
Abstract
Background
Arterial calcification is commonly found in patients with cerebrovascular disease and may negatively affect outcomes following endovascular thrombectomy (EVT) for acute ischemic stroke (AIS). This systematic review and meta-analysis aimed to evaluate the impact of intracranial or aortic arch calcification on procedural success and functional outcomes in AIS patients undergoing anterior circulation EVT.
Methods
We systematically searched the PubMed, EMBASE, and Cochrane databases to identify studies comparing EVT outcomes between AIS patients with and without arterial calcification. Outcomes assessed included first-pass effect (FPE), successful reperfusion at the end of the procedure, modified Rankin scale (mRS), mortality, and symptomatic intracerebral hemorrhage (sICH). Risk ratios (RRs) with 95% confidence intervals (CIs) were pooled using random effects models, with heterogeneity evaluated with I2 statistics.
Results
A total of six observational studies were included, with a total of 3834 patients (2303 with calcification and 1531 controls). Arterial calcification was associated with a lower chance of achieving FPE (RR: 0.50, 95% CI: 0.36–0.69, p < 0.001) and successful reperfusion (RR: 0.90, 95% CI: 0.86–0.94, p < 0.001). Patients with calcification had a greater risk of poor outcome (mRS 3–6) (RR: 1.29, 95% CI: 1.16–1.43, p < 0.001), mortality (RR: 1.51, 95% CI: 1.14–2.00, p < 0.001), and sICH (RR: 1.29, 95% CI: 1.16–1.43, p < 0.001). Heterogeneity was low, with I2 ≤ 34%.
Conclusion
Arterial calcification may be indicative of advanced vascular disease, potentially leading to diminished technical success and worse functional outcomes following EVT for AIS. These findings underscore that vascular calcification acts as an associative marker of procedural complexity and advanced vascular disease in EVT candidates.
Introduction
Endovascular thrombectomy (EVT) is the standard of care for patients with acute ischemic stroke due to large vessel occlusion and has been shown to significantly improve functional outcomes when successful reperfusion is achieved. 1 However, despite technical success in recanalization, a substantial proportion of patients fail to achieve favorable neurological recovery or independence at follow-up. 2 This discrepancy between technical success and clinical recovery has prompted growing interest in identifying patient-level and procedural factors that may influence EVT effectiveness and prognosis.
Among the many factors investigated to explain this variability, arterial calcification—both intracranial and extracranial—has emerged as a potential modifier of EVT success.3,4 Intracranial artery calcification (ICAC), frequently observed on non-contrast CT, is a common finding in this population and may reflect underlying atherosclerosis and increased arterial stiffness, potentially affecting hemodynamics and vascular compliance.1,5 Some studies suggest that symptomatic ICAC, especially when located at or near the site of occlusion, may impair device performance or clot retrieval and has been linked to reduced recanalization and poorer outcomes.6,7 Additionally, a U-shaped association between calcification burden and procedural success has been described, suggesting that both insufficient and excessive calcification may be associated with outcomes after EVT. 1
Calcifications in extracranial arteries, particularly the aortic arch and extracranial carotid, have also been associated with adverse outcomes. These include a reduced likelihood of functional independence, increased mortality, and a greater risk of symptomatic intracranial hemorrhage following EVT.8,9 These extracranial calcifications may lead to technical difficulties during catheter navigation, limit access to target vessels, reduce thrombus engagement, and increase the risk of vascular injury or dissection. 10 Furthermore, patients with significant extracranial calcification may present with a more advanced atherosclerotic burden and systemic vascular disease, which in itself may be an independent predictor of poor neurological recovery and increased mortality. 11
A recent study by Omura et al. 12 highlighted the negative impact of intracranial calcification on EVT outcomes. However, their analysis was strictly restricted to intracranial lesions and a limited set of clinical endpoints. This leaves a critical gap in understanding the effects of the entire vascular pathway to the brain. Incorporating extracranial and aortic arch calcifications is essential, as these lesions impose distinct mechanical challenges during catheter navigation. Furthermore, there is a crucial need to establish a comprehensive procedural safety profile by evaluating vital endpoints—specifically the First-Pass Effect (FPE), 90-day mortality, and symptomatic intracranial hemorrhage (sICH)—while leveraging data from a significantly larger cohort.
Despite these observations, existing evidence remains inconsistent due to heterogeneity in study designs, imaging protocols, calcification definitions, and outcome reporting.1,13 This systematic review and meta-analysis aims to assess the impact and prognostic value of arterial calcification on outcomes following EVT, comparing patients with intracranial and/or aortic arch calcifications to those with absent or considered insignificant calcification.
Methods
This systematic review and meta-analysis was conducted following the Cochrane Handbook for Systematic Reviews of Interventions and reported in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 14 The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420251078921.
Eligibility criteria
We included randomized controlled and cohort studies, both prospective and retrospective, evaluating adult patients >18 years old, diagnosed with acute ischemic stroke (AIS) who underwent EVT and had assessments for intracranial and/or extracranial artery calcification. Eligible studies compared outcomes between patients with the presence of calcification and those with an absence or considered insignificant calcification. We excluded case reports, reviews, editorials, studies not available in English and studies not reporting clinical or procedural outcomes.
Search strategy and study selection
A comprehensive literature search was carried out in three electronic databases, PubMed/MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL), from inception to May 2025. The search strategy used controlled vocabulary (e.g., MeSH terms) and keywords such as “calcification,” AND “stroke,” AND “endovascular,” AND “thrombectomy.” The complete search strategy is available in the Supplemental Material. The retrieved data were imported into Rayyan for systematic screening. Two reviewers independently screened all titles, abstracts, and full texts on the basis of predefined inclusion criteria, with disagreements resolved through discussion or consultation with a third reviewer.
Data extraction and risk of bias assessment
From each included study, the following data were extracted: first author, year of publication, country, study design, sample size, participant characteristics (mean or median age and baseline National Institutes of Health Stroke Scale (NIHSS), sex distribution), vascular risk factors (e.g., hypertension, diabetes), imaging modality used to assess or identify calcification (e.g., computed tomography (CT) and Chest X-Ray (CXR)), calcification location (intracranial and/or extracranial) and definition, and follow-up duration. Clinical outcomes included functional independence evaluated by the modified Rankin scale, mortality, and symptomatic intracranial hemorrhage (sICH). Procedural outcomes included first-pass effect (FPE) and successful reperfusion (TICI 2b–3) at the end of the procedure. The risk of bias was assessed using the ROBINS-I tool for nonrandomized studies, applied independently by two reviewers.
Outcomes, definitions, and subgroup analyses
Outcomes were analyzed in three domains: procedural (FPE and successful reperfusion), safety (mortality by 90 days and sICH), and functional (mRS 0–2 and mRS 3–6 at 90 days). We performed subgroup analyses to compare the effect of calcification location—intracranial artery calcification (ICAC) versus aortic arch/extracranial calcification—on each outcome.
Statistical analysis
Meta-analyses were conducted using random effects models to account for interstudy variability. Effect estimates were pooled as unadjusted risk ratios (RRs) with 95% confidence intervals (CIs) if outcomes were binary. Heterogeneity was quantified using the I2 statistic and categorized as low (<40%), moderate (40–60%), or high (>60%). When heterogeneity was high, sensitivity analyses were performed by sequentially excluding each study to evaluate robustness (leave-one-out analysis). Subgroup differences according to the artery calcified were tested using interaction p-values, considered significant when p < 0.05. Analyses were performed in R (version 4.5.2) using the meta package, employing both Mantel-Haenszel and Restricted-Maximum-Likelihood methods.
Results
Study selection and characteristics
The systematic search identified 584 records (PubMed: 143, Embase: 433, Cochrane: 8). After removal of duplicates and screening of titles/abstracts, 27 full-text articles were assessed for eligibility, of which 6 studies met the inclusion criteria (Figure 1), encompassing 3834 patients who underwent EVT for AIS. The included studies were conducted across South Korea (n = 2), the USA (n = 2), the Netherlands (n = 1) and Spain (n = 1) and included five retrospective cohorts and one prospective registry. Sample sizes ranged from 86 to 418 patients, with the largest study
15
contributing 2701 patients and the smallest
1
including 86. Figure 1 shows the PRISMA flow diagram detailing the study selection process, including the number of records identified, screened, assessed for eligibility, and included in the final meta-analysis. 2020 PRISMA flow diagram.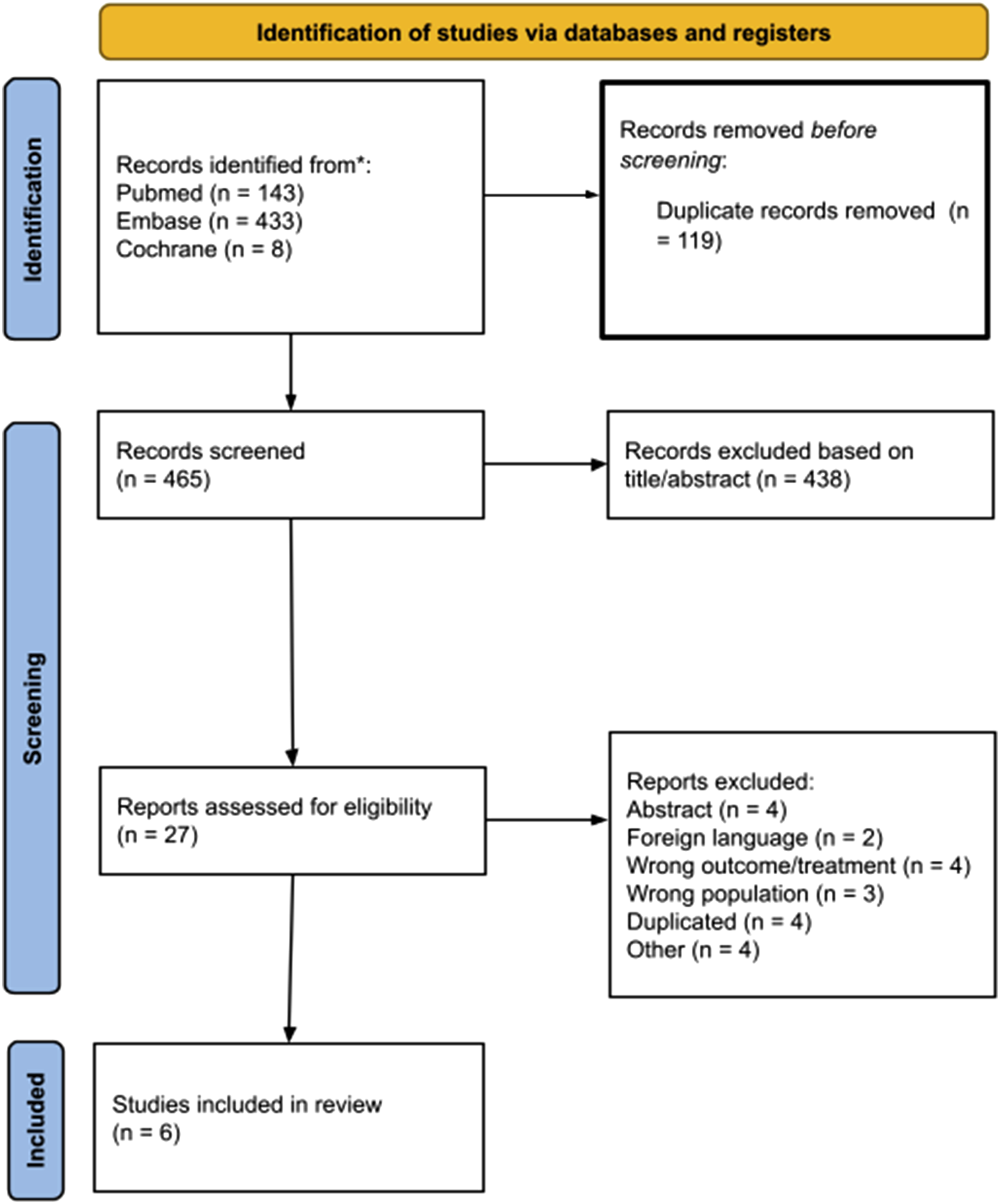
Baseline characteristics across studies.
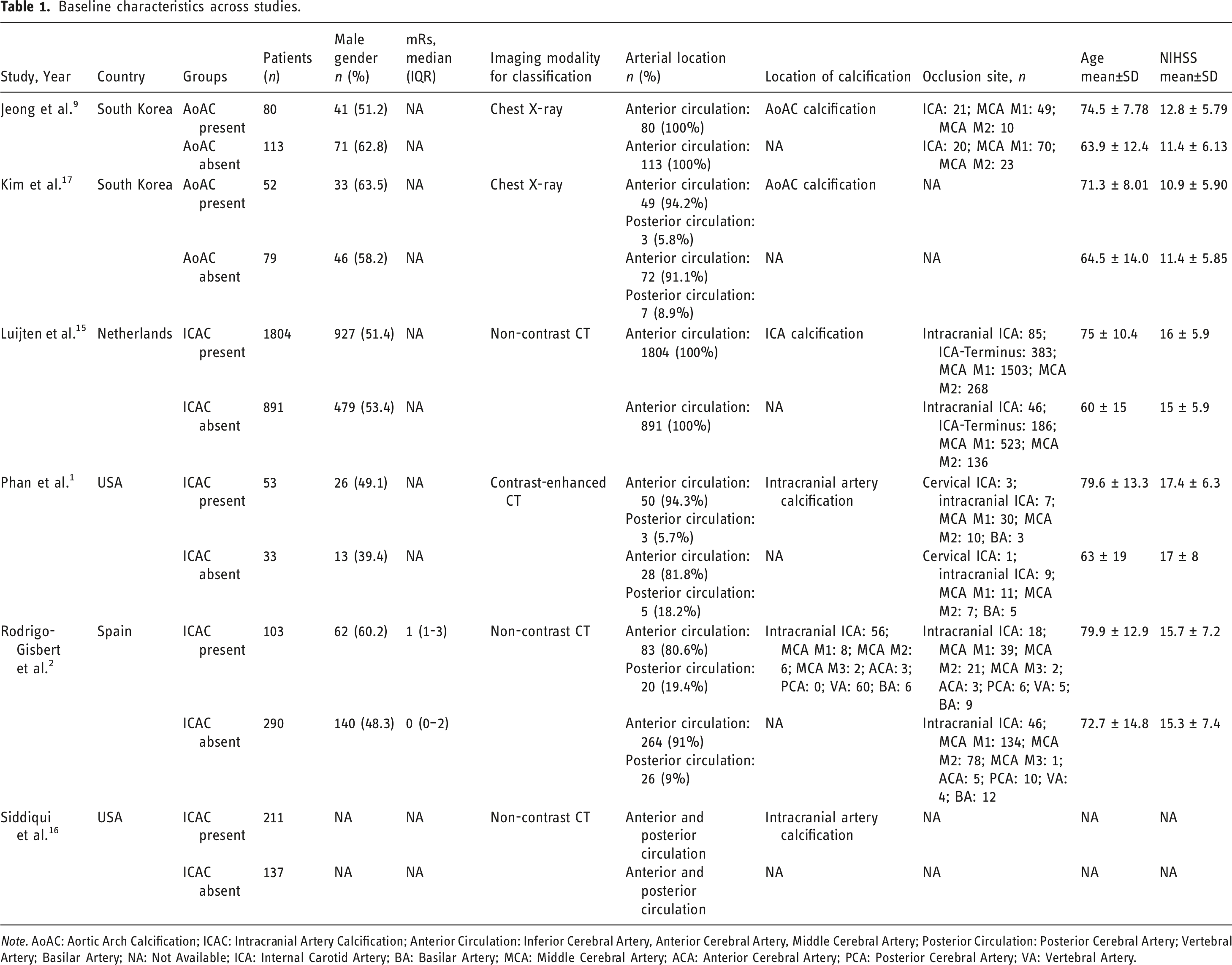
Note. AoAC: Aortic Arch Calcification; ICAC: Intracranial Artery Calcification; Anterior Circulation: Inferior Cerebral Artery, Anterior Cerebral Artery, Middle Cerebral Artery; Posterior Circulation: Posterior Cerebral Artery; Vertebral Artery; Basilar Artery; NA: Not Available; ICA: Internal Carotid Artery; BA: Basilar Artery; MCA: Middle Cerebral Artery; ACA: Anterior Cerebral Artery; PCA: Posterior Cerebral Artery; VA: Vertebral Artery.
Pooled analysis of included studies
Procedural outcomes
First-pass effect (FPE)
First-pass successful recanalization (mTICI 2b-3) was reported by three studies comprising 672 patients. Unadjusted pooled analysis demonstrated that arterial calcification reduced the likelihood of achieving first-pass successful recanalization (mTICI 2b-3) by 50% compared to controls (RR 0.50; 95% CI 0.36–0.69; p < 0.001; I
2
= 0%; Figure 2(A)). The effect was consistent across studies, with the largest reduction observed by Jeong et al. (RR 0.39; 95% CI 0.24–0.64). Meta-analysis of observational study data: forest plot depicting the procedural outcomes of first-pass effect (A) and successful reperfusion at the end of the procedure (B) in patients with AIS who underwent EVT with or without arterial calcification.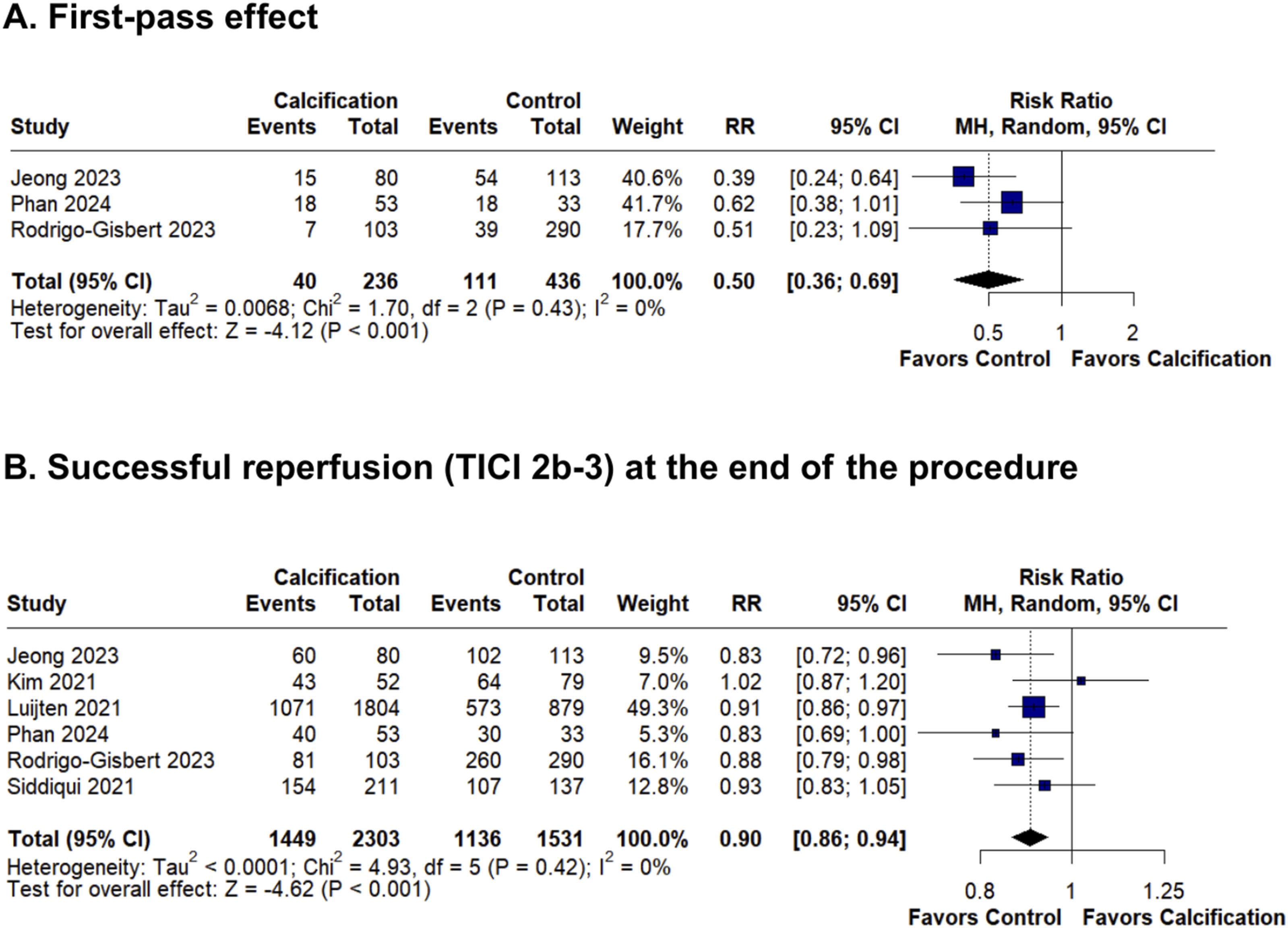
Successful reperfusion (TICI 2b-3) at the end of the procedure
Pooled analysis of all six studies including 3834 patients revealed that arterial calcification was associated with a 10% lower probability of achieving successful reperfusion (RR 0.90; 95% CI 0.86–0.94; p < 0.001; I2 = 0%; Figure 2(B)).
Safety outcomes
Mortality at 90 days
Two studies reported the outcome of mortality, comprising 457 patients, showing that arterial calcification was associated with a 51% higher mortality risk (RR 1.51; 95% CI 1.14–2.00; p < 0.001; I
2
= 0%; Figure 3(A)), driven by Rodrigo-Gisbert et al. (RR 1.53; 95% CI 1.13–2.06). Meta-analysis of observational study data: forest plot depicting the safety outcomes of mortality (A) and sICH (B) in patients with AIS who underwent EVT with or without arterial calcification.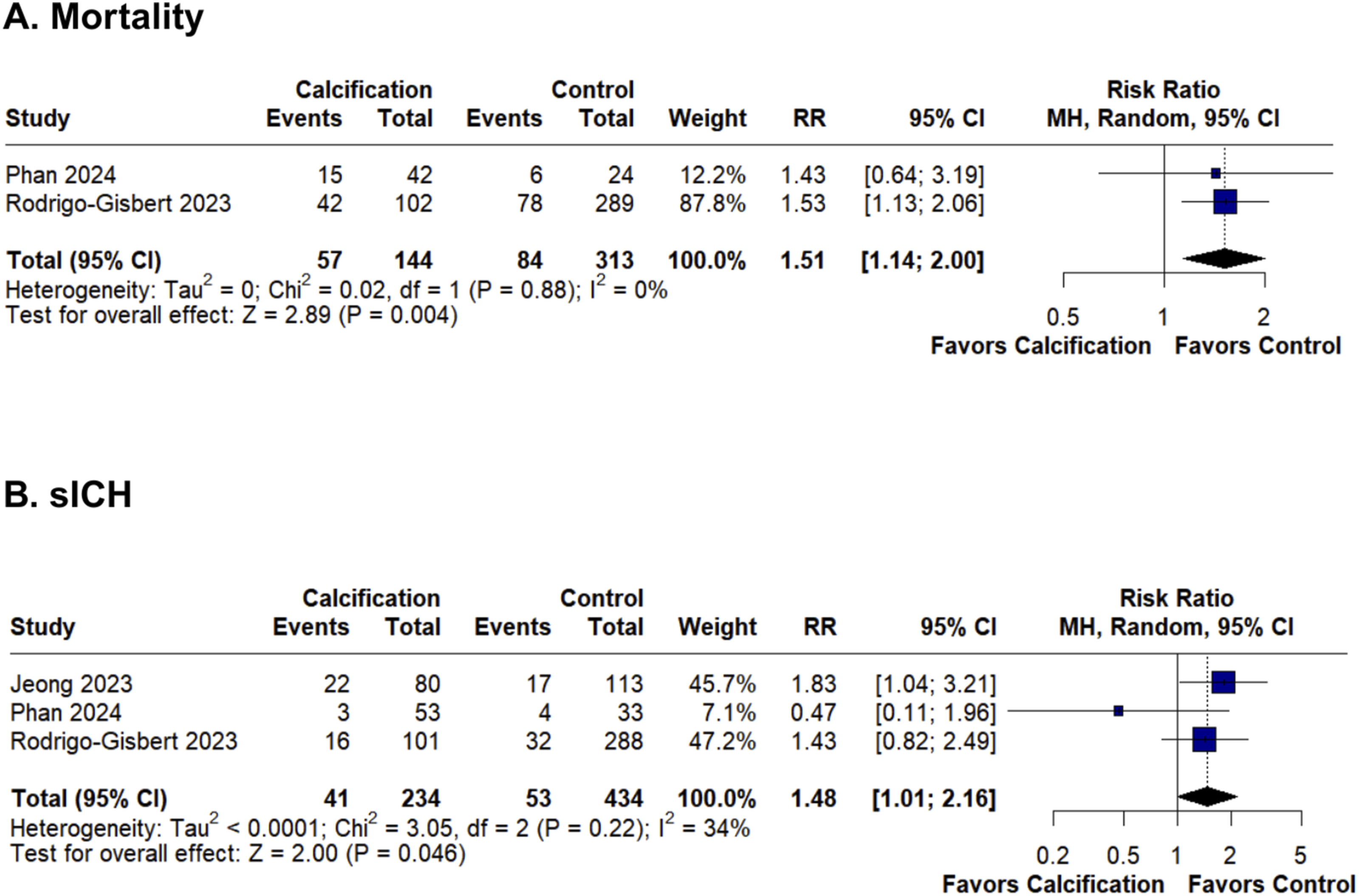
Symptomatic intracranial hemorrhage (sICH)
Three studies reported symptomatic intracranial hemorrhage, including 668 patients. Pooled analysis indicated that calcification was associated with a 45% greater risk of sICH (RR 1.45; 95% CI 1.01–2.16; p = 0.046; I2 = 34%; Figure 3(B)). This effect was driven by Jeong et al. (RR 1.83; 95% CI 1.04–3.21), whereas Rodrigo-Gisbert et al. reported a nonsignificant trend (RR 1.43; 95% CI 0.82–2.49).
Functional outcomes
mRS 0–2 at 90 days
Five studies comprising 1252 patients reported mRS 0–2 at 90 days, revealing that calcification reduced the probability of functional independence by 24% (RR 0.77; 95% CI 0.67–0.88; p < 0.001; I
2
= 22%; Figure 4(A)). The association was strongest in larger studies (Luijten et al.: RR 0.77; Rodrigo-Gisbert et al.: RR 0.59). Meta-analysis of observational study data: forest plot depicting the functional outcomes in patients with AIS who underwent EVT with or without arterial calcification.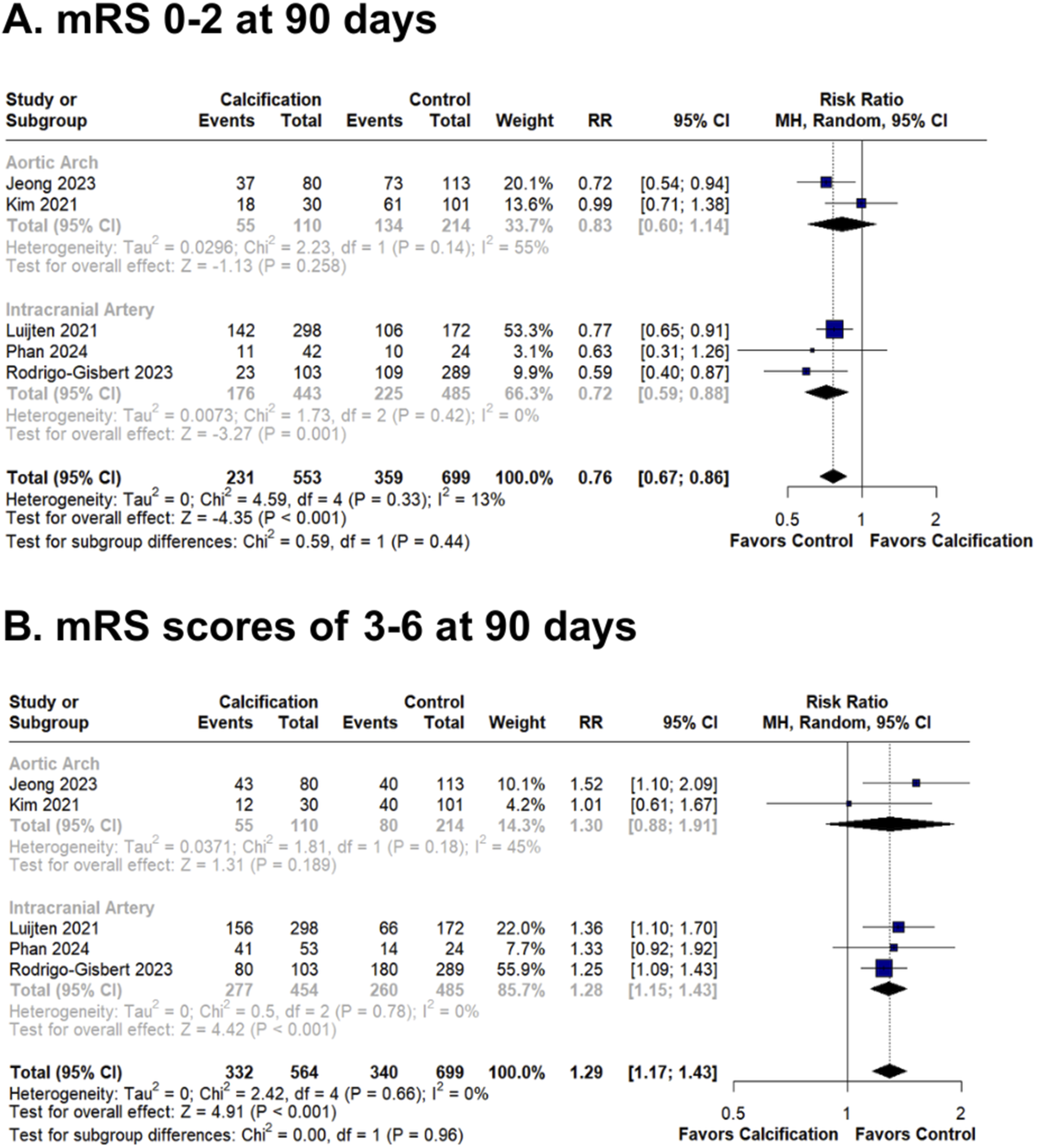
mRS 3–6 at 90 days
The same five studies reported mRS 3–6 at 90 days, with a pooled total of 1252 patients, demonstrating that calcification increased the risk of poor outcomes (mRS 3–6) by 29% (RR 1.29; 95% CI 1.16–1.43; p < 0.001; I 2 = 0%; Figure 4(b)). Jeong et al. reported the highest risk (RR 1.52; 95% CI 1.10–2.09), whereas Rodrigo-Gisbert et al. contributed the most weight (55.1%).
Subgroup analysis
We performed subgroup analyses to compare the impact of aortic arch calcification alone and intracranial calcification across procedural, safety, and functional outcomes. For first-pass effect (FPE), both aortic arch (RR 0.59; p = 0.011; Figure S1) and intracranial (RR 0.50; p < 0.001) calcifications were associated with reduced success. The difference between subgroups was not statistically significant (p = 0.22; Figure S1). Successful reperfusion at the end of the procedure (TICI 2b–3) was negatively affected by intracranial calcification (RR 0.89; p < 0.001; I2 = 0%), whereas aortic arch calcification had no significant effect (RR 0.94; p = 0.656; I2 = 82%) and subgroup interaction was not significant (p = 0.67; Figure S2).
For symptomatic intracranial hemorrhage (sICH), aortic arch calcification increased the risk (RR 1.83; p = 0.036; I2 = 0%), while intracranial calcification had a neutral effect (RR 1.00; p = 1.000; I2 = 51%). No significant difference was observed between subgroups (p = 0.31; Figure S3). Mortality was significantly higher in the intracranial calcification subgroup (RR 1.51; p = 0.004; I2 = 0%; Figure S4), and data for aortic arch calcification were not available. In terms of functional outcomes, intracranial calcification reduced the likelihood of achieving mRS 0–2 (RR 0.72; p = 0.001; I2 = 0%; Figure S5) and increased the likelihood of poor outcomes (mRS 3–6: RR 1.28; p < 0.001; I2 = 0%; Figure S6). Aortic arch calcification trended similarly but did not reach statistical significance for either mRS 0–2 (RR 0.83; p = 0.258; I2 = 55%; Figure S5) or mRS 3–6 (RR 1.30; p = 0.189; I2 = 45%; Figure S6). No subgroup differences were detected (p ≥ 0.44 for both).
Collectively, these findings highlight that intracranial calcification is consistently associated with worse outcomes, whereas aortic arch calcification shows suggestive but less consistent effects. Subgroup comparisons did not reveal statistically significant interactions according to calcification location across outcomes. We acknowledge that an I2 of 0% across most outcomes indicates the absence of statistical heterogeneity but does not rule out clinical or methodological heterogeneity arising from differing imaging protocols.
Risk of bias assessment
The risk of bias was evaluated using the ROBINS-I tool, and overall, the methodological quality of the included studies was considered reasonable for observational research. Most studies were rated as having a moderate risk of bias, mainly due to inherent limitations of retrospective designs and some residual confounding. However, strengths across studies included clear exposure classification, standardized EVT protocols, and minimal missing data, which helped reduce bias in several domains. Outcome measurement bias was generally moderate, mostly due to the nonblinded assessment of functional outcomes. Importantly, Luijten et al.
15
was rated as having an overall low risk of bias because of its prospective design, blinded imaging assessments, and comprehensive adjustment for confounders. Only one study
1
was rated as having a serious risk of bias, primarily due to confounding and outcome assessment concerns (Figure 5). ROBINS-I summary plot—risk of bias of observational studies.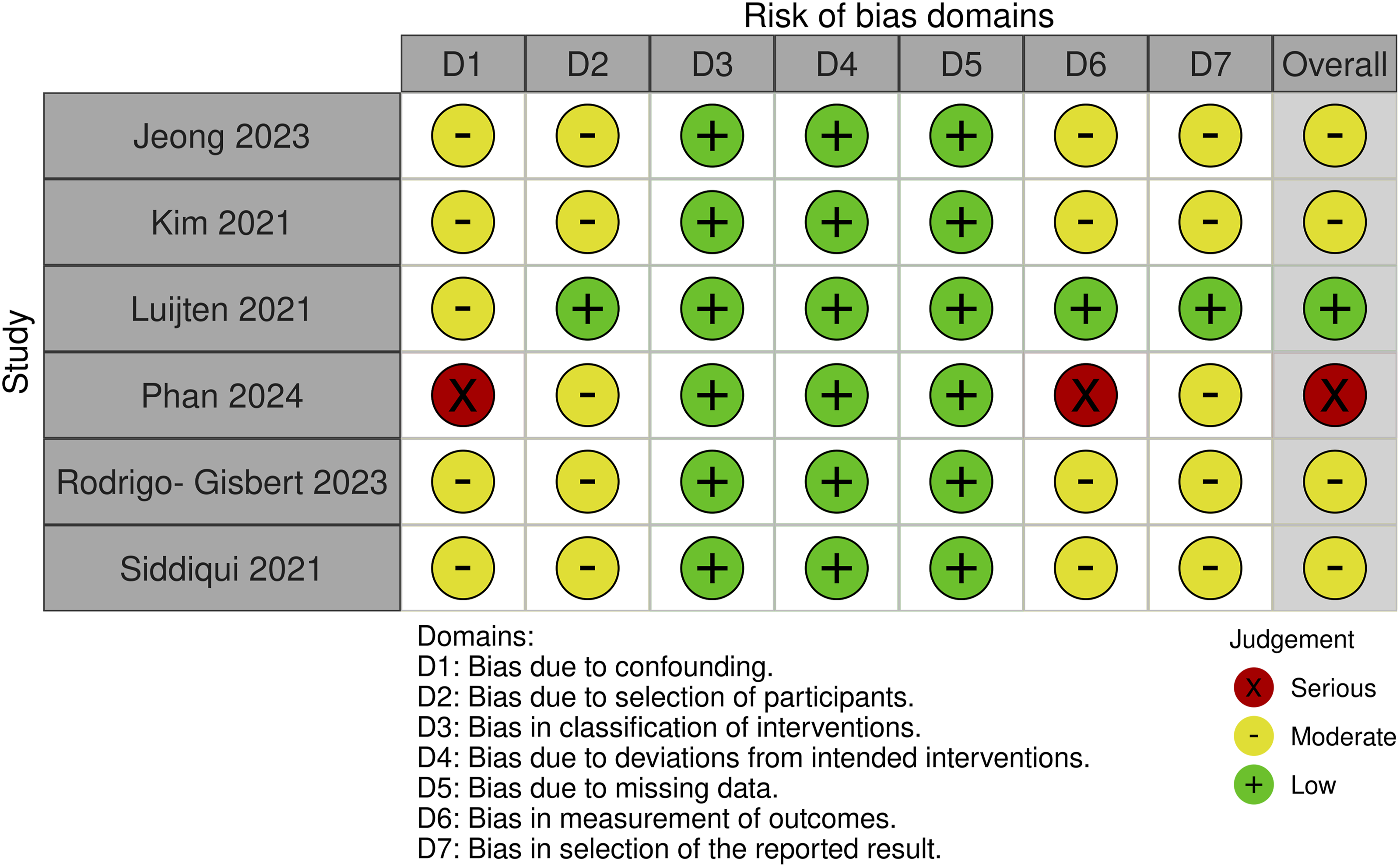
Discussion
This systematic review and meta-analysis aimed to investigate the prognostic impact of arterial calcification in patients with acute ischemic stroke treated with EVT. The pooled estimates of observational data revealed that arterial calcification, especially when located in intracranial segments, is significantly associated with lower procedural success and worse clinical outcomes. These results underscore the potential prognostic relevance of arterial calcification in the context of EVT for AIS. Specifically, calcification was linked to a 50% reduction in first-pass effect (RR 0.50; 95% CI 0.36–0.69) and a 10% lower likelihood of achieving successful reperfusion (RR 0.90; 95% CI 0.86–0.94). Previous investigations have also explored the association between arterial calcification and the risk of stroke recurrence, and more recent attention has shifted toward understanding how calcification burden may influence poststroke outcomes through its impact on vascular structure and function. 5 A proposed explanation is that arterial calcification contributes to greater vascular stiffness and potential luminal narrowing, which may impair device navigation or limit thrombus engagement during thrombectomy. These structural alterations could reduce the efficacy of recanalization and increase the likelihood of vessel injury, potentially culminating in incomplete clot retrieval or sICH. 17
With respect to safety outcomes, calcification was associated with a 51% higher risk of 90-day mortality (RR 1.51; 95% CI 1.14–2.00) and a 45% increased risk of symptomatic intracranial hemorrhage (RR 1.45; 95% CI 1.01–2.16). Functional independence (mRS 0–2) was 23% less likely in patients with calcification (RR 0.77; 95% CI 0.67–0.88), and the risk of poor outcome (mRS 3–6) was 29% higher (RR 1.29; 95% CI 1.16–1.43). These results underscore the prognostic relevance of arterial calcification, particularly intracranial calcification, in the context of EVT for acute ischemic stroke. Our findings build on prior research by reinforcing the association between arterial calcification and worse functional outcomes after stroke. 18 While the risk of poor outcomes (mRS score 3–6) increased by 29%, the probability of achieving functional independence (mRS score 0–2) decreased. These associations were homogenous across studies (I2 = 0% and 13%, respectively) and were linked primarily to intracranial calcification. Consistent with our findings, prior studies have reported that when intracranial atherosclerotic stenosis (ICAS) is the underlying cause of vessel occlusion, EVT may disrupt the atherosclerotic plaque surface, triggering platelet activation and increasing the risk of reocclusion and procedural failure.18,19,20 As such, vascular pathology seems to play a critical role in determining the success of EVT in patients with AIS.
The TICI score post-EVT has also been demonstrated to be closely linked to clinical outcomes.21,22 For successful reperfusion (TICI 2b–3), arterial calcification was associated with a modest but statistically significant reduction in the probability of achieving this procedural endpoint. While the absolute effect size was smaller than that for FPE, the consistency across six studies and moderate heterogeneity (I2 = 32%) suggest a clinically relevant signal. Subgroup analyses indicated that this effect was driven primarily by intracranial, rather than aortic arch, calcification.
Although it was not possible to assess whether the procedure outcomes were modified by the presence or absence of calcification in the artery involved in EVT, the association between arterial calcification and reduced FPE suggests a potential mechanical limitation imposed by calcified vessels during thrombectomy. This may be due to diminished vascular compliance in calcified vessels, which could negatively impact the effectiveness of thrombectomy and, consequently, functional outcomes.23,24 The pooled relative risk of 0.50 indicates that calcified arteries may impair device‒vessel interaction or clot retrieval efficiency.
The profound impact of arterial calcification on EVT success is driven by a multifactorial pathogenesis, particularly when the calcification is symptomatic, located directly at the occlusion site. 25 Symptomatic calcification frequently indicates underlying intracranial atherosclerotic disease (ICAD) rather than a purely embolic etiology, creating a high-risk environment characterized by significantly higher rates of intraprocedural reocclusion, prolonged procedure times, and a greater need for rescue interventions such as angioplasty and stenting. 26 Furthermore, calcification imposes severe mechanical impediments; calcium deposits reduce vessel pliability and create rigid target lesions or unyielding emboli that actively resist stent-retriever engagement, elevating the risk of device failure. 27 Beyond these macrovascular challenges, calcification also contributes to futile recanalization through systemic microvascular dysfunction. 28 The resulting loss of arterial compliance impairs cerebrovascular autoregulation and limits compensatory collateral flow, meaning that even when large-vessel patency is restored, tissue-level reperfusion often fails. 29 Ultimately, mechanical resistance to devices, a high risk of ICAD-related reocclusion, and impaired microcirculatory hemodynamics provides a comprehensive mechanistic explanation for the lower success rates and significantly poorer functional outcomes observed in these patients. 30
Even in populations with distinct clinical‒radiological characteristics, mortality at 90 days and the risk of symptomatic intracranial hemorrhage do not differ between patients with AIS who undergo EVT and those with standard medical care. 25 However, we observed that arterial calcification increased the risk of both 90-day mortality (RR 1.51) and sICH (RR 1.45), so its presence deserves to be carefully included in the risk stratification of EVT to avoid overshadowing its benefits. Previous studies have also examined the relationship between arterial calcification and outcomes such as hemorrhagic transformation or poor prognosis following thrombolysis; however, findings across the literature have been inconsistent.26,27,28
Overall, our subgroup analyses did not reveal significant interactions by calcification location across outcomes. However, intracranial calcification was more consistently associated with procedural inefficacy, adverse safety events, and poor functional outcomes.31,32 These findings may reflect location-specific vascular characteristics or differential relevance to the ischemic territory targeted by EVT.33,34 Although this meta-analysis provides evidence with potential clinical applicability, randomized controlled trials are still needed to strengthen causal inference and support decision-making in clinical practice.
Our study has several limitations that merit careful consideration. First, the included studies utilized substantial heterogeneity in calcification assessment, ranging from Agatston scores on CT to qualitative grading on X-Ray. While our statistical tests (I2) showed low heterogeneity, this likely reflects limited statistical power rather than true clinical homogeneity. Pooling these fundamentally different imaging criteria introduces a risk of measurement bias. Second, the use of unadjusted risk ratios means our estimates may be inflated by confounding variables. Older patients typically have more calcification and worse outcomes; without adjustment, it is difficult to isolate the independent effect of the calcification itself. Third, there is a potential for ecological bias and reverse causality. For instance, massive strokes might obscure vascular detailed imaging, or patients with higher frailty (and calcification) might be selected for EVT differently across centers. Missing baseline data in some included studies (e.g., age and sex distributions) prevented a more robust meta-regression to adjust for these potential confounders. Finally, the studies span different “eras” of thrombectomy technology, introducing heterogeneity in device performance that we could not control for.
Conclusion
Unadjusted pooled analyses indicate that arterial calcification, particularly intracranial calcification, may be correlated with advanced vascular disease. This condition can result in reduced procedural success and consequently poorer clinical outcomes in patients undergoing EVT for AIS. These findings underscore that vascular calcification acts as an associative marker of procedural complexity and advanced vascular disease in EVT candidates. Future prospective and interventional studies are warranted to better define the causal mechanisms, refine risk prediction models, and explore whether incorporating calcification metrics could enhance patient selection and optimize EVT outcomes.
Supplemental material
Supplemental material - Prognostic value of arterial calcification in acute ischemic stroke treated with endovascular thrombectomy: A systematic review and meta-analysis
Supplemental material for Prognostic value of arterial calcification in acute ischemic stroke treated with endovascular thrombectomy: A systematic review and meta-analysis by Marianna Leite, Luciano Falcão, Kenzo Ogasawara Donato, Ocilio Ribeiro Gonçalves, Gabriel Almeida Damasceno Gentil Arruda, Mariana Lee Han, Filipe Virgilio Ribeiro, Mariana Letícia de Bastos Maximiano, Ahmet Günkan, Christian Ferreira, Michel Ferreira Machado in The Neuroradiology Journal
Footnotes
Ethical considerations
Due to the open availability of data, ethical approval and informed consent statements do not apply to this project.
Consent to participate
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of the research.
Author contributions
All authors contributed to the study conceptualization and design. Conceptualization: M.L., O.R.G.; Data curation: L.F., G.A.D.G.A.; Formal analysis: K.O.D.; Investigation: M.L.A; Methodology: M.L.B.M.; Project administration: M.L., O.R.G.; Roles/Writing—original draft: M.L.A, M.L.B.M., M.L, F.V.R.; and Writing—review and editing: A.G., C.F., M.F.M. All authors have read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.