
Abstract
Background:
The European Heart SCORE model constitutes the basis for national guidelines for primary prevention and treatment of cardiovascular disease (CVD) in several European countries. The model estimates individuals’ 10-year CVD mortality risks from age, sex, smoking status, systolic blood pressure, and total cholesterol level. The SCORE model, however, is not mathematically consistent and does not estimate all-cause mortality. Our aim is to modify the SCORE model to allow consistent estimation of both CVD-specific and all-cause mortality.
Methods:
Using a competing risk approach, we first re-estimated the cause-specific risk of dying from cardiovascular disease, and secondly we incorporated non-CVD mortality. Finally, non-CVD mortality was allowed to also depend on smoking status, and not only age and sex. From the models, we estimated CVD-specific and all-cause 10-year mortality risk, and the expected residual lifetime together with corresponding expected effects of statin treatment.
Results:
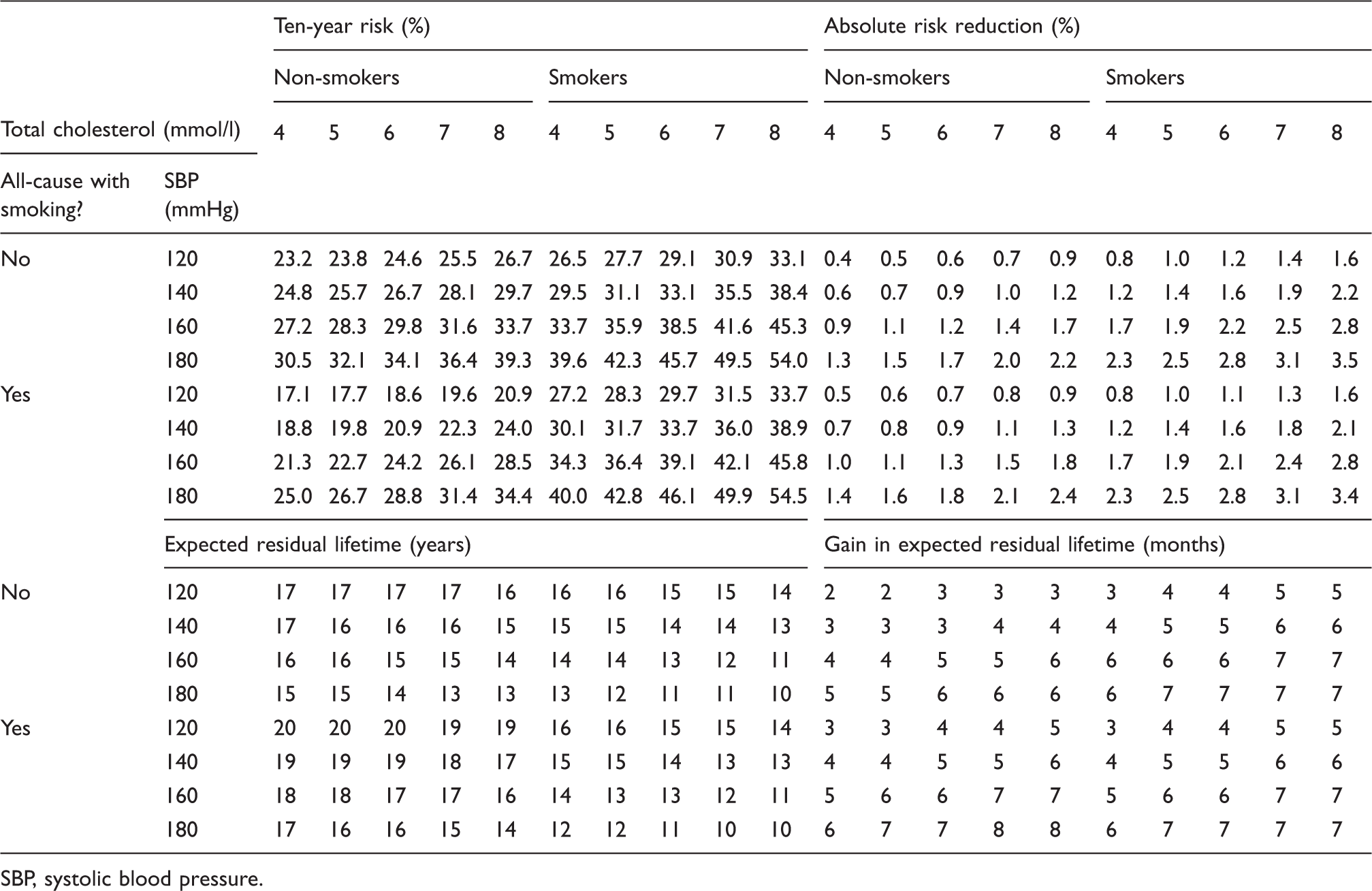
The modified model provided CVD-specific 10-year mortality risks similar to those of the European Heart SCORE model. Incorporation of non-CVD mortality increased 10-year mortality risks, in particular for older individuals. When non-CVD mortality was assumed unaffected by smoking status, the absolute risk reduction due to statin treatment ranged from 0.0% to 3.5%, whereas the gain in expected residual lifetime ranged from 3 to 11 months. Statin effectiveness increased for non-smokers and declined for smokers, when smoking was allowed to influence non-CVD mortality.
Conclusion:
The modified model provides mathematically consistent estimates of mortality risk and expected residual lifetime together with expected benefits from statin treatment.
Keywords
Introduction
Chronic diseases such as cancer, diabetes, respiratory, and cardiovascular diseases (CVD) account for more than 60% of mortality in Denmark1,2 and the proportion is probably about the same in most industrialized countries. A range of interventions are available to prevent such diseases, postpone their adverse consequences, or treat them once they have become symptomatic. Lifestyle changes, surgery, and pharmaceuticals are among relevant interventions. Increasingly, guidelines have been developed to assist patients and doctors in making decisions about such interventions. In the area of CVD, there are European guidelines 3 as well as national ones.4–12 These guidelines either use the SCORE model directly or a national modification of the SCORE model to assist clinicians in preventive decisions.13,14 The models typically predict the 10-year risk of a fatal CVD on the basis of gender, age (40–65 years), smoking habits, level of total cholesterol, and systolic blood pressure (SBP). The SCORE model is intended to guide decisions with respect to interventions for patients without previous CVD events.
Even though the SCORE model and similar models may represent important steps forward in the management of patients at risk of CVD, they have limitations. First, these models only present CVD mortality risk. Presumably, doctors and their patients are interested in the total mortality risk when making decisions, not only CVD mortality. 15 Second, in their current form they only present absolute risks and not other risk formats, such as the expected residual lifetime that may be easier to understand.16,17 Third, the current SCORE model does not provide estimates of benefits from interventions directed towards CVD risk factors. A major problem of the SCORE model is that it is based on an inconsistent mathematical model, since it in principle allows the risk of cardiovascular death to exceed one. This is because it estimates the CVD mortality risk on the basis of CHD risk and non-CHD risk without accounting for the fact that once a person is dead from one of the two types of risks, the person cannot die from the other (the issue of competing risks).
In this paper we propose modifications to the SCORE model in order to allow estimation of expected residual lifetime, while maintaining congruence with the present SCORE model in the sense that we preserve comparable estimates of the 10-year risks of death from cardiovascular disease. The first modification is to introduce a competing risk approach to make the cause-specific survivor function of SCORE consistent. This implies that the risk of dying from CVD can never exceed 100%, even among those with extremely high risk factor levels, or when computed as 20-year risks, 30-year risks, and so forth. The second modification is to extend the model by including non-cardiovascular mortality rates, again with a competing risk approach. The final modification is to incorporate an effect of smoking into the non-CVD mortality. We illustrate how the new models can be flexibly used to provide 10-year risks of dying, as well as credible estimates of expected residual lifetimes.
Methods
Baseline risk and expected residual lifetime
In the SCORE model, the risk of dying from coronary heart disease (CHD) is modelled by a Weibull distribution, where the survivor function is weighted with a function of the risk factors. The Weibull survivor function is parameterized as



To compute the overall 10-year risk of dying from either CHD or non-CHD CVD, the risks of dying from either are summed. While this definition may be useful for estimating 10-year mortality, it is straightforward to see that it suffers from two fundamental problems if the issue is to estimate average residual lifetime. First, the overall risk of dying will eventually exceed 1 since the risk at time t is given by
Thus, this ‘risk’ approaches 2 as t goes to infinity. Secondly, the estimated risk is, by definition, cause-specific, and thus ignores any other causes of death. For patients at high risk of death from other causes (e.g. elderly patients), this means that patients and doctors will underestimate the actual mortality risk when using the SCORE model, and estimates of residual expected lifetime will be unrealistically high.
As an alternative, we first consider a mathematically consistent model that allows different causes of death. This implies that an individual may die from only one of the different causes, whichever one occurs first. If we only consider the risk of dying from CHD or non-CHD CVD, and as before consider them to be independent, then the risk function is given by the following competing risk expression:
19

The risk function R(t) is consistent as it cannot exceed one. To evaluate its suitability as an estimate of the 10-year risks of CHD and non-CHD CVD, we compare the 10-year risk estimates obtained with Risk(t) and R(t) for the values of age, cholesterol, blood pressure, and smoking, reported by Conroy et al., 18 as well as with the actual values used by Danish GPs as proposed in the Danish guidelines.5,11
Secondly we extend the model by including information on mortality due to other causes for the Danish population. Using mortality data from Statistics Denmark, we calculated the number of non-cardiac deaths by subtracting the number of deaths attributable to CHD and non-CHD CVD from total deaths for each 5-year age category, by sex.1,2 When combining this with the population size in each age category, we could estimate the mortality rate, Logarithmic mortality rates estimated for non-cardiovascular deaths, Denmark 2006.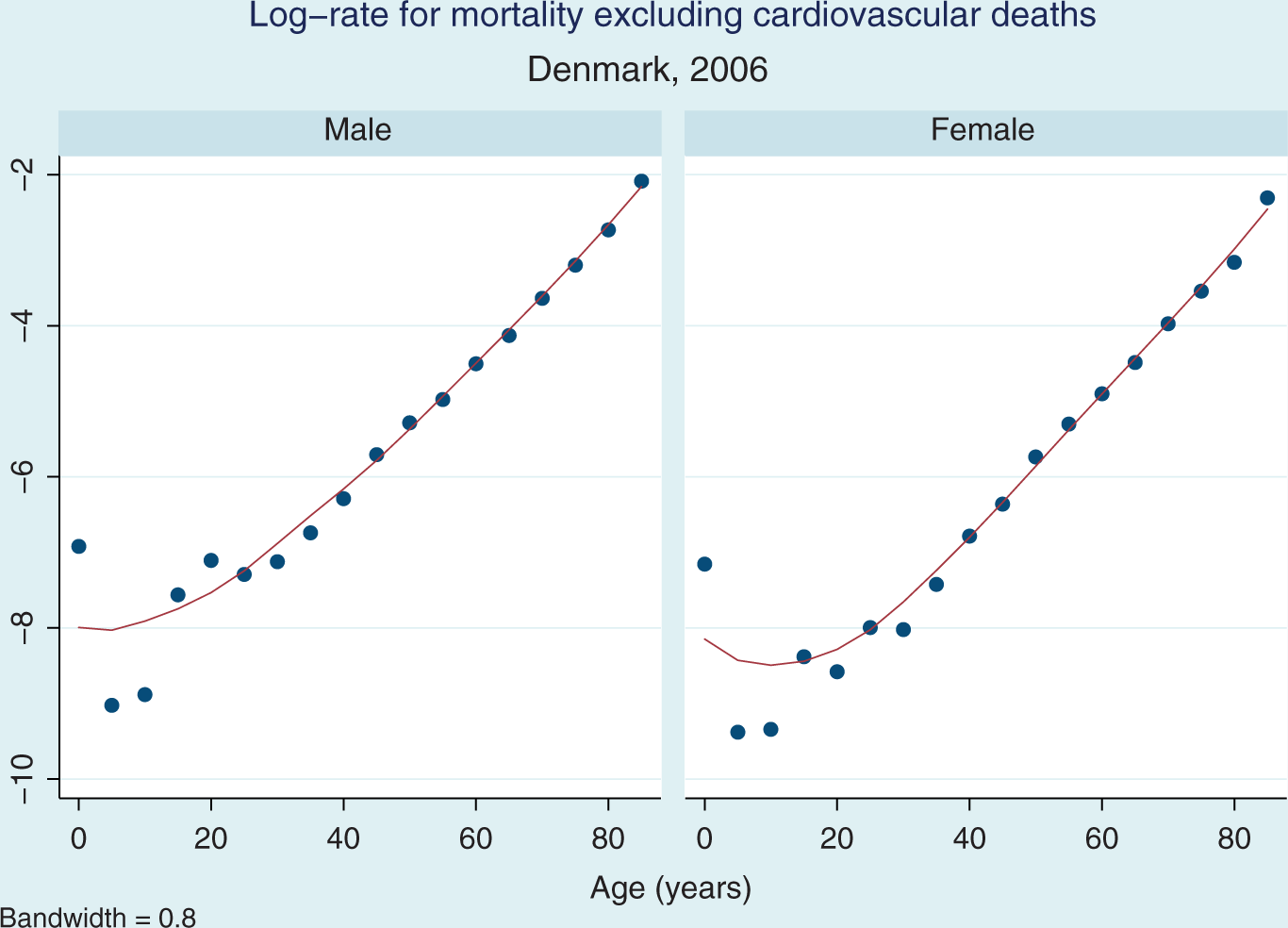
We exploited this relationship to facilitate subsequent computations and used linear regression to fit a straight line to the log-rates for ages above 40. For males, the fitted line had an intercept of −9.9 and a slope of 0.086. For females, the corresponding line had an intercept of −10.6 and a slope of 0.091.
This estimate of the non-CVD mortality was then combined with the cause-specific mortality as described by the modified Heart SCORE model developed above (Equation 1.1), although we now assumed that death resulted from one of three (rather than two) causes: non-CVD mortality, CHD, or non-CHD CVD. The overall survivor function is then a product of the three corresponding survivor functions. To make the estimated 10-year risks and residual lifetime expectancies as comparable as possible to the original Heart SCORE estimates, we chose not to let non-CVD mortality be influenced by risk factors involved in the SCORE model: i.e. smoking, blood pressure, and cholesterol level.
From this overall survivor function S(t), it is possible to compute the 10-year mortality risk, as well as the expected residual lifetime. For example, the risk of dying before age 70 of a 60-year-old is given by

As the survivor function is relatively simple and explicitly defined, the 10-year risk can be computed directly, but this is not the case for the integral used to compute the expected residual lifetime. The survivor function is, however, smooth and vanishing for survival times over 120 years, which allowed us to use a simple midpoint numerical integration technique over the finite interval from current age to 120.
In an extension of the model, we let the hazard rate for the non-CVD mortality depend on smoking, such that smokers had a doubled hazard rate compared to non-smokers for all ages and both genders. 20 We used Danish smoking prevalences in sex and age categories (35–44, 45–54, 55–64, 65–74, 75+ years) 21 and assumed that the overall non-CVD mortality was the same as above. Again we exploited that the log mortality rates increase approximately linearly with age above age 40, and fitted a line for smokers and non-smokers for each sex, respectively. The estimates are given in the Appendix (available online).
Treatment benefits
In order to provide estimates of the benefit obtained from treatment with a statin, we assumed that adherence to statin treatment was lifelong and led to a 30% reduction in cause-specific hazard rates for both CHD and non-CHD CVD. 22 We only performed the analysis for statins because we needed the data for an ongoing clinical trial (trial registration NCT01414751). This allowed computation of 10-year mortality risks and residual lifetime expectancies with treatment, which could be compared to corresponding baseline estimates, i.e. estimates computed above for untreated individuals. For risks, the difference between the two yielded an estimate of the absolute risk reduction, whereas for expected residual lifetime it yielded gain in lifetime, i.e. prolongation of life. All computations were performed in Stata 12.
Results
In the following, we only explicitly report estimates for males, and in certain instances only for some risk factor categories. The corresponding estimates for females, as well as all estimates for males may be found in the Appendix. The estimates for females display similar patterns as for males, although attenuated with respect to effect of treatment.
Cause-specific 10-year mortality risks for males using the Heart SCORE model and the modified (competing risk) approach
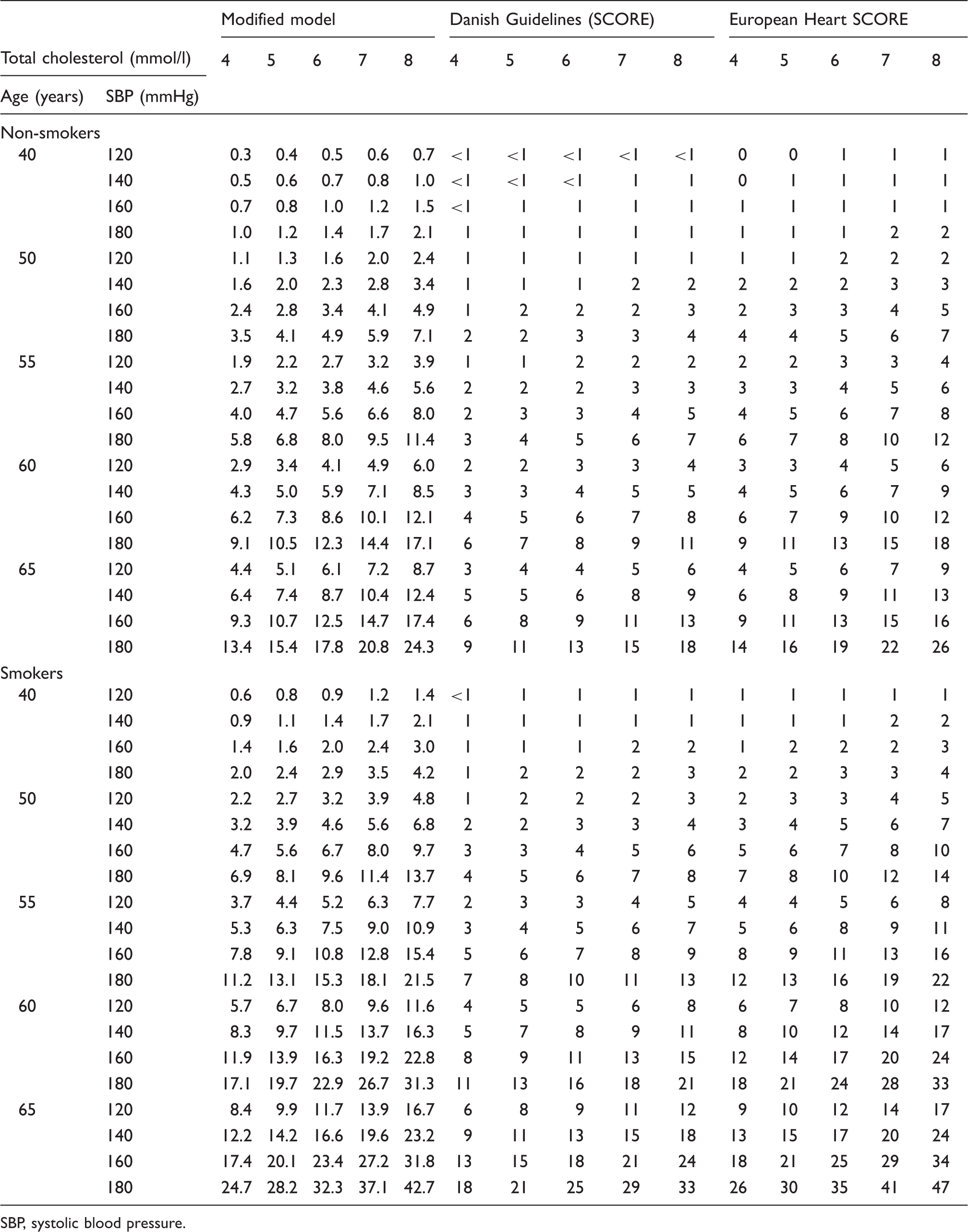
SBP, systolic blood pressure.
Ten-year mortality risks (%) without treatment and estimated absolute risk reduction with treatment for males due to cholesterol lowering (statin) treatment using the modified (competing risk) approach (all-cause mortality)
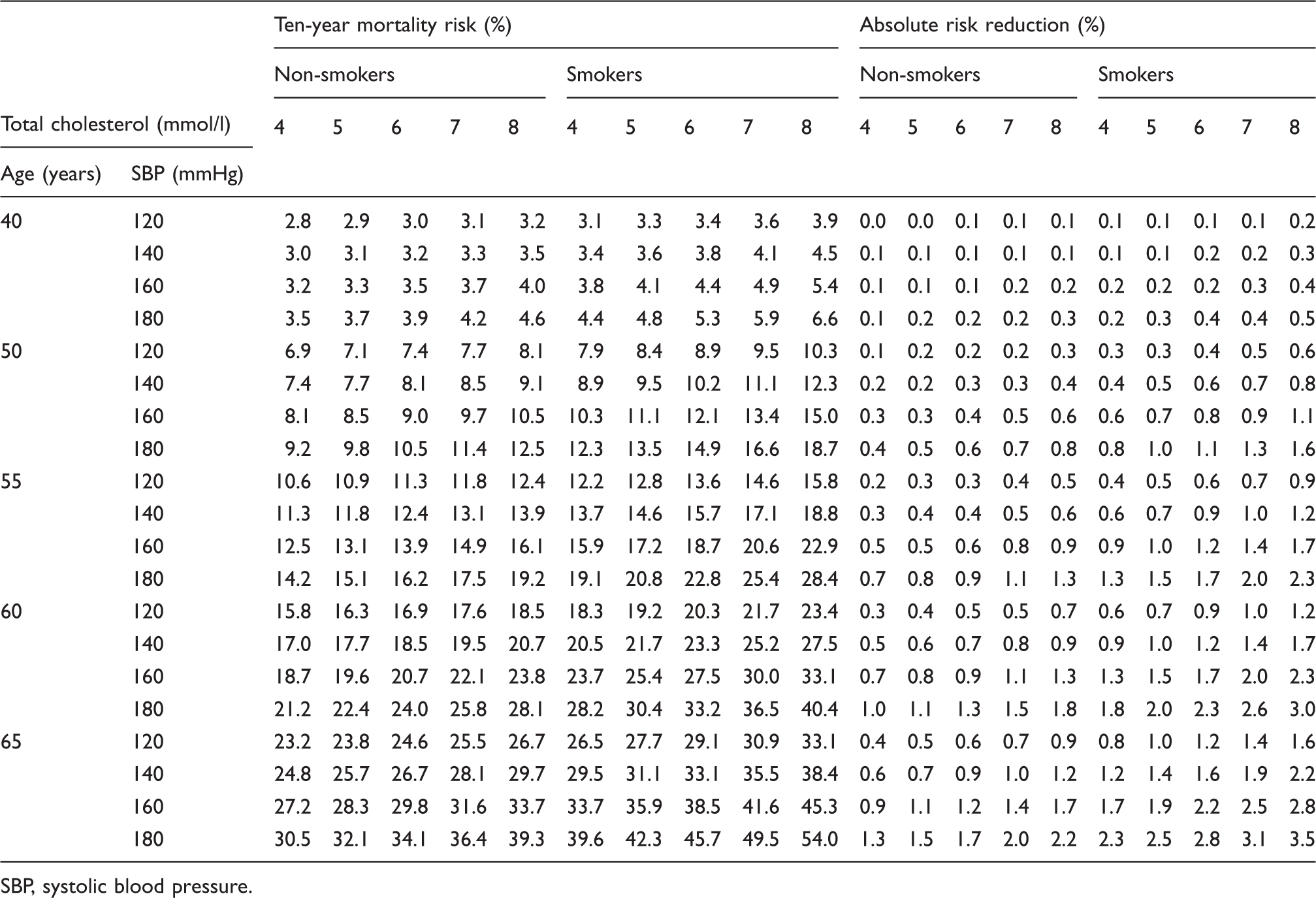
SBP, systolic blood pressure.
Expected residual lifetime (years) without treatment and gains in expected residual lifetime (months) due to cholesterol lowering (statin) treatment for males using the modified (competing risk) approach (all-cause mortality)
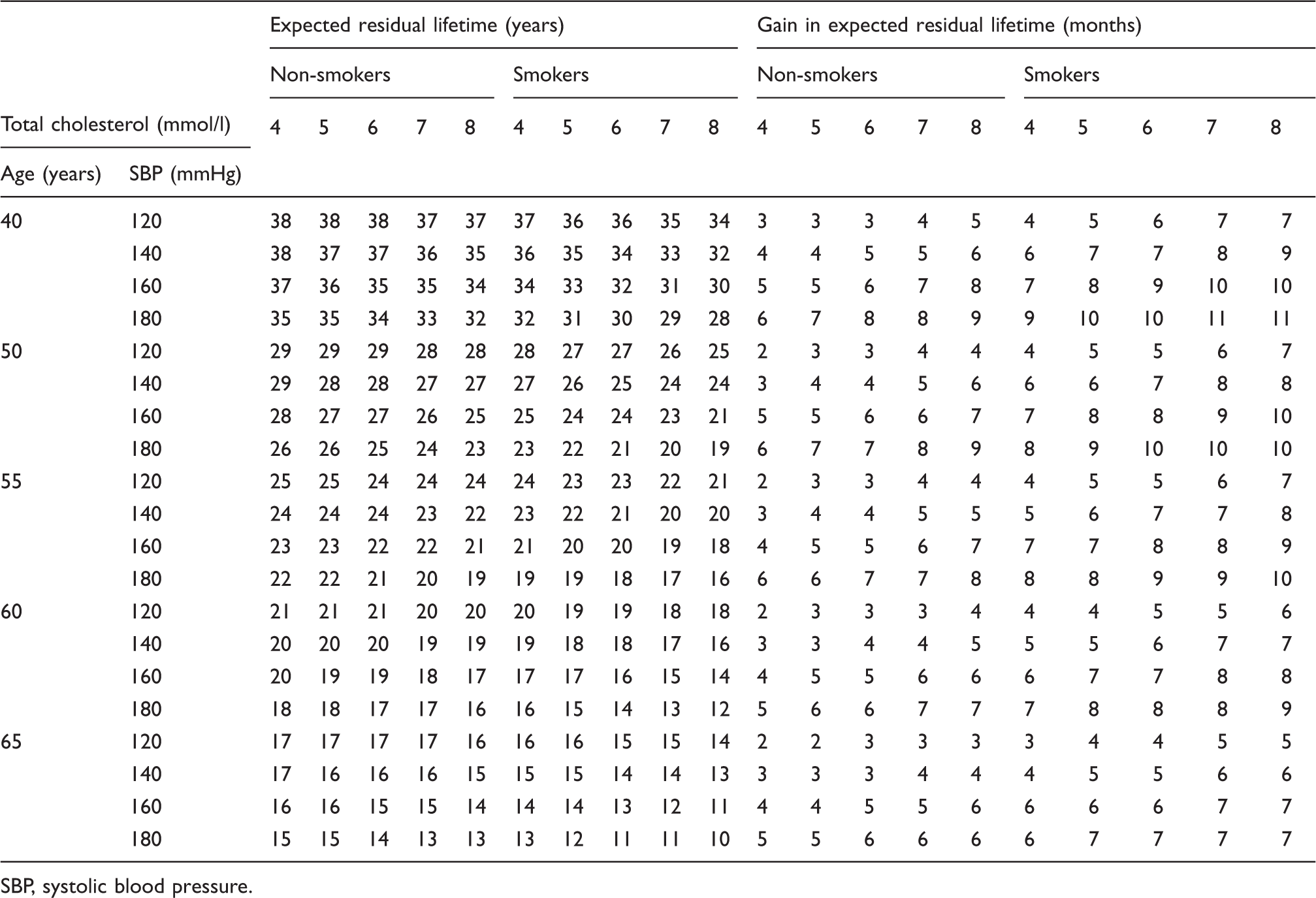
SBP, systolic blood pressure.
Ten-year mortality risk with absolute risk reduction and expected residual lifetime with gains due to cholesterol lowering (statin) treatment estimated from the modified (competing risk) approach for all-cause mortality, when all-cause mortality is either allowed to be influenced by smoking or not, for males aged 65
SBP, systolic blood pressure.
Discussion
The main result of this study is that a simple redefinition of the mathematical model underlying the European Heart SCORE can be used to obtain largely identical predictions to those of the SCORE model. The modification is based on considering the two types of fatal cardiovascular disease as competing risks, where only the first occurring will actually lead to death. Since the modified model is mathematically consistent, it allows computation of a variety of meaningful risk measures in contrast to the original SCORE model, which was specifically designed to predict cause-specific 10-year mortality risks. Not only is the modified model consistent, but the competing risk approach has further allowed extending the model to include non-CVD mortality without loss of consistency. If non-CVD mortality is not included, the estimated residual lifetime will seem unrealistically high for people with a low baseline risk of cardiovascular disease: in a scenario where only one cause leads to death, people without that cause become immortal. In contrast, the modified model, which incorporates non-CVD mortality, provides estimates of residual lifetime that seem realistic, and even more so when the non-CVD mortality is allowed to depend on smoking. The estimated treatment effects in the modified model are also more realistic than a naïve adaptation of the SCORE model since they represent reductions in overall mortality risks, i.e. reductions in risk of dying, not reductions in risk of dying from a specific cause. These two risks and reductions therein may differ substantially especially for the elderly.
The modified cause-specific 10-year mortality risks based on the competing risk approach yielded figures that were largely identical to both Danish Guidelines and the European Heart SCORE for all categories defined by sex, age, smoking, blood pressure, and cholesterol (Table 1), except when risks became high. The electronic version of the European Heart SCORE model yields estimates identical to our modified cause-specific 10-year mortality risks (www.heartscore.org, consulted March 2012). For none of the risk factor categories considered would the modified model lead to a change in treatment recommendation.
In the competing risk model used here, the various competing risks are assumed to be independent. Although this key assumption allows the simple representation of the joint survivor function as the product of the two survivor functions of each of the competing risks, and is therefore useful, it should be viewed with some scepticism, as a single underlying characteristic may influence different competing risks jointly. In our model, age, sex, and smoking habits all influenced the three competing risks, jointly. It is conceivable, however, that other factors may similarly jointly influence the competing risks and, in particular, various lifestyle factors other than smoking may influence all three risks. To the extent that these factors are explicitly allowed for in the model the assumption is likely unproblematic, but for latent, non-modelled factors the assumption is questionable. We estimated prognosis and treatment benefits from statins based on the assumption that smoking impacts CVD as well as non-CVD mortality. We cannot entirely exclude the possibility that other risk factors such as blood pressure and cholesterol levels influence non-CVD mortality. However, lacking data here, we disregarded such effects in the estimations. Thus the competing risk approach provides means for offsetting the problem by inclusion of additional risk factors considered to be important either for cardiovascular disease or non-CVD mortality, or both. 3
To be truly realistic in predicting all-cause 10-year mortality risk, the modified model should likely include information on many more risk factors known to influence mortality. In this paper, however, we strove to maintain congruence with the Heart SCORE, and thus we included exactly the same risk factors. Our modified model is mathematically consistent and can, in principle, if sufficiently detailed information is available, be extended to include other risk factors and remain consistent.
The SCORE model only presents the 10-year risk of CVD mortality and no estimates of intervention effectiveness. Nevertheless, some clinicians appear to use the SCORE model to estimate benefits from interventions, such as treatment with statins. Such use of the SCORE model would imply that excess risks are fully reversible by the intervention, which is rarely the case. In contrast, our modified model allows explicit incorporation of treatment effects as estimated from clinical trials, and thus more realistic estimates can be obtained from our modified model. Also, patients may have difficulties in understanding absolute risk reductions,23–25 while gains in life expectancy may seem more natural and thus easier to understand.16,17 For this reason we expanded the model to include gains in life expectancy (prolongation of life).
While both the absolute risk reductions and the estimated gains in residual lifetime may seem smaller than people generally imagine, they are nonetheless in line with similar estimates found in the literature. This was to be expected as we based the effect size due to lifelong statin treatment on a published meta-analysis on this. 22 The real problem with the seemingly small benefits is instead likely what Gigerenzer et al. 26 have described as a lack of statistical literacy of both doctors and patients. As a remedy, Gigerenzer et al. suggest that the public be generally made aware of meaningful estimates in terms of natural frequencies. In order to be able to compute such numbers, we submit that a consistent mathematical model, such as the one developed above, is needed. Further, we believe that the ability to provide estimates of overall mortality risk and of residual lifetime instead of cause-specific estimates can be considered a first step towards presenting meaningful risk estimates to the patient. There is, however, still a quintessential role left to the medical practitioner who must explain to patients when the balance between risk and benefit of treatment warrant medical treatment.
The clinical advice based on the modified SCORE model presented in this paper will, for most patients, not deviate significantly from the original SCORE model, except for high-risk individuals. However, the modified model is mathematically consistent and can be extended to include other risk factors including the interaction between different risk factors. Further, the modified model has a more general consistency and may be developed to fit other risk scenarios than CVD if the underlying risk information is available. Finally, because the modified model makes it possible to provide risk and benefit information in different formats, further studies of which formats are preferred by patients and medical practitioners are needed.
Footnotes
Acknowledgements
The authors would like to thank Anthony Fitzgerald, co-author of the original Heart SCORE paper, for helpful comments during review and for providing precise coefficients for the parameters used in the SCORE model.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.