
Abstract
Purpose
This study aimed to determine the MRI features of sporadic/simple lymphoepithelial cyst (SLEC) of the parotid gland.
Methods
Ten patients (seven men, three women; mean age, 60 years; age range, 38–77 years) with histopathologically and clinically proven SLEC of the parotid gland who underwent MRI before surgical resection were enrolled in this study. No enrolled patient had HIV infection or Sjögren syndrome. MRI findings of SLEC were retrospectively assessed.
Results
We confirmed 10 SLECs larger than 10 mm with a mean maximum diameter of 26.6 mm (range, 12–42 mm). Nine patients (90%) had a single cyst, and one (10%) had a large cyst accompanied by small cysts (<10 mm) within the ipsilateral parotid gland. Eight SLECs (80%) were unilocular, and two (20%) were bilocular, with complete septa. Among seven SLECs (70%) with internal septa, five unilocular SLECs (50%) had incomplete septa. Six SLECs (60%) had eccentric cyst wall thickening, and five (50%) were surrounded by small solid nodules that were isointense relative to lymph node. On T1-weighted images, all cyst contents were homogeneously hyperintense relative to cerebrospinal fluid.
Conclusion
SLECs of the parotid gland are usually single unilocular lesions. Internal septa, eccentric cyst wall thickening, and small solid nodules surrounding the lesion were often observed. Cyst contents are always homogeneously hyperintense on T1-weighted images.
Introduction
Benign lymphoepithelial cyst (BLEC) is a relatively rare lesion that develops within lymphoid tissue. In the head and neck region, BLEC most commonly occurs in the lateral neck and parotid gland; lesions in the oral cavity are rare. The term “branchial cleft cyst” refers to lesions that can be considered synonymous with cervical BLEC.
Benign lymphoepithelial lesions have an affinity for the parotid gland and arise from heterotopic salivary epithelial rests or inclusions in the intra- or periparotid lymph nodes. 1 These lesions cover a spectrum ranging from BLEC to lymphoepithelial sialadenitis of Sjögren syndrome and both HIV-related and HIV-unrelated cystic lymphoid hyperplasia. 2 They present a common microscopic appearance characterized by epimyoepithelial islands and/or epithelium-lined cysts in a lymphoid stroma.
Lymphoepithelial sialadenitis is a benign salivary gland lesion often found in patients with Sjögren syndrome. The histologic hallmark of this lesion is a benign lymphocytic infiltrate characterized by parenchymal atrophy, ductal hyperplasia, and lymphocytic epitheliotropism. 3 Patients with Sjögren syndrome can initially present with multiple bilateral parotid cystic masses, which are usually considered as lymphoepithelial cysts (LECs). 4
In patients with HIV, most cystic lesions of the parotid glands are lymphoepithelial cystic lesions, which are described using various terms, including BLEC, benign lymphoepithelial lesion, AIDS-related lymphadenopathy, and cystic lymphoid hyperplasia. 5 As HIV became endemic, the incidence of BLEC of the parotid gland increased, reportedly occurring in 3%–6% and 1%–10% of HIV-positive adults and children, respectively. 6 The first clinical manifestation of HIV infection is often painless bilateral parotid enlargement from BLECs. Multiple bilateral cystic lesions of the parotid are common imaging findings for BLEC in patients with HIV infection. 5
Sporadic/simple LECs (SLECs) of the parotid gland have no association with underlying disease or with either Sjögren syndrome or HIV infection. 7 Several case reports have described CT and MRI features of SLECs,6,8,9 but to the best of our knowledge, no previous studies have examined the MRI features of SLECs in detail. Thus, in this study, we aimed to describe the MRI features of parotid SLECs and determine radiologic–pathologic correlations.
Methods
Patients
The present study was approved by the human research committee of the institutional review board of our hospital and complied with the guidelines of the Health Insurance Portability and Accountability Act of 1996 and the Declaration of Helsinki. Due to the retrospective nature of the study, the requirement for informed consent was waived. Using our hospital’s electronic medical records system, we searched for patients with histopathologically proven LEC of the parotid gland who underwent preoperative MRI and subsequent surgical resection between July 2004 and January 2018. The 10 patients thus identified (seven men, three women; mean age, 60 years; age range, 38–77 years) were enrolled in the study. All had presented with a chief complaint of a lump in the parotid region. All underwent surgery for removal of the LEC and surrounding normal parotid gland tissues. Preoperative blood tests for HIV screening were negative in nine patients. The remaining patients did not undergo preoperative screening for HIV infection, but clinical signs suggesting such an infection were not observed. No patient had the clinical manifestations of Sjögren syndrome.
Imaging technique
MRI was performed using a 1.5-T MRI system (Signa Excite Twin Speed; GE Healthcare, Milwaukee, WI, USA or Intera Achieva 1.5 T Pulsar; Philips Healthcare, Best, The Netherlands) in all patients. All transverse MRI images were obtained at a section thickness of 3–4 mm with 1 mm intersection gap. T2-weighted fast spin-echo (TR/TE, 4,000–5,710/90–97 ms; field of view, 20 × 20 cm), T1-weighted spin-echo (TR/TE, 500–779/9–15 ms; field of view, 20 × 20 cm) images were obtained in all patients. Diffusion-weighted short-tau inversion recovery single-shot spin-echo echo-planar (TR/TE/TI, 5,086–18,580/70–72/170–240 ms; field of view, 24 × 24–40 × 40 cm; b value, 0 and 1,000 s/mm2) images were obtained in seven patients. Gadolinium-enhanced fat-suppressed T1-weighted spin-echo (TR/TE, 630–719/9–15 ms; field of view, 20 × 20 cm) images were obtained in three patients.
CT imaging was performed using an 8-slice CT scanner (LightSpeed Ultra; GE Healthcare, Milwaukee, WI, USA) or a 16-slice CT scanner (LightSpeed 16; GE Healthcare, Milwaukee, WI, USA) in five patients. Axial unenhanced CT images were obtained and reconstructed at a section thickness of 2.5-mm without overlap.
Image assessment
Two radiologists with 23 and 9 years of post-training experience in head and neck imaging reviewed all images. The reviewers were blinded to all clinical information. Any disagreement between the reviewers was resolved through discussion to arrive at a consensus.
For the qualitative assessment, the reviewers identified the number and location of parotid cystic lesions. The parotid gland was divided into superficial and deep lobes based on the retromandibular vein. The superior and inferior poles were defined as the superior and inferior halves of the parotid gland, respectively. The lesions themselves were classified as either unilocular or multilocular and were qualitatively evaluated for the presence of complete or incomplete/interrupted septa, eccentric cyst wall thickening, small solid nodules surrounding the lesion that were isointense relative to lymph node, and background parotid gland atrophy. The heterogeneity of the cyst content was assessed using T1-, T2-, and diffusion-weighted images and was classified as either homogeneous or heterogeneous. The signal intensity of the cyst content relative to cerebrospinal fluid (CSF) on T1-, T2-, and diffusion-weighted images was assessed. Contrast enhancement of the cyst wall was assessed on contrast-enhanced T1-weighted images.
For the quantitative assessment, the maximum and minimum diameters of the largest lesion were measured, and the ratio of minimum to maximum diameter was calculated. In patients with eccentric cyst wall thickening, the maximum thickness of the wall was also measured. Apparent diffusion coefficient (ADC) values (× 10−3 mm2/s) on ADC maps and CT value (Hounsfield Unit) on unenhanced CT images were measured by placing a region of interest over the cystic lesions. The region of interest was placed as broadly as possible within the cyst content.
Histopathologic assessment
A pathologist with 11 years of post-training experience macroscopically and microscopically reviewed surgically resected specimens of parotid SLECs. The pathologist assessed the types of epithelium composing the cyst wall and the presence of ciliated columnar epithelium and stratified squamous epithelium. The absence or presence of internal septa was used to classify lesions as either unilocular or multilocular. Eccentric cyst wall thickening, intraparotid lymph nodes/lymphoid follicles surrounding the lesion, and background parotid gland atrophy were also assessed. In SLECs with eccentric cyst wall thickening, histologic characteristics of the cyst wall were also assessed. When the cyst contents were available for pathology evaluation, the major components of the cyst content were assessed. Based on a previous study which proposed a hypothesis of the developmental process of LEC of the parotid glands, our SLECs were classified into three histologic subtypes: type I, a cystic dilation of parotid gland ducts without fibrous capsules; type II, a partially encapsulated cystic lesion from the surrounding parotid parenchyma by fibrous capsules; type III, a completely encapsulated cystic lesion from the surrounding parotid parenchyma by fibrous capsules. 10
Results
MRI findings
Summary of imaging findings of sporadic/simple lymphoepithelial cyst of the parotid gland.
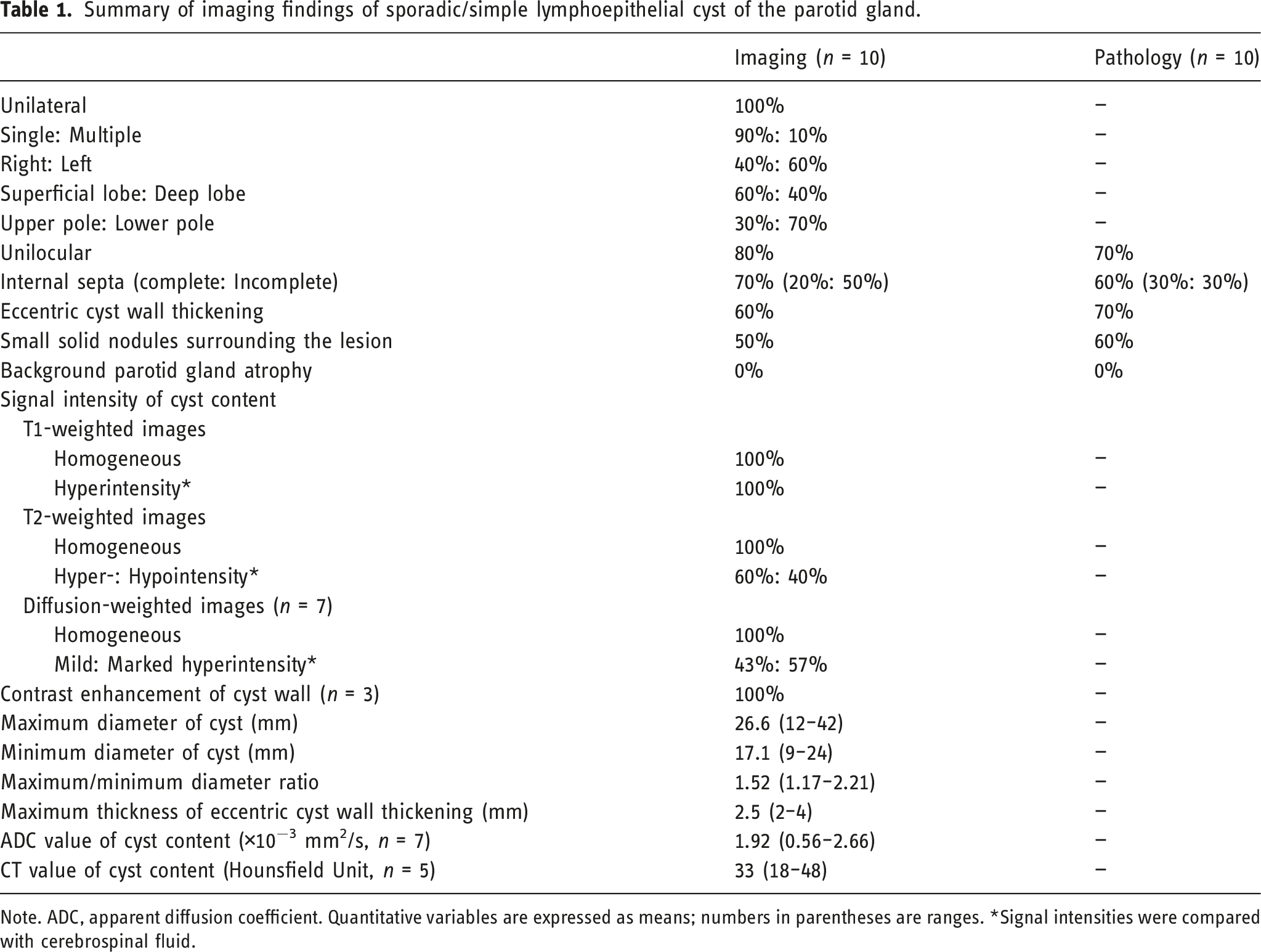
Note. ADC, apparent diffusion coefficient. Quantitative variables are expressed as means; numbers in parentheses are ranges. *Signal intensities were compared with cerebrospinal fluid.
Imaging findings of sporadic/simple lymphoepithelial cyst of the parotid gland.
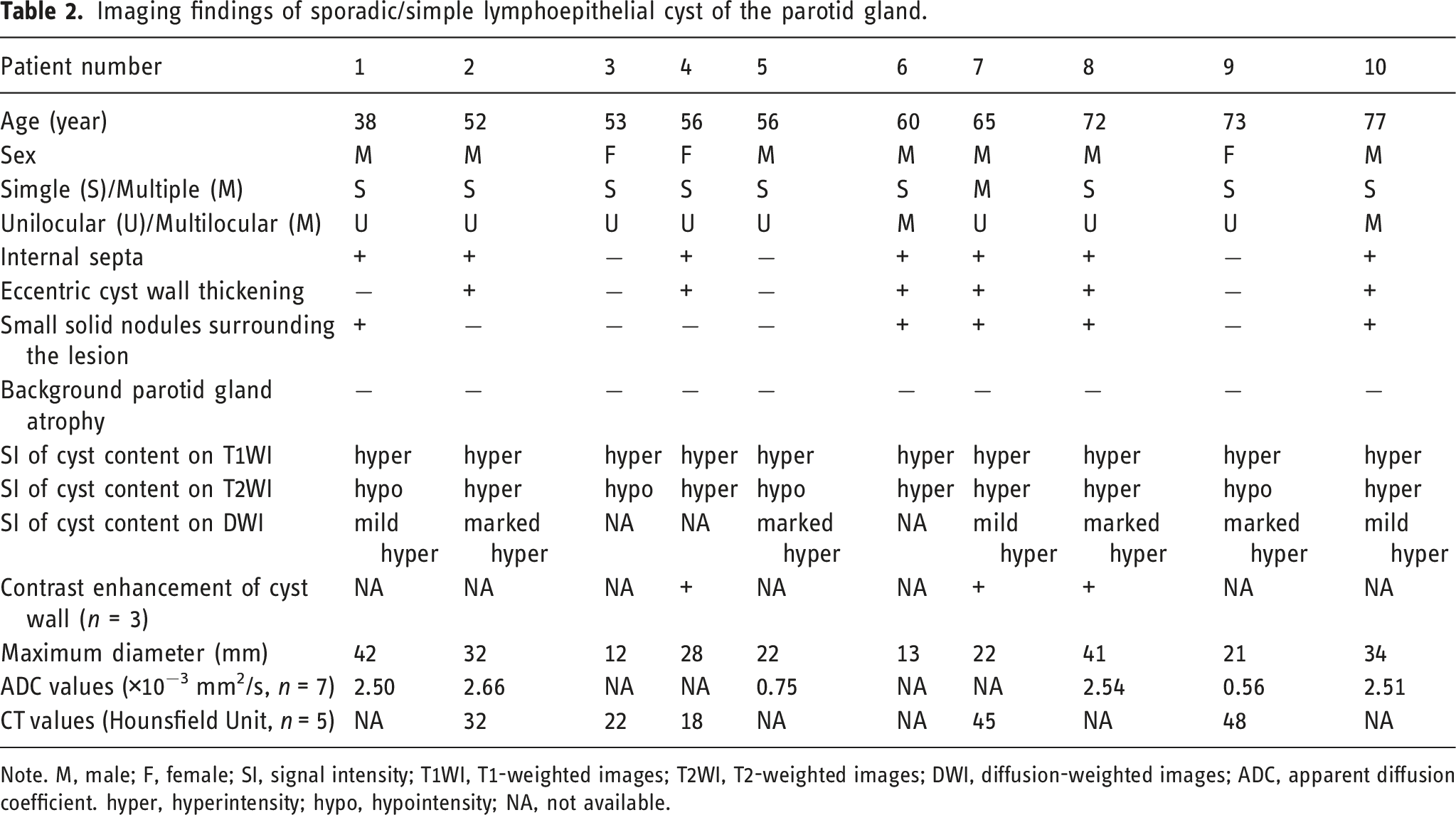
Note. M, male; F, female; SI, signal intensity; T1WI, T1-weighted images; T2WI, T2-weighted images; DWI, diffusion-weighted images; ADC, apparent diffusion coefficient. hyper, hyperintensity; hypo, hypointensity; NA, not available.
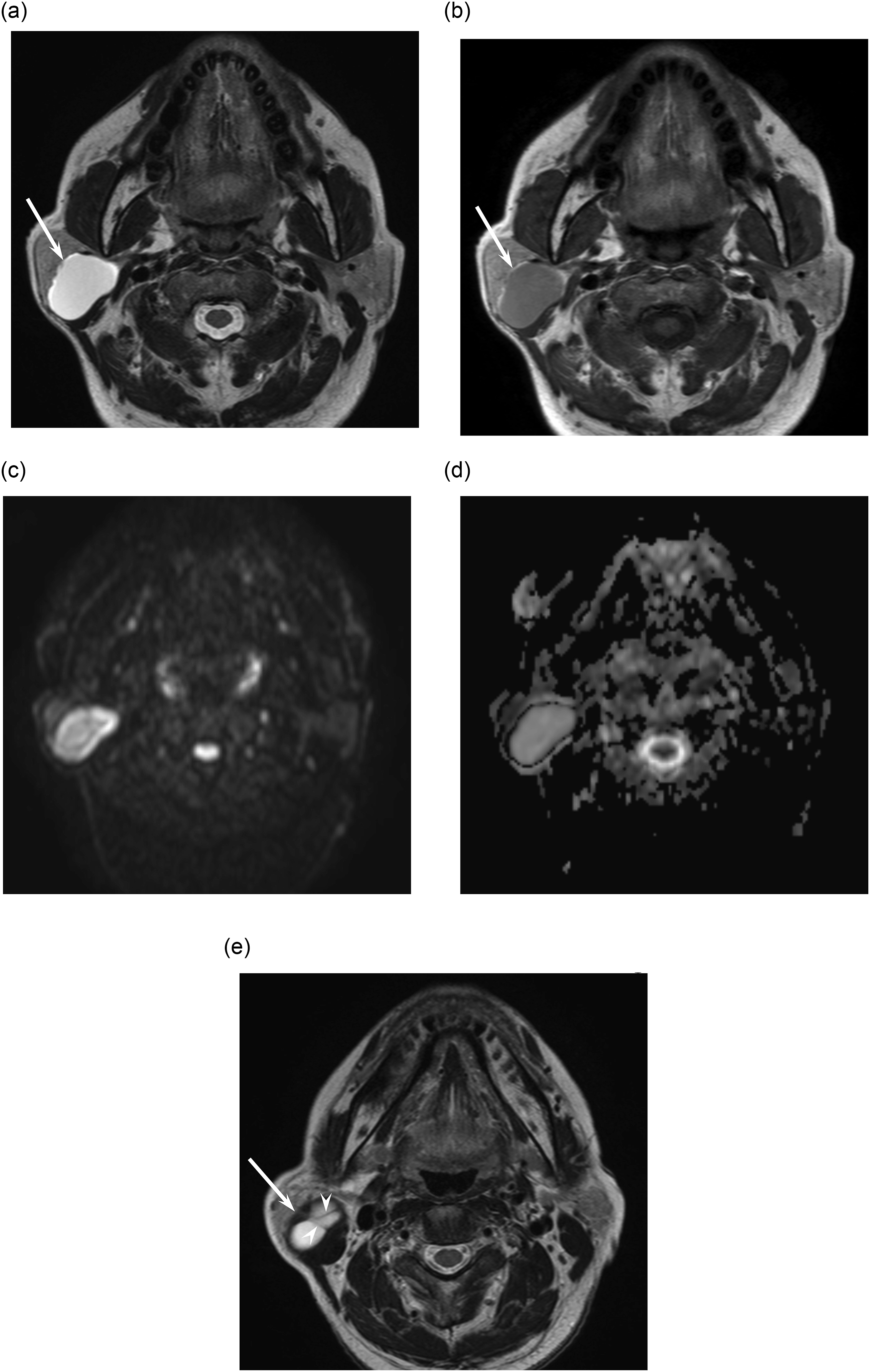
A 72-year-old man with sporadic/simple lymphoepithelial cyst of the right parotid gland (case 8). (a). T2-weighted image (TR/TE, 5,710/90 ms) shows a unilocular cystic lesion with hyperintensity relative to cerebrospinal fluid (arrow). (b). T1-weighted image (TR/TE, 779/15 ms) shows hyperintense cyst content relative to cerebrospinal fluid (arrow). (c). Diffusion-weighted image (TR/TE, 18,580/70 ms) shows markedly hyperintense cyst content (arrow). (d). ADC map shows high ADC value (2.54 × 10−3 mm2/s) (arrow). (e). T2-weighted image (TR/TE, 5,710/90 ms) shows eccentric cyst wall thickening (arrow) and internal septa (arrowheads).
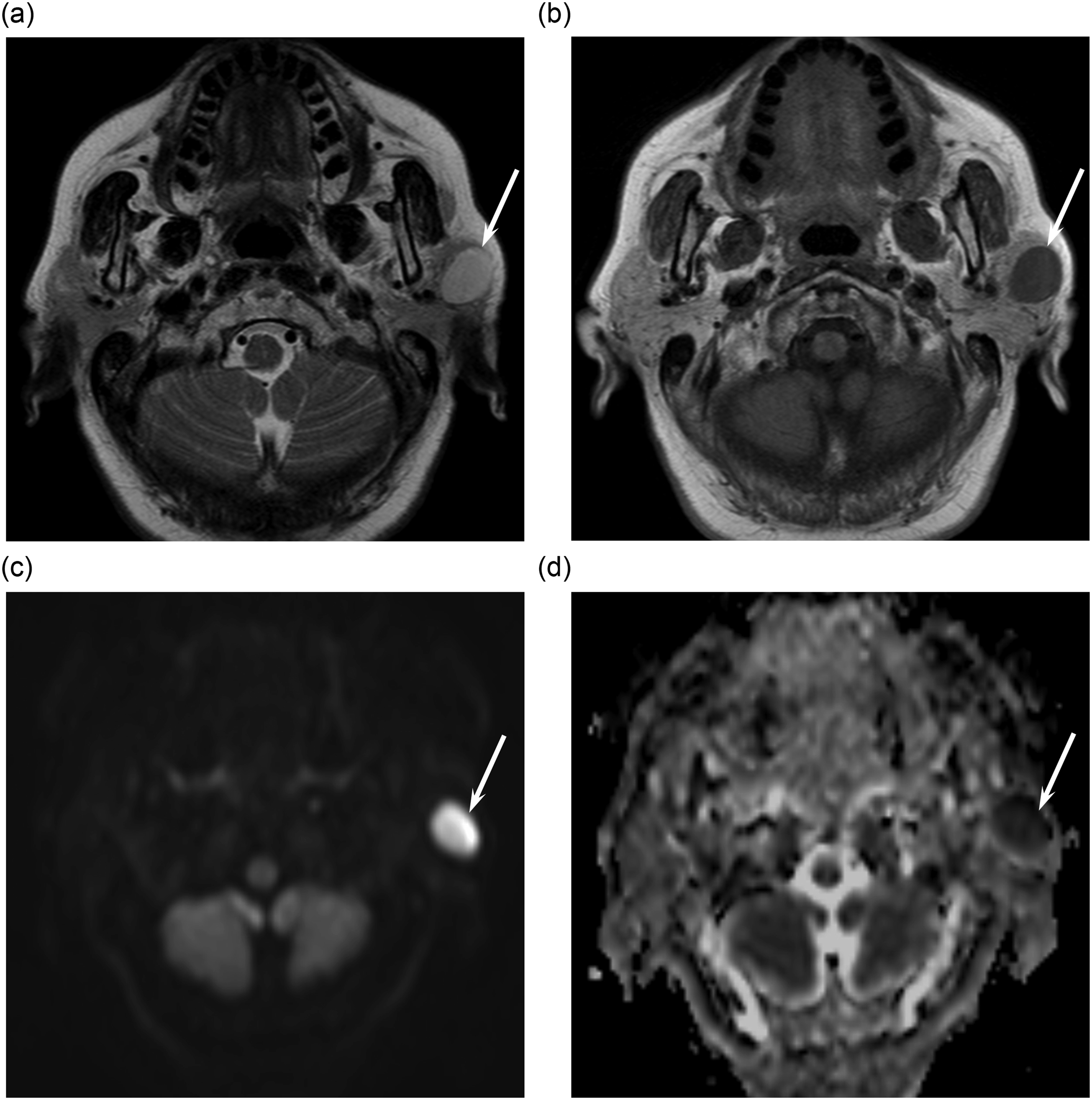
A 73-year-old woman with sporadic/simple lymphoepithelial cyst of the left parotid gland (case 9). (a). T2-weighted image (TR/TE, 4,102/90 ms) shows a unilocular cystic lesion with slight hypointensity relative to cerebrospinal fluid (arrow). (b). T1-weighted image (TR/TE, 719/9 ms) shows slightly hyperintense cyst content relative to cerebrospinal fluid (arrow). (c). Diffusion-weighted image (TR/TE, 5,086/72 ms) shows markedly hyperintense cyst content (arrow). (d). ADC map shows low ADC value (0.56 × 10−3 mm2/s) (arrow).
The mean maximum and minimum diameters of the cysts were 26.6 mm (range, 12–42 mm) and 17.1 mm (range, 9–24 mm), respectively. Thus, the mean ratio of minimum to maximum diameter was 1.52 (range, 1.17–2.21 mm). In six patients with eccentric cyst wall thickening, the mean maximum thickness of the cyst wall was 2.5 mm (range, 2–4 mm). In six patients whose ADC values were available, the mean ADC value of the cyst content was 1.92 × 10−3 mm2/s (range, 0.56–2.66 × 10−3 mm2/s). Among them, four SLECs had extremely high ADC values (2.50, 2.51, 2.54, and 2.66 × 10−3 mm2/s) and the remaining two SLECs had low ADC values (0.56 and 0.75 × 10−3 mm2/s). In five patients who underwent CT, the mean CT value of the cyst content was 33 HU (range, 18–48 HU).
Histopathologic findings
Pathologic findings of sporadic/simple lymphoepithelial cyst of the parotid gland.
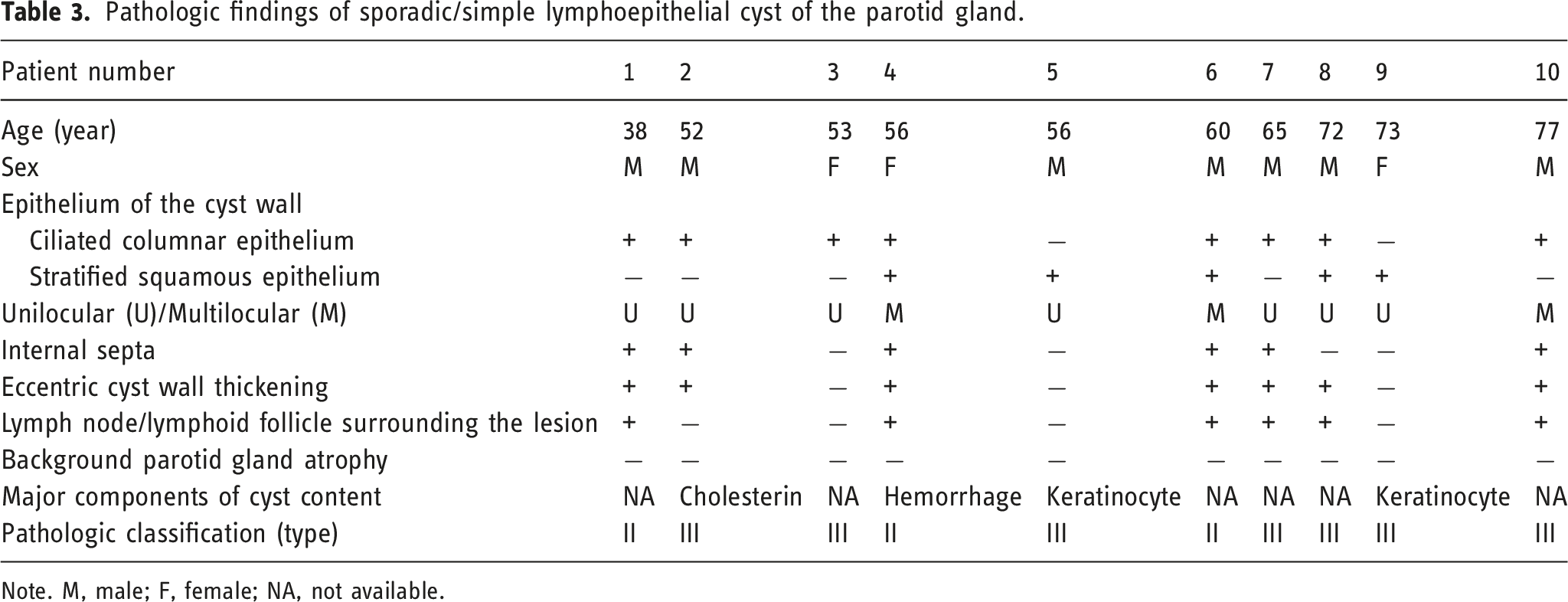
Note. M, male; F, female; NA, not available.
Discussion
Our investigation of MRI images revealed that the typical MRI finding of parotid SLECs was a single unilocular cystic lesion. Complete or incomplete internal septa, eccentric cyst wall thickening, and small solid nodules surrounding the lesion that appeared isointense relative to lymph node were also often observed. Background parotid gland atrophy was not observed. Cyst contents were always homogeneous in signal intensity, with hyperintensity, hyper- or hypointensity, and mild or marked hyperintensity on T1-, T2-, and diffusion-weighted images, respectively.
However, some discrepancies existed between image and histologic assessments. In case 9, the SLEC was radiologically unilocular, but histologically multilocular. It is because the histopathologically confirmed thin septa could not be detected on MRI image due to the limited spatial resolution of MRI. In case 8, internal septa were radiologically present, but histologically absent. Fold-like structures caused by extensive infiltration of the cyst wall by inflammatory cells such as lymphocytes were confirmed histologically in the latter case. The fold-like structures were regarded as incomplete septa on MRI assessment; however, they were classified as eccentric cyst wall thickening on pathologic assessment. In case 1, the histologically confirmed eccentric cyst wall thickening could not be identified on MRI assessment possibly due to the limited spatial resolution of MRI.
A previous study reported that type II SLECs had lymphoid infiltration forming incomplete lymphoid follicles, whereas type III lesions had more completely and functionally arranged lymphoid follicles. Therefore, lymphocytic infiltration and proliferation of secondary lymphoid follicles would be an important cause of eccentric cyst wall thickening; however, differentiating between type II and type III lesions radiologically would be most difficult. Alternatively, the radiological small solid nodules corresponded to histological intraparotid lymph nodes/lymphoid follicles. Various degrees of inflammatory cell infiltration or lymphoid follicle formation are typically observed within the cyst wall of an LEC; therefore, sialadenitis and inflammatory cell infiltration around salivary gland ducts are thought to be the underlying cause of LEC. Swollen intraparotid lymph nodes/lymphoid follicles around LECs could be considered to be reactive lymphadenopathy or lymphadenitis caused by inflammation.
In other published reports, inflammatory cells such as foamy macrophages, lymphocytes, and plasma cells, epithelial cells, and high-protein material have been identified as LEC content.8,11–13 Hemorrhagic, keratinized, and infectious content have also been reported.6,9,14 In this study, hyperintensity on T1-weighted images suggests high cellular density, high protein density, or hemorrhage as the cyst content. Two SLECs in this study (case 5 and 9) were markedly hyperintense on diffusion-weighted images, with extremely low ADC values because keratinocytes formed a major part of the cyst content. However, in the remaining four SLECs with extremely high ADC values, hyperintensity on diffusion-weighted images might be caused by T2 shine-through effects.
The differential diagnosis of SLEC includes non-neoplastic and neoplastic cystic lesions of the parotid gland. Non-neoplastic cystic lesions of the parotid gland fall into two categories: congenital or acquired cystic lesions (first branchial cleft cyst, lymphatic malformation, LEC, salivary duct cyst, pseudocyst) and inflammatory or infectious disease (sialodochitis fibrinosa, hydatid cyst, intraglandular lymphadenitis, parotid abscess). 7 Because first branchial cleft cyst, lymphatic malformation, and salivary duct cyst typically contain thin-walled cysts, eccentric cyst wall thickening plays a key role in making a correct diagnosis of SLEC. In Sjögren syndrome and HIV infection, lymphoepithelial lesions are usually multiple and bilateral and can be purely cystic, cystic and solid combined, or purely solid. Neoplastic cystic lesions of the parotid gland include Warthin tumor, pleomorphic adenoma, basal cell adenoma, and malignant salivary gland tumors such as mucoepidermoid carcinoma, adenoid cystic carcinoma, and acinic cell carcinoma. 15 Cystic parotid tumors usually contain a mixture of solid and cystic components, but SLECs are typically unilocular cystic lesions without solid components. Therefore, differentiating cystic parotid tumors from SLECs using MRI is usually easy. However, Warthin tumor, 16 basal cell adenoma, 17 and acinic cell carcinoma 18 can produce purely cystic lesions with hyperintense cyst content on T1-weighted images; differentiating them from SLECs can be difficult.
According to results of the present study, eccentric cyst wall thickening within parotid cystic lesions could be caused by benign SLECs and did not always indicate cystic tumors. However, the presence of mass-forming solid components and mural nodules would suggest neoplastic cystic lesions. Although the treatment strategy of SLECs of the parotid gland is still controversial, a careful observation is necessary during the follow-up periods because of the presence of malignant transformation of lymphoepithelial lesion of the parotid gland into lymphoma or carcinoma. 1 The usefulness of fine needle aspiration biopsy for cystic benign lymphoepithelial lesion has been reported 19 ; therefore, fine needle aspiration biopsy may be considered if eccentric cyst wall thickening is observed within parotid cystic lesions.
Our study has several limitations. First, it reports a small cohort recruited at a single institution. Second, the retrospective nature of the study means that imaging equipment and protocols were not standardized. Third, not all patients underwent diffusion-weighted and contrast-enhanced MRI.
In conclusion, SLECs of the parotid gland usually develop as single unilocular cystic lesions. Internal septa, eccentric cyst wall thickening, and small solid nodules surrounding the lesion are often observed. Eccentric cyst wall thickening correlates with lymphocytic infiltration and proliferation of secondary lymphoid follicles. Small solid nodules surrounding the lesion correlate with swollen intraparotid lymph nodes/lymphoid follicles. Cyst content is always homogeneously hyperintense relative to CSF on T1- and diffusion-weighted images, reflecting high cellular density, high protein density, or hemorrhage. These imaging characteristics help to differentiate SLECs from other non-neoplastic and neoplastic cystic lesions in the parotid gland.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.