
Abstract
Background:
Serotonin syndrome (SS) is a potentially life-threatening condition increasingly driven by complex drug-drug interactions (DDIs) as serotonergic agents expand beyond psychiatry into pain management and infectious disease treatment. Current clinical decision support tools often exhibit inconsistencies in detecting these risks, leading to potential under-recognition of severe interactions.
Objectives:
This study aimed to detect and validate clinically significant DDIs associated with SS by integrating multisource real-world data. We sought to identify high-priority drug combinations, evaluate the concordance of major DDI checking tools, and highlight critical information gaps to improve patient safety strategies.
Design:
A multisource, retrospective study combining a systematic literature review, a disproportionality analysis of spontaneous adverse event reports, and a comparative cross-sectional evaluation of online DDI databases.
Methods:
This study employed a multisource approach to detect and evaluate SS-related DDIs. We integrated findings from a systematic literature review (up to June 2025), a disproportionality analysis using the FDA Adverse Event Reporting System (FAERS) with four frequency statistical models, and a comparative assessment of five major DDI checkers (Micromedex, Lexi-Interact, Epocrates, Medscape, and Drugs.com).
Results:
The systematic review identified high-risk interactions involving not only antidepressants but also non-psychotropic drugs such as linezolid, fentanyl, and methylene blue. FAERS data revealed strong signals for combinations such as linezolid-sertraline and fentanyl-venlafaxine, indicating a rising trend in SS reporting over the past two decades. Evaluation of DDI checkers demonstrated significant discrepancies in sensitivity and severity grading. Notably, 10.16% were not indexed in any of the five databases, including several clinically documented DDIs (e.g., aripiprazole-paracetamol and trazodone-pantoprazole), highlighting critical information gaps.
Conclusion:
SS remains a significant clinical risk driven by increasingly complex polypharmacy. Relying on a single DDI checker may lead to an underestimation of risk due to inconsistent indexing and severity ratings. Hospital pharmacists should integrate multisource data and maintain high clinical vigilance, particularly for “hidden” serotonergic agents such as certain opioids and antibiotics, to ensure medication safety.
Plain language summary
Serotonin syndrome is a rare but potentially life-threatening condition caused by an excessive buildup of serotonin—a chemical that helps transmit signals in the brain. This usually happens when a patient takes two or more medications that affect serotonin levels at the same time, leading to a dangerous drug-drug interaction. While these risks are well-known in psychiatry, many other common medications, such as certain painkillers and antibiotics, can also trigger this condition. This study was conducted to identify which drug combinations pose the highest risk and to see how well current digital tools (DDI checkers) warn doctors about them. We combined three types of evidence: a review of all existing medical research, an analysis of over 20 years of global safety reports from the FDA, and a comparison of five major drug-interaction databases used by healthcare professionals. Our findings show that reports of serotonin syndrome have been increasing. We identified several high-risk combinations, including interactions between antidepressants and “hidden” sources like the antibiotic linezolid or the painkiller fentanyl. Crucially, we discovered that no single digital tool is perfect; about 10% of the dangerous interactions we found in real-world reports were not listed in any of the five major databases. Furthermore, the databases often disagreed on how severe an interaction was. For patients and families, this research highlights that medication safety is complex. For healthcare providers, the results suggest that relying on just one computer system to check for drug risks may not be enough. We recommend that hospital pharmacists use multiple information sources and stay extra alert when patients are prescribed new types of antibiotics or painkillers alongside their regular medications. This proactive approach is essential to catching “hidden” risks and keeping patients safe.
Introduction
Serotonin syndrome (SS), or serotonin toxicity, is a potentially life-threatening clinical condition resulting from excessive serotonergic activity within the central and peripheral nervous systems. Over recent decades, the incidence of SS has risen significantly because of the escalating global use of serotonergic antidepressants and the expanding clinical application of other pro-serotonergic agents in fields such as pain management and infectious diseases. 1 While often mild in its initial presentation, SS can rapidly progress to severe complications, including life-threatening hyperthermia, confusion, hypertonicity, respiratory failure, coma, and death, with reported mortality rates remaining a concern for clinicians. 2
The pathophysiology of SS is most frequently triggered by drug-drug interactions (DDIs). These interactions typically involve the concomitant use of two or more medications that enhance serotonin neurotransmission through distinct mechanisms, such as inhibition of serotonin reuptake, decreased serotonin metabolism, or direct agonist activity at serotonin receptors. 3 Clinically significant DDIs, such as those between selective serotonin reuptake inhibitors (SSRIs) and monoamine oxidase inhibitors (MAOIs) or other psychotropic drugs, have been well-documented. Yet, emerging interactions such as the antibiotic linezolid, opioid analgesics such as tramadol and fentanyl, and certain antiemetics continue to pose challenges in clinical practice.4,5 Given the rising prevalence of polypharmacy, especially among psychiatric and pain management patients, the detection and prevention of such DDIs have become a crucial aspect of patient safety, with pharmacovigilance efforts highlighting the need for robust screening tools.
Extensive research has been conducted to elucidate the mechanisms and risk factors of SS, with a focus on identifying high-risk drug combinations. Pharmacovigilance studies have utilized databases such as the FDA Adverse Event Reporting System (FAERS) to uncover signals of SS, revealing associations with SSRIs and other medications through disproportionality analyses. 6 Similarly, systematic reviews also found some high-risk pairs, such as serotonin reuptake inhibitors with methylene blue. 7 Furthermore, evaluations of online DDI checkers, including Micromedex and Lexi-Interact, have also been widely applied in the detection of DDIs, including SS. 8 However, these studies often rely on single data sources, limiting their comprehensiveness. There is an urgent need for multidimensional approaches that integrate systematic reviews, large-scale databases, and tool validations to enhance the credibility of DDI signals.
Therefore, this study aims to perform a multisource analysis to detect and evaluate clinically significant DDIs associated with serotonin syndrome. By integrating a systematic review of existing literature, a disproportionality analysis of the FAERS database, and an assessment of five major online DDI checkers, we seek to provide a robust framework for identifying high-risk drug combinations and improving the accuracy of clinical risk assessments.
Methods
This study was conducted in three phases. First, we conducted a systematic review to identify studies reporting serotonin syndrome associated with DDIs between different medications. Second, we identified DDI signals using the FAERS database. Third, we evaluated the ability of five online DDI checkers to identify potential interactions between different medications identified in the first two steps. The reporting of this study conforms to the READUS-PV 9 statement. The READUS-PV checklist is attached as a Supplemental File.
Systematic literature review
We systematically searched MEDLINE (via PubMed), Embase, and Web of Science databases from inception to June 30, 2025. Search terms included combinations of “serotonin syndrome,” “serotonin toxicity,” “drug interaction,” “drug-drug interaction,” “adverse drug reaction,” and names of serotonergic agents (e.g., SSRIs, serotonin-norepinephrine reuptake inhibitors (SNRIs), MAOIs, tramadol, fentanyl, triptans, linezolid, and other medications with known serotonergic activity).
Studies were eligible for inclusion if they met all of the following criteria: (1) original research articles, including case reports, case series, observational studies, and clinical trials, with no restrictions on study design or comparator groups; (2) human participants of any age, sex, or clinical setting; (3) serotonin syndrome diagnosed following the concomitant use of two or more medications, with a plausible temporal relationship and clinical assessment supporting a DDI etiology; (4) sufficient clinical information to permit data extraction, including at minimum the implicated drug combination and clinical presentation or outcome; and (5) peer-reviewed journal publications with full text available in English. Studies were excluded if they met any of the following criteria: (1) non-original publication types, including narrative, scoping, or systematic reviews, editorials, commentaries, letters without original case data, conference abstracts, and gray literature; (2) non-human studies, including animal experiments and in vitro studies; and (3) cases in which serotonin syndrome was attributable to a single agent or in which a DDI etiology could not be reasonably established. Where available, we extracted information on patient characteristics, including age, sex, comorbidities, clinical setting, details of the implicated drug combination (drug names, doses, duration of use, and timing of co-administration), diagnostic criteria applied (e.g., Hunter Serotonin Toxicity Criteria or Sternbach criteria), management strategies, and outcomes.
Adverse outcomes were defined as cases of serotonin syndrome explicitly attributed by the study authors to a DDI, based on a plausible temporal relationship and clinical assessment. Both subjective symptoms (e.g., agitation and tremor) and objective signs (e.g., hyperreflexia, clonus, and fever) were included if linked to serotonergic toxicity. Reference lists of all eligible studies and relevant narrative or systematic reviews were manually screened to identify additional potentially eligible reports. The complete search strategy for each database is provided in Table S1.
Two investigators independently screened titles and abstracts, followed by full-text assessment of potentially eligible articles. Discrepancies at any stage were resolved through discussion or consultation with a third investigator. Data extraction covered study characteristics, implicated drug pairs or combinations, proposed mechanisms of interaction (pharmacokinetic (e.g., CYP450 inhibition) or pharmacodynamic (e.g., additive serotonergic effects)), diagnostic criteria used, symptom profiles, and clinical outcomes. Study quality and risk of bias were assessed independently by two reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports and Case Series, 10 as appropriate to the study design. Any disagreements were adjudicated by the third reviewer. This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 11 The PRISMA checklist is attached as a Supplemental File.
Disproportionality analysis
A retrospective, disproportionality, pharmacovigilance study was conducted from 2004 quarter 1 (Q1) to 2025 Q2 using the FAERS database to detect potential DDIs that increase the incidence of serotonin syndrome. The FAERS database consists of seven data tables: demographic and administrative information (DEMO), drug information (DRUG), the Medical Dictionary for Regulatory Activities (MedDRA) preferred terms (PTs) coded for the adverse event (REAC), patient outcomes (OUTC), report sources (RPSR), therapy start dates and end dates for reported drugs (THER), and indications for use (INDI). Each drug is assigned a code according to its association with adverse events: primary suspected drug (PS), secondary suspected drug (SS), concomitant drug (C), and interaction (I). In the FAERS database, duplicates and multiple cases were excluded following the FDA-recommended method, which involves selecting the latest FDA_DT when CASEIDs are identical and choosing the higher PRIMARYID when both CASEIDs and FDA_DTs are the same. 12 In this study, the targeted AE was serotonin syndrome, which was extracted from FAERS using the PT of serotonin syndrome (PT code: 10040108). In these cases, all drugs classified as PS, SS, C, and I were included in the process to investigate DDIs. For signal detection, we focused only on combinations of two drugs with three or more cases.
We used four frequency statistical models for the detection of DDI signals, including the Ω shrinkage measure, chi-square statistic, combination risk ratio (CRR), and additive model (AM; see Supplemental Appendix 1 for the calculation methods). This ensures that signals detected by multiple methods are less likely to be statistical artifacts. Ω shrinkage was prioritized as the baseline model due to its robustness at handling sparse data and its ability to minimize false positives. The additive model demonstrates high sensitivity in detecting DDI signals, which estimates the risk of co-medication in terms of the incidence of target AEs under different drug exposure scenarios for signal detection. The chi-square statistics model was used to detect potential DDIs signals, and the CRR model was proposed as a risk assessment method for the concomitant use of drugs at the frequency of two drugs reported simultaneously, assuming that the possibility of a drug interaction is a combined risk in the occurrence of AEs. 13 For signal confirmation, all four statistical models were applied, with a positive signal defined as one consistently detected by all four methods. Subsequently, both a four-by-two contingency table (Table S2) and a two-by-two contingency table (Table S3) were constructed. A positive signal was considered when all four models detected a positive signal. The criteria for signal detection for each statistical model are outlined in Table 1.
The signal detection criteria for each statistical model.
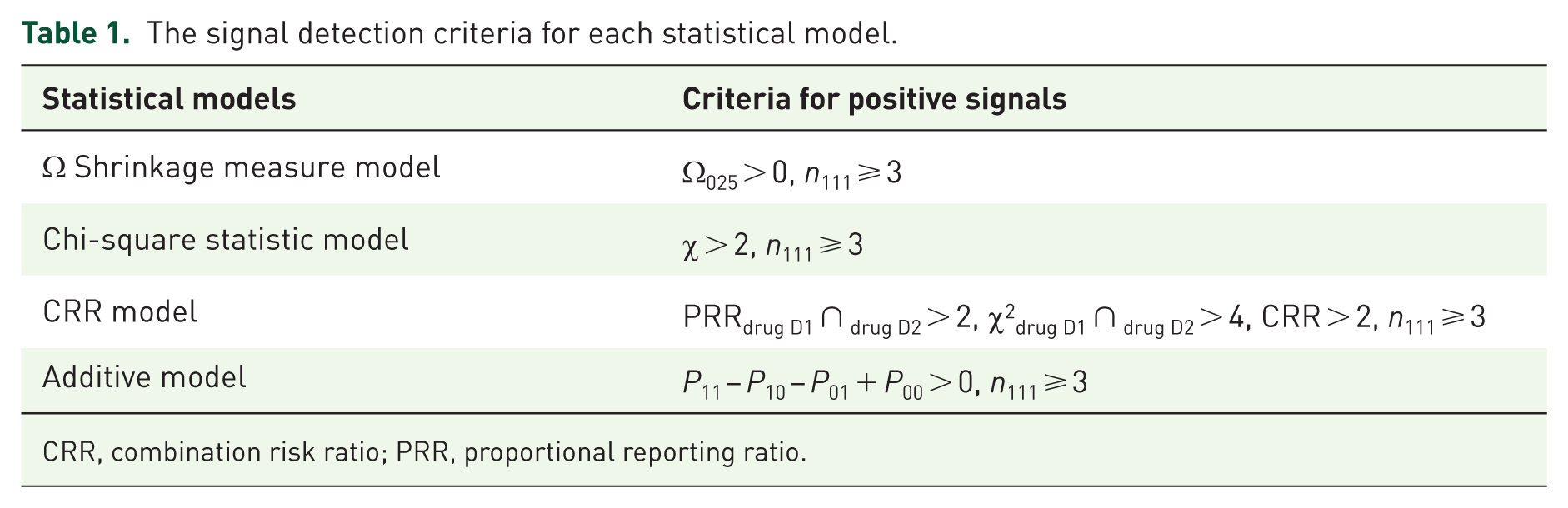
CRR, combination risk ratio; PRR, proportional reporting ratio.
Drug interaction checkers
The five online databases, including Micromedex, Drugs.com, Medscape, Epocrates, and Lexi-Interact, were used to validate DDI signals. Web scraping was conducted up to June 30, 2025. Each pair of medications identified in the first two steps was validated by all five online databases, which furnished in-depth details on the mechanisms of these potential DDIs and their respective severity levels. Although all online databases categorize DDI severity with similar groupings, they employ distinct labels. To address this, the severity classifications from various sources were unified into four standardized groups: severe (meaning contraindicated or major DDIs), moderate, minor, and unknown (Table S4). To enhance the clinical relevance of our findings, we included DDIs that were identified either through disproportionality analysis or systematic review.
Results
Identified DDIs from systematic review results
From the 9571 studies initially identified, 1146 duplicates were removed. After screening titles and abstracts, 231 studies underwent full-text evaluation, and among them, 158 studies met the inclusion criteria (Figure 1). These studies included 169 unique potential DDI pairs associated with SS (Table S5). Of the included studies, 143 were case reports, and 15 were case series. Among 158 studies, 24 studies involved two or more potential DDIs among multiple combinations. Among 169 unique potential DDI pairs, 30 DDI combinations involved two or more cases. The JBI quality scores indicated most case reports (114 of 143) and case series (13 of 15) had moderate to high methodological quality (scores ranging from 5 to 8). Patients in the included case reports and series ranged from 8 months to 90 years, comprising 108 females and 70 males. Most DDIs occurred in inpatient or emergency settings.
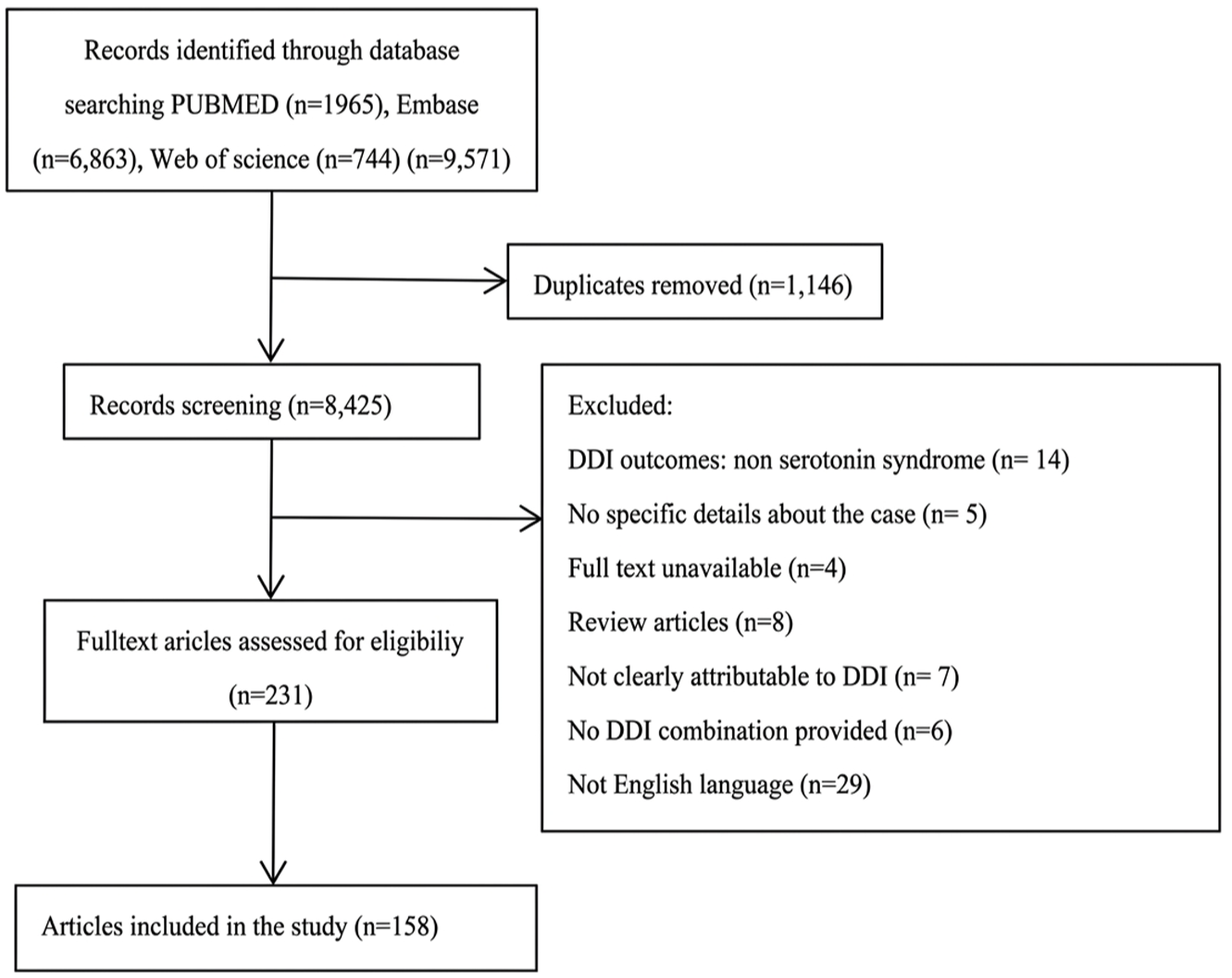
Flowchart of the systematic review.
Most studies identified DDIs primarily involving opioids, MAOIs, and antidepressants (especially SSRIs or SNRIs). The most frequently reported drug classification pairs with DDI were SSRIs-MOAIs (28 cases) and SSRIs-opioids (25 cases). For specific medications, SS associated with DDIs involving venlafaxine was the most common (30 cases), followed by linezolid (28 cases), sertraline (27 cases), and paroxetine (23 cases). The most frequently reported DDI pairs were linezolid-sertraline, linezolid-fluoxetine, and tramadol-paroxetine (four cases each), linezolid-venlafaxine, linezolid-escitalopram, moclobemide-clomipramine, methylene blue-citalopram, methylene blue-fluoxetine, linezolid-methadone, venlafaxine-lithium, and linezolid-fluoxetine (three cases each; Table S6). The outcomes of most cases were recovery or improvement in symptoms. Ten patients died, and six patients had deaths potentially related to DDIs, involving linezolid-methadone, paroxetine-risperidone, sertraline-phenelzine, tramadol-amitriptyline, sertraline-linezolid, and erythromycin-escitalopram/venlafaxine. In most cases, SS symptoms appeared 0.5 h to 7 days after taking the medications with DDI.
DDIs signals from the drug surveillance dataset
A total of 17,435 SS cases from 19,344,795 AE cases were included in the present study (Figure S1). Of the SS cases, 52.02% were female, and 35.89% were male, with an average age of 47.17 years (0–98 years), and 17.47% were over 65 years old. Serotonin syndrome proved to be a serious and potentially fatal condition: among the reported cases, 32.89% required hospitalization, 15.11% were classified as life-threatening, and 4.85% resulted in death. About 43.68% of these cases were reported from the United States (Table 2).
Characteristics of patients with SS in the FAERS database.

FAERS, FDA Adverse Event Reporting System; SS, serotonin syndrome.
A total of 279 drugs, each implicated in three or more reported cases, were identified across 17,036 serotonin syndrome cases. The most commonly reported medications (number of cases ⩾700) were sertraline (1188), venlafaxine (1080), fluoxetine (1141), duloxetine (978), bupropion (801), citalopram (791), tramadol (747), and paroxetine (725; Table S7). We evaluated the cases of SS for concomitant use of two of the 279 drugs, totaling 1319 medication combinations of DDIs; 499 medication combinations were reported in at least three cases. Two hundred twenty-seven DDI pairs were detected as positive by at least one statistical model. Among them, the additive model detected the most signals with 226 pairs (45.29%), followed by the CRR model with 143 pairs (28.66%), the chi-square statistic model, and the Ω shrinkage measure model, both with 103 pairs (20.64%; Table S8). Ninety-eight DDI pairs were simultaneously detected by four models (Figure 2). Antidepressants accounted for the majority of interactions (127 pairs after deduplication, 70 for SSRIs, 33 for SNRIs, 4 for TCAs, and 29 for other antidepressants), particularly fentanyl (22 pairs), sertraline (21 pairs), and venlafaxine (20 pairs), which were the most frequently involved medications in all 226 DDI pairs.
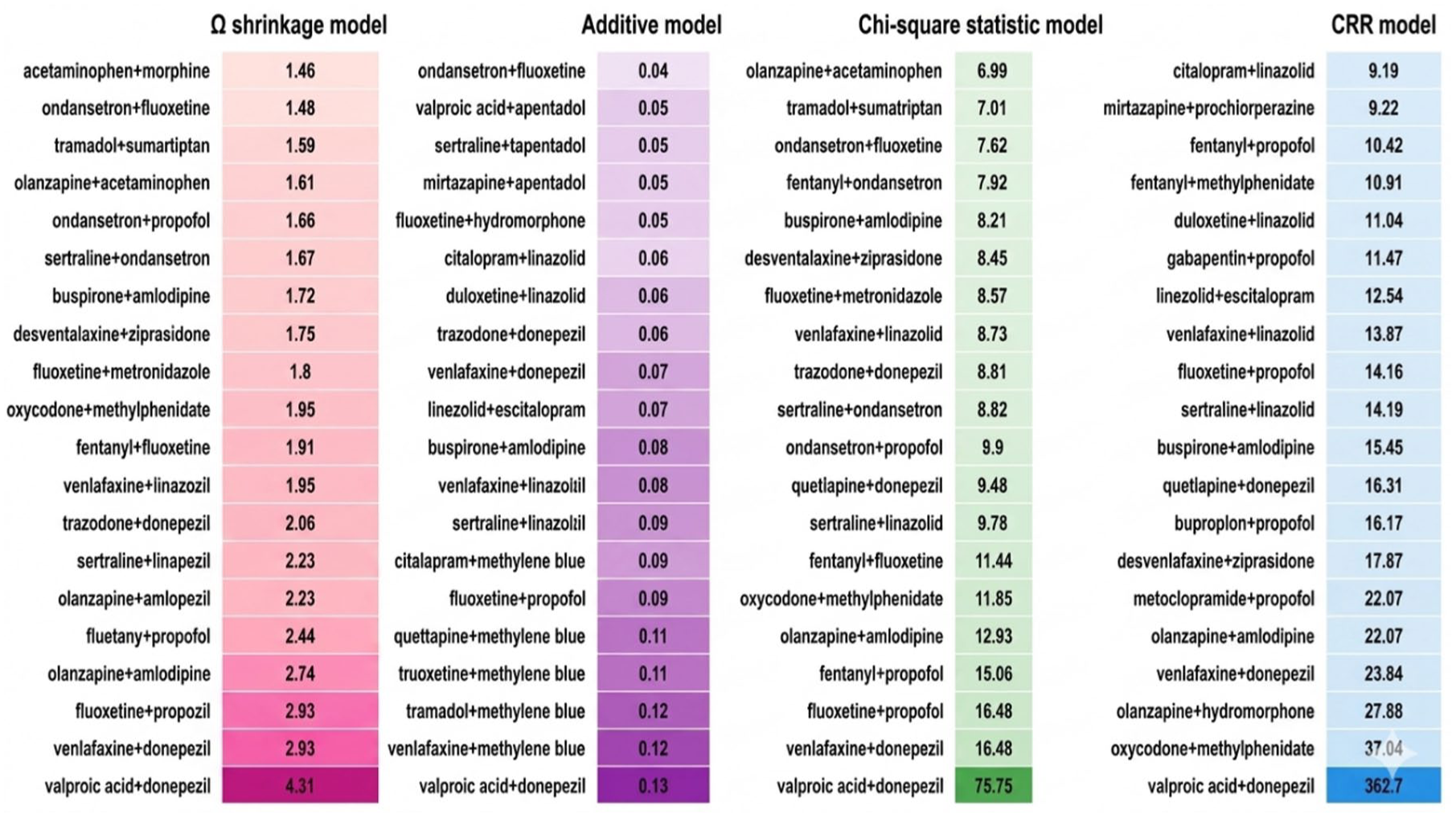
Top 20 drug-drug interaction pairs for serotonin syndrome ranked by signal strength in each of the four statistical models. Each panel is independently ranked in descending order by the corresponding model value.
The drugs with the most reported interaction cases were venlafaxine (294 cases), tramadol (279 cases), sertraline (277 cases), fentanyl (256 cases), fluoxetine (215 cases), linezolid (117 cases), escitalopram (113 cases), and quetiapine (112 cases). The medication pairs with the most reported interaction cases were duloxetine-tramadol (40 cases), fluoxetine-fentanyl (36 cases), and fentanyl-ondansetron (34 cases).
In the Ω shrinkage measure model, valproic acid-donepezil (Ω025: 4.31) showed the strongest interaction signal, followed by venlafaxine-donepezil (Ω025: 2.93) and fluoxetine-propofol (Ω025: 2.74). In the additive model, the strongest signal (showing interaction coefficients) was detected for valproic acid-donepezil (AM: 0.13), followed by venlafaxine-methylene blue (AM: 0.12) and methylene blue-tramadol (AM: 0.11). In the chi-square (χ) statistic model, valproic acid-donepezil also showed the strongest signal (χ: 75.75), followed by venlafaxine-donepezil (χ: 16.48) and fluoxetine-propofol (χ: 15.06). In the CRR model, valproic acid-donepezil still showed the strongest signal (CRR: 362.70), followed by oxycodone-methylphenidate (CRR: 37.04) and olanzapine-hydromorphone (CRR: 27.88; Figure 2).
Drug interaction checker analysis
In total, we identified 364 unique potential DDIs or DDI signals from both the systematic review and disproportionality analysis. Of these, 169 were identified exclusively through the systematic review, 226 from drug surveillance databases alone (three or more cases, and detected at least by one statistical model), and 31 were identified by both approaches. Then we used five DDI databases to verify the total of 364 DDI combinations. Two hundred and thirty-eight combinations indexed by Micromedex, 263 combinations indexed by Lexi-Interact, 291 combinations indexed by Epocrates, 239 combinations indexed by Medscape, and 288 combinations indexed by Drugs.com as of October 28, 2025 (Table S9). Severity classifications varied across five databases, underscoring inconsistency in DDI detection. In addition, 189 combinations were indexed, with 47 combinations (12.91%) classified as severe simultaneously by all five databases (Figure 3). Thirty-seven DDI pairs (10.16%) identified through both systematic review and disproportionality analysis were not indexed in any of the DDI databases (Figure 4).

Forty-seven drug-drug interaction pairs detected as severe by five drug-drug interaction checkers simultaneously.

Thirty-seven drug-drug interaction pairs identified through both systematic review and disproportionality analysis that were not indexed in any of the five drug-drug interaction databases.
Discussion
The present study offers a multidimensional perspective on the detection and clinical landscape of serotonin syndrome resulting from DDIs, integrating evidence from a systematic review, disproportionality analysis of the FAERS database, and evaluation of five major DDI checkers. Elli et al. 6 investigated the risk of SS among different SSRIs and assessed the influence of DDIs using the FAERS database, employing both the reporting odds ratio and the Ω shrinkage measure for signal detection. Building upon this foundation, our study extends the analytical framework by integrating four complementary frequency-based statistical models—the Ω shrinkage measure, CRR, chi-square statistic, and additive model—applied in combination, such that a DDI signal was only confirmed when detected by all four methods simultaneously. This multi-model confirmation approach substantially reduces the likelihood of false-positive signals and increases the robustness and reliability of the identified DDI pairs. Furthermore, by cross-validating signals against both a systematic literature review and five major DDI checker databases, our study provides a more comprehensive and multidimensional assessment of SS-related DDIs than has previously been reported.
Key findings indicate that while classic interactions, such as those between selective SSRIs and MAOIs, persist in clinical reports, emerging risks involve antibiotics such as linezolid and opioids such as tramadol and fentanyl. Linezolid, an oxazolidinone antibiotic used for resistant Gram-positive infections, possesses reversible non-selective monoamine oxidase inhibitory activity. 14 The frequent reporting of linezolid-induced SS and its association with high mortality in our reviewed cases, particularly when combined with venlafaxine or sertraline, suggests a dangerous “clinical blind spot” where specialists treating infections may be unaware of the patient’s psychiatric medication risks. 15 Furthermore, the prominence of opioids such as tramadol and fentanyl in both the systematic review and FAERS data underscores a growing intersection between pain management and serotonergic toxicity, which emphasizes the need for anesthesia-related vigilance. 16 Tramadol’s dual mechanism of μ-opioid receptor agonism and inhibition of serotonin and norepinephrine reuptake makes it a potent catalyst for SS when added to existing antidepressant regimens. 5
The DDIs identified in this study operate through two primary pathways. Pharmacodynamic interactions involve the additive or synergistic effects of multiple drugs on synaptic serotonin levels. This is best exemplified by the combination of an SSRI (which blocks reuptake) and an MAOI (which blocks degradation). However, our findings also highlight the critical role of pharmacokinetic interactions, particularly those involving the cytochrome P (CYP)450 enzyme system. 17 For instance, paroxetine and fluoxetine are potent inhibitors of CYP2D6. When these are combined with drugs like risperidone or certain opioids that are metabolized by CYP2D6, the resulting elevation in drug concentrations can precipitate toxicity. 18 The FAERS signal for quetiapine-venlafaxine combinations is particularly interesting; while quetiapine is not traditionally considered a highly serotonergic agent, it may contribute to SS via its 5-HT1A receptor affinity or through pharmacokinetic competition for CYP3A4 metabolism. 19
A core finding of this study is the low overlap (only 31 pairs) between the systematic review and the FAERS disproportionality analysis. This discrepancy is not necessarily a contradiction but rather a reflection of the unique strengths and biases of each data source.
Interpretation of the systematic review results reveals that 147 unique medication combinations were associated with SS, with linezolid-sertraline, linezolid-fluoxetine, and tramadol-paroxetine emerging as the most frequently implicated agents in four cases. This shift from traditional psychiatric polypharmacy to intersections with infectious disease and pain management reflects evolving prescribing patterns, where non-psychiatric specialists may overlook serotonergic risks. 20 The systematic review also noted that symptoms typically emerge within a very narrow window (30 min to 7 days). This rapid onset necessitates immediate patient education. Patients should be warned of SS symptoms—such as shivering, sudden sweating, or muscle twitches—whenever a new serotonergic agent or a CYP inhibitor is added to their regimen. Such temporal associations also emphasized the need for diagnostic tools such as the Hunter Serotonin Toxicity Criteria, which provide simple and accurate decision rules for identifying SS based on clinical manifestations such as hyperreflexia and clonus. 21 Systematic reviews capture high-quality, granular data, including dosages and temporal sequences. However, they are prone to publication bias, where clinicians are more likely to report “novel” or “extraordinary” cases (such as the erythromycin-escitalopram death found in our review) rather than well-known interactions like duloxetine-tramadol.
The FAERS data revealed a sobering mortality rate of 4.85% and a hospitalization rate of nearly 33%. This highlighted that SS is a high-stakes clinical event. In the disproportionality analysis, 98 medication pairs were detected as positive signals across all four statistical models, with antidepressants dominating (127 pairs). For a specific positive signal result, the more models that detected it, the more reliable the result is. Notably, pairs such as duloxetine-tramadol (40 cases), fluoxetine-fentanyl (36 cases), and fentanyl-ondansetron (34 cases) exhibited high reporting frequencies, suggesting under-recognized real-world morbidity. The low overlap (only 31 pairs) between systematic review and FAERS data highlights complementary strengths: literature captures granular, publication-biased cases, while FAERS offers breadth in spontaneous reporting. This discrepancy is not necessarily a contradiction but rather a reflection of the unique strengths and biases of each data source. FAERS analysis provides “real-world” breadth, identifying common patterns in large populations that might be considered too “routine” for individual case reporting. The high signal for duloxetine-tramadol in FAERS suggests that this combination is a frequent, perhaps under-recognized, cause of morbidity in the general population.
Comparative evaluation of five DDI checkers demonstrated inconsistencies, with only 47 combinations uniformly classified as severe among 246 identified DDIs. This variability contributes to alert fatigue, where discordant severity ratings desensitize clinicians, potentially overlooking interactions like those involving SSRIs and SNRIs. Thirty-seven pairs detected by reviews or FAERS were absent from all databases, which indicated that digital tools are struggling to keep pace with emerging evidence. This highlights a critical gap: DDI checkers are often conservative and may fail to alert clinicians to emerging risks until substantial post-marketing evidence accumulates. 22 As hospital pharmacists, this underscores the importance of clinical judgment and referring to primary literature rather than relying solely on automated alerts.
Broader implications of these results suggest that SS detection requires a multidimensional approach beyond traditional warnings. The expansion of serotonergic risks into non-psychiatric domains implies that primary care settings, where polypharmacy is common, must integrate proactive monitoring. 23 For instance, the frequent involvement of opioids highlights potential iatrogenic harm in pain management, consistent with pharmacokinetic-pharmacodynamic models of SS. Moreover, the study’s validation of DDIs flagged by at least three checkers, coupled with assessment against product summaries, provides a framework for prioritizing clinically relevant interactions, potentially reducing adverse events in vulnerable populations such as the elderly (17.47% of FAERS cases over 65). This aligns with efforts to improve drug interaction software performance, where specificity in alerting for major DDIs could mitigate over-alerting while capturing high-risk combinations. 24
Limitations
While this study is one of the most comprehensive of its kind, several limitations must be acknowledged.
First, the pharmacovigilance component relied on spontaneous adverse event reports from the FAERS, which is inherently subject to voluntary reporting bias. This dependency introduces the risk of both under-reporting and over-reporting, as not all adverse drug reactions occurring in clinical practice are submitted to the database. Furthermore, disproportionality analyses derived from spontaneous reporting systems are susceptible to confounding, most notably from concomitant medications that may not be fully or accurately captured in individual case safety reports. Consequently, the detected signals represent statistical associations rather than confirmed causal relationships, and the absence of a signal does not preclude the existence of a clinically meaningful interaction.
Second, the systematic review component was restricted to publications written in English, which may have introduced a language bias and potentially excluded clinically relevant case reports, observational studies, and pharmacovigilance data published in other languages. Given that serotonin syndrome cases and drug interaction profiles may vary across geographic regions and healthcare systems, this restriction may limit the representativeness and generalizability of the findings to non-English-speaking populations.
Third, the primary analytical focus on two-drug combinations may have inadequately captured the complexity of real-world prescribing practices. Polypharmacy scenarios involving three or more concomitant serotonergic agents—of which 32 such combinations were identified within the systematic review—were not fully examined within the disproportionality framework. The synergistic or additive serotonergic burden arising from multi-drug regimens may substantially differ from that predicted by pairwise interaction models, thereby limiting the generalizability of the findings to patients receiving complex, multi-drug therapeutic regimens.
Fourth, although statistical models incorporating the Ω shrinkage measure were employed to minimize false-positive signal detection—a recognized methodological strength of this study—the reliability of disproportionality estimates remains contingent on the volume of available reports for each drug pair. For drug combinations with sparse reporting, shrinkage-based corrections may not fully eliminate instability in signal detection thresholds, and the resulting estimates should therefore be interpreted with appropriate caution. In addition, disproportionality analyses do not account for differences in drug exposure prevalence across populations, which may further influence signal strength.
Finally, the cross-sectional evaluation of online DDI checkers was conducted at a single point in time, representing a static snapshot of database content. Given that DDI databases are continuously updated as new pharmacovigilance data, clinical evidence, and regulatory communications emerge, the findings regarding the indexing status of specific drug pairs may not accurately reflect the current capabilities of the evaluated platforms. The observed discordance between DDI checker outputs and the interaction pairs identified through systematic review and pharmacovigilance analysis should therefore be interpreted in the context of this temporal limitation, and periodic re-evaluation of DDI checker performance is recommended as evidence continues to evolve.
These limitations direct future research toward enhanced methodologies. Longitudinal studies should reassess DDI checkers periodically to track improvements in concordance and sensitivity. 25 Integration of machine learning into pharmacovigilance could refine signal detection, addressing biases in spontaneous reporting. 26 In the future, pharmacists and hospitalists must screen for SS risks when prescribing non-psychiatric drugs such as linezolid, tramadol, and triptans. For high-risk patients (e.g., those on multiple antidepressants), any new medication should be followed by 7 days of close clinical observation. Developers of Clinical Decision Support Systems (CDSS) should integrate pharmacovigilance signals (like those from FAERS) more rapidly into their alert logic to bridge the gap between real-world events and database updates.
Conclusion
This study enhances the understanding of serotonin syndrome-related DDIs, with direct relevance to clinical practice and pharmacovigilance. By integrating multisource data, it constructs a more comprehensive risk profile, supporting the adoption of combined screening tools to improve patient safety. The inconsistency of digital DDI checkers and the divergence between clinical reports and big data highlight the need for a more integrated approach. Future research should focus on developing real-time risk-stratification models that account for both the pharmacodynamic burden and the pharmacokinetic profile of a patient’s entire medication regimen.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261456115 – Supplemental material for Detection of clinically significant drug-drug interactions in serotonin syndrome: a multisource real-world data and pharmacovigilance study
Supplemental material, sj-docx-1-taw-10.1177_20420986261456115 for Detection of clinically significant drug-drug interactions in serotonin syndrome: a multisource real-world data and pharmacovigilance study by Shanshan Xu, Zhihui Song, Dong Wang, Yiman Li, Ente Wang, Jie Bai and Xinglong Wang in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.