
Abstract
Purpose
The aim was to investigate the use of cardioprotective drug therapies (aspirin or other antiplatelet agents, β-blockade, renin-angiotensin-aldosterone-system-blockade (RAAS-blockade) and statins) and treatment targets achieved in a large cohort of patients with established coronary artery disease and diabetes across Europe.
Methods and results
EUROASPIRE III is an observational cross-sectional study of stable coronary artery disease patients aged 18–80 years from 76 centres in 22 European countries conducted in 2006–2007. The glycaemic status (prevalent, incident or no diabetes), the guideline treatment targets achieved and the use of pharmacotherapies were assessed at one visit 6-36 months after the index event. Of all 6588 patients investigated (women 25%), 4295 (65%) had no diabetes, 752 (11%) had incident diabetes and 1541 (23%) had prevalent diabetes. All four drugs were used in 44% of the patients with no diabetes, 51% with incident diabetes and 50% with prevalent diabetes respectively. Individual prescriptions for patients with no, incident and prevalent diabetes were respectively: aspirin or other antiplatelet agents 91, 93, and 91%; β-blockers: 81, 84, and 79%; RAAS-blockers: 77, 76, and 68%; statins: 80, 80, and 79%. The proportion of patients with coronary artery disease and prevalent diabetes reaching the treatment targets were 20% for blood pressure, 53% for low density lipoprotein cholesterol (LDL-cholesterol) and 22% for haemoglobin A1c (HbA1c).
Conclusion
This European study demonstrates a low use of cardioprotective drug therapies among patients with a combination of coronary artery disease and diabetes, which will be contributing to the poor achievement of risk factor treatment targets for cardiovascular prevention.
Introduction
Cardiovascular disease is the major cause of death worldwide and in Europe alone 4 million people die from it every year, representing 50% of the regional mortality.1,2 Indeed, cardiovascular disease explains 31% of deaths in men and 26% of deaths in women before the age of 65 in Europe.1,2 Diabetes is a rapidly increasing cardiovascular risk factor, and around 30% of all patients with coronary artery disease have type 2 diabetes mellitus (from now on referred to as diabetes).3–5 Patients with a combination of coronary artery disease and diabetes have a two times higher mortality than those without diabetes, making them a group at particularly high risk for a second vascular event and death.6,7 By using target driven pharmacological treatment as recommended in available guidelines, the prognosis can be improved to become almost equivalent to that of patients without diabetes.8,9 Given their higher absolute risk, the number needed to treat to avoid one cardiovascular event is substantially lower in patients with coronary artery disease and diabetes compared to those without diabetes. 8 Despite some improvement over time, pharmacological therapy of cardiovascular patients is still inadequate, especially in those with diabetes.8–10
The aim of the present study was to investigate the use of four cardioprotective drug therapies (aspirin or other antiplatelet agents, β-blockade, Renin-Angiotensin-Aldosterone-System-blockade and statin) and treatment targets achieved in a large cohort of patients with coronary artery disease with and without diabetes across Europe.
Methods
A detailed report of the European Action on Secondary and Primary Prevention by Intervention to Reduce Events III (EUROASPIRE III) has been given elsewhere.
11
In brief, EUROASPIRE III was an observational cross-sectional study conducted between 2006 and 2007, in patients with established coronary artery disease recruited from 76 volunteering centres in 22 European countries. The inclusion criteria were: age 18–80 years and established coronary artery disease defined as: hospitalisation for either (1) elective or emergency coronary artery by-pass graft surgery; (2) elective or emergency percutaneous coronary intervention; (3) acute myocardial infarction (AMI; ST elevation and non-ST-elevation myocardial infarction) or (4) acute myocardial ischemia but no evidence of infarction (troponin negative). The index event had to be ≥6 and <36 months before the planned date of the patient interview. The median time between the index event and interview was 1.2 years (IQR 1.0–1.8). Patients were identified from diagnostic registries, hospital discharge lists or other valid sources and contacted by phone or mail. Figure 1 shows the flow-chart of patient recruitment, patients attending interview and whose glycaemic status was established through self-report or fasting glucose.
Flow-chart of patient recruitment.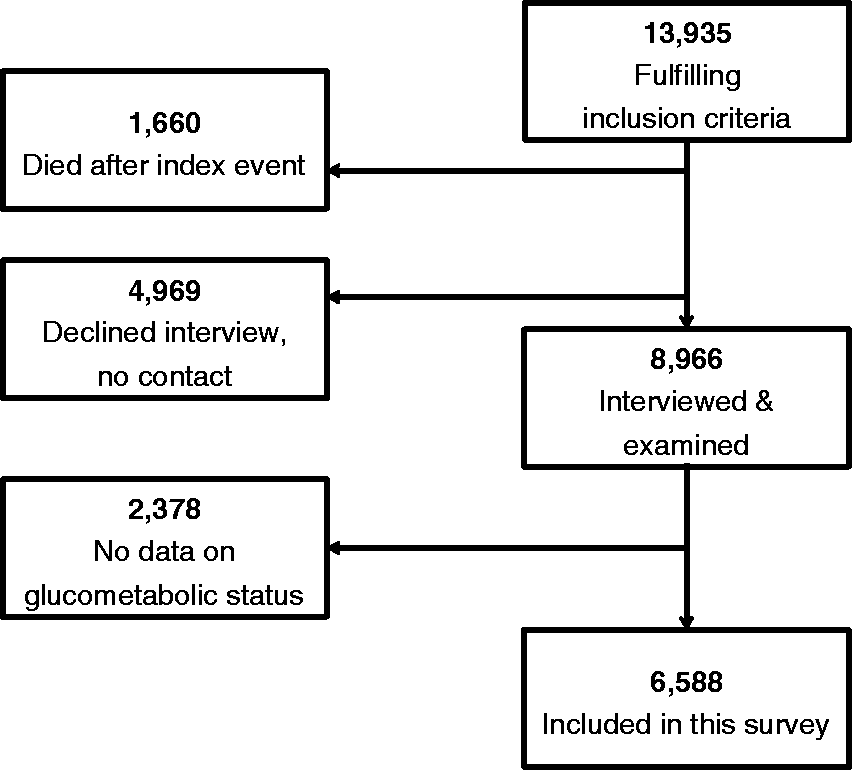
Trained research staff reviewed the medical records, interviewed and examined the patients and entered the data into an electronic central database.
The following measurements were performed:
Height and weight were measured in light indoor clothes without shoes (SECA scales model number 701 and measuring stick model 220; Hamburg, Germany). The scales were calibrated at the start of the survey. Blood pressure was measured twice on the right upper arm in the sitting position using automatic digital sphygmomanometers (Omron M5-I, Illinois, USA). Blood pressures in this report represent the average of these two recordings. Venous blood was retrieved for the analysis of serum analysis of serum total cholesterol and high density lipoprotein cholesterol (HDL-cholesterol), triglycerides, calculated low density lipoprotein cholesterol (LDL-cholesterol), plasma glucose (all patients) and in addition haemoglobin A1c (HbA1c) in those with self-reported diabetes. All analyses were performed at the Laboratory of Analytical Biochemistry, National Public Health Institute (Helsinki, Finland) fulfilling the requirements of the standard SFS-EN ISO/IEC 17025:2005 covering all analyses except glycated HbA1c.
Information about the patient’s pharmacological treatment was collected at the time of the interview. The patient was asked to bring an updated list of medications or the medication itself.
For this study patients were divided into three groups based on glycaemic state: prevalent (self-reported diagnosis of diabetes), incident (new cases of diabetes) and no diabetes. The diagnosis of incident diabetes (fasting glucose of > 7 mmol/L = 126 mg/dl), the use of four cardioprotective drug therapies (antiplatelet drugs, b-blockade, renin-angiotensin-aldosterone-system (RAAS) blockade and a statin) and treatment target attainment (blood pressure, LDL-cholesterol and HbA1c) were assessed at the time of the study visit. The treatment targets for patients with coronary artery disease were based on the joint 2003 European Guidelines on cardiovascular disease prevention: 12 (i) blood pressure <140/90 mmHg for patients without diabetes and <130/80 mmHg for patients with diabetes; (ii) total and LDL-cholesterol <4.5 mmol/L (175 mg/dL) and <2.5 mmol/L (<97 mg/dL) respectively; and (iii) HbA1c <6.1 DCCT % (43.2 mmol/mol). In addition, tests were performed to investigate the proportions that reached more as well as less strict treatment targets.
Data management
Data management was undertaken at the European Society of Cardiology's Euro Heart Survey Department, European Heart House, Nice, France. Data were collected electronically using a unique identification number for country, centre and individual. The data were submitted via the internet to the data management centre where checks for completeness, internal consistency and accuracy were run. All data were stored under the provisions of National Data Protection Regulations.
Ethical considerations
The study conformed to good clinical practice guidelines and followed the recommendations of the Helsinki Declaration. National coordinators obtained approvals from Local Research Ethics Committees and all participants signed a consent form following oral and written information.
Statistical analyses
Patient characteristics
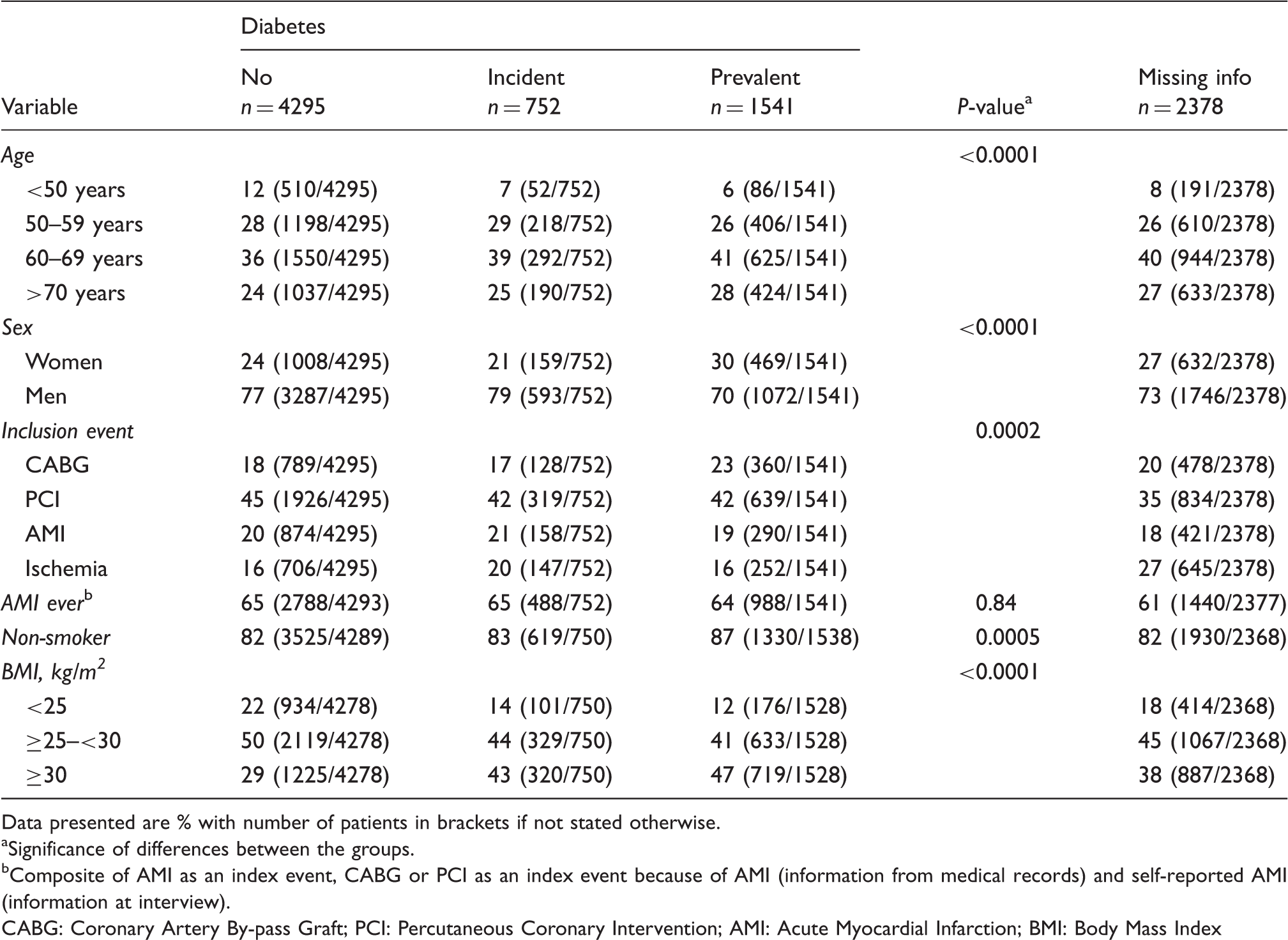
Data presented are % with number of patients in brackets if not stated otherwise.
Significance of differences between the groups.
Composite of AMI as an index event, CABG or PCI as an index event because of AMI (information from medical records) and self-reported AMI (information at interview).
CABG: Coronary Artery By-pass Graft; PCI: Percutaneous Coronary Intervention; AMI: Acute Myocardial Infarction; BMI: Body Mass Index
Results
A total of 13935 medical records were reviewed and 8966 (64%) patients interviewed. The present study population comprises 6588, 74% of those interviewed, with available information on their glycaemic state. In the study population 65% had no diabetes, 11% had incident diabetes and 23% had prevalent diabetes. Patient characteristics are presented in Table 1. Those with incident and prevalent diabetes were older and more obese but smoked less frequently. The baseline characteristics of the 2378 patients with missing data on their glycaemic state did not differ from the patients included in the analyses (Table 1). Likewise there were no major differences in gender, age and recruiting event between the 4969 patients not attending the interview, the 2351 interviewed but with missing data on glycaemic state and the investigated population of 6588 patients (data not shown).
Use of pharmacological therapy in percentage (n/total n)
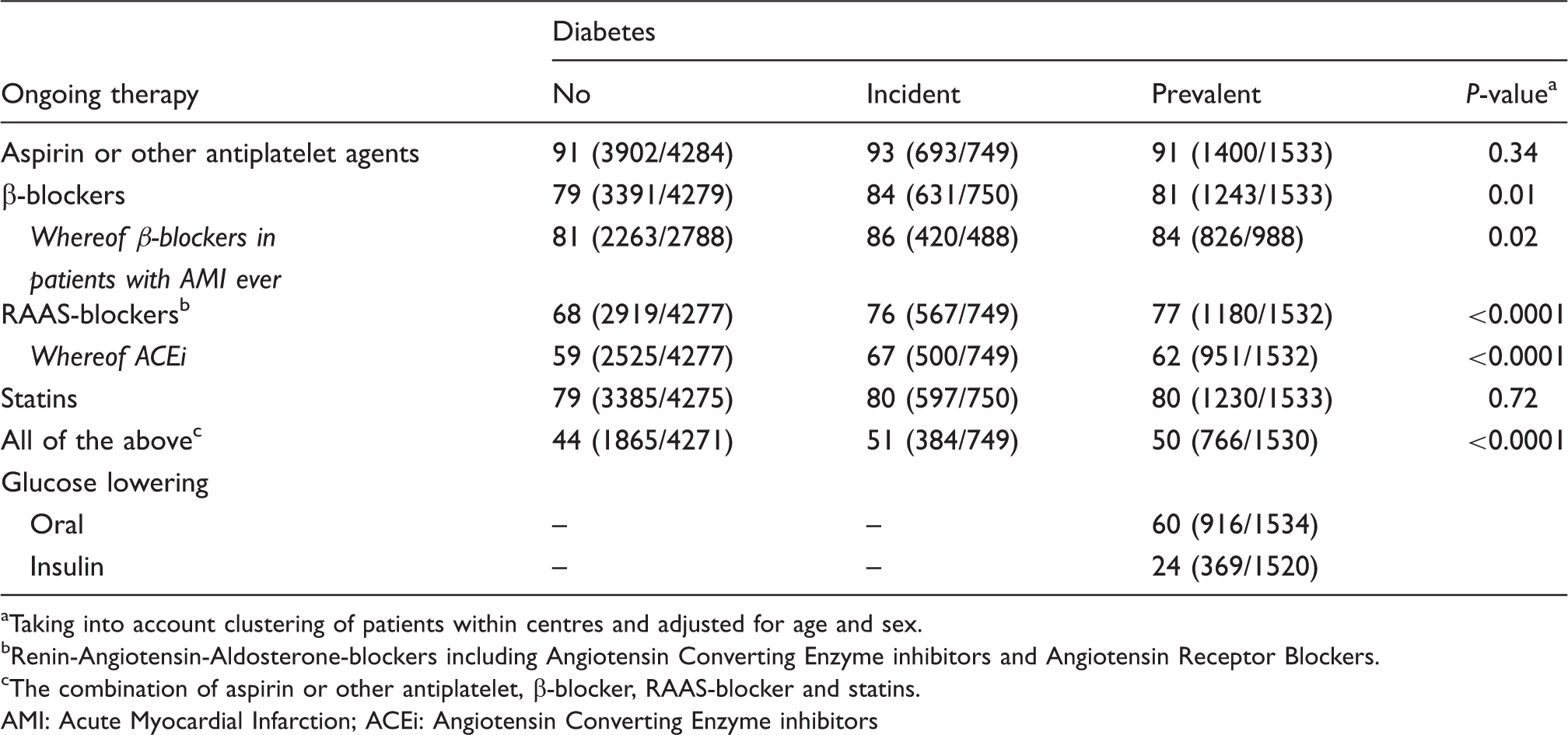
Taking into account clustering of patients within centres and adjusted for age and sex.
Renin-Angiotensin-Aldosterone-blockers including Angiotensin Converting Enzyme inhibitors and Angiotensin Receptor Blockers.
The combination of aspirin or other antiplatelet, β-blocker, RAAS-blocker and statins.
AMI: Acute Myocardial Infarction; ACEi: Angiotensin Converting Enzyme inhibitors
In all three groups >97% of the patients reported that they never or seldom missed or altered their medication.
Figure 2 shows the proportion of patients reaching different blood pressure levels (<150/100; <140/90; and <130/80 mmHg respectively). Half of the patients with no diabetes and one fifth of those with prevalent diabetes reached the recommended blood pressure target of <140/90 mm Hg and <130/80 respectively. When applying a blood pressure target of <140/80 as recommended in the 2012 prevention guidelines 28% of the patients with prevalent diabetes reached this treatment target.
14
Percentage of patients reaching blood pressure treatment target by diabetes state (no, incident, prevalent) accounting for clustering of patients within centres and adjusted for age and sex.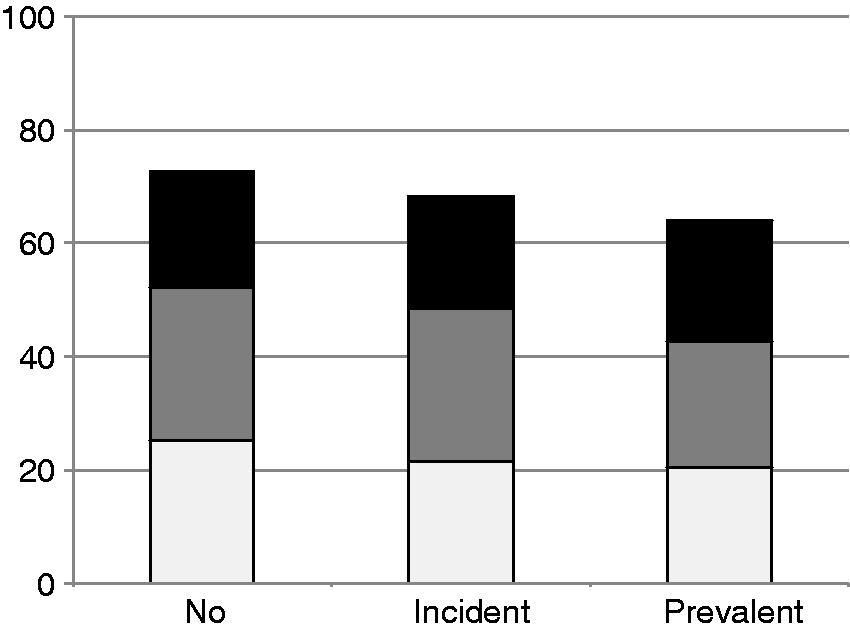
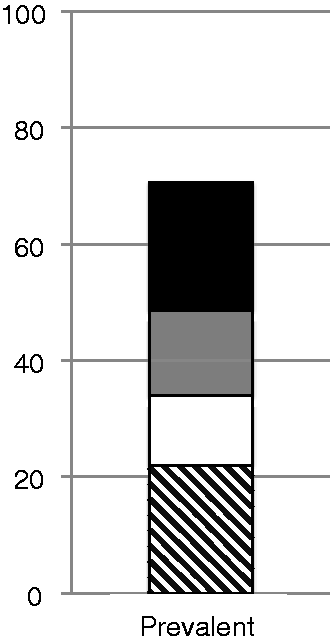
Forty-four per cent of the patients with no diabetes, 40% of those with incident diabetes and 53% with prevalent diabetes reached the treatment target for LDL-cholesterol of <2.5 mmol/l (<97 mg/dL) for all three groups. Figure 3 shows the proportion of patients reaching different LDL-cholesterol levels (<3.0; <2.5; <1.8 mmol/l =<116; <97; <70 mg/dL). The total cholesterol target of <4,5 mmol/L (<175 mg/dL) was reached by 49% of the patients with no diabetes, 41% in patients with incident diabetes and 55% in patients with prevalent diabetes. The differences between the groups were statistically significant (p < 0.0001). Out of the patients with prevalent diabetes 22% reached the guideline treatment target of HbA1c <6.1% (<43 mmol/mol) as shown in Figure 4.
Percentage of patients reaching LDL-cholesterol treatment target by diabetes state (no, incident and prevalent) accounting for clustering of patients within centres and adjusted for age and sex. Percentage of diabetes patients reaching HbA1c (DCCT) treatment targets accounting for clustering of patients within centres and adjusted for age and sex.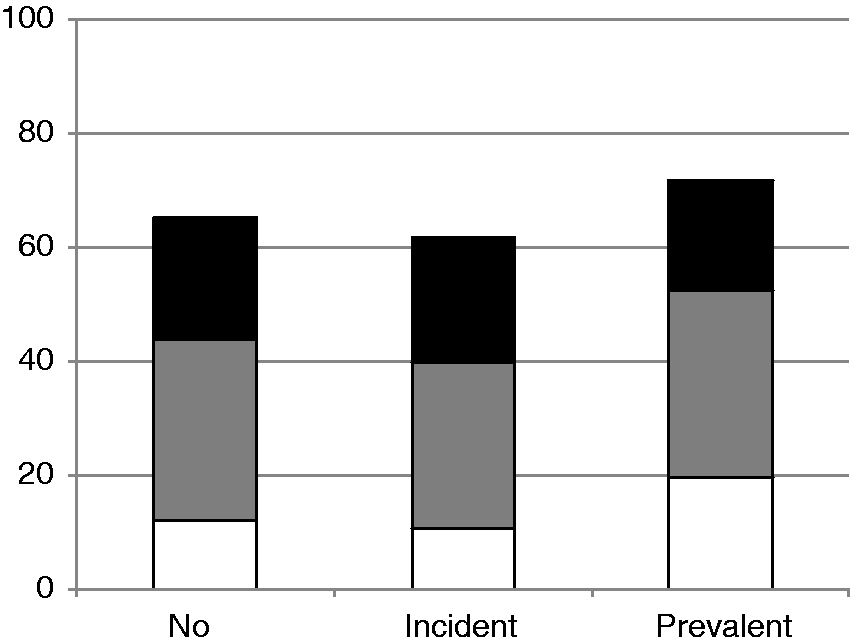
Healthcare provider delivering the care presented as percentage (n/total n)
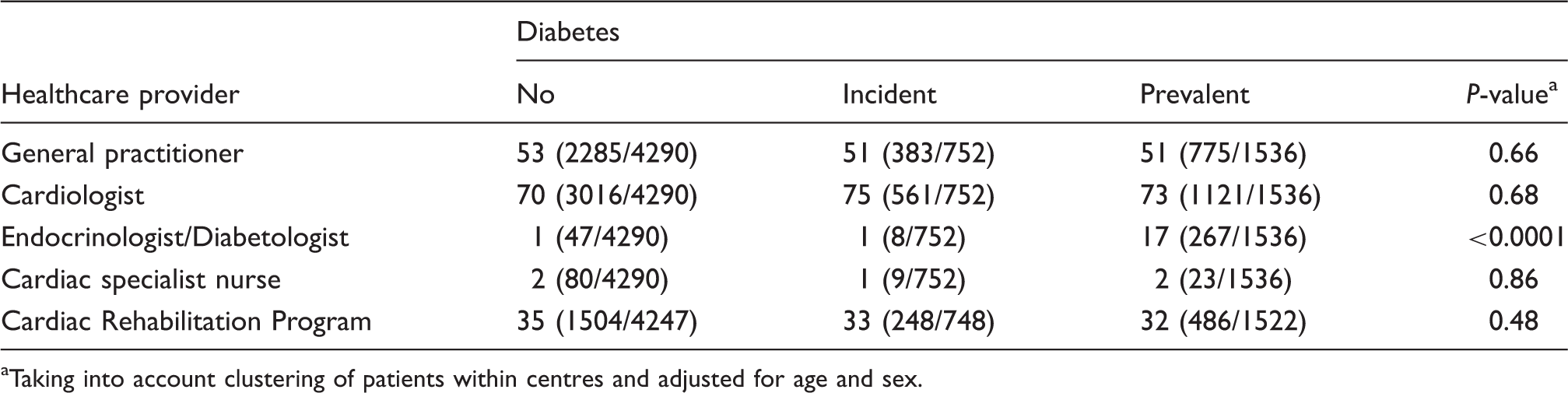
Taking into account clustering of patients within centres and adjusted for age and sex.
Discussion
This survey demonstrates a low combined use of the four cardioprotective drug therapies, which will have contributed to the poor attainment of risk factor treatment targets for cardiovascular prevention, especially among patients with diabetes.
These findings are consistent with previous reports of inadequate use of cardioprotective treatments and a failure to achieve blood pressure, lipid and glycaemic targets in patients with coronary artery disease and diabetes.9,11,15 In EUROASPIRE II, conducted between 1999 and 2000, 23% of the patients with coronary artery disease and diabetes used four or more out of eight specified drugs. In the Euro Heart Survey, conducted in 2003, the use of the same four drug therapies examined in this survey was about 43%. Thus, only marginal improvement has occurred in the care of patients with diabetes, of whom 50% now use all four drugs. It is noteworthy that patients with prevalent and incident diabetes used all four cardioprotective drug therapies more frequently than patients without diabetes. Still they reached the recommended treatment targets less often, indicating that intensified pharmacologic treatment is required.
Blood pressure, LDL-cholesterol and HbA1c were analysed according to different cut points to further investigate the distributions of these risk factors. The pattern of failing to reach treatment targets was still apparent when less stringent targets were analysed. To enable a comparison with current 2012 European prevention guidelines we have presented the most recent targets: LDL-cholesterol (<1.8 mmol/L or <70 mg/dL), blood pressure (<140/90 mmHg without and <140/80 with diabetes) and HbA1c (<7.0% or <53 mmol/mol). 14 Even with the more conservative targets for blood pressure and diabetes it is still only a minority of patients who achieve them, and with a more intensive LDL-cholesterol target the proportion achieving this is even smaller.
Patients with known diabetes received more pharmacological treatment than those without. This was largely a consequence of the higher prescription of RAAS-blockers, as previously observed in EUROASPIRE II and the Euro Heart Survey of diabetes and the heart.9, 15 Still blood pressure control was remarkably poor with only 20% of patients with prevalent diabetes within the recommended target; a similar proportion was reported in EUROASPIRE II (22%). Indeed 37% had a blood pressure exceeding 150/100 mmHg, which is far from optimal in this population. Adequate blood pressure control in patients with diabetes often requires two or three different antihypertensive drugs, and thus a potential explanation might be that an insufficient number of drug classes were used in dosages that were too low. 16
The combination of Angiotensin converting enzyme inhibitor (ACEi) and angiotensin receptor blocker (ARB) to one group, RAAS-blockade, may be discussed in the light of some, but not all, meta-analyses indicating that ARB may be less efficient as regards cardiovascular protection. 17 However, the head to head comparison of the ARB telmisartan and the ACEi ramipril in the ONTARGET trial showed no significant differences in any of the outcome measures. 18 Moreover the position to combine the two types of RAAS- blockers gains support by the recently published European guidelines for hypertension. 19
A similar proportion of patients with and without diabetes were on statins, and the use of such drugs had increased considerably from EUROASPIRE II (54%) to EUROASPIRE III (85%). As a consequence 53% of patients with diabetes had a LDL-cholesterol <2.5 mmol/l (<97 mg/dL) compared to just 25% in EUROASPIRE II. This shows that new knowledge can be widely adopted even if it takes time. Gaede and Pedersen 20 applied the UKPDS risk engine 21 to calculate the actual contribution of different risk factors for cardiovascular risk reduction in the comprehensively treated group of the STENO 2 population. They found that the most important contributor was lowering of lipids (about 75% of the impact) followed by glucose (13%) and blood pressure-control (11%).
Glucose control was poor in the patients with prevalent diabetes with only 22% reaching the HbA1c target of <6.1% (43 mmol/mol). Despite an association between increasing hyperglycaemia and macrovascular complications the benefits of strict glucose control had at the time of the survey been seen as less compelling and the optimal glucose target put under debate. 22 The most recent guidelines recommend an HbA1c of <7.0% (53 mmol/mol) rather than <6.1% (43 mmol/mol). 23 A target of 7.0% was, however, reached by only 50% of the patients. Considering that microvascular complications appear above the recommended HbA1c target this cannot be seen as a satisfactory patient management.22,24 Even though patients with incident diabetes cannot be expected to be treated to diabetes-targets it is noteworthy that 11% of the investigated population were diagnosed with new diabetes based on an elevated fasting glucose at the EUROASPIRE III study visit. As they had remained undiagnosed for 6–36 months after their index coronary event this indicates a lack of knowledge or organisation on the importance to investigate glucose metabolism. 23
A minority (17%) of patients with diabetes were seen by an endocrinologist, and this very low access to specialist care might have had a negative impact on their treatment. Moreover, many patients were attended by multiple healthcare providers, which might have led to no specific physician perceiving himself or herself as responsible for the complete care of the patient. It has previously been shown that the transfer of patients to outpatient care is suboptimal which might also be the case in the present study. 25 It is reasonable to state that the organisation of the care for these patients is largely responsible for the inadequate therapeutic management and risk factor control demonstrated by this survey. One improvement to the organisation of care could be to depute one responsible healthcare provider and/or a nurse-led clinic providing comprehensive prevention including guided lifestyle advice including smoking cessation, risk factor monitoring and adherence with cardioprotective drugs. 26 In this perspective education, not only of the healthcare providers, but also the patients and their relatives, may serve as a tool to accomplish better treatment with healthcare providers and patients taking joint responsibility working towards the same targets. 27 Another potential improvement might be check lists and indication-specific order sets incorporated in electronic medical records making clinical guidelines easily accessible to the responsible physician, who also may become automatically alerted if a target is not reached. Such an alerting system may activate improved management or a note why, in a specific patient, treatment can or should not be driven further. 28 This strategy might help to decrease the impact of clinical inertia that is often seen in the management of cardiovascular risk factors. 29
The time elapsed between the index event and the interview (1.2 years) should be sufficient to institute and alter treatment towards guideline recommended targets. Moreover, patient compliance is not believed to play a major role since >97% of the patients responded that they never or seldom missed or altered their medication. A more likely explanation is that many patients were simply not prescribed the full combination of all four cardioprotective drug therapies. In this study we evaluated the same four drug therapies as those analysed in the Euro Heart Survey on diabetes and the heart. 9 It is reasonable to assume that patients with coronary artery disease and diabetes should have a combination of aspirin or other antiplatelet agents, statin and ACEi/ARB-inhibitors and quite frequently also a beta-blocker as prophylaxis following a myocardial infarction or angina treatment. Although there are contraindications to the use of each of these drugs they are unlikely to be relevant in the vast majority of the patient population described in this study because. The benefits of prescribing such drug therapies outweigh any potential harms.
Study limitations
The classification of a patient as having incident diabetes was based on a single fasting glucose. This diagnosis should preferably be based on two fasting glucose values, which was impossible because of study logistics. Using fasting glucose alone will not detect those patients with impaired postprandial glucose metabolism that would have been disclosed by an oral glucose tolerance test or possibly by an HbA1c.3,30,31 This means that the group free from diabetes is likely to contain some individuals with undetected diabetes. Never the less the proportion of 35% patients with self-reported diabetes concurs with prevalence estimates from other studies reporting on dysglycaemia in patients with coronary artery disease.15,32 The potential misclassification of patients with no diabetes when they do have diabetes is of limited importance in the present context since the major differences are between patients with prevalent and those with no diabetes.
It may be argued that beta-blockers should only be included as evidence-based treatment in patients with a previous myocardial infarction or with heart failure. However, and as underlined in the 2013 ESC guidelines on stable coronary artery disease beta-blockers may be protective in patients with stable coronary artery disease and are recommended as first line therapy against angina pectoris. 33 Moreover people with diabetes often require a combination of several blood pressure lowering drugs to reach the recommended target and beta-blockers, although not a first line choice, is recommended as add on therapy. 23
As can be seen in Table 1 the proportions recruited because of acute AMI are similar in the three groups and when a composite was created 64–65% of the patients in all groups had an AMI before the interview. This proportion is likely to be an underestimate since the information was retrieved retrospectively during the interview or from medical records. No information on left ventricular dysfunction was retrieved from the medical record and echocardiography was not performed.
Furthermore, EUROASPIRE III may have a positive selection bias. Participating centres included university teaching hospitals and specialist cardiac centres. Such centres may have a particular interest in cardiovascular prevention, likely underestimating the true problem.
Conclusion
Although the use of cardioprotective drugs individually was common there was a low use of all four cardioprotective drug therapies in combination and as a consequence treatment targets were often not reached. This was particularly apparent for blood pressure and glucose control in patients with self-reported diabetes, and is a serious threat to the patient’s prognosis. The delivery of preventive care, the type of healthcare provider and how care is organised are likely to be important factors in determining patient outcomes.
Footnotes
Acknowledgements
The EUROASPIRE III survey was carried out under the auspices of the European Society of Cardiology, Euro Heart Survey programme. EUROASPIRE Study Group is grateful to all the hospitals in which the study was carried out. Their administrative staff, physicians, nurses and other personnel helped us in many ways and we very much appreciate this. We are also grateful to the patients who participated in the study.