
Abstract
Background
The pseudoaneurysms of the internal carotid artery (ICA) at the skull base form a unique subset of craniofacial pseudoaneurysms with varied diagnostic and therapeutic challenges. Recurrence in a surgically treated pseudoaneurysm may become a nightmare due to very limited number of open and endovascular options.
Report
We report a rare case of recurrent pseudoaneurysm of petrous ICA, which presented with massive epistaxis following an initial successful occlusion by surgical trapping of the parent arterial segment with surgical clip. Cerebral angiography revealed filling of the pseudoaneurysm by small arterial channels from the external carotid, contralateral internal carotid and basilar arterial branches and emptying through the “slipped” distal clip. After a meticulous analysis of the cerebral angiogram, the recurrent pseudoaneurysm was eventually embolized retrogradely through the “slipped” clip after crossing the anterior communicating artery taking a contralateral internal carotid access.
Conclusion
Scrupulous planning and execution of ICA pseudoaneurysms is necessary to prevent recurrence. Naturally occuring collateral routes through the Circle of Willis aid in treatment of “unreachable” vascular lesions.
Introduction
The pseudoaneurysm of the internal carotid artery (ICA) in the petro-cavernous segment is a rare entity, usually associated with craniofacial trauma. Apart from the potentially fatal oto-nasal hemorrhages, atypical clinical presentations, and the tendency of recurrences, it poses peculiar therapeutic and technical problems. 1 A prompt definitive treatment is the key to a good clinical outcome. 2 Recurrence following surgical treatment may occur and prove catastrophic if not dealt with suitably. Retreatment is much more challenging as in most cases the access may be compromised by the first surgery. We describe the following case, after obtaining a written informed consent of the patient, of a recurrent ICA pseudoaneurysm with massive epistaxis following surgical trapping, which was managed with trans-communicating (via anterior communicating artery) access through the distal trap door.
Initial presentation and surgical management
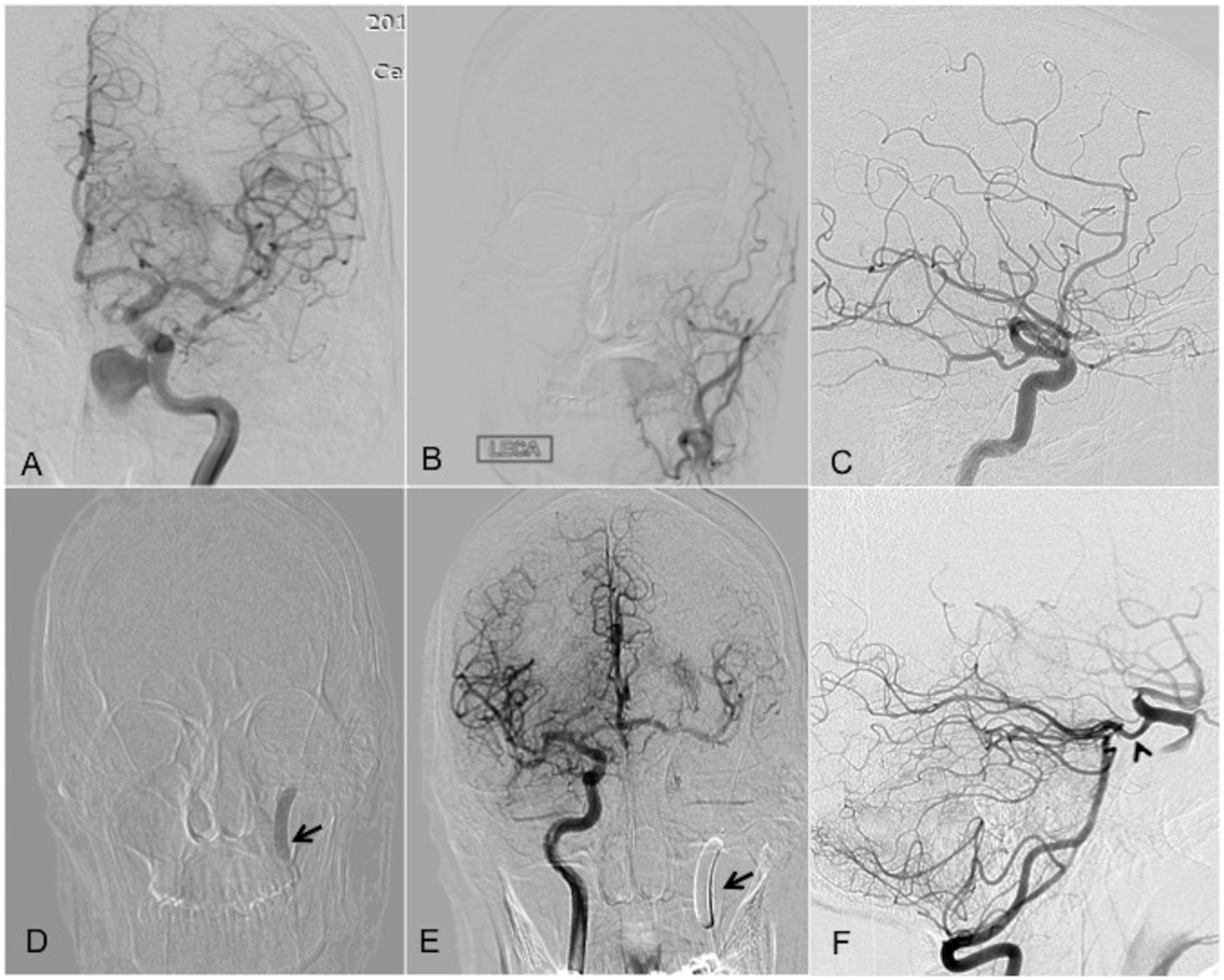
A 42-year-old male, having a history of painless episodic left-sided epistaxis of about 4 months duration (3–4 episodes per month), was referred from a peripheral center with massive nasal bleed of approximately 1.5 L. Immediate resuscitative measures were adopted in the form of hydration with crystalloids and three units of blood. Simultaneous nasal packing was performed leading to temporary tamponade with cessation of nasal bleed. Detailed historical evaluation at this time revealed a road-traffic accident 5 years back for which he required transient hospital admission but suffered no major injuries or neurological issues. There was no other relevant history or systemic complaints or infection related to the paranasal sinuses. MRI done elsewhere revealed abnormal flow-related signal in the left sphenoid sinus showing enhancement on gadolinium enhanced T1 sequence (Figure 1). It was surrounded by hematoma in the remaining sinus. There was expansion of the sinus cavity with erosive bony changes. Subsequent digital subtraction angiography (DSA) confirmed the pseudoaneurysm arising from the infero-medial wall of petrous ICA projecting into the sphenoid sinus with no active contrast extravasation (Figure 2(a)). No opacification was noted from the left external carotid artery injection (Figure 2(b)) or right ICA injection (Figure 2(c)). Balloon test occlusion (BTO) was performed which was well tolerated with adequate flow across the ACom and PCom arteries (Figure 2(d) to (f)). The options of endovascular carotid reconstruction by a flow-diverting stent or a stent graft and surgical/endovascular trapping of the pseudoaneurysm segment were discussed with the patient who opted for surgical ligation due to cost constraints and its definitive nature with perceived negligible recurrence rates. Thereafter, the aneurysm harboring left petro-cavernous ICA segment was trapped by means of a surgical clip distal to the ophthalmic artery and ligation of the left ICA at origin. The patient recovered well and was discharged in a stable condition with no repeat bout of bleed. Diagnostic imaging at presentation with massive epistaxis using MRI (A–C); axial T2 (A), non-contrast T1 (B), and post-contrast T1 (C) weighted imaging showing the flow void (white arrowhead) within the hemosinus with homogeneous contrast enhancement suggestive of a pseudoaneurysm. Note the perianeurysmal hematoma within the sinus cavity. Left internal carotid DSA (A) demonstrating the petro-cavernous segment pseudoaneurysm projecting inferomedially into the sphenoid sinus. Left external carotid (B) and right internal carotid (C) angiograms are unremarkable. Subsequent balloon test occlusion (BTO) showing balloon inflation (arrow) in the left distal cervical ICA (D) which the patient tolerated well. Crossflow across the ACom A. and PCom A. (arrowhead) is demonstrated on right ICA (E) and left vertebral (F) angiograms.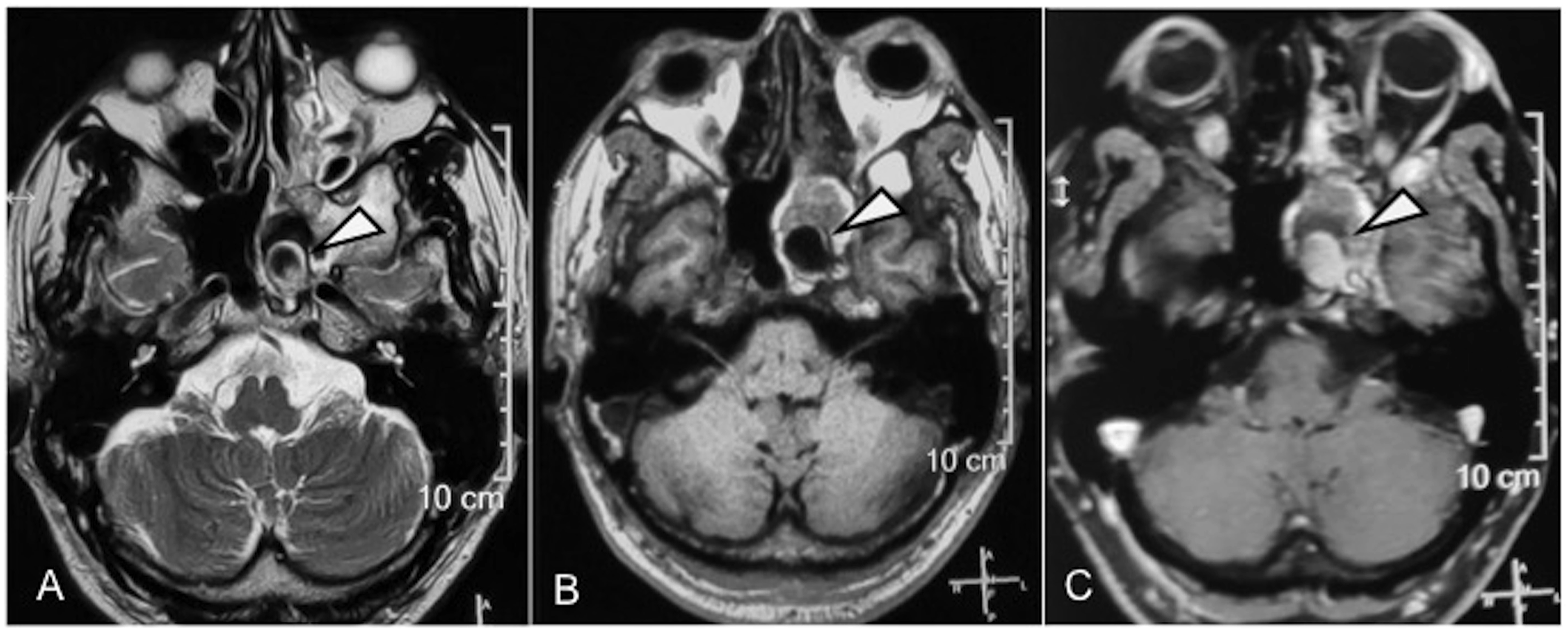
Second admission and definitive endovascular management
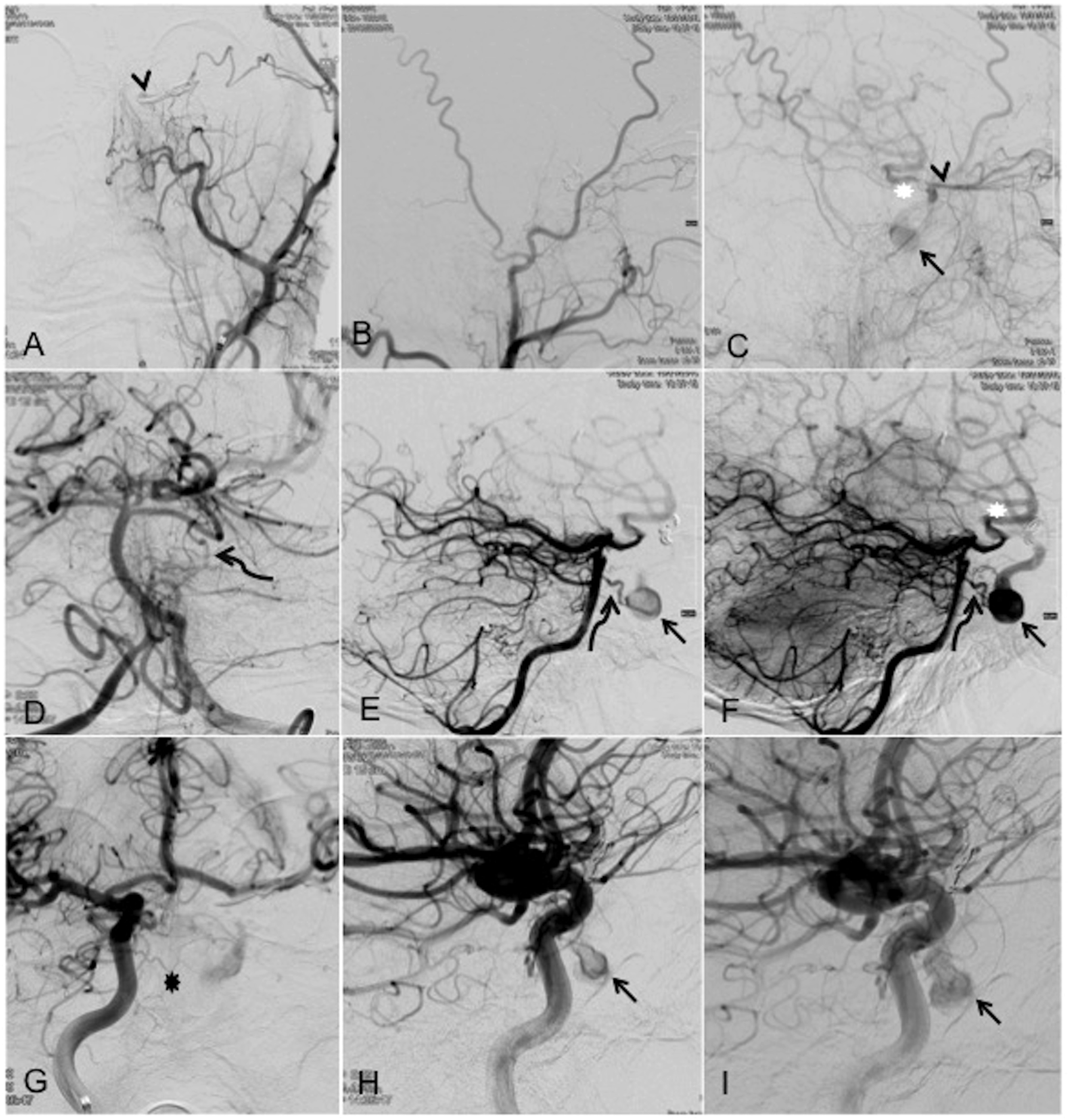
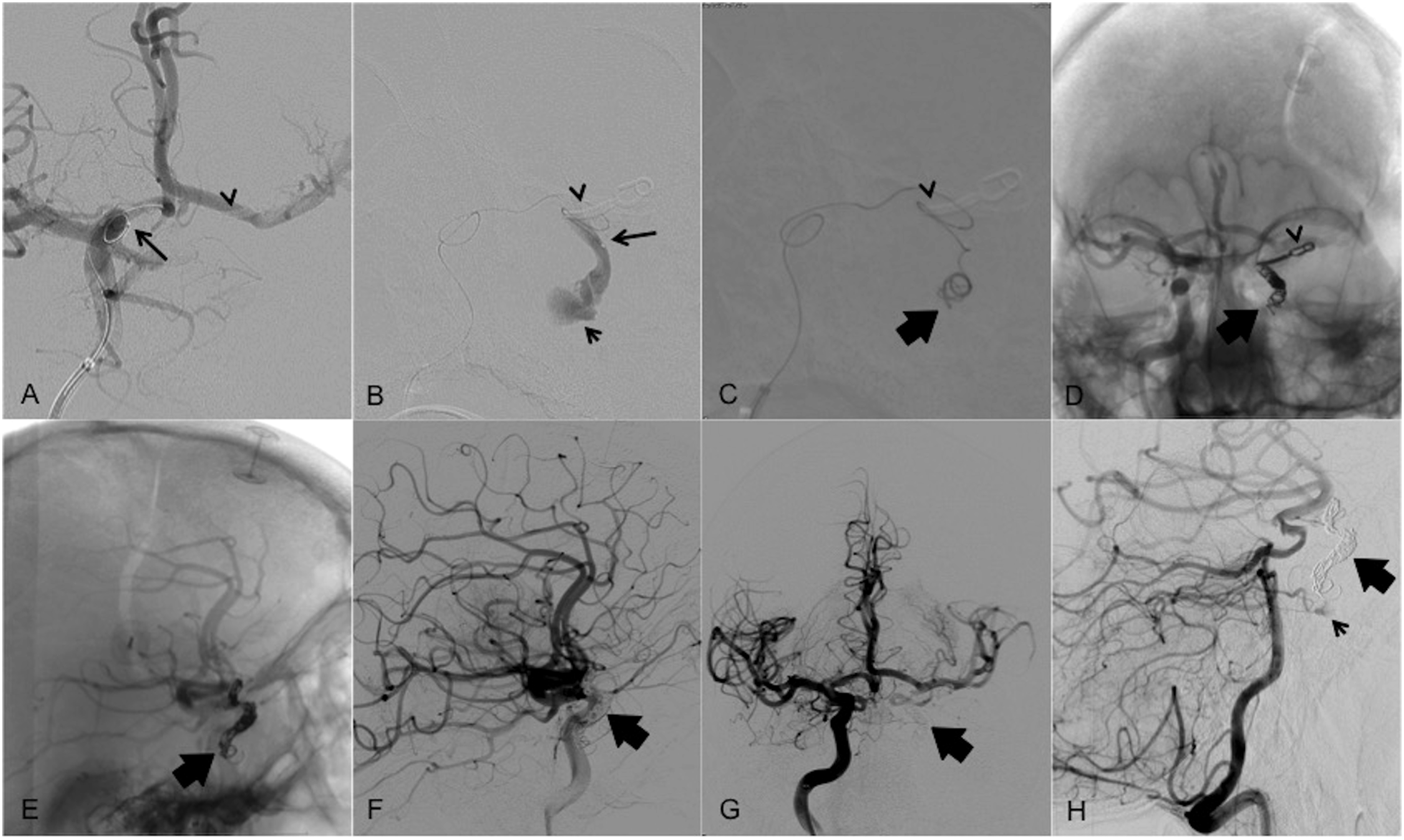
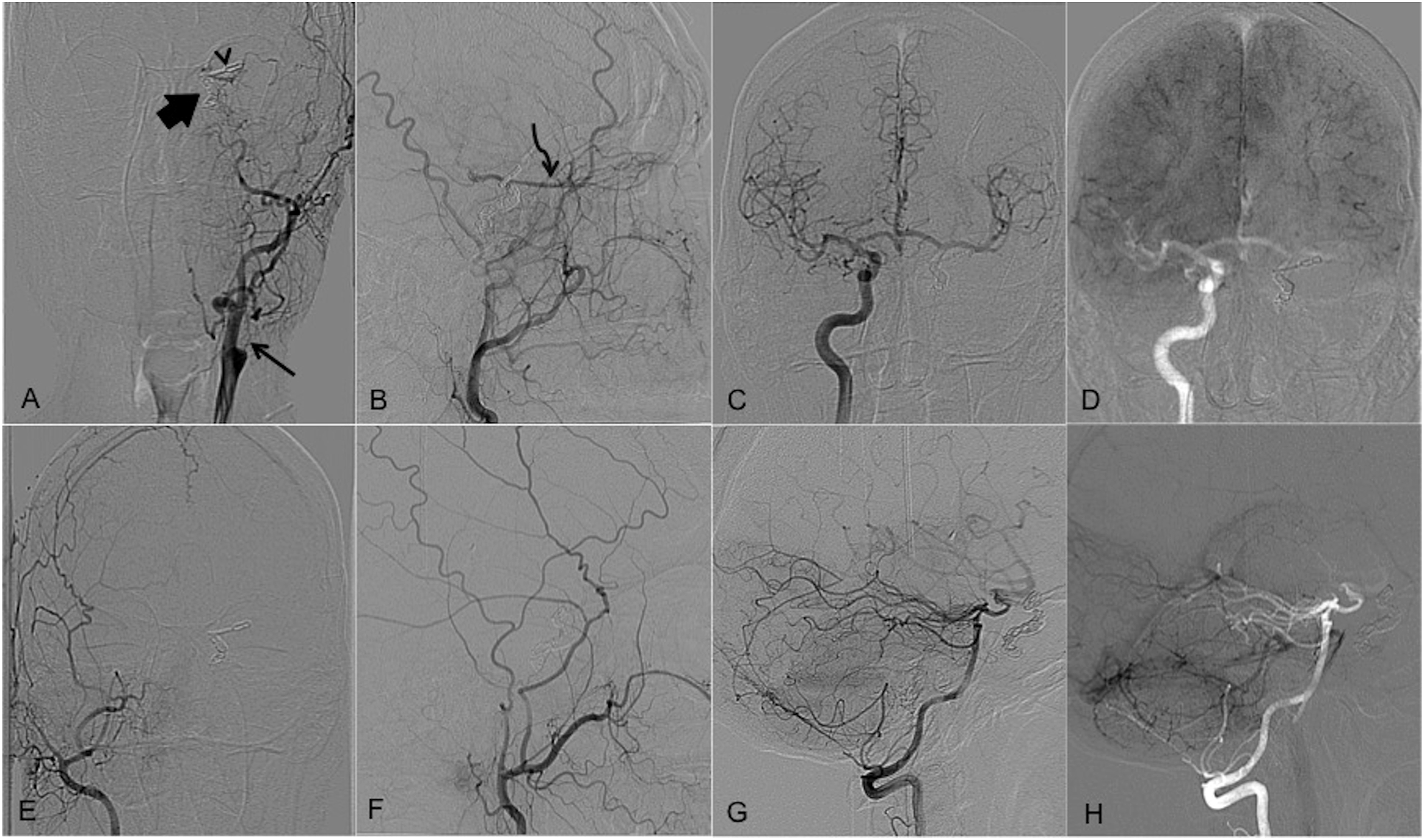
He reported again within a month with a bout of massive nasal bleed of approximately 1L over a span of a few minutes for which he underwent nasal packing at a peripheral center. Urgent non-contrast computed tomography (NCCT) and CT angiogram revealed recurrent filling of the ICA pseudoaneurysm (Figure 3(a) and (b)). As it was a single-phase study, the source of contrast opacification of the pseudoaneurysm could not be deciphered for which a DSA was planned. The left common carotid injection (Figure 3(c)) showed optimal occlusion at the ligated origin of the left ICA with no antegrade contrast flow. However, there was faint opacification of the left sided intracranial circulation (Figure 3(d)). Left external carotid, right internal carotid (IC), and left vertebral angiograms, however, showed filling of the pseudoaneurysm through the left temporal-ophthalmic artery anastomosis, bilateral ICA petro-cavernous dural anastomosis, and left superior cerebellar-left cavernous ICA (presumed hypoplastic persistent primitive trigeminal artery-PTA) anastomosis, respectively (Figure 4). Notably, the contrast run-off was seen into the left supra-ophthalmic ICA, across the surgical clip. No opacification of the aneurysm was visualized on right ECA runs. Open surgical means of pseudoaneurysm occlusion was now out of question except for the difficult resort of coagulating it through the trans-sphenoidal access. With the preparedness to tackle the pseudoaneurysm by endovascular access, the patient was prepared for angiographic means of cure through one of the indirect accessory-anastomotic routes. Unfortunately, the external carotid and vertebral arterial accesses through the temporal-ophthalmic and supposed primitive PTA anastomosis proved futile due to extreme tortuousity and narrow caliber of these channels. After diligently studying the angiograms at this time and ascertaining the fact that the injected contrast was able to make an exit from the pseudoaneurysm through the “surgically clipped” supra-ophthalmic ICA prompted us to attempt retrograde navigation across the clipped artery through the anterior communicating artery (ACom A.) access from the contralateral ICA (Figure 5). A 6 F guiding catheter, Neuron 6F (Penumbra, Alameda, California, USA) was placed in the right distal-most cervical ICA, and optimal 3D rotational angiography was obtained. Careful navigation of the microguidewire, Traxcess 14 (MicroVention, Tustin, California, USA) through the steam-shaped Headway Duo® 156 cm (MicroVention, Tustin, California, USA) was done across the ACom A. and retrogradely till the left ICA just beyond the clipped segment (Figure 5(a) and (b)). At this point, gentle rotatory movements were initiated in a bid to cross the clip. During one of these rotations, the guidewire tip slipped into the trapped ICA with a minor jerk. It was stabilized just distal to the pseudoaneurysm over which the microcatheter was threaded diligently in a smooth uniform motion. Successive coiling was done thereafter (Figure 5(c) to (e)) resulting in complete obliteration of the pseudoaneurysm. Needless to say, in the absence of adjunctive options like balloon assistance or distal access catheter, a strict vigil was kept at all the curves (three near perpendicular curves) throughout the coiling upto the endpoint of optimal coil mass density within the distal trapped segment of the artery near the surgical clips. Post-coiling right carotid run (Figure 5(f) and (g)) showed no filling of the pseudoaneurysm from the cavernous ICA dural branches. Left vertebral artery angiogram showed stasis of contrast in the pseudoaneurysm (Figure 5(h)). The patient was subsequently discharged in a stable condition. Follow-up four-vessel angiogram at 1 month (Figure 6) showed complete pseudoaneurysm occlusion with no other abnormality. He is doing well clinically at 6 months with no further episodes of epistaxis. Diagnostic imaging after segmental entrapment of left petro-cavernous ICA: Maximum intensity projection images of CT angiography in coronal (A) and axial (B) planes showing the recurrent pseudoaneurysm (white arrow) projecting into the sphenoid sinus. DSA images of the left common carotid run (C, D) show smooth cut-off at the ligated left ICA origin (black arrow) with faint opacification of the intracranial MCA branches (star) signifying some flow through probable ophthalmic anastomotic route. Note the clip (arrowhead) applied at the supraclinoid ICA. Diagnostic subtraction angiograms after segmental entrapment of left petro-cavernous ICA demonstrating recurrent ICA pseudoaneurysm (arrow): Left ECA frontal (A) and lateral (B, C) projections showing progressive retrograde filling of the pseudoaneurysm (arrow) through the temporal-ophthalmic artery (arrowhead)-ICA anastomosis. The supra-ophthalmic ICA (white star) is also opacified with contrast flowing antegradely across the clip. Left vertebral angiogram frontal (C) and lateral (E, F) projections show antegrade pseudoaneurysm opacification (arrow) through a tortuous channel arising from the superior cerebellar artery (curved arrow) that could represent a remnant of primitive persistent trigeminal artery and subsequently seen to clear off into the supra-ophthalmic ICA (white star). Antegrade contrast filling of the pseudoaneurysm (arrow) is also seen on right ICA angiograms—frontal (G) and lateral (H, I) projections through intercavernous dural branches. Endovascular coiling with contralateral carotid access showing pseudoaneurysm (short arrow), microcatheter tip (long arrow), surgical clip (thin arrowhead), and coil mass (thick arrow) positions: Digital subtraction angiographic images show microcatheter maneuvering at the anterior communicating artery (A) and across the surgical clip (B). The fluoroscopic images show initial (C) and final (D, E) coil mass configuration. Post-coiling right internal carotid artery angiograms lateral (F) and frontal (G) projections show no opacification of the pseudoaneurysm or the entrapped segment of left ICA. Left vertebral run (h) shows minimal contrast staining of the pseudoaneurysm through the anomalous tiny feeder. Follow-up angiogram after 1 month following endovascular coiling showing no residual pseudoaneurysm with coil mass (thick arrow) and surgical clip (thin arrowhead) in situ. Left common carotid runs frontal (A) and lateral (B) projections showing occluded ICA origin and retrograde flow in the left ophthalmic artery (curved arrow), partially reforming the supraclinoid ICA flow. Right internal carotid (C) and left vertebral (G) artery runs with corresponding re-masked images (D and H) in the late parenchymal phase show no residual pseudoaneurysm. Right external carotid artery injections (E, F) do not show any abnormal contrast staining. The anomalous tiny feeder from the left superior cerebellar artery, seen in the immediate post-embolization angiogram is also not seen.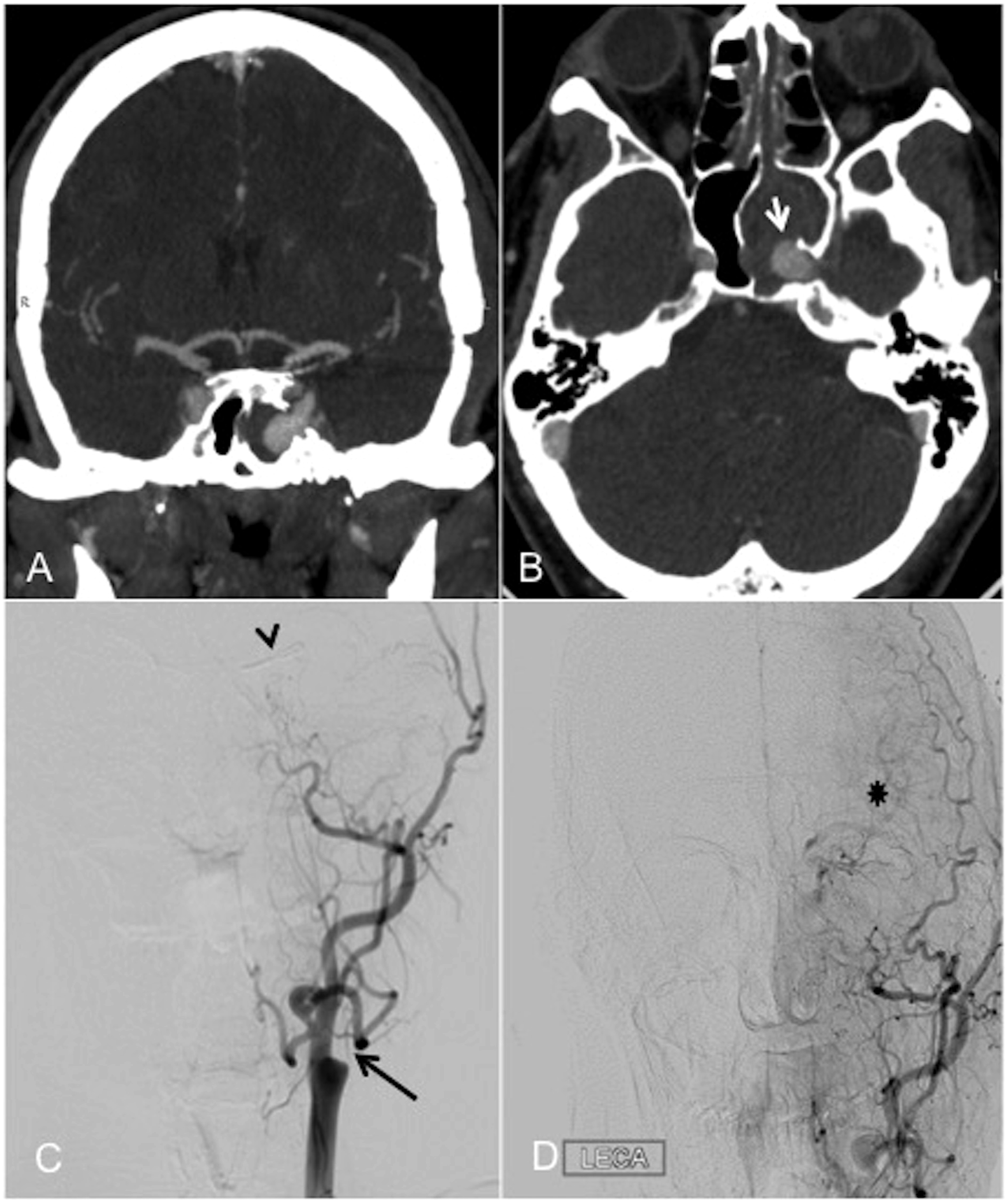
Discussion
The ICA pseudoaneurysms around the base of the skull are known to present usually with a clinical triad (Maurer’s triad) of prior craniofacial trauma, massive epistaxis, and ipsilateral visual disturbances. 3 The causes other than the trauma can be skull base infections, malignancy, arteriopathy, radiation, iatrogenic, or a combination of these. 4-6 The myriad clinical presentations may also include otorrhagia, tinnitus, Horner’s syndrome, and cranial nerve palsies.7,8 Our patient did not have upfront clinical or imaging-based markers of trauma, neither the audio-visual abnormalities. The petro-cavernous (extradural) variety ICA pseudoaneurysms are rare entities, posing unique treatment challenges to open surgery as well as endovascular intervention alike, owing to the anatomical and hemodynamic intricacy therein. The BTO tolerance opens up the options of deconstructive methods without an ECA-MCA bypass. 9 With the recent surging advances in the hardware, technology, and skills, endovascular neurointervention is becoming a safe and effective alternative management strategy. Although newer endovascular parent vessel sparing techniques using flow diverters and covered or layered stents are also well-described, their utility in the tortuous anatomy at the skull base may become limited many times.10–12
Surgical clipping is known to score over coiling for lasting protection against intracranial aneurysmal recurrence in general; however, the causes of incomplete occlusion can be multifold including a difficult surgical approach at the skull base, incompletely included vessel wall within the clip and clip-slippage among few others.
13
The index case is unique for a variety of reasons, the foremost of which is the slippage of aneurysmal clip, which permitted blood flow to and from the pseudoaneurysm to the supra-ophthalmic ICA through the “clipped” arterial segment. To the best of our knowledge, this has not been reported previously in the neurosurgical literature. Although this was a probable reason for the re-establishment of blood flow in the pseudoaneurysm sac and therefore its recurrence, as it provided an exit of blood into the intracranial circulation across the clip, it ironically also proved to be a blessing in disguise as it also provided an access channel to reach the pseudoaneurysm. A second open surgery was naturally out of the question due to the challenges of adhesions related to previous surgery and a host of other technical and access limitations. Endovascular option also seemed challenging due to loss of direct access, recruitment of non-cannulable small feeders, dangerous arterial anastomoses, and challenging alternative access routes. However, this seemed to be the more realistic of the two options. Endovascular routes thus available were: 1. Ipsilateral external carotid artery route through the temporal-ophthalmic artery ICA anastomosis (Figure 4(a) to (c)). This access was taken and the microcatheter tip was ferried till very close to the ophthalmic artery. However, it was far enough to warrant injection of liquid embolic agent for the embolizing material to reach the pseudoaneurysm. The disadvantages of this could be two-fold high probability of central artery occlusion and resultant blindness and left MCA thromboembolism (due to exit of the liquid embolic through the patent clipped segment) causing right hemiparesis. This was thus aborted. 2. Vertebral artery route though branches originating from the superior cerebellar artery (suspected primitive PTA remnant) demonstrated on vertebral artery angiograms (Figure 4(d) to (f)). High frame rate injections however indicated that these channels were too thin to allow microcatheter navigation. This route was thus truncated, too. 3. Contralateral ICA through the ICA intercavernous anastomotic channels (Figure 4(g)). For reasons similar to 2, this route also was not considered suitable. 4. Vertebral artery route through the ipsilateral posterior communicating artery (PCom) into the pseudoaneurysm crossing the clipped segment. This was initially considered but was kept as a second resort due to narrow caliber of P1 segment of left posterior cerebral artery, which had the potential of a failure as well as injury to that segment and consequent rupture. 5. Contralateral ICA through the Acom A. and thence retrogradely into the pseudoaneurysm across the clipped segment of the artery. This route was finally opted due to its relative safety and seemingly successful outcome. It is to be reiterated here that maneuvering across the ACom A. requires gentle dexterity due to chances of twisting the vessel during manipulation leading to dissection, rupture and thromboembolism. A dedicated roadmap is really helpful to guide the path of the microcatheter. The step of finding way retrogradely through the “clipped” artery also needs precise and careful hand–eye coordination lest may cause vascular injury.
Multiple studies have described coiling after clipping of cerebral aneurysms, 14 but coiling across the clipped segment has not been previously described. We propose naturally occurring intracranial anastomotic channels, namely, ACom A. and PCom A. as reasonably efficacious routes to access “difficult-to-access” lesions requiring some skills. A rare possibility of spontaneous transnasal coil extrusion as a cause of recurrence may also need emphasis 15 at this point, the risk of which, though, was extremely remote in this setting of complete on table occlusion of the pseudoaneurysm.
The case also highlights the value of studying the angiograms in detail. Meticulous observation of the flow of contrast on successive frames in respective arterial injections is mandatory. The clearing of contrast injection through the clipped arterial segment prompted us to take the same path for microcatheter access successfully. “Searching for suitable routes” to access the pseudoaneurysm was our major goal and once it was achieved, gentle and careful navigation across the tortuous but precious vascular route was our prerogative, which too was realized through patient maneuvering. The end result was extremely satisfying, to say the least. To the best of our knowledge, successful coiling of the petrous ICA pseudoaneurysm after parent artery entrapment surgery using surgical clips, other than our case, stands hitherto unreported with the index case being the first report in literature.
Conclusions
The pseudoaneurysms of ICA around the base of the skull may have life-threatening presentations and pose peculiar diagnostic as well as therapeutic challenges. Managing a recurrent pseudoaneurysm following parent artery trapping may prove to be challenging. The patency of contralateral endovascular access routes, awareness of ECA collaterals, and flow dynamics around the circle of Willis are the critical issues for ensuring appropriate endovascular rescue therapy. With optimal hardware choice and careful maneuvering, contralateral access across the ACom A. is a feasible and safe approach for complete and lasting occlusion of pseudoaneurysm.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.