
Abstract
Background
Home-based interventions might facilitate the lifelong uptake of a physically active lifestyle following completion of a supervised phase II exercise-based cardiac rehabilitation. Yet, data on the long-term effectiveness of home-based exercise training on physical activity and exercise capacity are scarce.
Objective
The purpose of the TeleRehabilitation in Coronary Heart disease (TRiCH) study was to compare the long-term effects of a short home-based phase III exercise programme with telemonitoring guidance to a prolonged centre-based phase III programme in coronary artery disease patients. The primary outcome was exercise capacity. Secondary outcomes included physical activity behaviour, cardiovascular risk profile and health-related quality of life.
Methods
Ninety coronary artery disease patients (80 men) were randomly assigned to 3 months of home-based (30), centre-based (30) or a control group (30) on a 1:1:1 basis after completion of their phase II ambulatory cardiac rehabilitation programme. Outcome measures were assessed at discharge of the phase II programme and after one year.
Results
Eighty patients (72 (91%) men; mean age 62.6 years) completed the one-year follow-up measurements. Exercise capacity and secondary outcomes were preserved in all three groups (Ptime > 0.05 for all), irrespective of the intervention (Pinteraction > 0.05 for all). Eighty-five per cent of patients met the international guidelines for physical activity (Ptime < 0.05). No interaction effect was found for physical activity.
Conclusion
Overall, exercise capacity remained stable during one year following phase II cardiac rehabilitation. Our home-based exercise intervention was as effective as centre-based and did not result in higher levels of exercise capacity and physical activity compared to the other two interventions.
Trial registration
ClinicalTrials.gov NCT02047942. https://clinicaltrials.gov/ct2/show/NCT02047942
Introduction
Cardiac rehabilitation (CR) contributes significantly towards the care of cardiovascular disease patients, 1 and is now considered as a class IA recommendation by all international guidelines.2,3 CR is a complex multidisciplinary intervention that comprises different therapies: that is, risk factor education and modification, health behaviour change, psychological support, vocational support and nutritional counselling. These interventions target risk factors for coronary artery disease (CAD), 4 and have physical activity (PA) and exercise as their core accounting for 30–70% of the total programme. Among patients with established CAD, participation in an exercise-based CR programme provides major health benefits including a reduced risk of cardiovascular mortality and hospitalisation (and associated healthcare costs) and improvements in health-related quality of life (HRQoL). 5
Nevertheless, long-term adherence to a healthy active lifestyle remains the biggest challenge for these patients. 6 Evidence shows that PA levels decline after CR completion, with as few as 28% of patients maintaining the recommended levels at 12 months of usual care. 7 This is especially worrisome because PA might underlie the maintenance of exercise capacity (EC; VO2P) which when compared with other known cardiovascular risk factors is the strongest predictor of mortality among CAD patients. 8
In Belgium, 15–20% of patients participate in an ambulatory CR programme (phase II), whereas only 5% participate in a long-term phase III maintenance intervention. 9 As it is often easier to integrate an exercise routine into the home and community environment, 10 the use of home-based (HB) CR carries the potential to improve compliance to an active lifestyle compared to centre-based (CB) CR in the long term post-hospitalisation. 10
Current technological advances have allowed moving away from the hospital setting towards the use of exercise training in the patients’ home. Among others, telerehabilitation involves the guidance and monitoring of the patient from a distance, and the provision of personalised feedback on a regular basis. Earlier meta-analytic data already showed that HB rehabilitation could be an alternative for supervised CR for promoting the maintenance of EC in the short term. 11 However, the long-term effects of HB have not been widely studied. Recently Claes et al. 12 identified, respectively, three and seven studies evaluating PA and EC at least one year following HB CR. Small, though clinically non-significant, effect sizes for EC were found in favour of HB CR compared to CB CR in the longer term with similar effects on PA behaviour. Moreover, none of these studies used objective tools to assess PA.
Given the limited data available, the objective of the current report was to compare the long-term effects (i.e. one year after completion of an ambulatory phase II CR programme) of a 12-week HB programme or a 12-week prolonged CB programme on EC by objectively measuring PA behaviour in CAD patients. We hypothesised that patients enrolled in the HB group would show a smaller decrease in peak oxygen consumption (VO2P) and higher levels in PA compared to patients in the CB and usual care control group (CG).
Methods
Study design and population
The TeleRehabilitation in Coronary Heart disease (TRiCH) study is a randomised controlled clinical trial designed to investigate the long-term effect of a HB exercise intervention with telemonitoring guidance on EC and PA in CAD patients after discharge from a phase II CR programme. A detailed description of the experimental design, 13 recruitment procedure and eligibility criteria as well as the short-term results 14 have been reported elsewhere. The study protocol was approved by the medical ethical committee of UZ Leuven/KU Leuven and all patients provided written informed consent. The TRiCH study was registered in the ClinicalTrials.gov database: NCT02047942.
In summary, 90 CAD patients who completed a supervised phase II CR programme were randomly assigned on a 1:1:1 basis to HB, prolonged CB or a usual care CG for 12 weeks. The HB group received an individualised exercise prescription recommending them to exercise for at least 150 minutes a week at a target heart rate of 70–80% of heart rate reserve (HRR) at home for 3 months. Patients were asked to log all exercise data by means of a Garmin Forerunner (Garmin Forerunner 210, Wichita, USA) and to upload the data on the online web application (https://connect.garmin.com/nl-NL/) for review by the investigators. 15 Once a week, patients received feedback by phone or e-mail. Patients randomly assigned to CB continued their training on an ambulatory basis at the outpatient clinic of UZ Leuven. This intervention included three weekly sessions, consisting of approximately 45 minutes of endurance training at 70–80% of HRR followed by relaxation. The CG was advised to maintain a physically active lifestyle and was invited for the follow-up visits at 12 weeks and one year. Following completion of the 3-month intervention, all groups were encouraged to continue exercising. No further contact was provided during the subsequent 9 months.
Primary outcome measure
Cardiorespiratory fitness or EC
EC was determined as VO2P assessed by a maximal graded test on a bicycle until volitional exhaustion with breath-by-breath respiratory gas analysis (Ergometrics 800S, Ergometrics, Bitz, Baden-Württemberg, Germany) and continuous 12-lead electrocardiogram. The test started at 20 W and was increased by 20 W/minute. We defined VO2P as the 30 seconds average oxygen uptake at the highest workload. 13 In addition, we measured peak heart rate, calculated peak respiratory exchange ratio and determined both ventilatory thresholds. 13 The first ventilatory threshold (VT1) (ventilatory anaerobic threshold) was defined as the nadir or first increase of ventilation (VE) over oxygen uptake (VO2) (VE/VO2) versus workload without a simultaneous increase in VE over carbon dioxide production (VCO2) (VE/VCO2) versus workload. The second ventilatory threshold (VT2) (respiratory compensation point) was defined as the nadir or non-linear increase of VE/VCO2 versus workload.
Secondary outcome measures
Physical activity
PA was measured with a Sensewear Mini Armband (BodyMedia, Inc., Pittsburgh, PA, USA) worn on the non-dominant arm for a minimum of five consecutive days. Steps, sedentary time (duration of sedentary activity at an intensity of <1.5 metabolic equivalents of task (METs); minutes), duration of light intensity physical activity (≥1.5 and <3 METs; minutes) and duration of moderate and vigorous PA (≥3 METs; minutes) were used in the analyses. 16 Patients meeting the international guidelines of a minimum 150 minutes of moderate physical activity or 75 minutes of vigorous activity at the one year follow-up were labelled as ‘physically active’. 17
Muscle function
The sit and rising test, 18 handgrip strength (JAMAR grip strength dynamometer)19,20 and quadriceps maximal isometric knee extension strength and isokinetic total work (Biodex Medical Systems Inc., 840-000 System 4, New York, USA) were also obtained. 20
Traditional cardiovascular risk factors
We measured traditional cardiovascular risk factors including anthropometric characteristics (body mass index, waist and hip circumference), blood pressure and biochemical analysis of a fasting blood sample (glucose, total cholesterol, low-density lipoprotein-cholesterol, high-density lipoprotein-cholesterol and triglycerides).
Health-related quality of life
The SF-36 was used to assess HRQoL. 13
Statistical analysis
Statistical analyses were performed using SPSS (version 20; SPSS for windows; SPSS Inc., Chicago, IL, USA). The current report compares the data obtained at discharge of the phase II CR programme (baseline) and after one year of follow-up between the different groups. The Shapiro–Wilks test was used to assess the normality of distributions. Continuous variables are reported as means ± standard deviation (SD) or median, categorical data as numbers and percentages. One-way analysis of variance and chi-square tests were used to analyse differences in demographic and clinical data between groups at baseline. We applied a linear mixed modelling method to evaluate time, group and time × group interaction effects. Spearman correlation coefficients (ρ) were calculated between VO2P and PA characteristics. A two-tailed P ≤ 0.05 was considered statistically significant.
Results
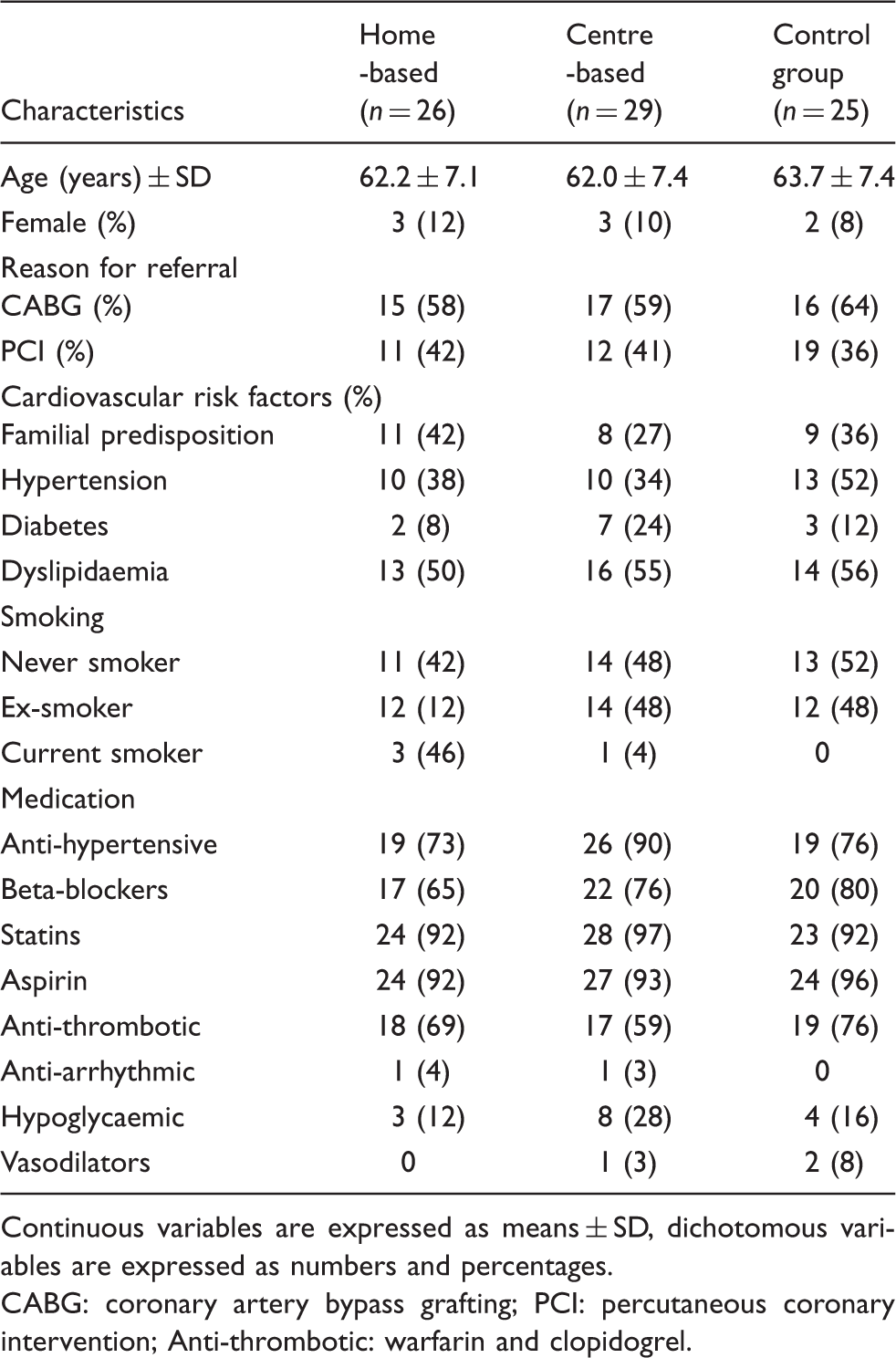
Figure 1 shows the flow of patients throughout the study. In total, 91% or 80 patients completed the one-year follow-up measurements, while four patients (three men) from the HB group, one patient from the CB group (one man) and five patients (four men) from the CG group dropped out. At baseline, groups were equal with regard to demographic and clinical characteristics, reason for referral and pharmacological treatment (Table 1). The demographic characteristics of patients that dropped out were not different from the other participants.
Flow of patients throughout the study. Baseline characteristics of patients. Continuous variables are expressed as means ± SD, dichotomous variables are expressed as numbers and percentages. CABG: coronary artery bypass grafting; PCI: percutaneous coronary intervention; Anti-thrombotic: warfarin and clopidogrel.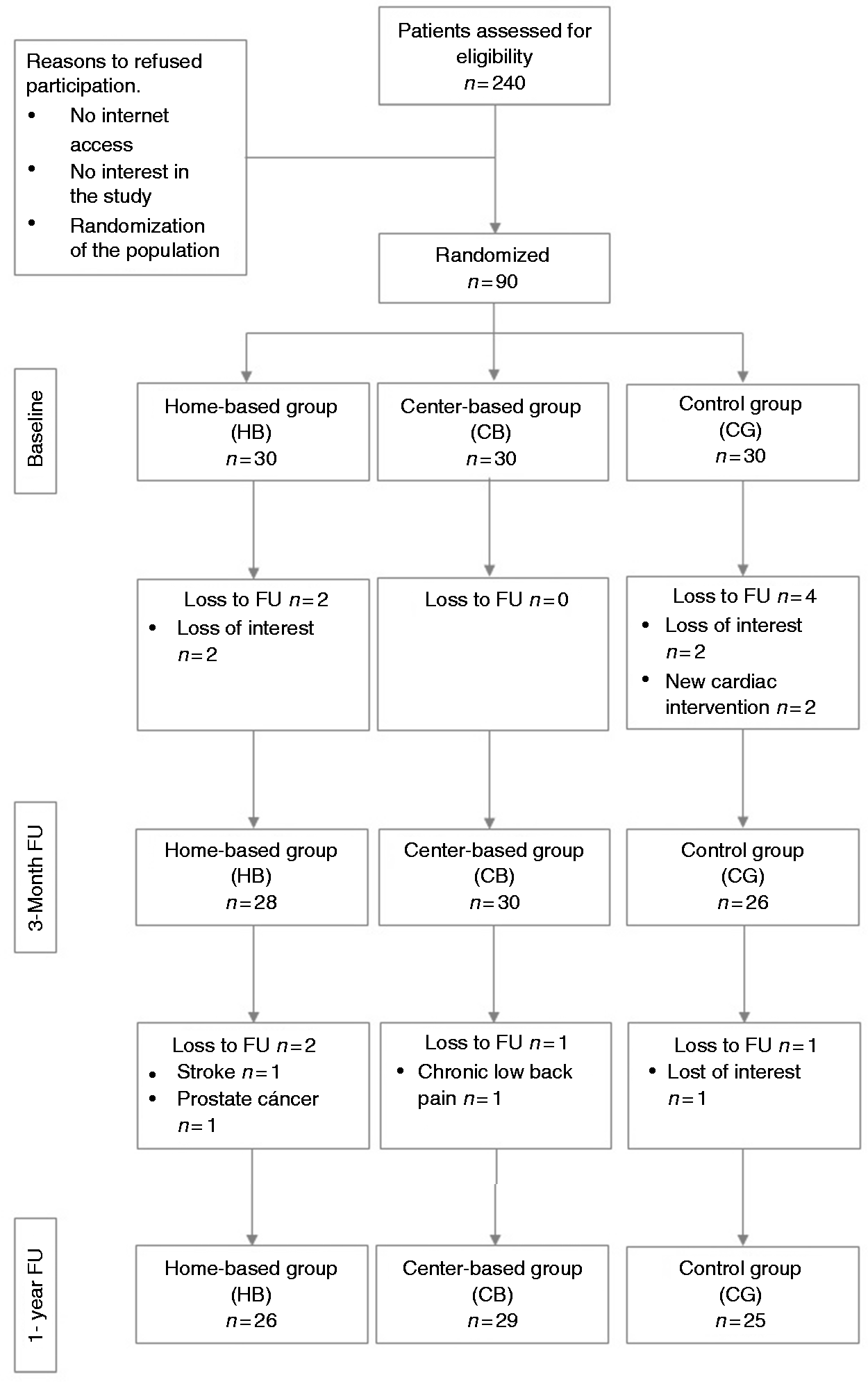
Primary outcome measure
Changes in primary outcome and other respiratory parameters during the study.
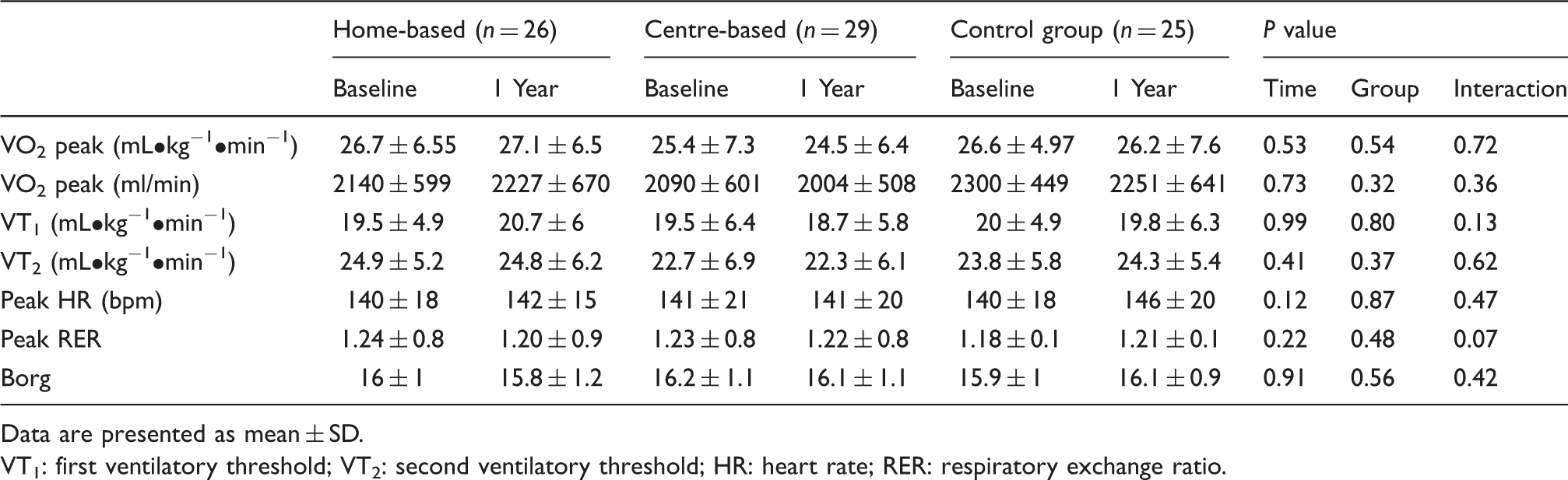
Data are presented as mean ± SD.
VT1: first ventilatory threshold; VT2: second ventilatory threshold; HR: heart rate; RER: respiratory exchange ratio.
Secondary outcome measures
Figure 2 shows PA data of the groups at the end of CR and at one-year follow-up. Overall, 96.6% of the population met the international guidelines of 150 minutes or more of moderate PA per week at discharge from phase II CR. At one year of follow-up, the number of patients fulfilling these guidelines had decreased to 85% (P = 0.1). There were no differences across groups (Pgroup = 0.12). PA, by measurement of average steps per day, trended up in the HB group from a median of 7896 (2018–12,554) at baseline to 8002 (1612–17,237) at follow-up, and down in the other groups although showing no significant interaction (Pinteraction = 0.75). Although the time spent in light PA trended up in the three groups, it showed no significant interaction (Pinteraction = 0.72). The time spent in moderate to vigorous PA was lower at 12 months of follow-up compared to baseline (Ptime = 0.01). However, the decrease was similar in all groups (Pinteraction = 0.95). As shown in Table 3, the improvement in isometric quadriceps extension, isokinetic total work and handgrip strength reached statistical significance (Ptime ≤ 0.001) without significant differences among groups (Pinteraction ≥ 0.05).
Daily physical activity at baseline and follow-up. Data are presented as percentage, mean ± SE. (a) Physical activity guidelines (>150 minutes/week); (b) steps/day; (c) sedentary behaviour = ≤1.5 metabolic equivalents of task (METs); minutes/day; (d) physical activity duration = >3 METs; minutes/day. HB: home-based group; CB: centre-based group; CG: control group. White column: baseline; dark grey column: one-year follow-up. Changes in strength during the study. Data are presented as mean ± SD.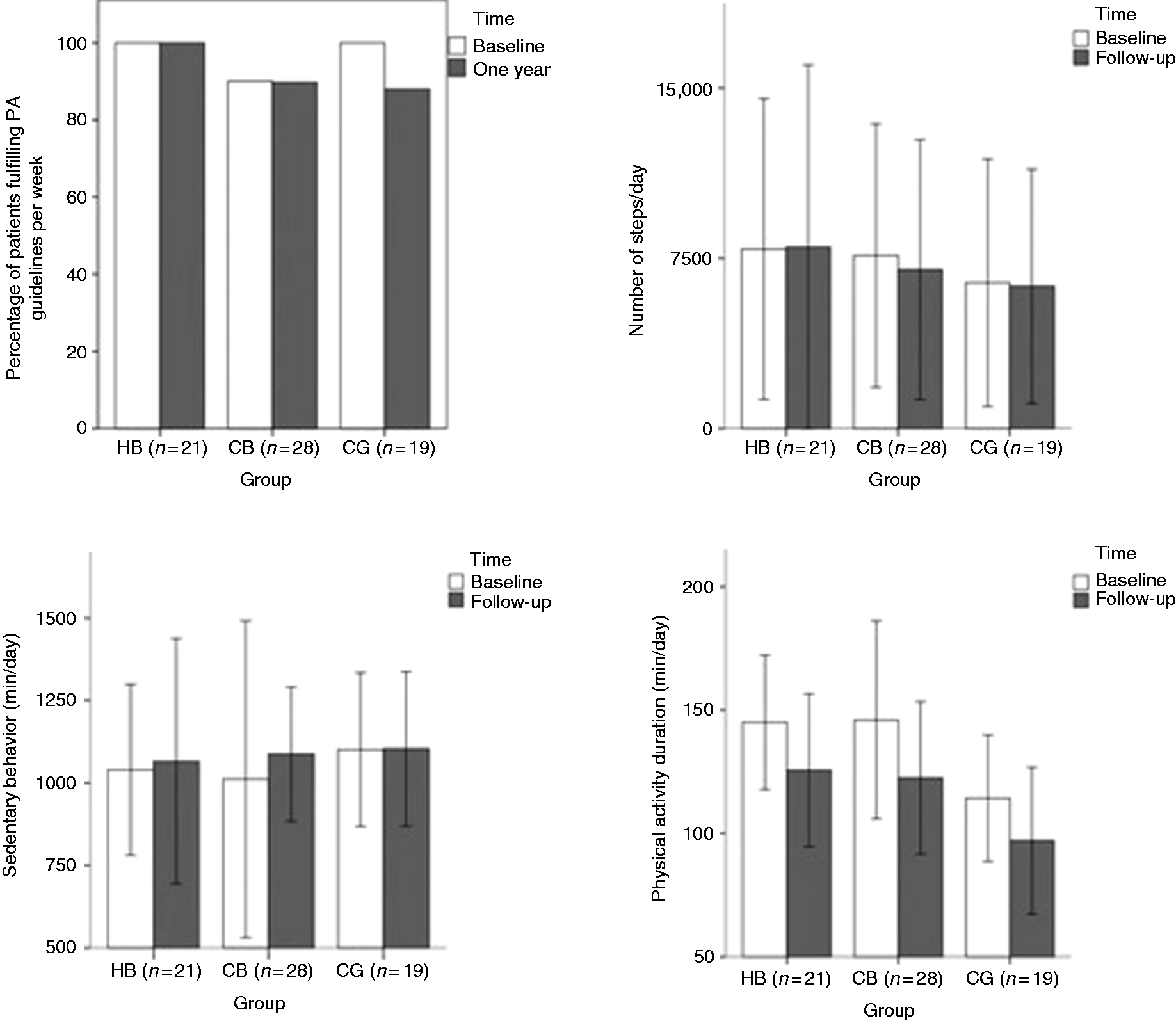

Cardiovascular risk factors and anthropometrics characteristics during the study.
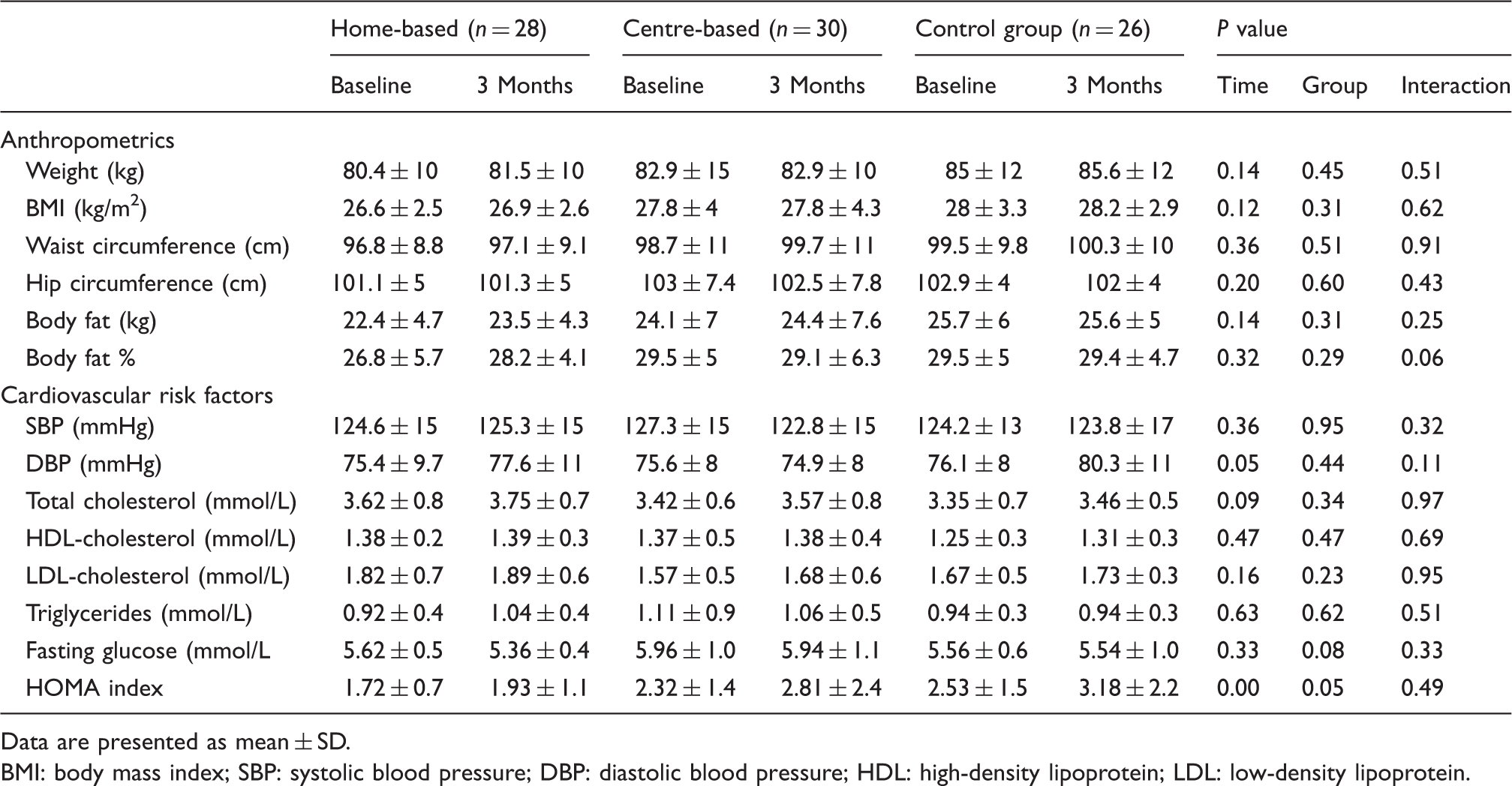
Data are presented as mean ± SD.
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein.
Finally, all groups maintained high scores for all HRQoL parameters at one year of follow-up, the interactions in the overall score as well as the subscores were not significant between the groups (Pinteraction = 0.70) as can be seen in Figure 3.
Changes in health-related quality of life during the study. Data are presented as percentage, mean ± SE. HB: home-based group; CB: centre-based group; CG: control group. White column: baseline; dark grey column: one-year follow-up.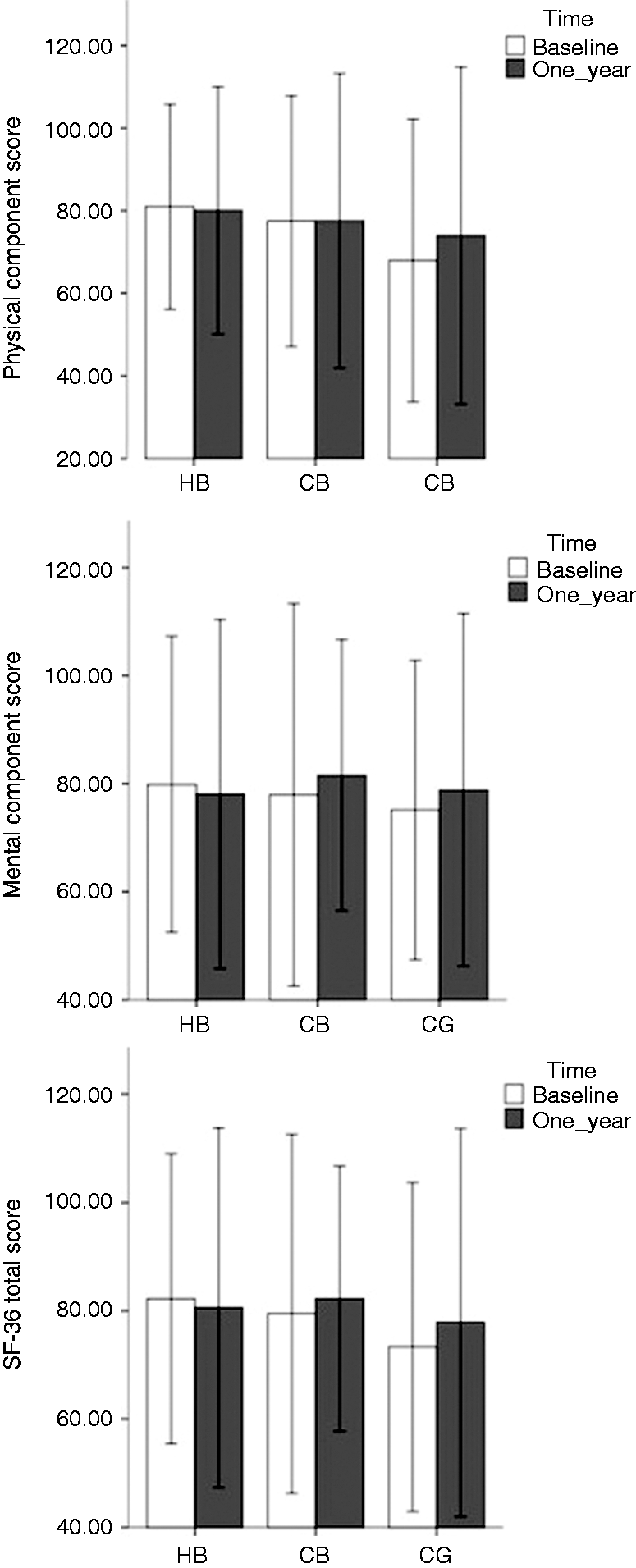
Discussion
The aim of our study was to compare the longer-term effects of a 12-week HB exercise programme with telemonitoring guidance to a prolonged 12-week CB CR programme following completion of a phase II CR in patients with CAD. Overall, we showed that HB CR is as effective as a prolonged CB CR programme to maintain EC and PA levels. We also found maintenance of EC and PA at one year of follow-up; in fact, 85% of our patients met the international guidelines of 150 minutes of moderate PA per week. 17
Contrary to our hypothesis, we could not demonstrate higher levels of PA at one year of follow-up, in patients randomly assigned to a HB training programme with telemonitoring guidance, therefore we could not document higher levels of EC compared to the patients enrolled to the other groups.
Yet, our results are in line with the findings of the FIT@Home study 21 in which 90 low-to-moderate cardiac risk patients initiating a phase II CR programme were randomly assigned to 3 months of either HB training with telemonitoring guidance or CB CR. At one year of follow-up, they reported an improved EC in both groups, without between-group differences. Our study complements their results because our intervention started in phase III CR showing no differences between HB training with telemonitoring guidance and CB training in the long term. Our results also confirm those published in a report by Claes et al., 12 who showed no influence on EC in HB CR compared to usual care when both were offered after completion of a phase II CB CR programme.
These results suggest that although exercise-based CR is often aimed at short-term improvement of EC, it might also prepare the patients for independent lifestyle changes that favour the long-term maintenance of the benefits obtained at completion of a phase II CR programme.
Frederix and colleagues published the Telerehab III trial,22,23 a randomised controlled trial (N = 140) comparing the efficacy and cost-efficiency of a 24-week telerehabilitation programme in addition to conventional CR versus conventional CR alone. Patients in their intervention were provided with an internet-based telerehabilitation programme in addition to conventional CB CR. The telerehabilitation programme was composed of PA telemonitoring, dietary, smoking cessation and activity telecoaching. Contrary to our intervention, they showed an improvement in EC in favour of the patients receiving telerehabilitation. The different outcomes of the studies might be explained by the lack of a clear definition for ‘HB CR’. As such, the contents of HB CR interventions varied widely and ranged from the use of manuals for a healthier lifestyle to personalised exercise prescriptions. 12 One such example is the study by Park et al., 24 who described a positive adherence using an intervention of daily text messages (SMS) in combination with a supporting website. The majority of participants (85%) in this study reported reading their SMS while the median number of visits to the website was only three visits in a 6-month period, thus they suggested that telemonitoring interventions such as SMS may have a higher likelihood of patient participation and adherence than internet-based programmes. 24 Complementary, Coorey et al. hypothesised that integrating gamification principles into telemonitoring technologies may increase motivation for sustaining essential, but repetitive, routine lifestyle tasks over the longer-term. 25
Cardiac telerehabilitation has been introduced as an adjunct or alternative to conventional CR to increase uptake rates, enable more prolonged care and improve long-term success. 22 Although we observed a small decrease in the proportion of patients meeting the international guidelines for PA, still 85% of patients was doing more than 150 minutes of moderate PA one year following completion of the phase II CR programme, which is much more than the 39–46% reported in earlier studies. 26 We speculate that patients underwent a real lifestyle change due to acquired self-motivation during the CR, although behavioural modifications were not measured in our study. 16 However, we cannot rule out the impact of a selection bias whereby we potentially have recruited the more motivated patients. Furthermore, the awareness of follow-up testing could have motivated patients to maintain their PA level. 27
Cowie et al. 28 randomly assigned 60 patients with heart failure to home training, hospital training or control. There were no significant differences in mean steps per day, or walking pattern at long-term assessment. They attributed these results to the nature of the intervention, which was based on PA alone without behavioural counselling similar to our study. Reid et al. 29 found a significant decrease in habitual PA during long-term follow-up after hospital discharge in patients with CAD. Along the same lines, Hansen et al. 30 found that only 27% of patients participating in CR adhered to the minimal PA level required to obtain significant health benefits 18 months after completion of a CB CR programme. In this TRiCH study, the Sensewear Mini Armband data showed that the PA levels were regular and maintained in the long term for all groups. This finding is clinically important because the long-term success of CR rests in part on the patient’s ability to maintain healthy behaviours, including participation in regular PA. Giannuzzi et al. 31 indicated that continued patient interaction and monitoring, as well as continuation of a lifestyle intervention (phase III rehabilitation), is required to obtain long-term clinical benefits. However, we considered that prolonging the supervised exercise intervention for HB or CB groups in our study would not have resulted in differences between groups.
Although numerous studies have illustrated the effects of telemonitoring interventions on the incidence of cardiovascular disease, controversy still remains; a meta-analysis of Neubeck et al. 32 has shown significantly favourable changes in total cholesterol, its lipoprotein fractions and smoking habits with telehealth participation compared to usual care at medium to long-term follow-up. However Gu et al. 33 noted that several telehealth intervention trials reported a non-significant reduction of cardiovascular disease risk factors in patients with prior CAD. Reasons for these different findings could be due to differences in sample sizes, follow-up duration and design of studies centred on cardiovascular risk factors as the primary endpoint. We considered that the patients included in our TRiCH study were at low risk over the first year after enrolment, thus the likelihood of detecting a beneficial effect was small. Furthermore, the incremental benefit of secondary prevention programmes over usual care may be very small if the medical management of the patients is probably close to optimal. 34
In relation to HRQoL, Frederix et al. 23 evaluated the generic health status through the 5Q–5D questionnaire at baseline and at 24 weeks of follow-up. They described an improvement of quality of life in their intervention group derived as the result of a reduced cardiovascular rehospitalisation rate while a deterioration in the control group was observed. However, the FIT@home study 21 showed that HRQoL was similar from baseline and one year of follow-up with no significant between-group differences. Similar to their results, 21 we were unable to detect changes in HRQoL for either group after one year of follow-up; in fact, it remained stable during the time of the study, which is important as HRQoL seems to have a bi-directional relationship with increased PA. 16
A reduction of 15–20% in strength has been reported in every decade after 50 years of age, leading to deleterious effects on the performance of basic activities of daily living. 35 Seco et al. 36 described that 26% of adults over the age of 70 years could not easily climb stairs, 31% had problems carrying a bag weighting 35 kg and 36% had walking difficulties. Although no strength differences between the interventions were found in our study, there was a significant improvement in muscular strength during the follow-up that was not accompanied by an improvement in muscular endurance. We considered the long-term maintenance of handgrip and quadriceps strength in all participants as a positive result, as in older individuals increased muscular strength and endurance tend to reduce disability and to improve functional independence and HRQoL. 37 Further research regarding muscle strength and telerehabilitation interventions are needed in order to confirm our results.
Strengths and limitations
The present TRiCH study has several strengths. First, we were able to obtained objective measures of PA using an accelerometer while previous studies of internet-based interventions have relied solely on self-reported PA data. 38 Second, many patients expressed their preference for CB training; however, the random assignment allowed us to have a proper representation of the CR population in all groups and their behaviour in the long term. Third, although long-term adaptations are the ultimate goal of CR, 12 the number of studies evaluating the longer-term effects of CR interventions are disappointingly low. Thus the TRiCH study with a follow-up period of one year is one of the few studies that allowed a reasonable timeframe to assess the long-term effects of a telemonitoring programme during phase III of CR.
A limitation of this study is the lack of blinding of test personnel. However, as the main outcome measure was physical fitness, the effort of the participants can be compared through the RER and the Borg scale. 39 The study, as do most randomised controlled trials, had missing outcome data due mainly to technical problems or missing numbers in specific tests, but these were missing completely at random. CR includes important core components such as nutritional counselling, risk factor management and psychosocial management; but PA training comprises up to 70% of all CR activities. Therefore, in this study PA telemonitoring rather than telerehabilitation was assessed. 40
Conclusion
The results of this TRiCH study show that HB CR and usual care or prolonged CB CR are of similar value for maintaining EC, PA, anthropometric measures, muscle strength and HRQoL in the long term in CAD patients who participated in phase II CR.
Footnotes
Acknowledgements
The authors thank the patients who participated in the TRiCH study as well as the staff of the cardiac rehabilitation centre in UZ Leuven hospital for their support.
Author contribution
The first two authors are joint first authors. VC contributed to the conception and design of the work. AA and JC contributed to the acquisition, analysis, or interpretation of data for the work. VC and AA drafted the manuscript. JC, RB, MA and LV critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AA is supported by a doctoral research grant funded by the European Commission through MOVE-AGE, an Erasmus Mundus Joint Doctorate programme (2011-0015).