
Abstract
Background:
Acetaminophen (APAP) overdose, common during pandemics like COVID-19, causes liver injury through oxidative stress. Ginger, known for its antioxidant properties, is suggested as a potential natural remedy.
Objective:
This study aimed to evaluate the therapeutic and prophylactic efficacy of ethanol ginger extract (GE) and ginger suspension (GS) on APAP-induced hepatotoxicity and dyslipidemia in rats.
Methods:
Rats were assigned to ten groups: a control group, dimethyl sulfoxide group, and groups receiving either GE or GS (150 mg/kg) for two weeks. A group given a single high dose of APAP (2500 mg/kg), groups pre-treated with GE or GS before a single dose of APAP, a group receiving three repeated doses of APAP (500 mg/kg), and groups co-administrated GE or GS along with APAP over two weeks.
Results:
APAP administration at the two regimens significantly impaired liver function, antioxidant defenses, and lipid metabolism. These disruptions included reduced levels of antioxidant markers such as reduced glutathione (GSH), catalase (CAT), superoxide dismutase (SOD), glutathione S-transferase (GST), glutathione reductase (GR), glutathione peroxidase (GPx), and glucose-6-phosphate dehydrogenase (G6PDH). Lipid metabolism alterations were evident from increased triacylglycerols (TAGs), total cholesterol (T-chol), low-density lipoprotein cholesterol (LDL-chol), alongside decreased high-density lipoprotein cholesterol (HDL-chol). The high dose of APAP resulted in severe damage, indicated by elevated malondialdehyde (MDA), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and altered protein fractions. Both GE and GS treatments significantly alleviated these APAP-induced changes, particularly in MDA, ALT, GPx, and LDL-chol levels. GE demonstrated superior protective effects compared to GS, particularly in restoring levels of GSH, ALP, CAT, SOD, GST, GR, G6PDH, HDL-chol, albumin and alpha-1 globulins. In contrast, GS showed slightly greater effects on reducing TAGs and T-chol levels.
Conclusions:
Ginger extracts offer significant protection against APAP-induced liver damage and dyslipidemia, with GE providing more pronounced therapeutic effects.
This is a visual representation of the abstract.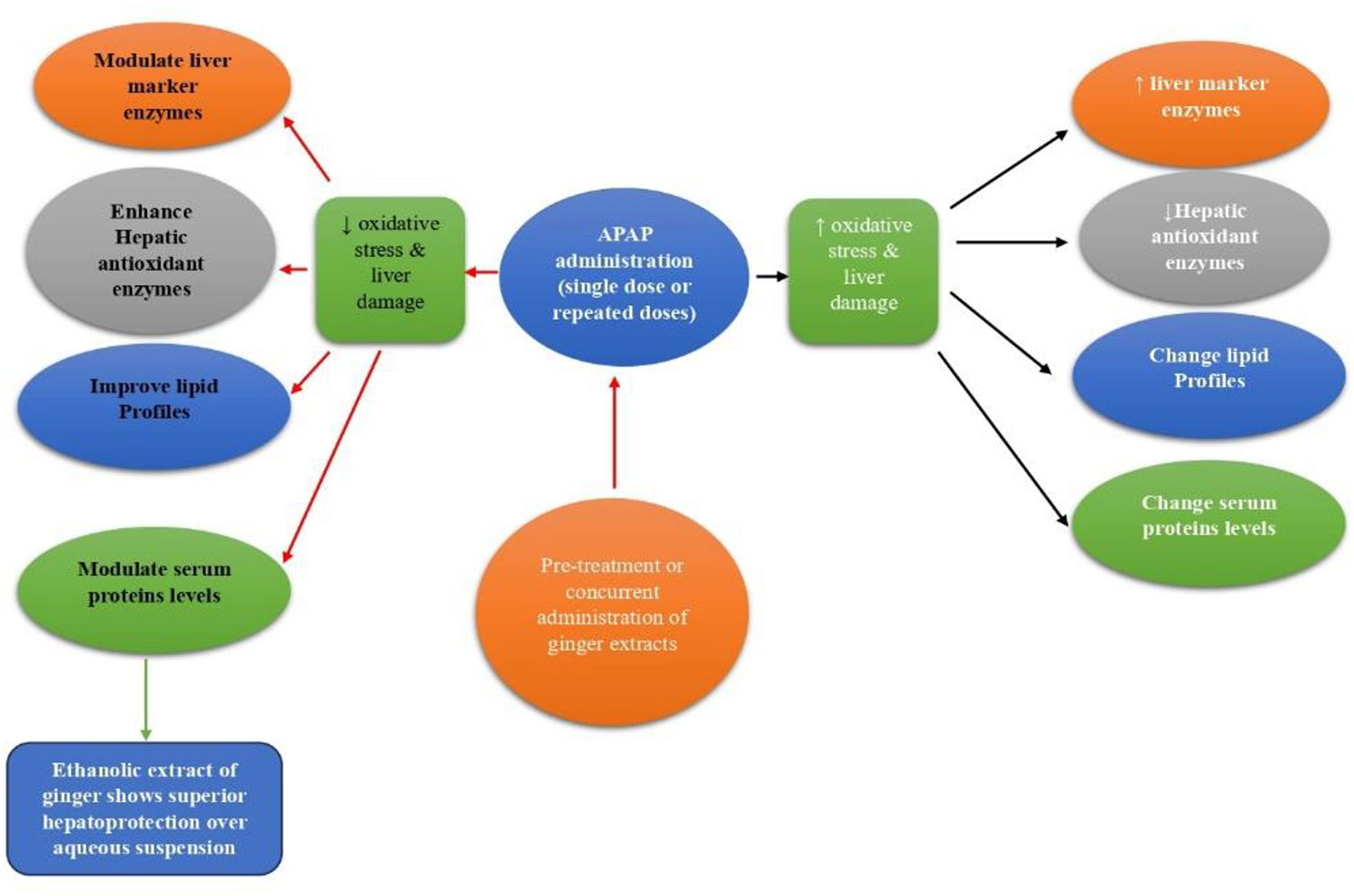
Introduction
The liver plays a vital role in detoxifying drugs and toxins through various phase I and phase II xenobiotic-metabolizing enzymes. However, this process can produce reactive oxygen species (ROS), which contribute to hepatotoxicity, cancer, and neurodegenerative diseases such as Alzheimer's.1,2 Particularly during phase I reactions, reactive metabolites and ROS can damage hepatic biomolecules, leading to mitochondrial dysfunction and endoplasmic reticulum stress. 3 To counteract oxidative stress, the liver relies on both enzymatic antioxidants, including superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx), and non-enzymatic antioxidants, such as glutathione (GSH).4,5
Acetaminophen (APAP), a widely used analgesic, can cause severe liver damage at high doses due to the formation of the toxic metabolite N-acetyl-p-benzoquinone imine (NAPQI), which depletes GSH and triggers oxidative stress, ultimately leading to hepatocyte necrosis. 6 The accumulation of NAPQI further exacerbates oxidative stress through ROS generation. 7 This highlights the need for effective protective strategies against drug-induced liver injury, such as natural antioxidants that may provide therapeutic benefits with minimal side effects.
Ginger (Zingiber officinale) has long been recognized for its medicinal properties, particularly its antioxidant, anti-inflammatory, and hepatoprotective effects. The bioactive compounds in ginger, such as gingerols, shogaols, and zingerone, have been shown to possess significant antioxidant properties, which help mitigate oxidative damage and protect against liver injury.8,9 Several studies have demonstrated that ginger can enhance antioxidant enzyme activities, inhibit lipid peroxidation, and reduce markers of liver damage, making it a promising natural remedy for liver protection.10,11
Given these potential benefits, the current study compares the hepatoprotective and antioxidant effects of two different forms of ginger—ethanol extract (GE) and water suspension (GS)—in a rat model of APAP-induced liver damage. The primary aim of this research is to assess which form of ginger more effectively mitigates liver damage and oxidative stress, by evaluating their impact on liver function markers, antioxidant enzyme activities, and lipid profiles. This study seeks to contribute to the development of plant-based therapeutic and prophylactic strategies for drug-induced liver injury and to support the use of natural remedies in hepatic damage treatment.
Materials and methods
Chemicals
Dried rhizomes of ginger were purchased from Cairo Market. The plant material was identified by a colleague from the Botany Department, and a voucher specimen (Ginger-4-17) has been deposited at the Department of Botany, Faculty of Science, Ain Shams University (Cairo, Egypt). Acetaminophen was obtained from Sigma (St Louis, MO, USA). Reagents for Helena serum protein electrophoresis were purchased from Helena Bio-Sciences Europe (Saint Leu La Foret, France).
Plant preparations
Ginger rhizomes were ground with a lab electric grinder. For GE, 75 g of powdered ginger was extracted with 300 mL of 95% ethanol at 78.1 °C for two hours using a Soxhlet apparatus. The solvent was evaporated under vacuum with a rotary evaporator, leaving a dark brown residue. This residue was dissolved in 2 mL of dimethyl sulfoxide (DMSO) and diluted with distilled water. GS was prepared by mixing 10 g of ginger powder with 100 mL of distilled water.
Experimental animals
Adult male albino healthy rats weighing approximately 170 ± 20 g at the beginning of the experiment were used throughout the study. The animals were obtained from the National Research Center (Dokki, Egypt) and housed in suitable cages for one week for acclimatization to laboratory conditions. A 12-h dark/light cycle was maintained with access to fresh water and standard laboratory rodent pellets. All experiment procedures were approved by the Institutional Ethics Committee at the Faculty of Science, Ain Shams University (Protocol # 2017-AW01-2) and followed the “Guide for the Care and Use of Laboratory Animals.” Rats were monitored daily for behavioral changes and signs of sickness, with any abnormalities documented. No animals died during the experiment. Rats were excluded if they exhibited signs of pre-existing liver disease, infection, or other abnormal physiological conditions that could confound the results. Additionally, animals that showed significant changes in body weight (either loss or gain outside the expected range for their age and gender) were excluded to ensure uniformity in the study population.
Experimental design
In this study, 70 adult male albino rats were divided into ten groups (n = 7 each). Group one served as the negative control. Group two received DMSO as a vehicle control. Groups three and four were administered GE and GS, respectively, at 150 mg/kg orally for two weeks. 10 Group five received a single oral dose of acetaminophen (APAP) (2500 mg/kg). 12 Groups six and seven were pre-treated with GE and GS, respectively, for two weeks before receiving a single dose of APAP. Groups 8–10 were given a total of three repeated oral doses of APAP (500 mg/kg) over two weeks. 13 Groups nine and ten co-administered APAP with GE or GS (150 mg/kg), respectively, for two weeks. A DMSO-only group was included as a vehicle control to isolate the solvent's effects and distinguish them from those of GE.
Blood sampling and tissue extraction
At the end of the experiment, animals were anesthetized with isoflurane and sacrificed. Isoflurane was administered at a concentration of 3% in oxygen for induction and 2% for maintaining anesthesia. Blood samples were collected into sterile test tubes and allowed to coagulate at room temperature. The samples were immediately centrifuged to separate the serum, which was aliquoted and stored at −80 °C for subsequent analysis. Immediately after sacrifice, the livers were perfused with cold isotonic saline via the hepatic portal vein. They were then dissected, weighed, wrapped in aluminum foil, and stored at −80 °C. The liver tissues were perfused with cold isotonic saline, homogenized in a cold buffer (50 mM potassium phosphate buffer, pH 7.3, containing 2 mM EDTA), and β-mercaptoethanol was added for the glutathione peroxidase assay. After centrifugation at 1500 × g for 15 min at 4 °C, the supernatant was collected and stored at −80 °C for further assays, while an aliquot was retained for protein determination.
Biochemical assays
The assays for alanine aminotransferase (ALT), alkaline phosphatase (ALP), CAT, SOD, glutathione reductase (GR), glutathione S-transferase (GST), glucose 6-phosphate dehydrogenase (G6PDH), GPx, reduced GSH, malondialdehyde (MDA), total cholesterol (T-chol.), triacylglycerols (TAGs), and high-density lipoprotein (HDL) cholesterol were conducted using kits from Biodiagnostic Company (Cairo, Egypt); following the manufacturer's instructions. The methods of measurements could be reviewed elsewhere.14–16 Serum low-density lipoprotein (LDL) cholesterol levels were calculated using the Martin-Hopkins equation:

The Helena serum protein electrophoresis procedure separates and quantifies serum proteins based on their electrical charges at pH 8.8 using cellulose acetate plates. Proteins are separated by electrophoretic and electroosmotic forces, fixed with sulfosalicylic and trichloroacetic acids, and stained with Ponceau S, where staining intensity indicates protein concentration. Plates are cleared, dehydrated, and analyzed for quantification. Reagents include Ponceau-S stain (0.5% in 3.5% sulfosalicylic and trichloroacetic acid), Electra R HR buffer (tris-barbital, pH 8.6–9.0), clearing solution (glacial acetic acid, methanol, polyethylene glycol), Titan R III cellulose acetate plates, 5% acetic acid, and absolute methanol. The procedure involves soaking Titan R III plates in HR buffer for 20 min. Electrophoresis chambers are prepared with buffer-filled sections, and wicks are positioned without air bubbles. Samples (3 µL), including normal rat serum for comparison, are loaded on plates using a microdispenser, blotted, and aligned in the chamber. Electrophoresis is conducted at 180 volts for 15 min. Protein bands are visualized by staining plates in Ponceau S for 6 min, followed by destaining in 5% acetic acid (3 washes, 2 min each). Plates are dehydrated in methanol (2 washes, 2 min each), cleared for 10 min, and dried at 50–60 °C for 15 min. Bands are scanned at 525 nm using a densitometer, and their concentrations are calculated with a Helena computerized system. 18
Statistical analysis
Data are presented as Mean ± Standard error of the mean (SEM). Statistical analyses of the data were performed using One-Way Analysis of Variance (ANOVA) followed by Tukey's multiple comparison test to assess significant differences among groups. Values of p < 0.05 were considered significant.
Results
Effect on oxidative stress milieu and liver functions
Treating rats with GE at 150 mg/kg for two weeks resulted in significant elevation in hepatic GSH content by 611.87% compared to the control group (Figure 1(a)). Conversely, a single dose of APAP at 2500 mg/kg led to a significant decrease in hepatic GSH levels by 57.44% compared to the control group (Figure 1(a)). However, pretreatment of rats with GE or GS prevented the decline in hepatic GSH levels and exhibited significant increases by about 1595% and 178%, respectively, compared to the APAP group (Figure 1(a)). In a therapeutic regimen administering three equal doses of APAP (500 mg/kg) over two weeks, there was a substantial decline in hepatic GSH levels by 56% compared to the control group. Concurrent use of GE or GS during this period notably increased GSH levels by 734% and 171%, respectively, compared to the APAP (500 mg/kg) group (Figure 1(a)).
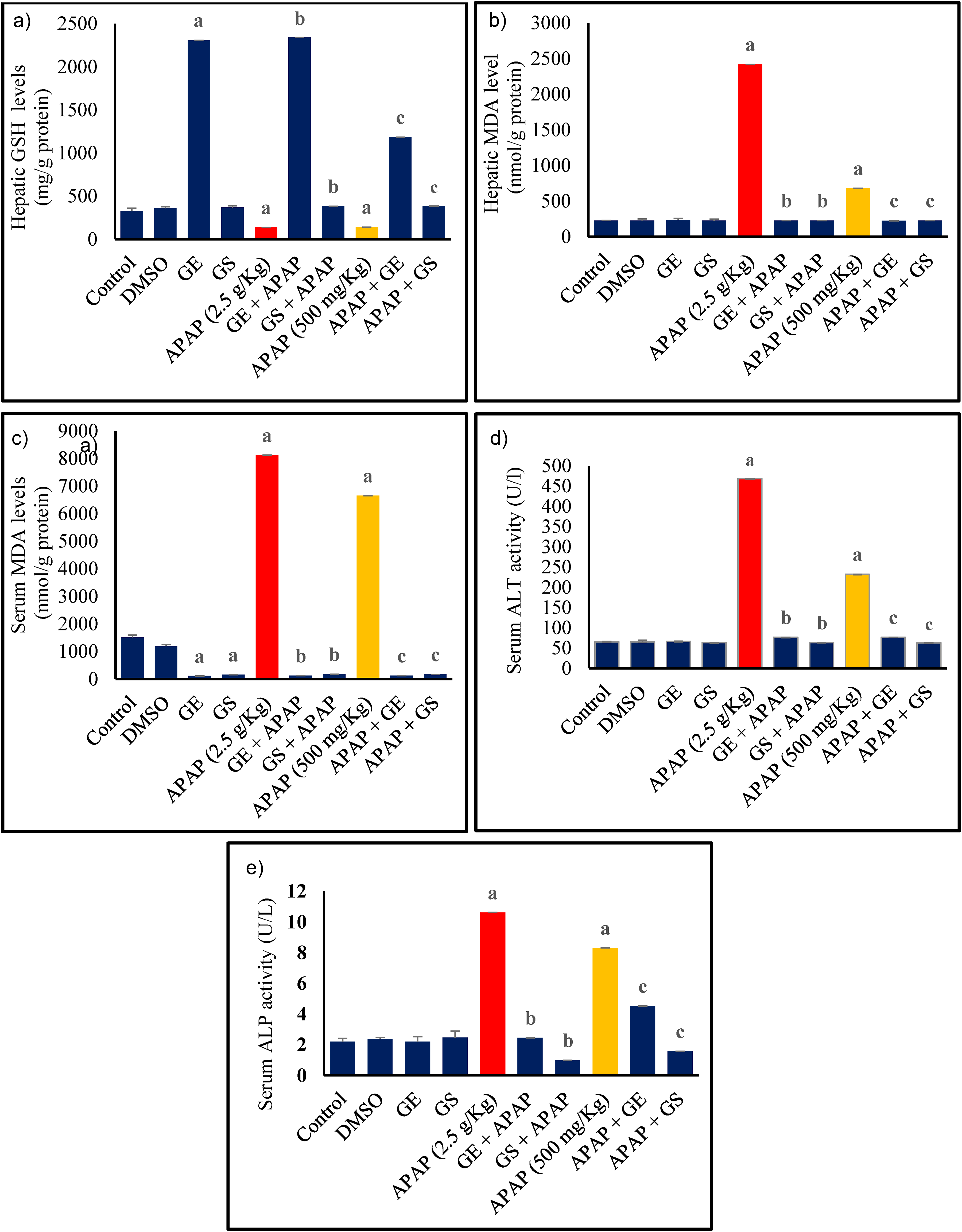
Effect of ginger on (a) hepatic reduced glutathione (GSH), (b) hepatic malondialdehyde (MDA), (c) serum malondialdehyde (MDA), (d) serum alanine aminotransferase (ALT), (e) serum alkaline phosphatase (ALP). Results are expressed as the Mean ± SEM, n = 7. a Significant difference vs. control; b significant difference vs APAP (2.5 g/kg) group; c significant difference vs. APAP (500 mg/kg). Abbreviations: APAP: Acetaminophen; SEM: Standard Error of the Mean; GE: Ginger Ethanol Extract; GS: Ginger Suspension; DMSO: Dimethyl Sulfoxide.
Treating animals with GE or GS did not significantly alter the level of hepatic MDA (Figure 1(b)). Figure 1(c) demonstrates that treatment with GE or GS significantly reduced serum MDA levels by 93% and 90%, respectively, compared to the control group. A single dose of APAP significantly increased serum and hepatic MDA levels by 439% and 974%, respectively, compared to controls (Figure 1(b) and (c)). Conversely, pre-treatment with GE and GS resulted in a 99% reduction in serum MDA levels and a 91% reduction in hepatic MDA levels compared to the APAP (2500 mg/kg) group. Similarly, administering three doses of APAP over two weeks caused an increase in serum and hepatic MDA levels by 341% and 201%, respectively, compared to the control group. However, concurrent GE or GS treatment significantly reduced serum MDA levels by 98%, and hepatic MDA levels by 67%, relative to the APAP (500 mg/kg) group (Figures 1(b) and (c)).
Regarding liver function markers, a single high dose of APAP significantly elevated serum ALT and ALP activities by 621% and 386%, respectively, compared to the control group (Figures 1(d) and (e)). Rats pre-treated with GE or GS exhibited significantly lower serum ALT and ALP activities, with ALT reductions of 84% and 87%, and ALP reductions of 78% and 91%, respectively, relative to the APAP-only group. Similarly, three doses of APAP over two weeks resulted in increased ALT and ALP activities by 257% and 280%, respectively, compared to controls. Concurrent administration of GE or GS during this period substantially reduced these elevated enzyme levels, with ALT reductions of 67% and 73%, and ALP reductions of 46% and 80%, respectively, compared to the APAP (500 mg/kg) group, underscoring their therapeutic efficacy.
Figure 2 shows that a two-week treatment with GE significantly increased hepatic CAT and SOD activities by 1147% and 115%, respectively compared to the control group (Figure 2(a)). Hepatic CAT and SOD activities were significantly reduced by a single dose of APAP, with CAT and SOD activities dropping by 81% and 61%, respectively, compared to controls (Figures 2(a) and (b)). However, rats pre-treated with GE or GS displayed significantly higher CAT and SOD activities, with CAT increasing by 4194% and 754%, and SOD increasing by 383% and 93%, respectively, compared to the APAP-only group. Similarly, the three-dose APAP regimen caused a decline in CAT and SOD activities by 75% and 60%, respectively, compared to control. Co-administration with GE or GS significantly elevated these activities, with CAT increasing by 4632% and 463%, and SOD increasing by 131% and 288%, respectively, relative to the APAP-treated group.
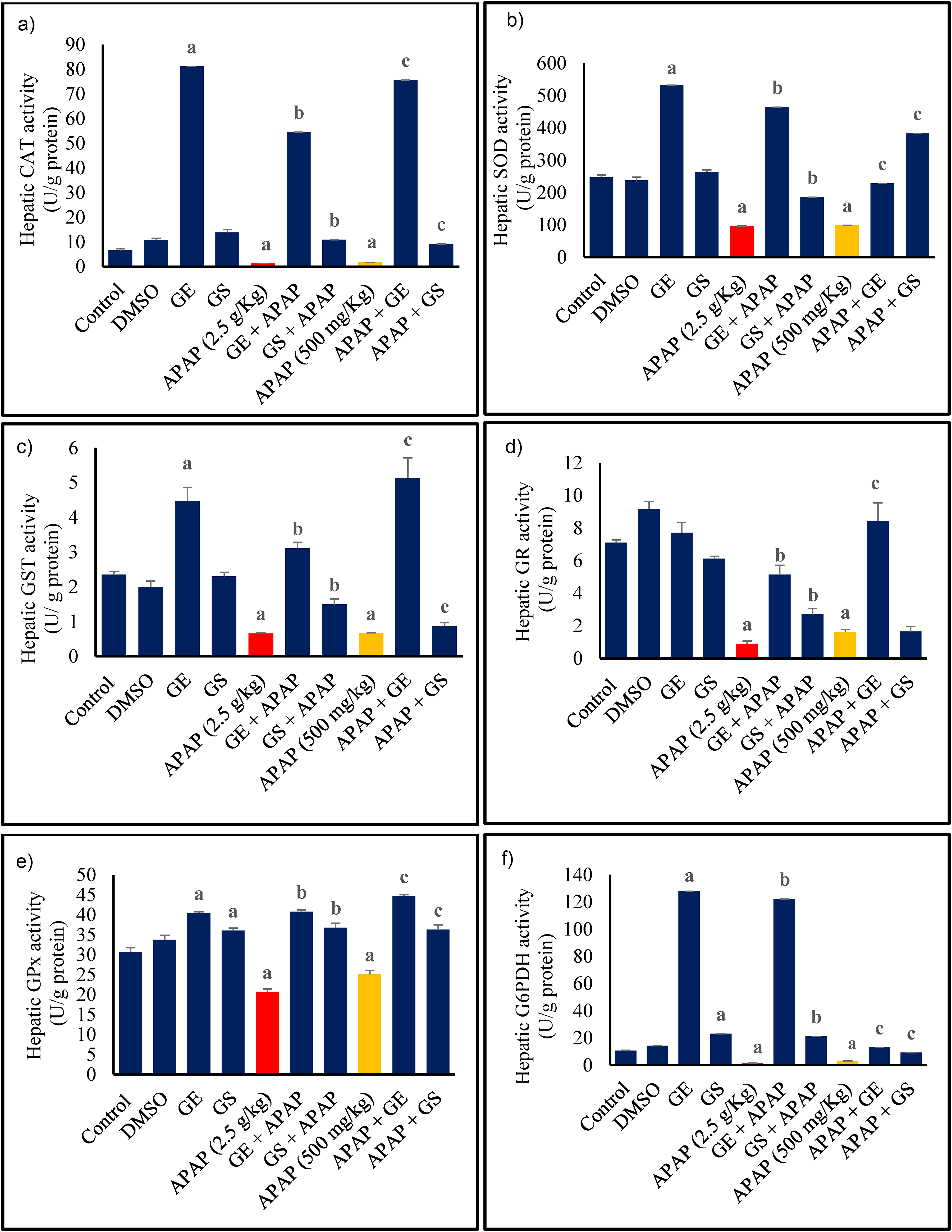
Effect of ginger on hepatic (a) catalase (CAT), (b) superoxide dismutase (SOD), (c) glutathione S-transferase (GST), (d) glutathione reductase (GR), (e) glutathione peroxidase (GPx), (f) glucose 6-phosphate dehydrogenase (G6PDH). Results are expressed as the Mean ± SEM, n = 7. a Significant difference vs. control; b significant difference vs APAP (2.5 g/kg) group; c significant difference vs. APAP (500 mg/kg). Abbreviations: APAP: Acetaminophen; SEM: Standard Error of the Mean; GE: Ginger Ethanol Extract; GS: Ginger Suspension; DMSO: Dimethyl Sulfoxide.
Additionally, GE treatment significantly increased hepatic GST, GPx, and G6PDH activities by 91%, 32%, and 1125%, respectively, compared to control. While GS treatment notably elevated hepatic GPx and G6PDH by 18% and 120%, respectively. In contrast, a single dose of APAP markedly reduced hepatic GST, GR, G6PDH, and GPx activities by 71%, 87%, 86%, and 32%, respectively (Figures 2(c)–(f)). Rats receiving GE or GS followed by APAP exhibited significantly increased hepatic enzyme activities. Specifically, GE resulted in increases of 370%, 470%, 8058%, and 96% in GST, GR, G6PDH, and GPx, respectively, compared to the APAP-only group. Similarly, GS led to increases of 125%, 200%, 1287%, and 77% in these enzymes, respectively. Three equal doses of APAP over two weeks decreased these activities by 65%, 58%, 85%, and 37% for GST, GR, G6PDH, and GPx, respectively. However, co-administration with GE or GS during this period restored these enzyme activities. Specifically, APAP + GE treatment increased GST, GR, G6PDH, and GPx activities by 677%, 418%, 312%, and 78%, respectively, while APAP + GS increased GST, G6PDH, and GPx activities by 32%, 191%, and 45%, respectively, compared to the APAP-only group.
Effect on serum lipid profile
Regarding the serum lipid profile, treatment with GS or GE resulted in significantly lower serum triacylglycerol (TAG) levels compared to controls, with reductions of 45% for GE and 21% for GS (Figure 3(a)). A single dose of APAP, however, significantly increased serum TAG levels by 60% compared to controls, which were mitigated by prior daily GE or GS treatment, reducing TAG levels by 67% for GE and 44% for GS (Figure 3(a)). Similarly, three doses of APAP also elevated serum TAG levels by 37%, but concurrent GE or GS administration significantly reduced these levels by 60% and 35%, respectively, compared to the APAP-only group. APAP treatment alone increased T. chol. levels by 58%. However, GE or GS pre-treatment significantly lowered these levels by 21% and 31%, respectively (Figure 3(b)). Similarly, three doses of APAP elevated serum T. chol. levels by 56%, but concurrent GE or GS administration significantly reduced these levels by 19% and 31%, respectively, compared to the APAP-only group. Serum high-density lipoprotein cholesterol (HDL-chol.) levels were significantly reduced by a single dose of APAP by 67%. Yet, GE or GS pre-treatment prevented this reduction and resulted in significant increases of 293% for GE + APAP and 231% for GS + APAP (Figure 3(c)). Repeated APAP doses similarly decreased HDL-chol. by 51%, but co-administration with GE or GS significantly improved HDL-cholesterol levels with increases of 169% and 102%, respectively (Figure 3(c)). GE and GS treatments significantly reduced low-density lipoprotein cholesterol (LDL-chol.) levels compared to controls, with decreases of 96% for GE and 77% for GS (Figure 3(d)). In contrast, high dose of APAP caused a dramatic increase in LDL-chol. levels, rising by 3205% compared to the control group. However, pretreatment with GE or GS effectively mitigated this effect, significantly decreasing LDL-chol levels by 95% and 34%, respectively compared to the APAP-only group. Additionally, administering three equal doses of APAP over two weeks resulted in 2904.4% increase in LDL-chol. compared to the control group. Yet, concurrent administration of GE or GS decreased these elevated LDL-chol. levels by 94% and 86%, respectively.
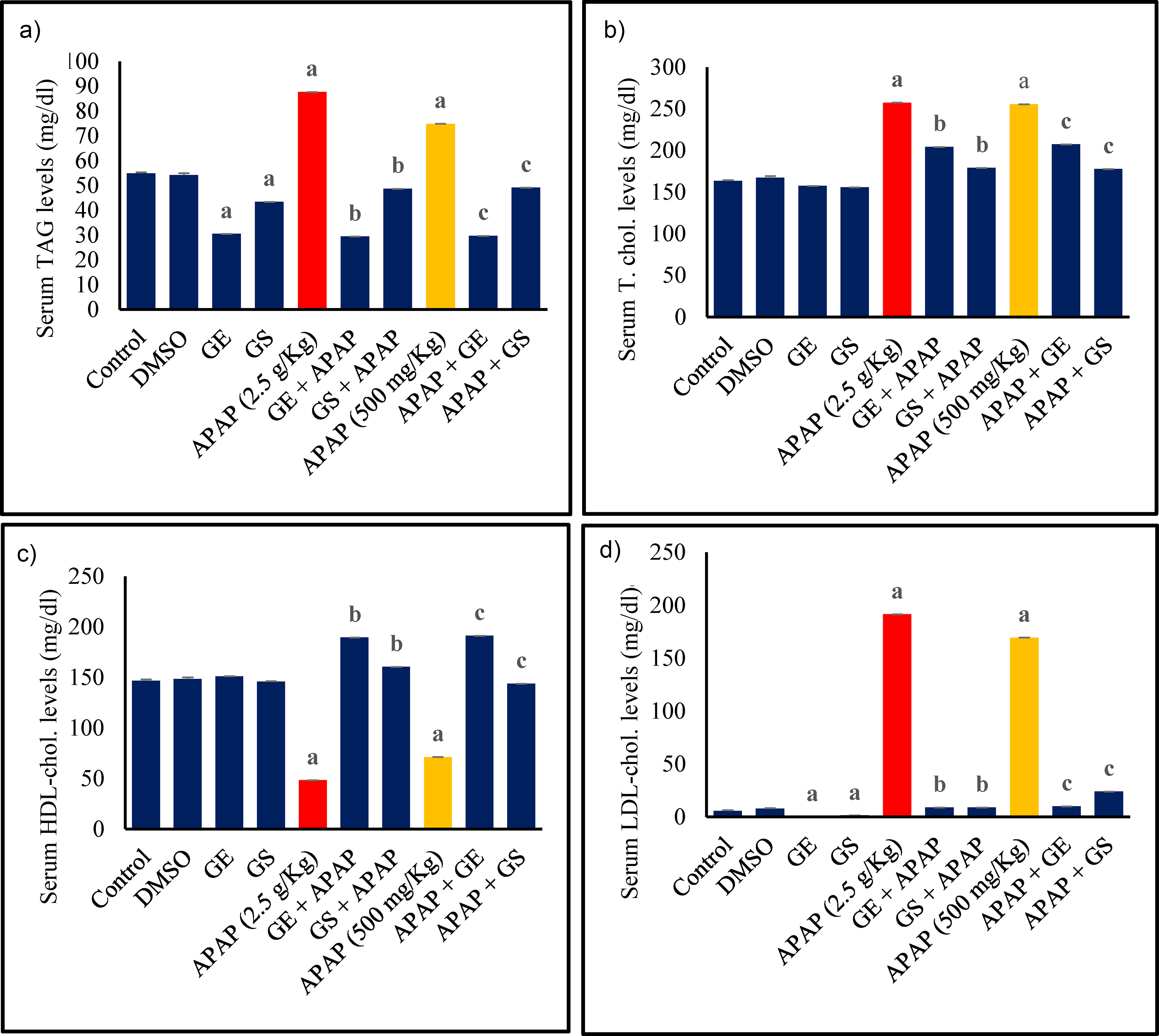
Effect of ginger on serum (a) triacylglycerol (TAG), (b) total cholesterol (T. chol.), (c) cholesterol in high density lipoprotein (HDL-chol.), (d) cholesterol in low density lipoprotein (LDL-chol.). Results are expressed as the Mean ± SEM, n = 7. a Significant difference vs. control; b significant difference vs APAP (2.5 g/kg) group; c significant difference vs. APAP (500 mg/kg). Abbreviations: APAP: Acetaminophen; SEM: Standard Error of the Mean; GE: Ginger Ethanol Extract; GS: Ginger Suspension; DMSO: Dimethyl Sulfoxide.
Effect on serum protein fractions
A single high dose of APAP caused a significant reduction in serum albumin levels by 40% compared to the control group (Figure 4). When rats were pre-treated with GE for two weeks before receiving APAP, there was a notable recovery in serum albumin levels, which were 51% higher than those in the APAP-only group. GS pre-treatment showed only an insignificant increase of 29% in albumin levels compared to the APAP-only group. For rats receiving three doses of APAP over two weeks, serum albumin levels decreased slightly by 18%, but this reduction did not achieve a statistical significance compared to the control group.
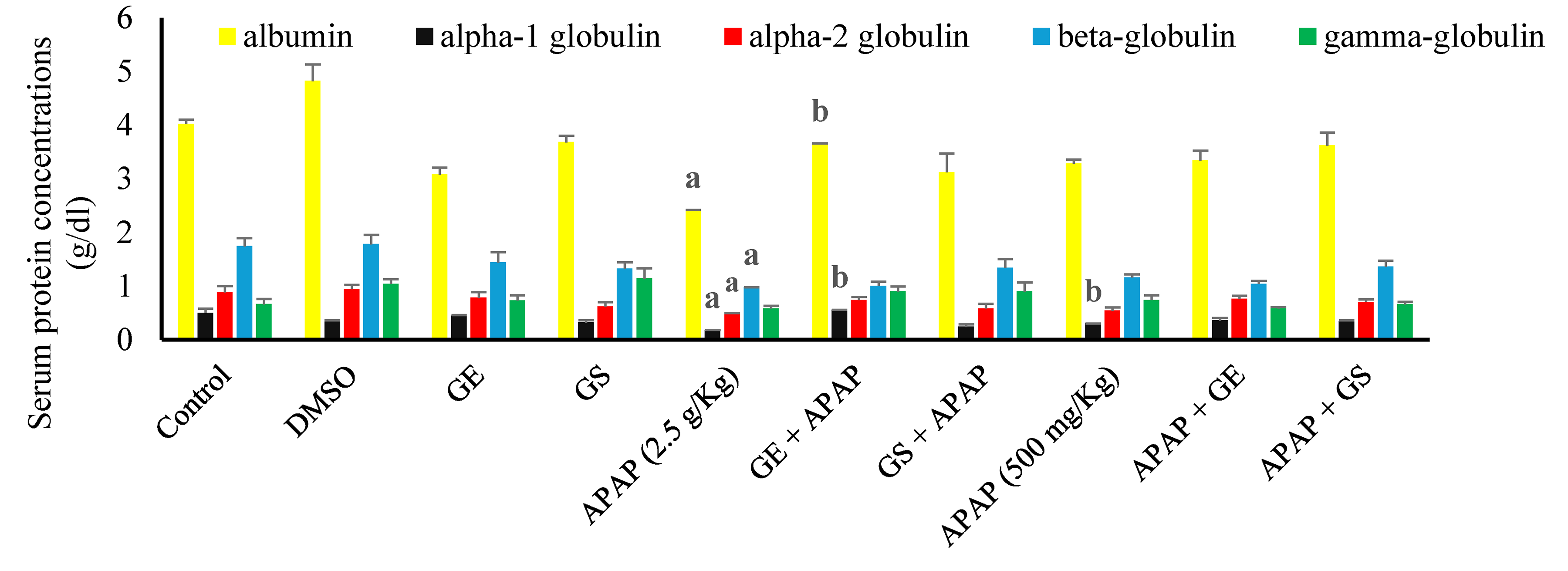
Effect of ginger on serum protein concentrations. Results are expressed as the Mean ± SEM, n = 7. a Significant difference vs. control; b significant difference vs APAP (2.5 g/kg) group; c significant difference vs. APAP (500 mg/kg). Abbreviations: APAP: Acetaminophen; SEM: Standard Error of the Mean; GE: Ginger Ethanol Extract; GS: Ginger Suspension; DMSO: Dimethyl Sulfoxide.
A single dose of APAP led to significant reductions in serum alpha-1, alpha-2, and beta-globulins by 64%, 43%, and 44%, respectively, compared to the control group (Figures 4 and 5). Pre-treatment with GE or GS did not result in significant changes in these globulin levels compared to the APAP-only group, with the exception of the significant elevation of 211% for alpha-1 globulins after GE protective dosing regimen. When administered in three doses, APAP also caused a significant decrease in alpha-1 globulins by 40%, with neither GE nor GS significantly restoring these levels compared to the APAP-only group. APAP also reduced alpha-2-, beta-, and gamma- globulins but insignificantly (Figures 4 and 5).
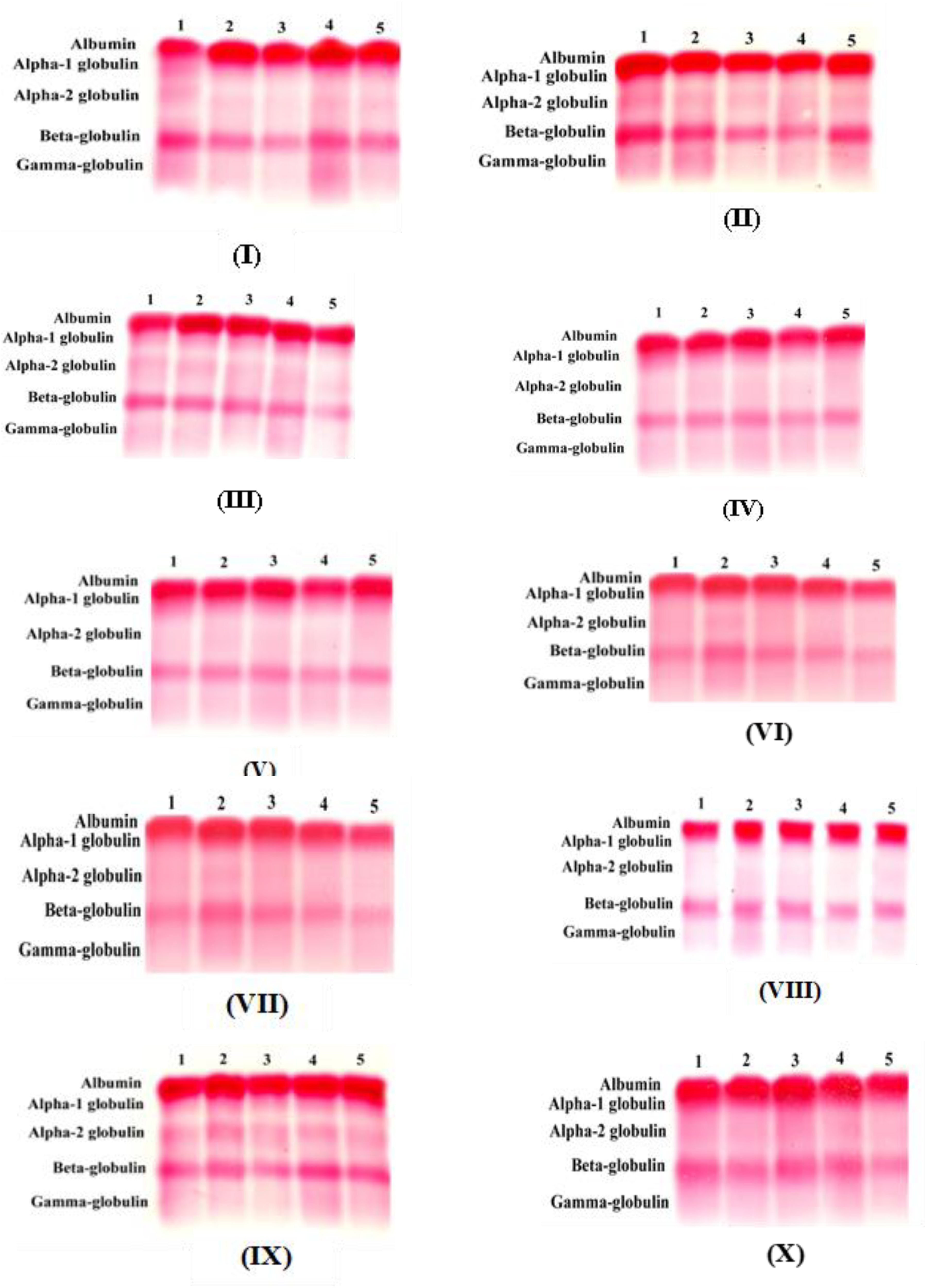
Photograph of cellulose acetate serum protein electrophoresis. (I) Control, (II) DMSO, (III) ginger ethanolic extract (GE), (IV) ginger water suspension (GS), (V) APAP (2.5 g/kg), (VI) GE + APAP, (VII) GS + APAP, (VIII) APAP (500 mg/kg), (XI) APAP + GE, and (X) APAP + GS.
Discussion
Acetaminophen (APAP) is commonly used as an antipyretic and analgesic, but excessive consumption can lead to severe liver damage and other complications. 19 APAP is primarily metabolized in the liver through phase II conjugation pathways, such as glucuronidation and sulfation, converting it into non-toxic metabolites. 20 However, a small portion is metabolized by the cytochrome P450 enzyme CYP2E1, producing a highly reactive and toxic metabolite, NAPQI. Under normal conditions, NAPQI is detoxified by conjugation with GSH, preventing cellular damage. During an APAP overdose, however, GSH reserves are depleted, leading to the accumulation of NAPQI. This metabolite binds to liver proteins, inducing oxidative stress and hepatocellular injury.21,22
Both treatments with a high single dose (2500 mg/kg) and three doses (500 mg/kg) of APAP caused hepatotoxicity and led to a similar detrimental effects on GSH, CAT, SOD, GST, GR, GPx, G6PDH, TAGs, T.chol, LDL-chol, and HDL-chol. However, the high dose of APAP resulted in more severe deteriorations in MDA, ALT, ALP, and protein fractions assessed by electrophoresis. APAP at 2500 mg/kg dose rapidly depleted hepatic GSH, compromising the liver's ability to detoxify NAPQI. With GSH levels diminished, ROS accumulated, leading to oxidative stress, marked by a significant increase in MDA, a key marker of lipid peroxidation. Elevated serum and hepatic MDA levels indicate extensive oxidative damage to cellular membranes, compromising hepatocyte integrity.23–25 This oxidative damage caused the leakage of intracellular contents, including liver marker enzymes such as ALT and ALP into the bloodstream. Elevated activities of these enzymes in serum serve as biomarkers of hepatocellular injury, reflecting compromised liver function.26–28
Additionally, APAP treatment significantly reduced the activities of key hepatic antioxidant enzymes, including CAT, SOD, GST, GR, G6PDH, and GPx. This reduction weakened the liver's antioxidant defenses, leading to further accumulation of ROS and exacerbating oxidative damage. CAT, responsible for decomposing hydrogen peroxide (H2O2), showed reduced activity, impairing the liver's ability to detoxify H2O2 and worsening oxidative stress. Similarly, diminished SOD activity led to an accumulation of superoxide radicals that contributed to further oxidative damage. The decreased activity of GST reduced the liver's capacity to detoxify harmful substances, while the reduced activity of GR compromised the regeneration of GSH, further impairing the liver's antioxidant capacity. The decline in G6PDH activity, crucial for producing NADPH to support GSH regeneration, limited the liver's ability to counteract oxidative stress.29–31
Moreover, APAP-induced liver injury disrupted lipid metabolism, evidenced by elevated serum levels of TAG, total cholesterol, and LDL cholesterol, alongside reduced HDL cholesterol. These changes reflect impaired liver function as APAP's hepatotoxic effects overwhelmed the liver's ability to regulate lipid metabolism.32–34 Furthermore, APAP at a dose of 2500 mg/kg led to a reduction in serum levels of albumin, alpha-2, and beta-globulins, indicating impaired protein synthesis and liver dysfunction. Interestingly, the repeated lower-dose regimen resulted in a more severe reduction in alpha-1 globulins compared to the single high dose. This decline in protein fractions confirms liver dysfunction, as the liver's capacity to synthesize essential proteins was compromised, closely linked to the oxidative stress and cellular injury induced by APAP.35,36
Both treatments with GE and GS equally alleviated the deterioration caused by APAP in MDA, ALT, GPx, and LDL-chol. However, for most parameters, GE provided superior mitigation effects compared to GS. This was particularly evident in GSH, ALP, CAT, SOD, GST, GR, G6PDH, HDL-chol, and protein fractions, specifically albumin and alpha-1 globulins. In only two parameters, GS demonstrated better alleviation than GE, specifically in TAGs and T-chol. Pre-treatment and concurrent administration of GE or GS (150 mg/kg/day) for two weeks significantly improved hepatic GSH levels and reduced MDA levels compared to the APAP-only groups, effectively enhancing the liver's antioxidant capacity and mitigating oxidative stress. By boosting GSH levels, GE and GS counteracted the harmful effects of APAP, reducing lipid peroxidation and alleviating cellular damage and inflammation associated with APAP toxicity.37–39
Both treatments also significantly reduced serum ALT and ALP activities, indicating reduced hepatocellular injury. The bioactive components in ginger enhance antioxidant defenses by replenishing GSH levels and neutralizing ROS, thereby reducing oxidative damage to hepatocytes. Additionally, ginger extracts may modulate inflammatory responses and inhibit apoptotic pathways, further contributing to liver protection.40–43
In terms of lipid metabolism, both pre-treatment and concurrent administration of GE or GS restored serum TAG levels to near-control values and countered the elevations of total cholesterol as well as altered HDL and LDL cholesterol levels induced by APAP. This improvement is attributed to their antioxidant, anti-inflammatory, and lipid-modulating properties.44–46 Moreover, pre-treatment with GE for two weeks prior to APAP exposure significantly elevated serum albumin and alpha-1 globulin levels compared to the APAP-only group. This improvement can be attributed to GE's potent antioxidant properties, which enhance liver function by increasing GSH levels and boosting antioxidant enzyme activity, thus preserving liver function and preventing severe reductions in protein synthesis typically seen in APAP-induced liver damage.47–49
In this study, both a single high dose of APAP (2500 mg/kg) and repeated lower doses (500 mg/kg administered three times over two weeks) were evaluated for their effects on liver injury and oxidative stress. While both regimens caused significant liver damage, the single high dose led to more severe oxidative stress and hepatocellular injury compared to repeated lower doses. These findings underscore the risks associated with administration of high-dose APAP, even within therapeutic ranges, while repeated lower doses, though harmful, resulted in less acute liver damage.50–52
This study highlights the distinct effects of GE and GS on oxidative stress and lipid metabolism, offering valuable insights for optimizing ginger's hepatoprotective potential. By exploring both therapeutic and preventive models, it emphasizes the dual role of natural antioxidants in treating and preventing drug-induced hepatotoxicity. Additionally, the ability of ginger extracts to restore lipid profiles disrupted by acetaminophen extends their benefits to metabolic health. These findings pave the way for future research into the molecular mechanisms and bioactive compounds responsible for ginger's protective effects. This study, although novel in investigating GE and GS as adjunctive therapies for APAP-induced hepatotoxicity and dyslipidemia, has some limitations. Measuring the levels of CYP2E1, glucuronosyl transferase, and NAPQI could have provided further insights into the molecular mechanisms associated with the alleviations provided by ginger. Another limitation of this study is the lack of detailed information about the cultivation and post-harvest conditions of the ginger rhizomes used, as they were sourced from a local market. Factors such as geographic origin and agricultural practices can impact the concentration of bioactive compounds like gingerols and shogaols, potentially affecting the extract's therapeutic efficacy. Despite this variability, the findings remain significant, reflecting the practical use of readily available ginger. Future studies should ensure consistent sourcing of rhizomes to better correlate bioactive content with biological effects.
Conclusions
In conclusion, this study demonstrated that both a single high dose (2500 mg/kg) and repeated lower doses (500 mg/kg) of APAP result in significant liver injury and oxidative stress, with the single higher dose leading to more severe liver deterioration. Both treatments with GE and GS equally alleviated the damage caused by APAP in MDA, ALT, GPx, and LDL-chol. However, for most parameters, GE consistently outperformed GS in providing both prophylactic and therapeutic effects against APAP-induced liver toxicity. This was particularly evident in GSH, ALP, CAT, SOD, GST, GR, G6PDH, HDL-chol, and protein fractions, specifically albumin and alpha-1 globulins. In only two parameters did GS demonstrate better alleviation than GE, specifically in TAGs and T-chol. Overall, these findings indicate that GE's antioxidant, hepatoprotective, and lipid-modulating effects make it a superior option compared to GS for both preventing and treating APAP-induced hepatic injury. The superior effectiveness of GE can be attributed to its higher concentration of bioactive compounds such as gingerols, shogaols, and paradols, obtained through ethanol extraction, which are known for their strong antioxidant, anti-inflammatory, and hepatoprotective properties. Moreover, GE ensures enhanced bioavailability, better stability, and a longer shelf life compared to water-based extracts, making it a more potent option for therapeutic use.
Footnotes
Author contributions
Conceptualization and Experimental Design of the Study: WME. Data Curation: MAA, WME. Methodology: MAA. Formal Analysis: MAA, WME. Investigation: MAA. Validation: WME. Supervision: NME, WME. Writing original draft: MAA. Review and editing: WME. All authors have read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data are presented in the manuscript.