
Abstract
Background
Quadriceps strength is related to exercise capacity in normal subjects and different patient populations, but the relationship between maximal quadriceps isometric strength (QIS) and different exercise capacity levels in coronary artery disease (CAD) patients has not been systematically evaluated yet.
Method
We studied 621 patients (60.6 ± 9.9 years, 538 males) with recent coronary artery bypass grafting or myocardial infarction, who underwent treadmill exercise testing, maximal QIS measurement (hand-held dynamometry), and coronary arteriography. Maximal QIS was expressed as absolute value (kg), %bodyweight, and %predicted maximum. Logistic regression was used to assess the relationship of maximal QIS, age, sex, number of diseased coronary vessels, peak systolic blood pressure, peak heart rate, brain natriuretic peptide, and left ventricular ejection fraction with 5, 7, and 10 estimated metabolic equivalents (eMETs) exercise capacity levels.
Results
Maximal QIS %bodyweight was the strongest predictor of exercise capacity in each eMETs category. Receiver-operating characteristics curves identified maximal QIS of 46, 51, and 59 % bodyweight as the best predictive cut offs for 5, 7 and 10 eMETs, respectively, with positive predictive values of 0.72, 0.66, and 0.67, respectively.
Conclusions
Maximal QIS is related with eMETs levels reached at exercise testing in CAD patients, and identified maximal QIS cut-off values for eMETs prediction may be used to set strength training goals according to patients’ needs with regard to habitual physical activity level. Hand-held dynamometry may meet the need of easiness of use and low cost required for strength evaluation in large-scale clinical trials.
Introduction
Exercise capacity, as assessed by peak VO2 or estimated metabolic equivalents (eMETs), is known to be an important predictor of physical disability and mortality in healthy individuals and patients with cardiovascular disease.1,2 For this reason, improvement in exercise capacity is one of the main goals of cardiac rehabilitation, resulting in both a reduction of mortality risk and an increased level of everyday habitual activities.3,4 The reduction of mortality risk for each 1-eMET increase in exercise capacity ranges between 10% and 25% and is evident in young and elderly subjects of both sexes with and without cardiovascular disease with mortality risk decreasing with increasing exercise capacity and reaching an asymptote at around 10 eMETs. 2
Besides aerobic exercise, many reports document that strength training also effectively improves exercise capacity in individuals with and without cardiovascular disease.5–8 The bulk of evidence suggests that loss of muscle strength is an important predictor of physical disability 9 and reduced exercise capacity in cardiac patients.11–15 Moreover, analogously to and independently of exercise capacity, muscle strength has been shown to predict mortality in both young and elderly normal and in different patient populations.16–19 Hence, resistance training is currently accepted as a main component of comprehensive cardiac rehabilitation, leading to improvements in quality of life and raising the performance level for occupational and recreational activities.6,20
Several papers have assessed the relationship between quadriceps strength and exercise capacity in normal subjects and chronic heart failure patients,11,12,21 but such relationship has been addressed to date only in small groups of patients with coronary artery disease (CAD) with contradictory results.9,13–15,22 Our working hypothesis was that a positive correlation would exist between maximal quadriceps isometric strength (QIS) and exercise capacity in CAD patients and that, if this were true, such a relationship would provide useful information in the clinical setting for a strength training prescription tailored on daily habitual activities in this population. The purpose of the present study was thus to investigate the relationship between maximal QIS and exercise capacity and to identify the levels of maximal QIS corresponding to those of given habitual activities in a large cohort of patients with CAD.
Methods
Study population
Patients’ characteristics
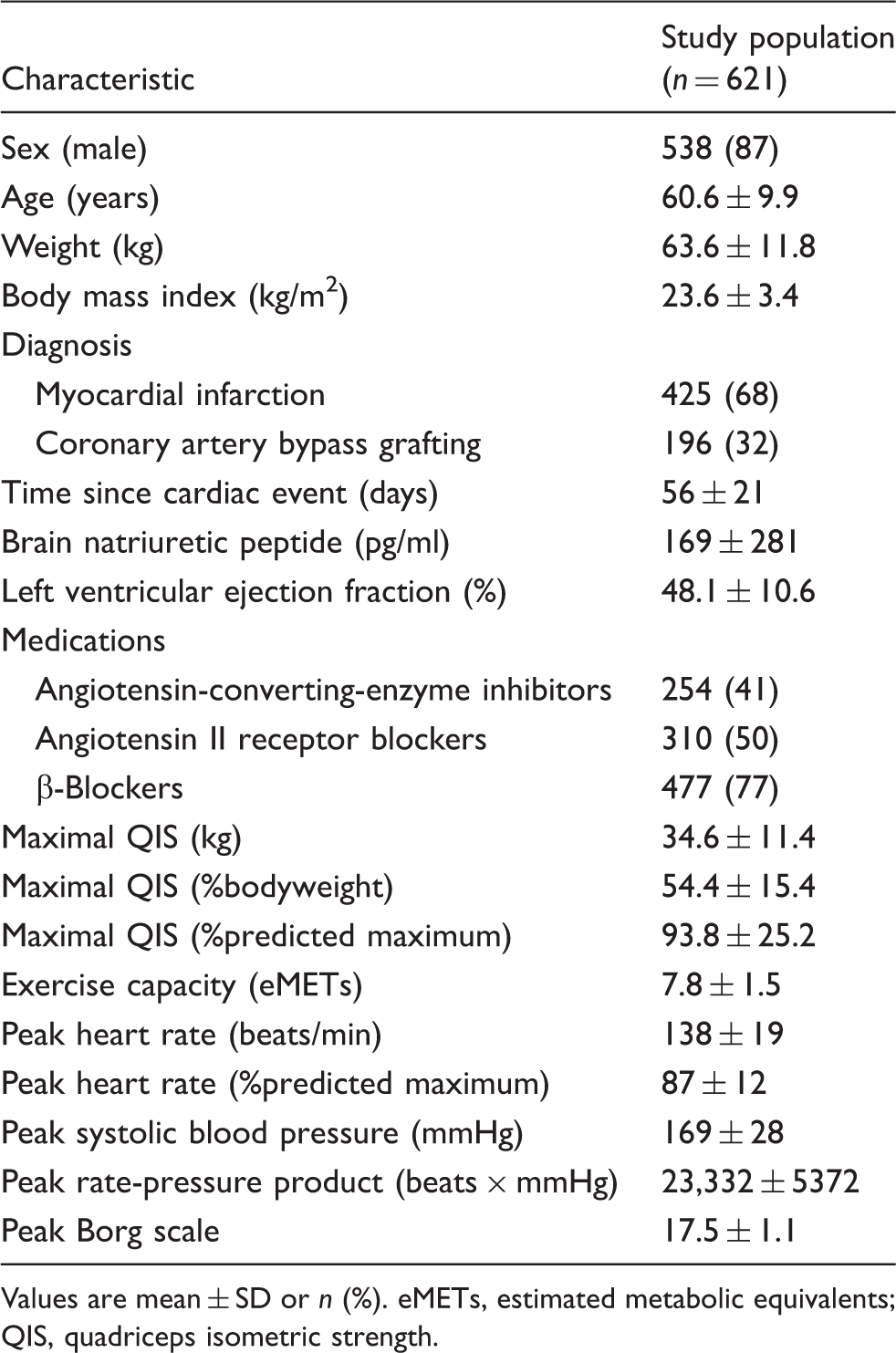
Values are mean ± SD or n (%).
eMETs, estimated metabolic equivalents; QIS, quadriceps isometric strength.
All patients underwent an echocardiography and a selective coronary arteriography as a part of their routine clinical/instrumental evaluation. Coronary lesions were considered haemodynamically significant when they caused a 75% reduction of the coronary luminal diameter (50% reduction for the left main coronary artery). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the Ethics Committee of Kitasato University Hospital. All patients gave their informed, written consent to participation in the study.
Treadmill exercise testing
All patients underwent a symptom-limited treadmill exercise testing according to the Bruce protocol. ECG was continuously recorded with an ergometric stress test system (ML-6500; Fukuda Denshi, Tokyo, Japan), and blood pressure was measured every minute by the cuff method with an automatic manometer (FB-300; Fukuda Denshi). Rating of perceived exertion (6–20 Borg scale) was assessed every 3 minutes during the exercise phase and just before its interruption. Exercise capacity was expressed in eMETs, calculated according to the following Bruce protocol-specific equation accounting for handrail use: 23 eMETs = (2.587 × TT + 6.004)/3.5, where TT is exercise time in minutes.
Maximal quadriceps isometric strength measurement
A few days after exercise testing, maximal QIS was measured by a hand-held dynamometer (µ Tas MT-1, ANIMA, Tokyo, Japan). Patients sat on a bench, and the dynamometer was fixed to a rigid bar. 24 Three 5-second maximal isometric voluntary contractions of the quadriceps were collected for both legs, with the knee joint angle fixed at 90° of flexion and hip joint angle set at approximately 90° of flexion, respectively. Right and left quadriceps were tested consecutively. A rest period of 30 seconds was provided between sets of bilateral contractions. Electrocardiographic data were continuously monitored via telemetry and blood pressure was evaluated manually before and immediately after strength measurements. Patients were told not to hold breathing during contractions to avoid the Valsalva manoeuver. The highest right and left side strength values were averaged and expressed as absolute value (kg), relative to body weight (%bodyweight), and relative to age- and sex-predicted values (%predicted maximum) based on available normative data. 25
Statistical analysis
Spearman’s rank correlation was calculated to evaluate the correlation between maximal QIS strength (absolute value, %bodyweight, and %predicted maximum) and eMETs. The maximal QIS parameter most correlated to eMETs was adopted in following analyses. Stepwise logistic regression was used to evaluate the relationship between exercise capacity categories of 5, 7, and 10 eMETs and maximal QIS, age, sex, number of diseased coronary vessels, brain natriuretic peptide level, left ventricular ejection fraction, peak systolic blood pressure, and heart rate. The above-mentioned eMETs categories were chosen as energetic costs equal to 5, 7, and 10 METs and include, respectively, most light-to-moderate, moderate-to-high, and high-to-vigorous intensity household, occupational, and sports activities. 26 In further analyses, we calculated the area under the curve (AUC) acquired from receiver-operating characteristics (ROC) curves to evaluate the discriminating power of maximal QIS in prediction of the three eMETs categories. The relationship between sensitivity and specificity of maximal QIS for prediction of 5, 7, and 10 eMETs attainment was examined by constructing sensitivity and specificity curves. 26 An optimal cut-off point maximizing sensitivity and specificity for each eMETs category was determined from the intersection of the sensitivity and specificity curves. 27
All analyses were carried out with the use of SPSS for Windows 20.0 statistical package (SPSS Japan, Tokyo, Japan). The level of statistical significance was set at a 2-tailed p-value of < 0.05.
Results
Clinical characteristics
The study population was composed mainly by males (Table 1). About one-half of the patients had 2/3-vessel CAD, with a left ventricular systolic function on average at lower normal limits and a quite well-preserved haemodynamic balance, as witnessed by only slightly elevated mean brain natriuretic peptide levels; most patients were on angiotensin-converting enzyme inhibitors/sartanics and/or beta-blockers (Table 1).
Maximal QIS corresponded on average to around one-half of body weight (even if with a large standard deviation) and was very close to predicted maximum (Table 1). Mean exercise capacity was >5 eMETs, attesting a good average exercise tolerance of the study population, but also in this case with a quite wide dispersion of individual values around the mean (Table 1). Mean peak heart rate expressed as a percentage of predicted maximum and mean peak rate-pressure product were consistent with significant exercise-induced whole body and myocardial stress, respectively (Table 1).
Exercise capacity predictors
Logistic regression models for different eMETs levels
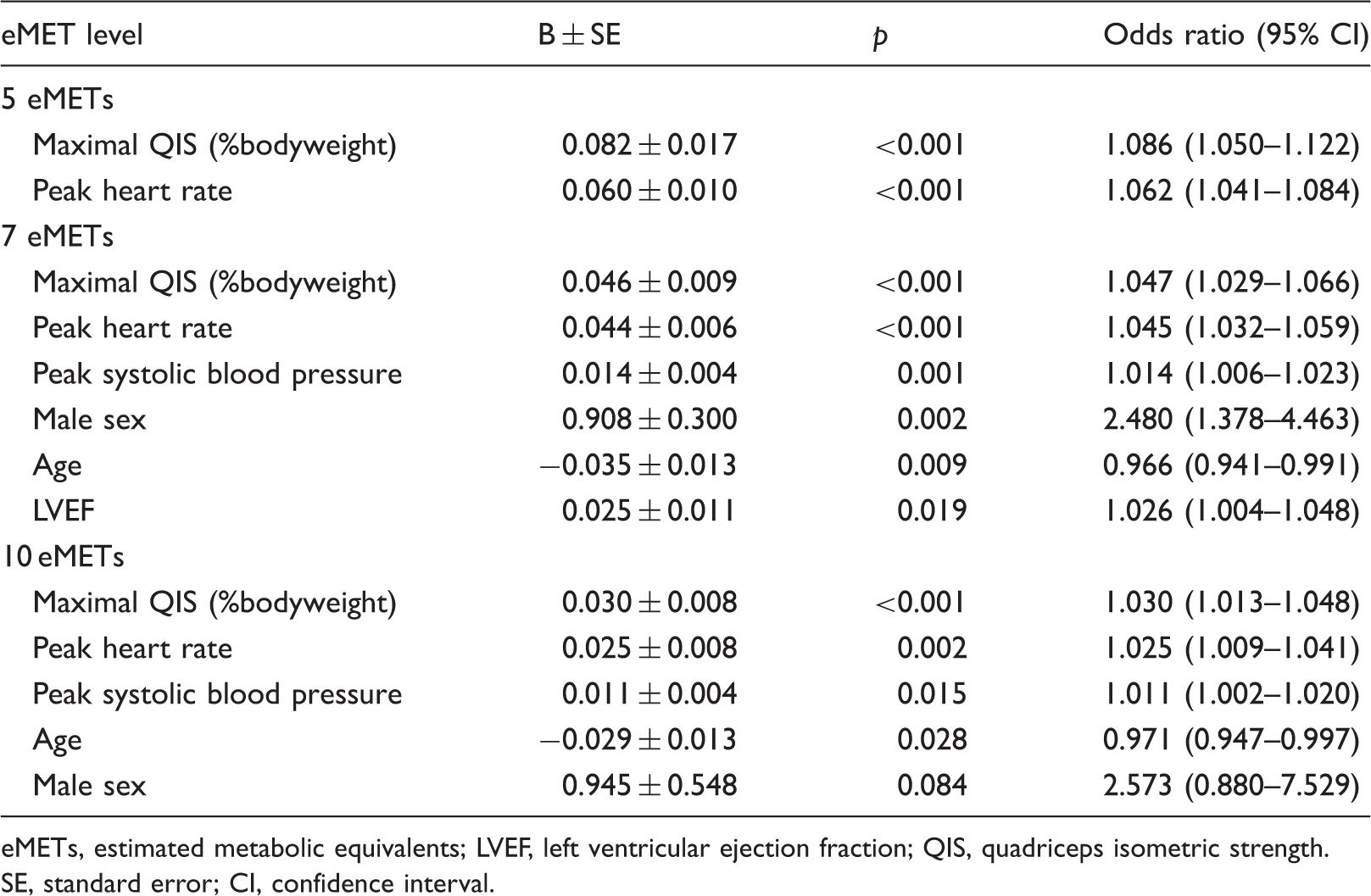
eMETs, estimated metabolic equivalents; LVEF, left ventricular ejection fraction; QIS, quadriceps isometric strength. SE, standard error; CI, confidence interval.
Validity of maximal QIS as an exercise capacity predictor
The AUC acquired from ROC curves for maximal QIS as a predictor of a 5, 7, and 10 eMETs exercise capacity attainment was 0.784 (95% CI 0.715–0.854), 0.719 (95% CI 0.672–0.767), and 0.720 (95% CI 0.634–0.806), respectively (all p < 0.001). The sensitivity and specificity curves for maximal QIS as a predictor of each eMETs level attainment are shown in Figure 1. Maximal QIS of 46, 51, and 59 %bodyweight were identified as optimal cut-off points maximizing sensitivity and specificity for prediction of 5, 7, and 10 eMETs exercise capacity attainment, respectively, with positive predictive values of 0.72, 0.66, and 0.67, respectively.
Sensitivity and specificity curves for maximal quadriceps isometric strength (%bodyweight) as a predictor of eMET attainment.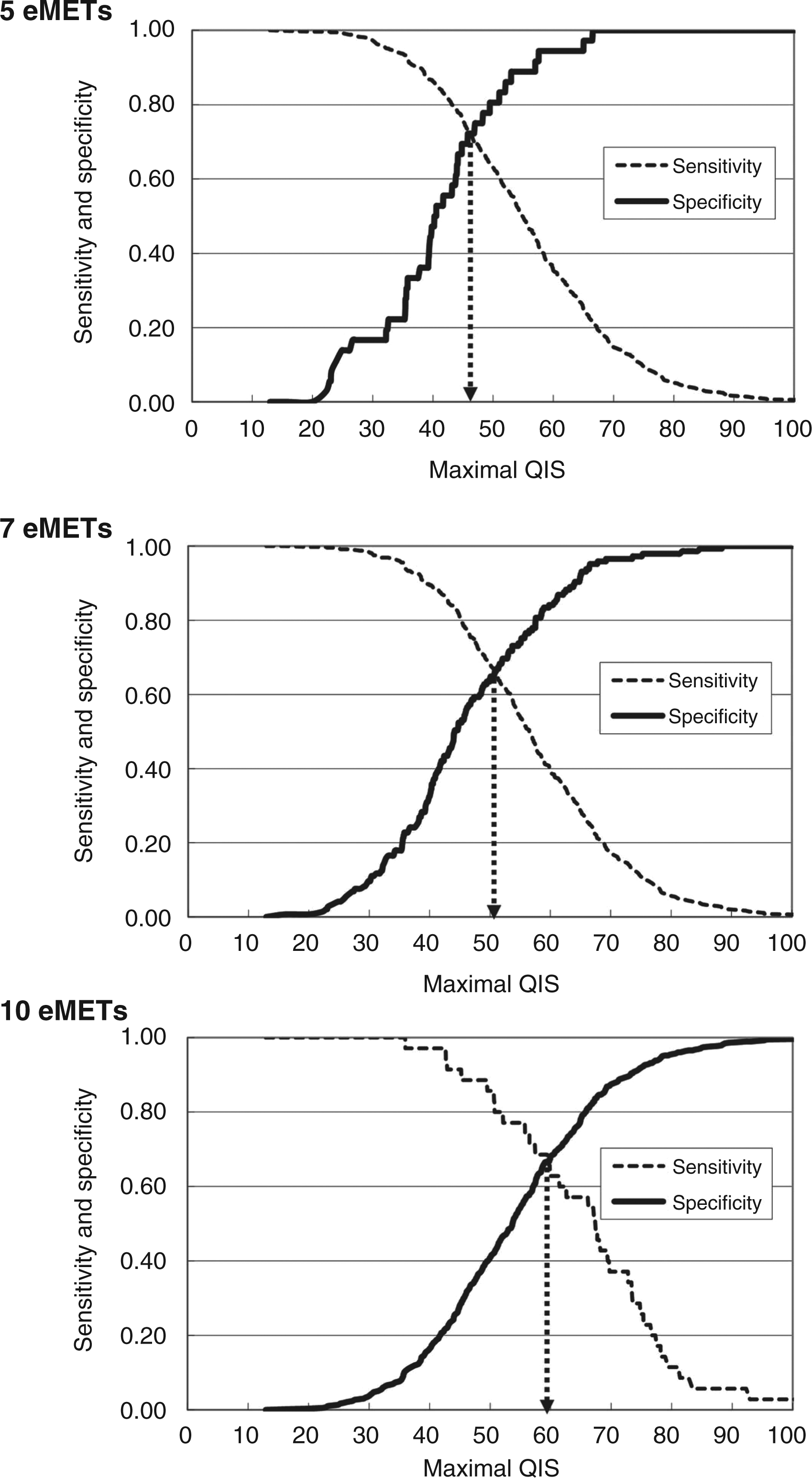
Discussion
The main finding of this study was that maximal QIS is significantly related to exercise capacity in patients with CAD; as a consequence, exercise capacity, as expressed in eMETs categories, can be predicted according to maximal QIS measurement in this population. Overall, these results can help clinicians to set the goal of strength training programmes in CAD patients according to patients’ needs about household, occupational, and sports activity level and to ascertain patients’ exercise capacity when exercise testing is not available or feasible.
Maximal QIS and exercise capacity in CAD patients
It is well known that exercise capacity is related to age, physical activity level, and cardiovascular clinical status. Additionally, many reports refer to muscle mass or strength as a factor linked to exercise capacity both in healthy subjects 5 and patients with chronic heart failure.8,10,11,21 However, the relationship between muscle strength and exercise capacity in CAD patients has been evaluated only in small patient groups, with contradictory results.9,13–15,22 The present study is the first o systematically examine the association between maximal QIS and exercise capacity in a large cohort of CAD patients. Our results show that maximal QIS was among the strongest independent predictors of each exercise capacity category after adjusting for several confounding factors. Of note, the logistic regression model for the 5 eMETs category included only maximal QIS and heart rate, whereas the 7 and 10 eMETs exercise capacity levels were independently predicted also by several other parameters. These findings lend support to the hypothesis that, in more unfit people (i.e. older and/or diseased), exercise capacity may be limited not only by central cardiovascular factors, but also by leg strength itself. 5
Clinical implications of maximal QIS cut offs in CAD patients
Association of quadriceps isometric strength with levels of exercise capacity and habitual activities
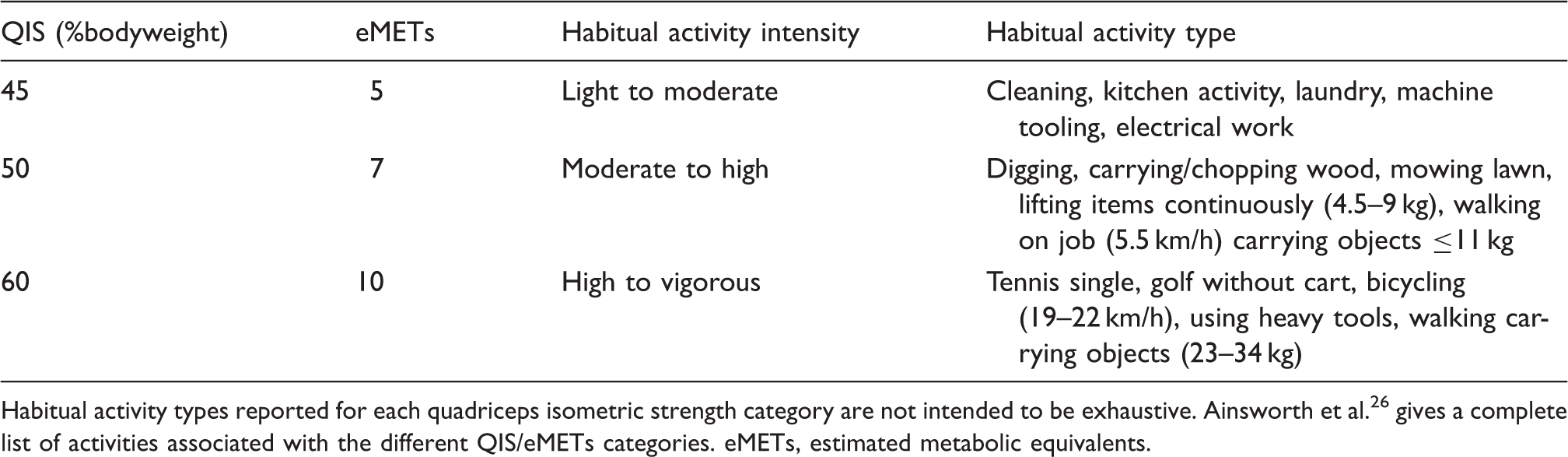
Habitual activity types reported for each quadriceps isometric strength category are not intended to be exhaustive. Ainsworth et al. 26 gives a complete list of activities associated with the different QIS/eMETs categories.
eMETs, estimated metabolic equivalents.
QIS measurement by hand-held dynamometer
We used a hand-held dynamometer to measure maximal QIS. Such dynamometer is widely used in clinical practice or community medicine because of its simplicity, objectivity, and responsiveness in measuring quadriceps strength, as compared to manual muscle testing or isokinetic dynamometry.25,28,29 Isokinetic dynamometers provide accurate assessments of dynamic and static muscle strength and are usually the preferred option for clinical studies. However, their use in large-scale epidemiological studies is limited, because the equipment is costly and not portable, and, as a consequence, muscle strength measurement is often omitted. 29 As the normative values for hand-held dynamometry and its test–retest reliability in measurement of the isometric muscle strength have already been established in healthy persons, 25 the expected values of muscle strength obtained in the present study can be universally applied in many kinds of hospital and home rehabilitation settings.
Study limitations
The use of an indirect descriptor of aerobic power (eMETs) for exercise capacity assessment may be questionable, since aerobic power can be overestimated when indirectly assessed using the Bruce protocol, especially in patient populations. 30 However, the equation for peak METs estimation used in the current paper has been shown to provide the lowest discrepancy between estimated and actual METs, with a mean value of 0.51 METs in patients with signs and symptoms suggestive for myocardial ischemia. 23 Such a value equals a mean difference of around 1.8 ml/kg/min between the estimated mean peak VO2 of 27.3 ml/kg/min in the study population (calculated as 7.8 eMETs × 3.5 ml/kg/min) and the actual peak VO2, i.e. a 6% discrepancy, which seems indeed acceptable. Also the exclusion from the study of patients who stopped exercise testing for reasons other than muscular fatigue may be questioned, as this group does include patients in whom a peak exercise capacity evaluation with tools different by exercise testing would be most indicated. However, the inclusion in the study of patients likely not attaining ‘true’ maximal effort, would have significantly confounded the interpretation of the maximal QIS vs. eMETs relationship.
Conclusions
The results of this study demonstrate that maximal QIS is related to exercise capacity in patients with CAD and that maximal QIS values of 45, 50, and 60 %bodyweight can be used to predict exercise capacity levels of 5, 7, and 10 eMETs, respectively. These findings can be used in cardiac rehabilitation for the definition of strength training goals according to patients’ needs about daily activity level, and to indirectly evaluate exercise capacity when exercise testing is not available. Finally, the results of this study lend support to the use of hand-held dynamometry for maximal QIS measurement in large-scale clinical trials in CAD patients.
Footnotes
Funding
This study was supported in part by the Ministry of Education, Science and Culture in Japan (no. 15500383).
Conflict of interest
The authors declare that there is no conflict of interest.