
Abstract
Purpose:
To evaluate the effects of weight loss on heart rate (HR) and heart rate variability (HRV) parameters in overweight postmenopausal women.
Design and Methods:
Forty-nine overweight postmenopausal women with an average body mass index of 28.8 ± 1.9 kg/m2 underwent a 12-week dietary weight-loss programme. Accepted variables for characterization of HRV were analysed before and after the weight loss by 24-h ambulatory ECG monitoring; mean and standard deviation for the time between normal-to-normal complexes (MeanNN and SDNN, respectively), and the mean of standard deviations of normal-to-normal intervals for each 5-min period (SDNNindex). Baseline body fat mass (FM%) and changes in body composition was determined by dual X-ray absorptiometry. Before and after the weight-loss period, total abdominal fat, intra-abdominal fat (IAAT), and subcutaneous abdominal fat (SCAT) were measured by single-slice MRI at L3.
Results:
The weight loss of 3.9 ± 2.0 kg was accompanied by an improvement of HRV. SDNN increased by 9.2% (p = 0.003) and SDNNindex increased by 11.4% (p = 0.0003). MeanNN increased by 2.4%, reflecting a decrease in mean heart rate from 74.1 to 72.3 beats/min (p = 0.033). Systolic blood pressure (SBP) decreased by 2.7%, total cholesterol by 5.1% and high-sensitivity C-reactive protein (hsCRP) by 15.8% (p = 0.002). Improvements in SDNN and cholesterol were correlated with weight loss (r = −0.329, p = 0.024 and r = 0.327, p = 0.020, respectively) but changes in HR, SBP, and hsCRP were not. IAAT and the IAAT/SCAT-ratio were found to be negatively associated with HRV parameters but changes in body composition were not associated with changes in HRV.
Conclusions:
The observed improvement of HRV seems to be facilitated by weight loss. IAAT and the IAAT/SCAT ratio were found to be associated with low HRV.
Keywords
Introduction
Heart rate variability (HRV) reflects changes in autonomic nervous activity and reduced HRV has been shown to be an independent predictor of mortality in various patient populations, including healthy subjects 1 as well as in patients surviving myocardial infarction. 2 It is speculated that an increased sympathetic activity increases the risk of myocardial ischaemia and fatal arrhythmias. 3 Weight loss after dietary intervention or gastroplasty in morbidly obese patients has been shown to reverse the unfavourable impacts of obesity on cardiac autonomic nervous system modulation.4–7 Obesity-related illnesses present a major health problem and place a considerable burden on the economy by increasing rates of healthcare usage and associated costs. The EUROASPIRE Study Group found the prevalence of obesity (body mass index, BMI, ≥30 kg/m2) amongst patients with coronary artery disease (CAD) in 1997 to be 25.3%. 8 In the World Health Organization (WHO) European Region, the prevalence of obesity has risen 3-fold or more since the 1980s. The current age-adjusted prevalence of overweight (BMI ≥25 kg/m2) in women aged 25–64 in Europe is reported to be 50–60% and the age-adjusted prevalence of obesity (BMI ≥30 kg/m2) in the same group is 15–25%. 9
Incidence of ischaemic heart disease increases with age in both genders, yet it occurs a decade later in women, largely after menopause. During menopause, an altered distribution of fat tissue and weight gain often occur leading to development of risk factors consistent with the metabolic syndrome, which are hypertension, dyslipidaemia, chronic inflammation, sleep apnoea, insulin resistance, and type II diabetes. These changes often lead to pharmacological treatment with statins, anti-hypertensive, and anti-diabetic drugs. This group of moderately overweight postmenopausal women is a group not well examined, but of considerable size. Non-pharmacological interventions to improve risk factor status and prevent manifest cardiovascular disease in these subjects would be of great interest.
In light of this, we aimed to assess the effects of weight loss and changes in body fat distribution achieved during a 12-week dietary weight-loss programme on HRV parameters, blood pressure, cholesterol, and inflammatory as well as metabolic markers, in moderately overweight postmenopausal women.
Methods
This study is part of the Copenhagen Obesity Risk Assessment study. The COBRA-study is a 16-week randomized, double blind, parallel dietary intervention trial that aimed to address the effect of a daily intake of 15.7 g trans-fatty acids in overweight but otherwise healthy postmenopausal women. Results from intervention with trans-fatty acids have been published previously.10–12 The subjects were recruited from Copenhagen, Denmark, and the surrounding areas by advertising in the local media. After the 16-week intervention, the women underwent a 12-week weight-loss programme with biweekly consultations with a clinical dietician. The dietary instructions aimed at an energy deficit of 2500 kJ/day. The subjects were encouraged to increase the level of physical activity during the weight-loss period; however, the activity level was not assessed. Inclusion criteria were: postmenopausal women 45–70 years of age with BMI between 25 and 32 kg/m2 and a waist circumference of ≥80 cm. Exclusion criteria were: smoking within the prior 6 months, systolic blood pressure (SBP) >160 mmHg or/and diastolic blood pressure >100 mmHg at the screening visit, total cholesterol >7.0 mmol/l, triglyceride >3.0 mmol/l, diabetes, and known cardiovascular disease. Before and after the intervention and after the 12-week weight-loss programme, HRV was measured by 24-h ambulatory electrocardiography (ECG) monitoring by use of three-channel ‘Rozinn’ digital recorders (ScottCare Corporation, Cleveland, Ohio, USA). Analyses were performed using Holter for Windows+, Analysis and Review Station by trained personnel with no access to the participants’ files. The following time-domain variables were assessed: mean and standard deviation of all normal RR intervals (MeanNN and SDNN, respectively) and the mean of standard deviations of normal-to-normal intervals for each 5-min period (SDNNindex). In these terms, MeanNN represents the average 24-h heart rate (HR): i.e. 60,000/MeanNN = average 24-h HR in beats/min. SDNN summarizes both long- and short-term HRV and can be considered as a broad-band measure of autonomic balance while SDNNindex represents short-term HRV. Bodyweight and blood pressure were measured by standard procedures and fasting blood samples were collected before and after the 12-week weight-loss programme and analysed for plasma cholesterol, serum high-sensitivity C-reactive protein (hsCRP), and serum adiponectin. To determine baseline body fat mass (FM%) and changes in body composition, whole body dual X-ray absorptiometry was performed. Before and after the weight-loss period, total abdominal fat (TAF), intra-abdominal fat (IAAT), and subcutaneous abdominal fat (SCAT) were measured by single-slice magnetic resonance imaging (MRI) at the level of L3.
Statistical analysis
Statistical software MedCalc (version 11.5.1, MedCalc Software, Mariakerke, Belgium) was used for statistical analyses and graphics. For normally distributed variables, mean and standard deviations are presented, and for non-normally distributed variables, median and interquartile range (Q1–Q3) are presented. Parameters before and after the weight-loss period were compared using Student paired t-test. Wilcoxon signed-rank test was used to evaluate the changes in non-normally distributed variables from baseline to after the weight-loss period. The associations between changes in parameters (delta of variables) of interest from baseline to after the intervention were evaluated by using Spearman’s coefficient. Logistic regression analysis was used to evaluate the covariate-adjusted associations between weight loss and changes in parameters of interest. In forward selection procedures, p < 0.05 was used to enter and stay in the model. p-values <0.05 were considered statistically significant.
Results
Variables at baseline and after the 12-week weight-loss programme
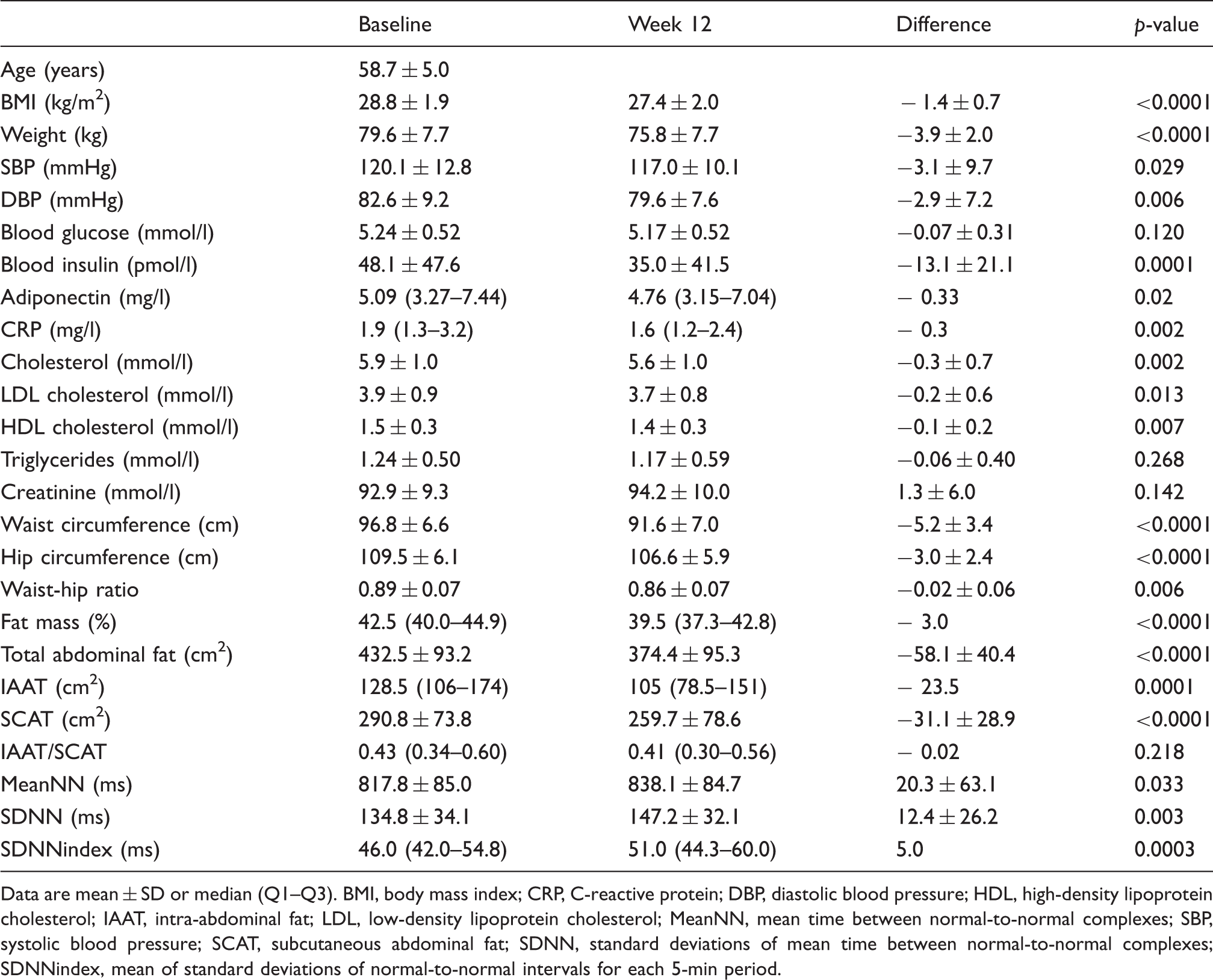
Data are mean ± SD or median (Q1–Q3). BMI, body mass index; CRP, C-reactive protein; DBP, diastolic blood pressure; HDL, high-density lipoprotein cholesterol; IAAT, intra-abdominal fat; LDL, low-density lipoprotein cholesterol; MeanNN, mean time between normal-to-normal complexes; SBP, systolic blood pressure; SCAT, subcutaneous abdominal fat; SDNN, standard deviations of mean time between normal-to-normal complexes; SDNNindex, mean of standard deviations of normal-to-normal intervals for each 5-min period.
Heart rate variability parameters
Forty-six study subjects had acceptable Holter recordings for HRV measurements both before and after the weight-loss period. Three subjects were excluded from analyses because of substandard quality of recordings. The weight loss was accompanied by a significant improvement of HRV parameters (Table 1). SDNN increased by 9.2% (p = 0.003) and SDNNindex increased by 11.4% (p = 0.0003). MeanNN increased from 818 ± 85 ms to 838 ± 85 ms (p = 0.033), which reflects a decrease in mean heart rate from 74.1 beats/min to 72.3 beats/min (increase in MeanNN of 2.4%).
Systolic blood pressure, C-reactive protein, and cholesterol
A significant decrease of 2.7% in SBP was observed (p = 0.029) (Table 1). hsCRP decreased from median 1.9 µg/l to 1.6 µg/l (p = 0.002). Total cholesterol decreased by 5.1% (p = 0.002). Low-density lipoprotein (LDL) cholesterol decreased by 5.1% (p = 0.013) and high-density lipoprotein cholesterol decreased by 6.7% (p = 0.007).
Changes in variables of body composition
As expected, FM% decreased significantly from median 42.5% to 39.5% (p < 0.0001), representing a decrease of 7.1%. MRI before and after the weight loss revealed that TAF decreased by 13.4%, IAAT by 18.3%, and SCAT by 10.7%. The IAAT/SCAT ratio, which is a measure of amount total fat deposited as IAAT, did not change during the weight-loss period (p = 0.218).
Correlation analyses between variables of body composition and HRV
At baseline, SDNN was found to be negatively associated with the IAAT/SCAT ratio and the same significant association was found between SDNN and IAAT/SCAT ratio after the weight-loss period, indicating a correlation between the distribution of body fat and SDNN (Figure 1). Furthermore, we found SDNN at baseline and after weight loss to be negatively correlated with IAAT in rank correlation analyses (r = −0.341, p = 0.02; r = −0.459, p = 0.001, respectively) suggesting that the greater amount of fat deposited intra-abdominally, the lower SDNN. No significant association was seen between SDNN and FM%, TAF, or SCAT (data not shown). SDNNindex was also found to be negatively associated with IAAT at baseline and after the weight-loss period (r = −0.377, p = 0.013; r = −0.351, p = 0.016, respectively). SDNNindex was also negatively correlated with the IAAT/SCAT ratio, both at baseline and after the 12 weeks of calorie restriction, (r = −0.309, p = 0.039; r = −0.543, p = 0.0001, respectively). As with SDNN, SDNNindex was not correlated with FM%, TAF, and SCAT (data not shown).
Association between SDNN and IAAT/SCAT ratio at baseline (A) and after the 12-week weight-loss period (B). IAAT, intra-abdominal fat; SCAT, subcutaneous abdominal fat; SDNN, standard deviations of mean time between normal-to-normal complexes.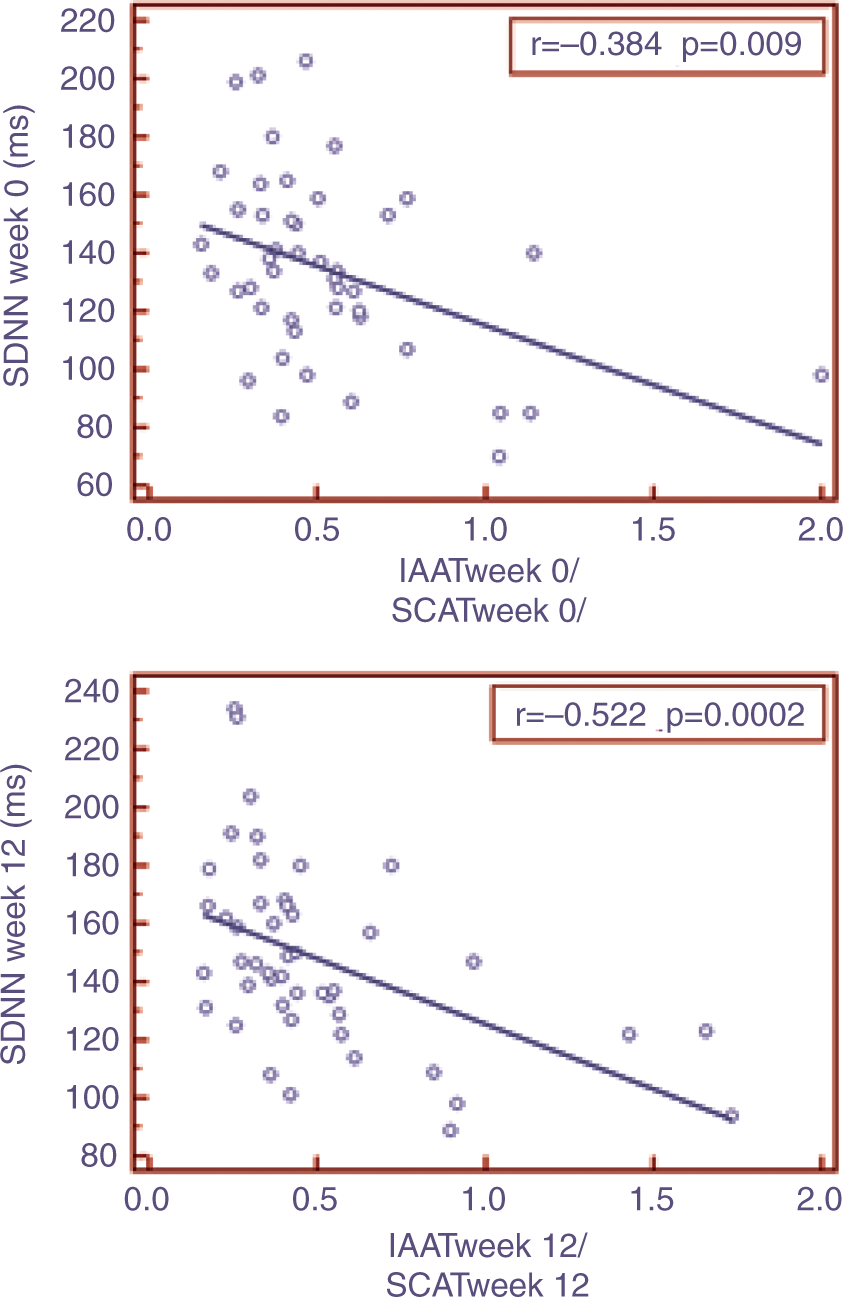
Changes in HRV, haemodynamic, and metabolic parameters during weight loss
In rank correlation analyses, the increase in SDNN was associated with the observed weight loss, (r = −0.329, p = 0.024; Figure 2). The correlation between MeanNN and weight loss and SDNNindex and weight loss did not reach statistical significance. The increase in SDNN was not correlated with the decrease in IAAT (r = 0.002, p = 0.990) and neither was the increase in SDNN correlated with changes in the IAAT/SCAT ratio (r = 0.072, p = 0.645). The same was found between delta SDNNindex as well as delta MeanNN: no correlation with changes in IAAT and the IAAT/SCAT ratio (data not shown).
Relationship between deltaWeight and deltaSDNN. SDNN, standard deviations of mean time between normal-to-normal complexes.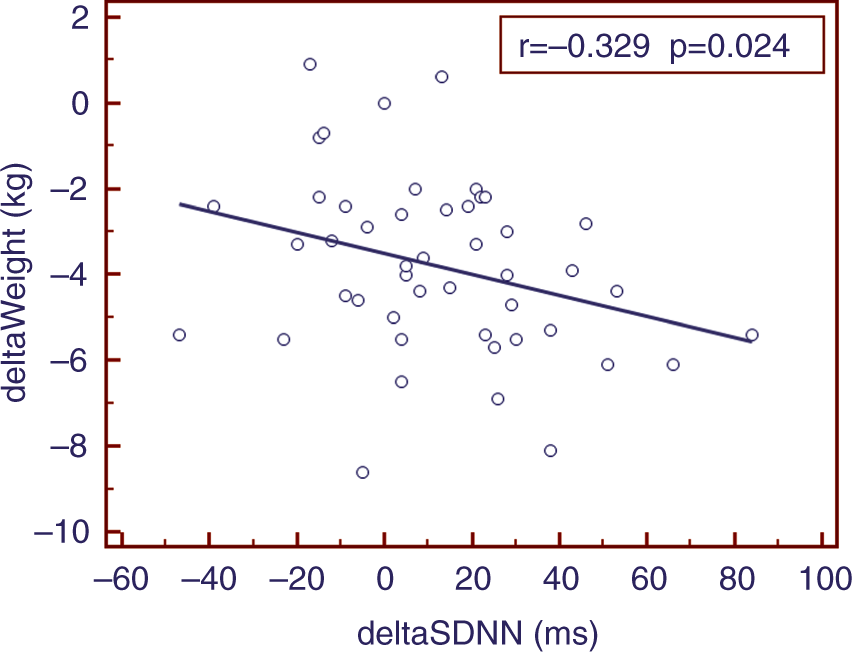
Correlation coefficients from multiple regression analyses with deltaSDNN as the dependent variable
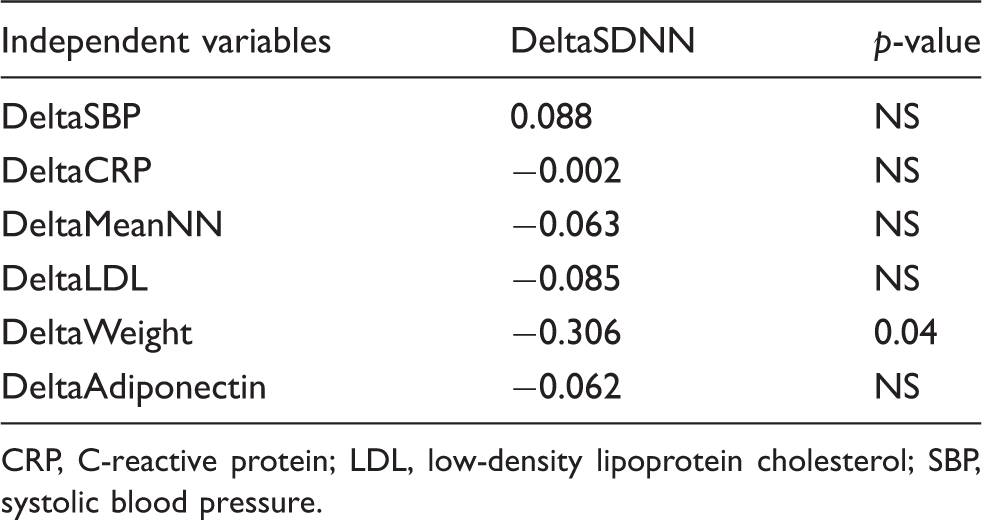
CRP, C-reactive protein; LDL, low-density lipoprotein cholesterol; SBP, systolic blood pressure.
Discussion
Increase in risk of CAD has been observed in women following surgical or natural menopause. This increase in prevalence of CAD could be related to a multitude of metabolic and hormonal changes occurring during the menopausal transition and early postmenopause, e.g. increased abdominal fat deposition leading to the metabolic syndrome. 13 In this study we demonstrate that the distribution of fat has a great impact on HRV. Both IAAT and the IAAT/SCAT ratio measured by single-slice MRI were associated with low HRV. TAF, SCAT, and FM% did not seem to affect HRV. These results suggest that deposition of IAAT causes increased sympathetic activity and decreased HRV. This connexion is in agreement with the widely accepted opinion that increased deposition of visceral fat causes increased risk of cardiovascular morbidity and mortality.14,15 Even though we found an association between IAAT as well as the IAAT/SCAT ratio and HRV parameters at baseline and also after the weight-loss period, we were not able to demonstrate a significant association between changes in fat distribution variables and changes in HRV parameters. Why this is so is not obvious, but it is possible that delta weight loss in this setting is a better ‘estimate’ of changes in body composition because it also reflects changes in intramuscular fat. It is also possible that the observed changes in body composition were too small to cause significant changes in HRV parameters. This statement is supported by the fact that the IAAT/SCAT ratio did not change significantly during the weight-loss period. However, we did find that a weight loss of only 5% of bodyweight was accompanied by a significant improvement of SDNN. The increment of HRV after weight reduction is an interesting observation because it may represent a correction of autonomic imbalance. Whether this imbalance is just a marker of low fitness, or whether it is a risk factor by itself, is unknown.
These findings support conclusions from other trials examining obese subjects before and after weight reduction. A study by Karason et al. 5 found that both short-term HRV, reflecting vagal activity, and long-term HRV, reflecting sympathetic activity, are altered in obese subjects. They also found that a mean weight loss of 32 kg (28% of bodyweight) normalized the observed imbalances in the autonomic nervous system. Other trials examining obese subjects also found an improvement of HRV4,7 and heart rate recovery 16 during weight loss. The current findings are consistent with a study by Astrup et al., 17 which demonstrated that the sympathetic nervous activity was altered in overweight persons and that it seemed to be further increased by a high-carbohydrate diet. This observation of increased norepinephrine response as a reflection of sympathetic nervous activity persisted after weight reduction. 18 Common to most of the studies in this field is that they have examined morbidly obese subjects with weight reductions of more than 10% of bodyweight. The women in the present study are only moderately overweight with a body mass index between 25 and 32 kg/m2. This population is traditionally not considered to be at high risk of developing CAD.
The observed decrease in HR in this study was not directly correlated with weight loss. Changes in SDNN, on the other hand, was correlated with weight loss, also after adjustment for the changes in HR. This is quite an interesting aspect because it illustrates that the increase in HRV is not solely caused by a decrease in HR. It is well established that overweight and obesity per se increases HR and that HR decreases during weight loss. 19 It is also widely accepted that an increased resting HR, reflecting an increased sympathetic and decreased parasympathetic nervous activity, is associated with increased mortality and morbidity. 20
We found no significant increase in adiponectin concentrations. These findings are in contrast with those of Yang et al., 21 who observed a 46% increase in adiponectin in obese patients who underwent partial gastrectomy, resulting in a weight loss of 22% of bodyweight. Other studies with weight reductions of more than 10% of bodyweight have reported similar results. 22 However, it must be noted that no significant changes in adiponectin were observed in other studies after minor/moderate weight reductions.23,24 Thus, it seems likely that only large weight reductions will result in increase in adiponectin.
The results of this study suggest non-pharmacological treatment when evaluating moderately overweight postmenopausal women. In an era where the medical industry advertises on a huge scale for pharmacological intervention and captures the attention of both physicians and patients, focusing on non-pharmacological therapy and its beneficial effects seems necessary. Weight loss through calorie restriction, increased physical activity, and cognitive therapy may be sufficient intervention in many cases and is accompanied by other desirable effects on health status, such as improved quality of life and wellbeing. It is well known that psychological factors affect HRV parameters 25 and it is possible that increased psychological wellbeing during the weight-loss period has contributed to the observed changes in HRV. A study by Bonnemeier et al. 26 found that HRV decreases with increasing age. They found that HRV decreases gradually, reaching 50.2% (SDNNindex) and 66.3% (SDNN) in the sixth decade compared to baseline values measured in the second decade. It is possible that by keeping a normal bodyweight throughout life and especially through menopause, this decrease in HRV can be diminished.
While documenting positive effects of weight loss in overweight persons, another challenge presents itself. Keeping the achieved weight loss is difficult and little is known about factors associated with successful weight-loss maintenance. A study by Svetkey et al. 27 investigating a group of overweight adults who had lost 8.5 kg (mean) during a 6-month weight-loss programme found that monthly brief personal contact provided modest benefit in sustaining weight loss. However, although weight regain with personal-contact intervention was statistically less than weight regain in the self-directed group, the mean effect being a modest 1.5 kg at the end of the study. Preventing weight regain is extremely challenging and further studies in this field are therefore needed to understand the aspects of successful weight-loss maintenance.
Limitations
Study subjects were moderately overweight postmenopausal Caucasian women, thus the data may not be valid for other ethnic groups and men. Lack of a control group with no weight loss is a major limitation of the study. Nevertheless, it is well known that without any dietary instruction no weight loss occurs, so any placebo effect for the weight-loss effect is at best minor. However, it is possible that the women were more relaxed and comfortable during the third 24-h Holter monitoring compared to the second 24-h Holter monitoring and that the sympathetic activity therefore was higher during the second monitoring, which may potentially have affected the results. Lack of evaluation of physical fitness at baseline and lack of registration of physical activity during the weight-loss period is also a limitation. Increased physical fitness is well known to influence HRV and inflammatory as well as metabolic markers.
This study included 49 women of whom three had unacceptable Holter recordings, resulting in 46 women being included in the statistical analyses. We did not find any association between changes in HRV parameters during weight loss and changes in haemodynamic and metabolic parameters and it is possible that the current study is underpowered to illustrate a weak but true association.
Conclusions
A modest weight loss of 5% of bodyweight achieved by diet intervention in moderately overweight postmenopausal women causes a significant decrease in SBP, hsCRP, and total cholesterol as well as LDL cholesterol and improves parameters of HRV. The observed increase in SDNN seemed to be directly facilitated by weight loss. IAAT and the IAAT/SCAT ratio were found to be associated with low HRV but the changes in fat composition were not found to be significantly correlated with changes in HRV parameters.
Footnotes
Acknowledgements
This study has been presented at the 2011 ESC congress in Paris during an oral abstract session.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.