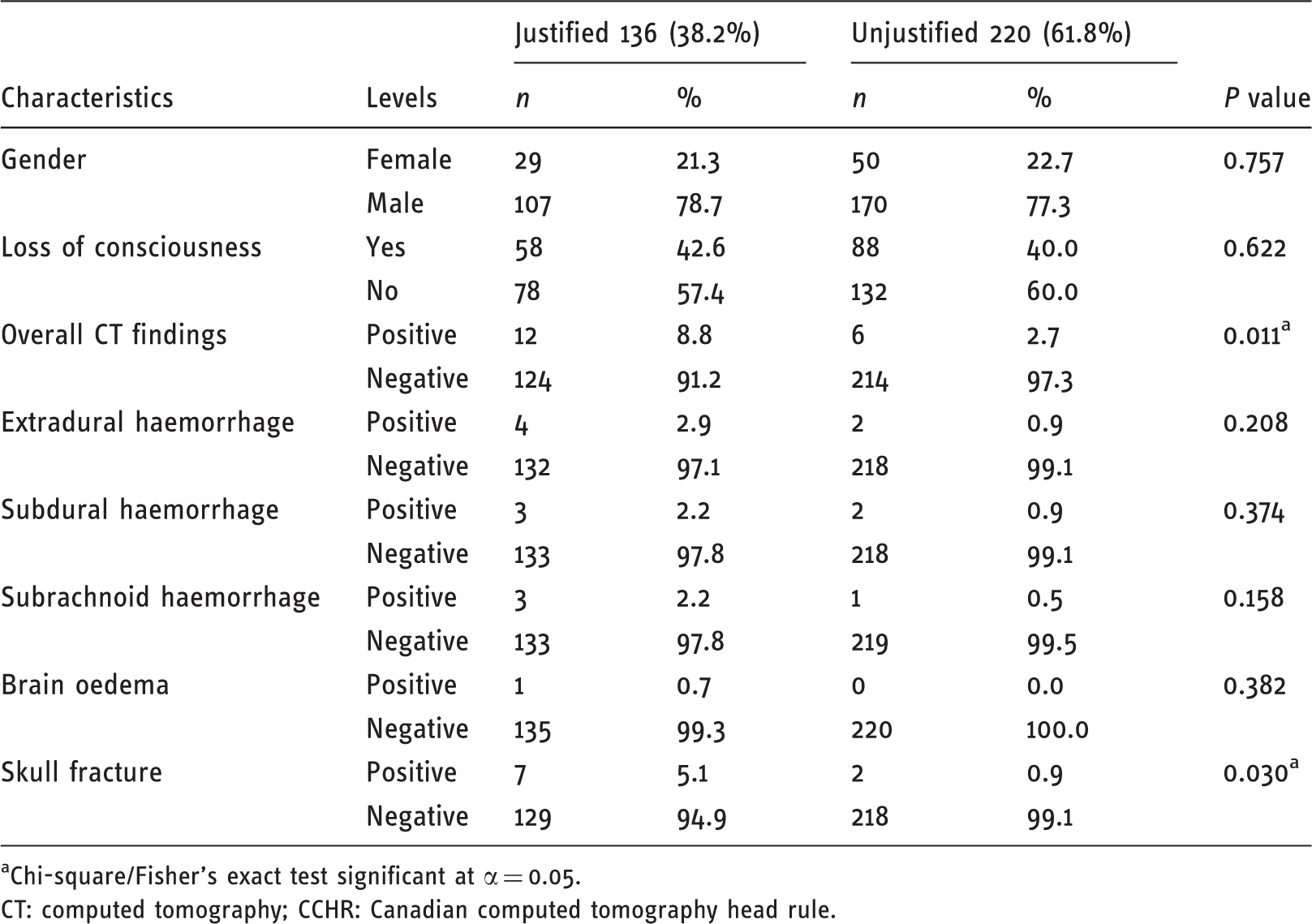
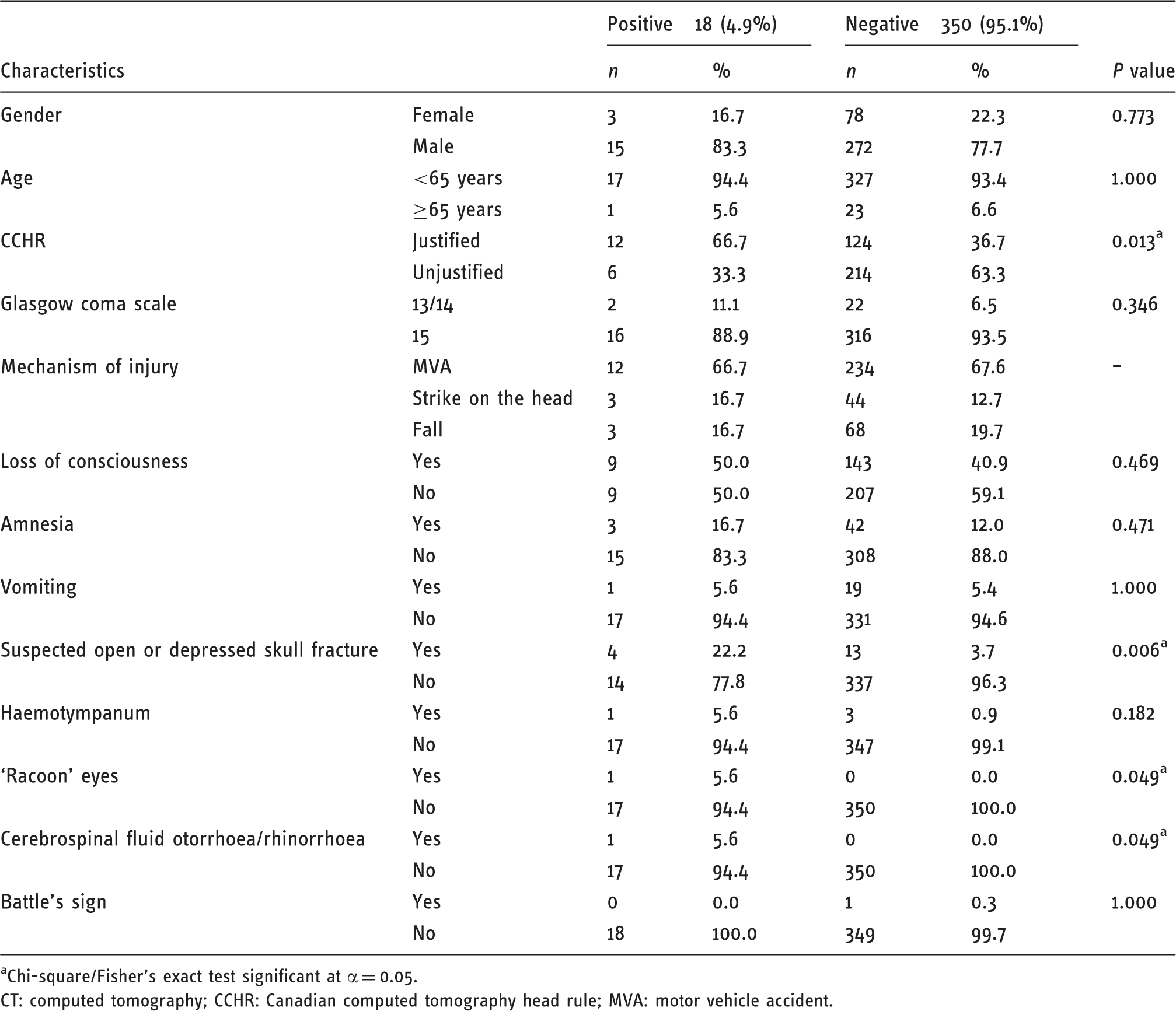
CCHR in relation to demographics and clinical features of head injury.
Chi-square/Fisher’s exact test significant at α = 0.05.
CT: computed tomography; CCHR: Canadian computed tomography head rule.
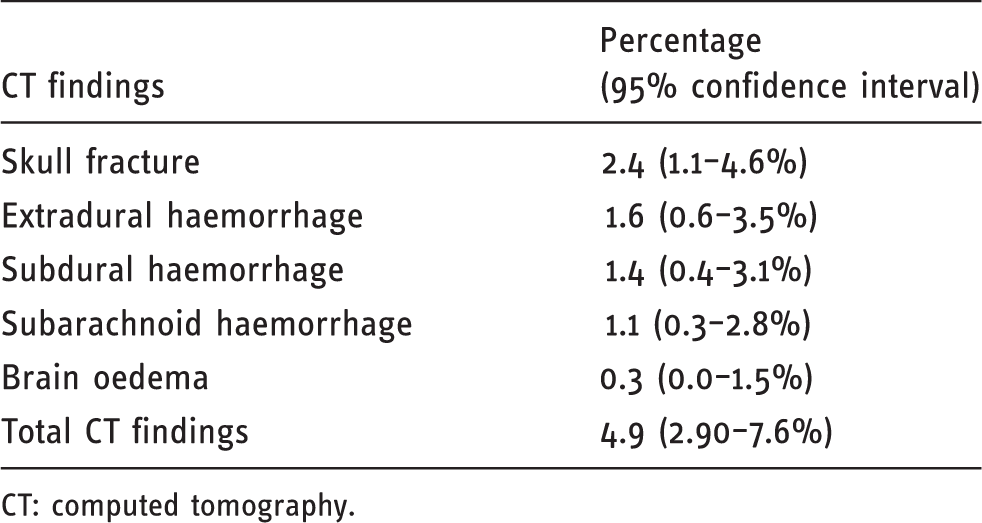
Prevalence of positive findings in all CT examinations with 95% confidence interval.
CT: computed tomography.
Differences in positive findings CT examinations by GCS.
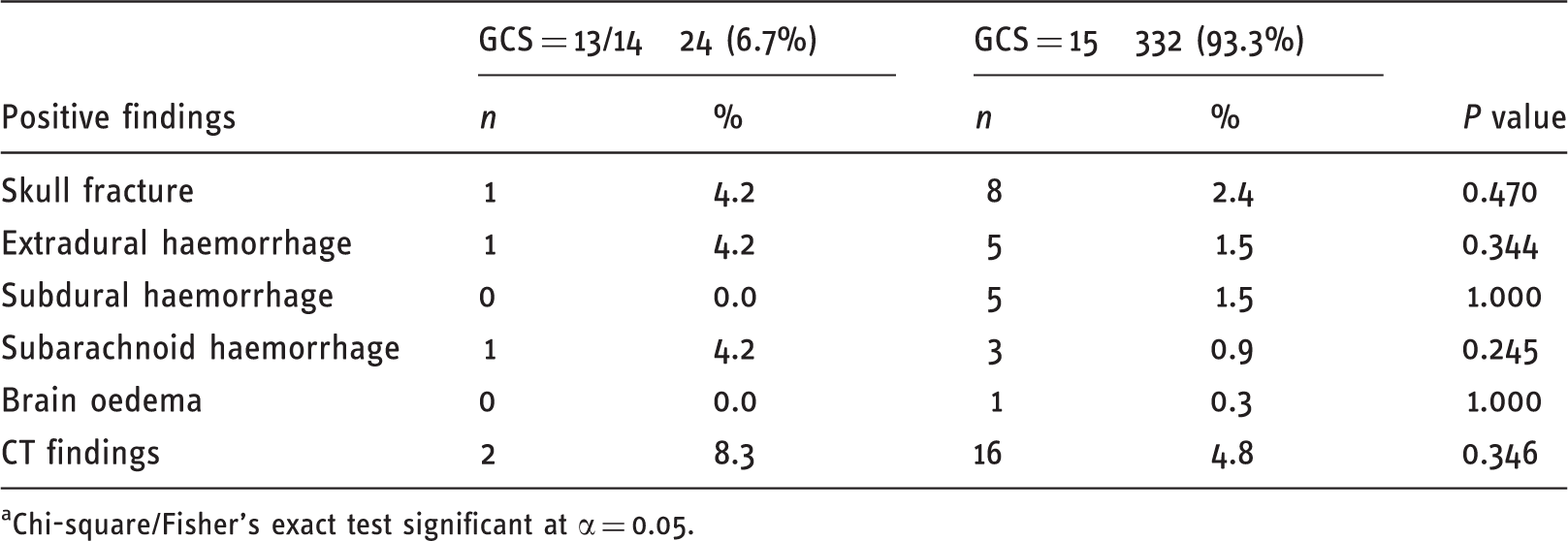
Chi-square/Fisher’s exact test significant at α = 0.05.
CT findings in relation to demographics and clinical features of head injury.
Chi-square/Fisher’s exact test significant at α = 0.05.
CT: computed tomography; CCHR: Canadian computed tomography head rule; MVA: motor vehicle accident.
Accuracy of GCS and CCHR in predicting CT scans findings.

GCS: Glasgow coma scale; CCHR: Canadian computed tomography head rule; CT: computed tomography; CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value.
Agreement/accuracy of physician diagnosis relative to CCHR.

CCHR: Canadian computed tomography head rule; CI: confidence interval.
Results
The study sample consisted of 368 patients who underwent CT scans out of an estimated 600 patients who presented to the ED with head injury during the study period from June 2010 to July 2011. Two hundred and eighty-seven (78%) were men. The average age was 30.5 (±17.3) years (range 14–106 years). The majority (61.8%; 95% CI 56.5–66.9%) of CT scans were not justified and only 38.2% complied with the CCHR guidelines (Table 2). Out of the patients who had abnormalities on the justified CT scans, only two had follow-up CT scans at 24–48 hours. One had stable haematoma and the other had interval improvement in the size of haematoma. None of the patients with unjustified CT scans had a follow-up CT scan as the haemorrhage was minor and the neuroradiologist only detected it when the study was conducted.
Table 2 also shows the CCHR in relation to demographics and clinical characteristics. The study observed a higher percentage of positive head CT findings in patients with justified CT scans than in patients with unjustified CT scans (8.8% vs 2.7%, P = 0.011; Figure 1). There were more positive findings of skull fracture in patients with justified CT scans than in patients with unjustified CT scans (5.1% vs 0.9%, P = 0.030; Figure 2).
Percentage of justified and unjustified CT scans by CT findings. Percentage of justified and unjustified CT scans by skull fracture.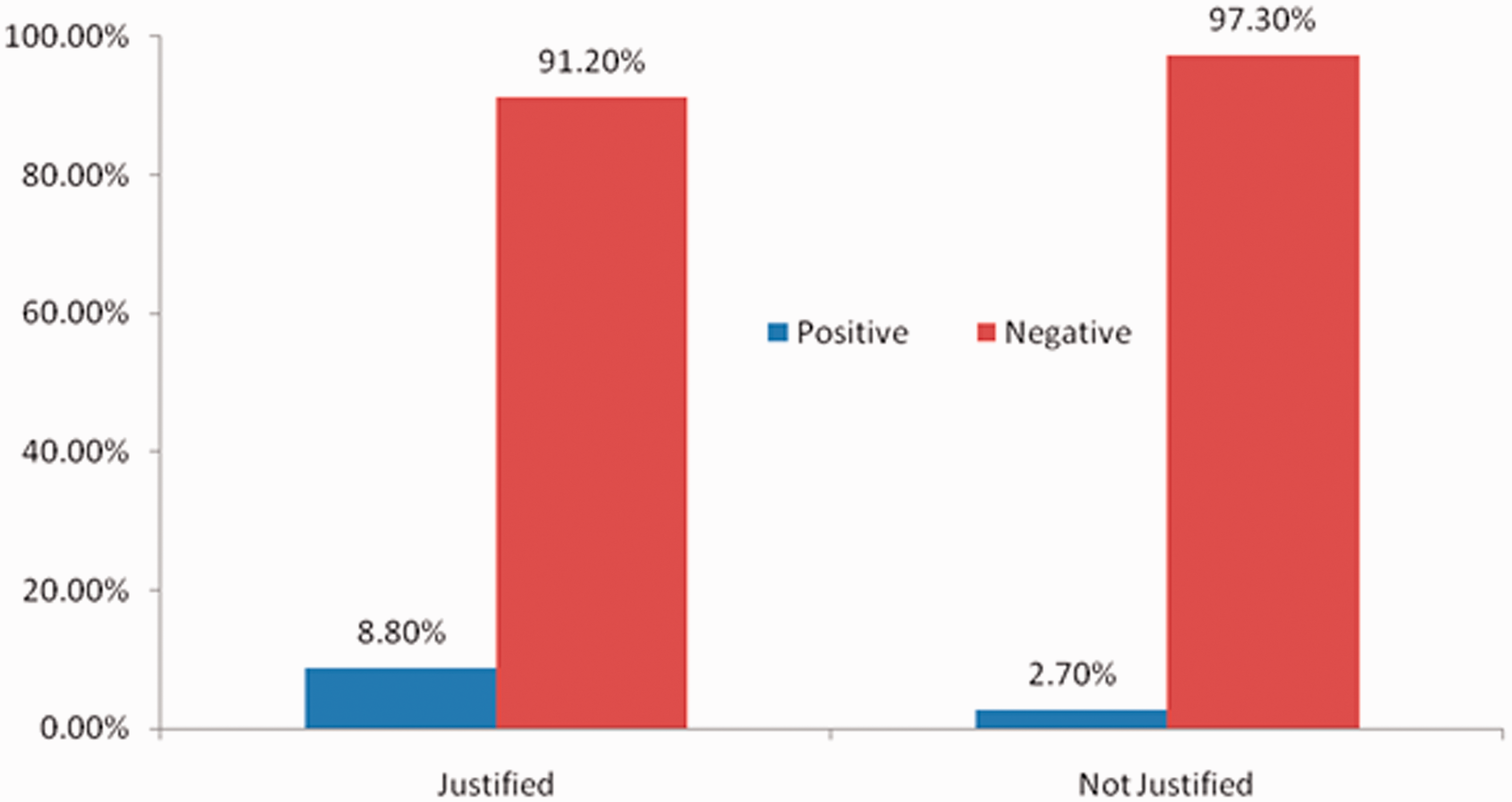
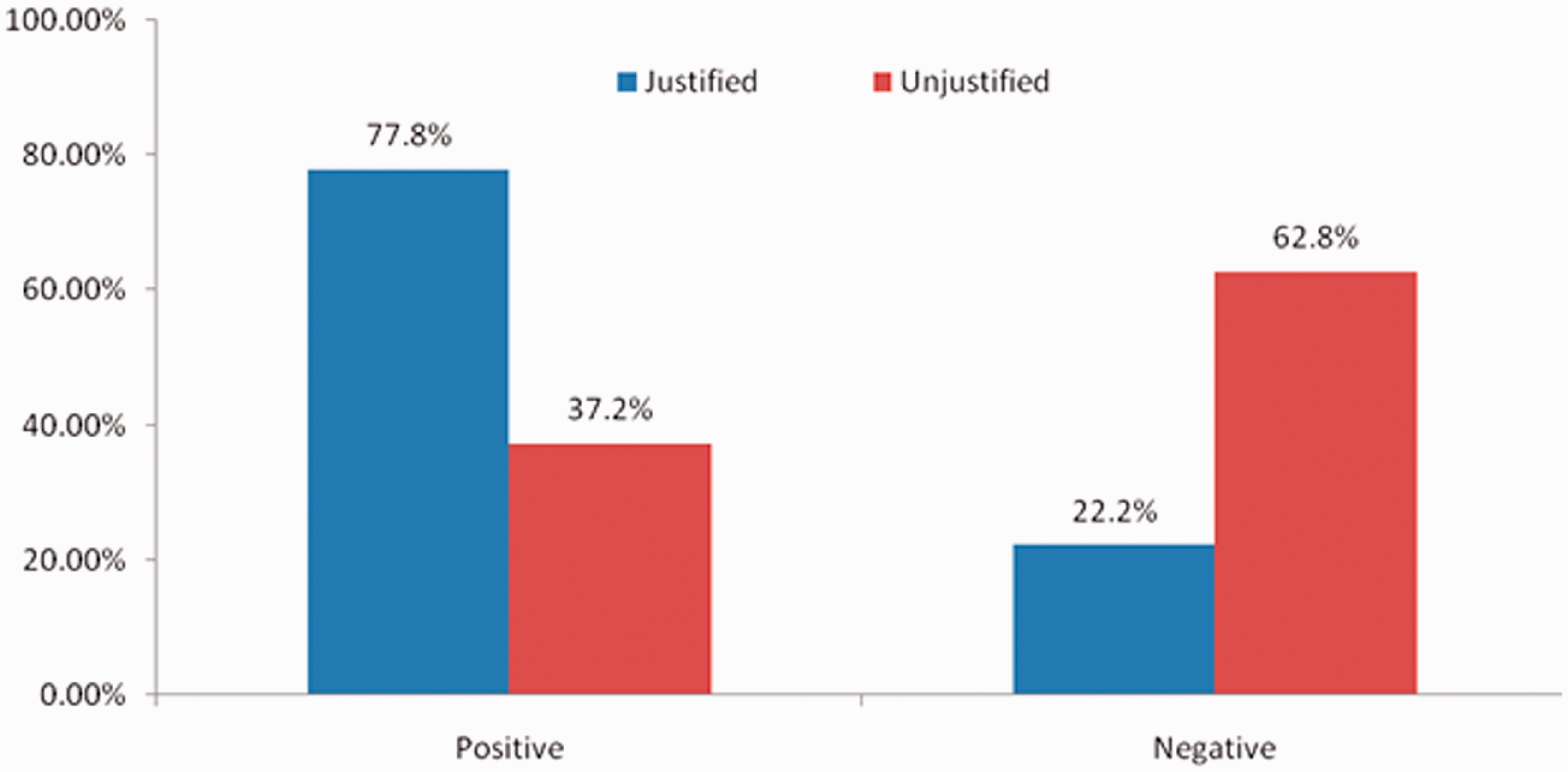
Table 3 shows positive head CT findings with 95% CIs. Excluding soft tissue swelling and facial bone fracture, the occurrence of positive CT findings was observed in 18/368 (4.9%) with 95% CI 2.9–7.6% (Table 3). The most common CT finding was skull fracture (2.4% of the patients with 95% CI 1.1–4.6%). Extradural haemorrhage (1.6%), subdural haemorrhage (1.4%) and subarachnoid haemorrhage (1.1%) were other positive findings. Please refer to Table 3 for other positive findings.
Table 4 shows positive head CT findings in relation to GCS. The majority (332; 93.3%) had a GCS of 15, and 24 (6.7%) had a high risk of traumatic intracranial lesion with a GCS of 13/14 (95% CI 4.4–9.9%). The percentages of positive CT findings were similar in patients with a GCS of 15 and a GCS of 13/14 (P > 0.05).
Table 5 shows CT findings in relation to demographics and clinical features of head injury. Motor vehicle accidents were the leading cause of head injuries (67.6%), followed by falls (19.5%), and strikes on the head accounted for (12.9%). Loss of consciousness occurred in (41.3%) of the patients. The CT scans revealed that 120 (32.6%) of the patients had at least one positive finding and (67.4%) had normal imaging. Nine (2.4%) of the 120 CT findings had skull fracture and 26 (7.1%) had facial bone fracture.
In patients with justified CT scans 66.7% had positive CT findings compared with 36.7% with negative CT findings (P = 0.013). In patients with suspected open or depressed skull fracture 22.2% had positive CT findings compared to 3.7% with negative CT findings (P = 0.006). The CT findings in patients with ‘racoon’ eyes or cerebrospinal fluid otorrhoea were positive in 5.6% of the patients and negative in none of the patients (P = 0.049). However, gender, age, loss of consciousness and mechanism of injury were not associated with positive CT findings (P > 0.05).
The accuracy of the GCS and CCHR in predicting positive CT scan findings are shown in Table 6. The value of a GCS score less than 15 in patients with MHI has very low sensitivity (11.11%; 95% CI 1.38–34.71%) but high specificity (93.49%; 95% CI 90.31–95.88%). Of 18 cases with positive CT findings, the CCHR identified only 12 cases with 66.67% sensitivity (95% CI 40.99–86.66). The specificity of the CCHR is nearly equivalent to the sensitivity (63.31%; 95% CI 57.93–68.46).
Table 7 shows the agreement/accuracy of physicians relative to the CCHR. The kappa (κ) value for the first physician’s (R1) interpretation of the CCHR was 61%. This was considered to be substantial agreement with the CCHR. In other words, R1 overestimated the risk in only 19.0% (four patients). R2 underestimated the risk in 33.3% (seven patients) with fair agreement (κ = 35%). R3 overestimated the risk in 26.3% (five patients). This was also considered fair agreement with the CCHR (κ = 41%). R1 and R3 had similar sensitivity (100%; 95% CI 71.51–100%). R2 had higher specificity (100%; 95% CI 69.15–100%) but low sensitivity (36.4%; 95% CI 10.93–69.21%).
Discussion
To avoid controversy and improve consistency in the care of MHI, many institutions have established guidelines such as those of the CCHR. We conducted this study in the largest trauma centre of our region that has adopted the CCHR guidelines by policy.
Patients above the age of 14 years were included because it is the age of adulthood in our centre based on local legislation. The indiscriminate scanning of patients with MHI is disadvantageous as it will be time consuming, costly and expose more patients to radiation. The cost of a single head CT scan in our centre is about US$400, which is 10 times that of a single CT scan in other countries. In addition, this practice will expose young trauma patients to unnecessary radiation.2,3,8
In this study, we surveyed ED physicians to assess their level of knowledge regarding the CCHR. The cases used in the survey were real cases that were selected randomly from the ED database, and the physicians were blinded to the cases in the survey. The survey was conducted in an office setting. Therefore, ED physicians may have scored even higher if it were conducted in a real setting. The results showed that they had moderate knowledge to use the CCTR as a guide in their practice. This could be another factor that led to the increase in the unjustified CT scans. Out of three ED physicians, two physicians had equivalently high sensitivity (100%) for identifying the CCHR. The third ED physician had higher specificity (100%) but low sensitivity (36.4%). However, the degree of agreement with the CCHR was found to be fair to substantial among emergency physicians using a case-based scenario survey. Therefore, there is a need to educate ED physicians.
Although our study observed a higher percentage of positive head CT findings in patients with justified CT scans than patients with unjustified CT scans, none of the patients required any neurosurgical intervention. In our study, the CCHR has shown relatively low sensitivity and specificity in predicting positive CT scan findings as compared to the study by Stiell et al. 4 These variations could be related to a smaller sample size and the skills of ED physicians.
The literature supports the use of guidelines for managing MHI because it does not miss significant injuries that require neurosurgical intervention. 9 However, these studies have assessed their applicability prospectively or retrospectively in a controlled setting unlike our study that assessed its applicability retrospectively in a hospital that applies the CCHR as the standard of care. Where several studies have proved the efficacy of the CCHR in reducing the number of unjustified CT scans, a prospective study by Stiell et al. had an opposing result that showed that use of the CCHR had increased the number of CT scans and hospital admissions instead of decreasing them, which was consistent with our results.3,10–12 Further studies are needed to evaluate the benefits and limitations of the CCHR.
There are a few limitations to this study including its retrospective design. However, a retrospective design was appropriate to study the application of the CCHR in a real-life setting. The study is also limited to one institute; naturally a multicentre study would yield a more confident measure of the applicability of the CCHR.
Conclusion
The CCHR is a useful tool to diagnose MHI and reduce the number of unnecessary head CT scans. The chance to miss a CT abnormality is estimated to be 0.87%. However, its application in the busy ED setting of our institution was not very efficient. The percentage of unjustified CT scans remains high. We, along with other investigators, however, continue to be concerned that the criteria have too low a sensitivity and specificity for predicting the need for neurological intervention. As our institution has officially adopted the CCHR guidelines, we decided to assess the validity of the guidelines in our institution to determine its sensitivity, specificity, reliability and acceptability.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.