
Abstract
Background
Cardiac rehabilitation (CR) is an evidence-based intervention to increase survival and quality of life. Yet studies consistently show that elderly patients are less frequently referred to CR, show less uptake and more often drop out of CR programmes.
Design
The European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE) project consists of an observational study and an open prospective, investigator-initiated multicentre randomised controlled trial (RCT) involving mobile telemonitoring guided CR (mCR).
Objective
The aim of EU-CaRE is to map the efficiency of current CR of the elderly in Europe, and to investigate whether mCR is an effective alternative in terms of efficacy, adherence and sustainability.
Methods and results
The EU-CaRE study includes patients aged 65 years or older with ischaemic heart disease or who have undergone heart valve surgery. A total of 1760 patients participating in existing CR programmes in eight regions of Europe will be included. Of patients declining regular CR, 238 will be included in the RCT and randomised in two study arms. The experimental group (mCR) will receive a personalised home-based programme while the control group will receive no advice or coaching throughout the study period. Outcomes will be assessed after the end of CR and at 12 months follow-up. The primary outcome is VO2peak and secondary outcomes include variables describing CR uptake, adherence, efficacy and sustainability.
Conclusion
The study will provide important information to improve CR in the elderly. The EU-CaRE RCT is the first European multicentre study of mCR as an alternative for elderly patients not attending usual CR.
Introduction
Cardiovascular disease (CVD) is responsible for over four million deaths in Europe each year. 1 The population of elderly patients with coronary heart disease (CHD) has increased because of increasing age at onset of CVD, the aging of the population and the development of life-saving pharmacological and interventional therapies. A cardiac event in an elderly person is often the beginning point of gradual deterioration and is followed by a high rate of recurrent events. The burden of CVD is not only huge for patients and the healthcare sector, but also encompasses a large economic strain with estimated annual costs of €169b in Europe. 2 As a result, maintaining autonomous, independent and active elderly patients, after acute coronary syndrome (ACS) or coronary revascularisation, is a huge health and social challenge within Europe and the urgent need for effective (and cost-effective) patient-centred cardiac care is increasing.
Only about one third of CVD patients in Europe receive any form of cardiac rehabilitation (CR), with generally lower uptake in the elderly.3,4 The elderly patient is characterised by more co-morbidities, more physical impairment, reduced mobility and a less physically active lifestyle. Additionally, a larger proportion of elderly patients have psychosocial disadvantages such as living alone and transportation difficulties. Although the elderly account for the majority of cardiac admissions and procedures, programmes and studies on CR have traditionally focused on younger patients. The current approach for CR is therefore often less appropriate for the elderly, despite the similar benefits from CR as their younger counterparts.5,6 Together with their high risk of recurrent events, the elderly CHD patient is the group most in need of CR, yet studies consistently show that elderly patients are less frequently referred to CR, show less uptake and drop out more often from CR programmes.7–9
Home-based CR programmes have been suggested as an alternative to centre-based CR and may provide a good alternative for the elderly patient unable or unwilling to participate in a centre-based CR.10,11 Studies have indicated that home-based programmes are non-inferior to centre-based, supervised programmes.7–9 For many elderly patients, transportation to the standard, centre-based, centralised CR programme is a barrier to participation and leads to lower participation rates and inequality in access to care. This barrier may be overcome by utilising novel technologies developed in tele-rehabilitation. Investigation of mobile telemonitoring guided CR (mCR) as an effective, comprehensive CR programme for the elderly is very promising.
The European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE) project (www.eu-care.org) is a programme conducted in collaboration between eight European healthcare institutions in seven European countries. The main objective of the EU-CaRE project is to obtain the evidence base to improve, tailor and optimise CR programmes regarding sustainable effectiveness, cost-effectiveness and participation level in the elderly, a group defined as patients aged 65 years or above.
Methods
This aim will be pursued in two parallel studies (Figure 1): EU-CaRE, an observational study focusing on predictors of uptake, cost-effectiveness, adherence and sustainability of diverse CR programmes in Europe, and EU-CaRE RCT, a randomised controlled trial (RCT) testing the ability of mCR to improve sustainable effects of CR in elderly patients that would not participate in the regular CR programme offered, to establish its cost-effectiveness, and to investigate the means of increasing CR participation among the elderly by mCR. Both EU-CaRE studies are approved by all relevant medical ethics committees and registered at trialregister.nl (NTR5306 and NTR5308). All patients gave written informed consent before entering a EU-CaRE study. In this article, the EU-CaRE RCT will be explained in context of the total project and in relation to the observational study.
Flowchart of European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE) patient inclusion. CR: cardiac rehabilitation; RCT: randomised controlled trial.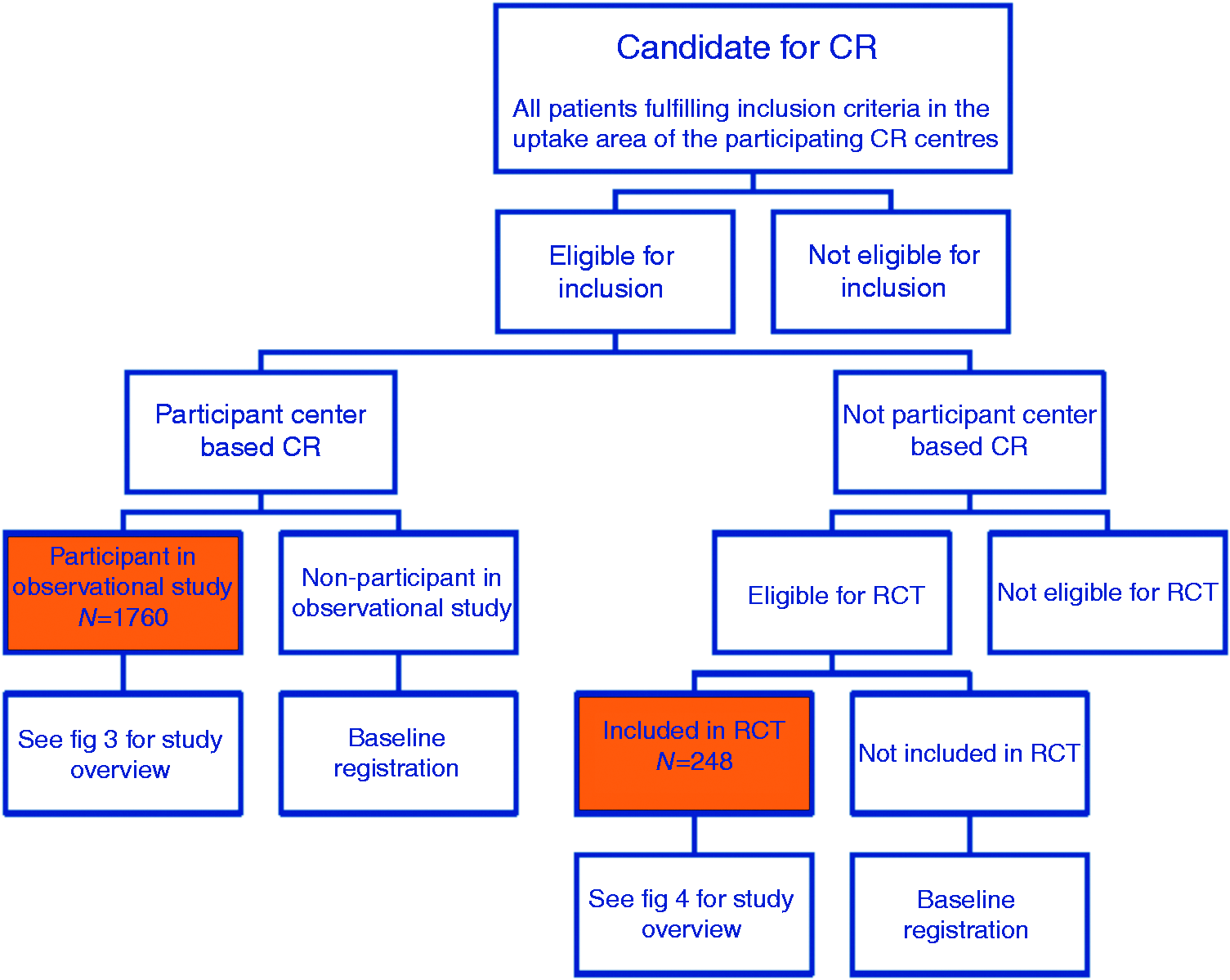
EU-CaRE observational study
Design and objective
Description of centre-based cardiac rehabilitation (CR) programme in participating centres.

CAD: coronary artery disease; CHF: chronic heart failure; CPET: cardiopulmonary exercise testing; FKT: function test; GP: general practitioner; GUCH: grown ups with congenital heart diseas; PAD: peripheral artery disease.
Study population
Inclusion and exclusion criteria for European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE).
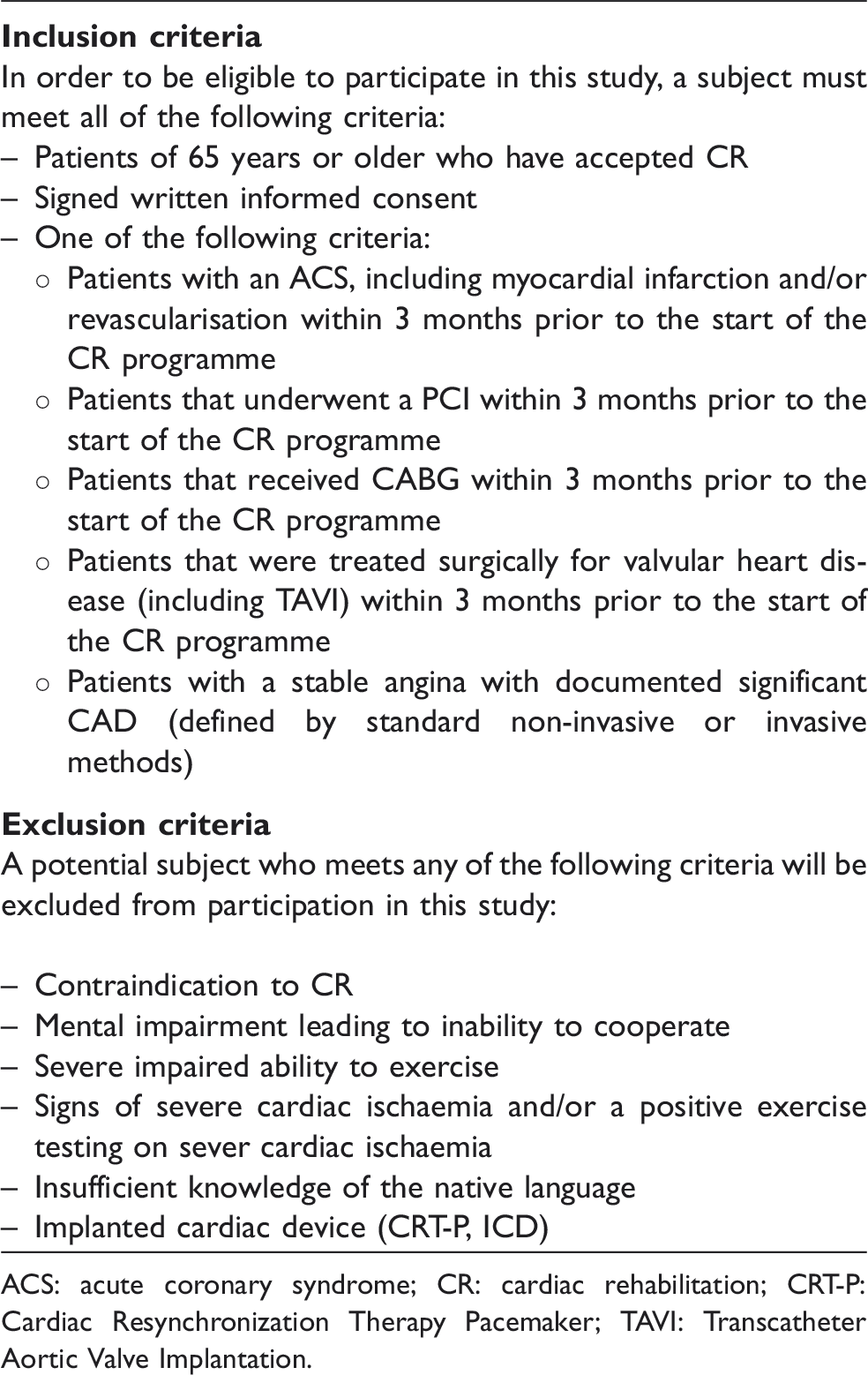
ACS: acute coronary syndrome; CR: cardiac rehabilitation; CRT-P: Cardiac Resynchronization Therapy Pacemaker; TAVI: Transcatheter Aortic Valve Implantation.
Participants in the observational study will be monitored at start of the CR programme, T0, end of CR programme, T1, and 12 months after start of the CR programme, T2. Drop-outs from the study will be registered as well as their reason for drop-out.
Outcome measures
Overview of data acquisition in the observational study.

BMI: body mass index; CR: cardiac rehabilitation; CV: cardiovascular; GP: general practitioner; QoL: quality of life; HBA1c: Hemoglobine A1c; HIIT: High Intensity Interval Training; LVEF: left ventricular ejection fraction.
All data sought registered on participants and non-participants of CR alike.
For measuring care utilisation, costs per patient based on clinical admission days, emergency and outpatient clinic visits, general practitioner (GP) visits for cardiac (related) complaints or issues, cardiac-related radiology/physiology, nuclear or laboratory tests and other cardiac interventions will be calculated. This endpoint is essential for assessing cost-effectiveness.
The setting in which CR programmes is carried out may be of influence on outcome, especially in the elderly. A number of CR programme-related parameters that might influence outcome will be registered: in/out patient, separate/same institution, with/without multidisciplinary counselling, duration of programme, frequency of exercise session, training volume and training intensity.
For patients enrolled in CR the following data will be registered: demographics, race/ethnicity, educational attainment, employment status, cohabitation, social network, involvement in voluntary work, medical history including co-morbidity including chronic heart failure (CHF), valvular heart disease or atrial fibrillation, indication for CR (index event), exercise capacity, CVD risk factors, medication, symptoms (chronic compartment syndrome (CCS) and New York Heart Association functional classification (NYHA)) and left ventricular ejection fraction. Clinical assessment of patients includes: Cardiopulmonary exercise testing (CPET) or alternatively six-minute walk test (6MWT) in elderly patients not able to perform a CPET, blood pressure, body mass index (BMI), waist-hip ratio, lean body mass, spirometry, heart rate and rhythm. Blood samples will be analysed for the following: renal function, HbA1c and serum lipids. Questionnaires include three distinct validated questionnaires Patient Health Questionnaire-9 (PHQ-9), Generalised Anxiety Disorder-7 (GAD-7) and 36-item Short Form Health Survey version 2 (SF-36v2).
EU-CaRE RCT
Design and objective
The trial is an open, prospective, investigator initiated multicentre RCT. The objective of EU-CaRE RCT is to assess whether mCR as an alternative for patients who decline participation in a conventional CR programme, is an effective means of increasing participation and adherence of elderly patients to a CR programme, and whether this results in better sustained effects. Patients will be randomised in two study arms to either: (a) join mCR programme for six months, or (b) no mCR programme (control). Both groups have an additional six months of follow-up after the first period without any intervention.
Study population
A total of 238 patients will be included from five European countries. The Departments of Cardiology of five European cardiac institutions participate in the EU-CaRE RCT: Isala (Zwolle, The Netherland), Region Hovedstaden (Copenhagen, Denmark), Assistance Publique – Hôpitaux de Paris (Paris, France), Univerisität Bern (Bern, Switzerland), and Servizo Galego de Saúde (Santiago de Compostella, Spain). All patients eligible for inclusion in EU-CaRE observational study (Table 2), but refusing regular CR are candidates for EU-CaRE RCT. No access, availability or insufficient knowledge of a computer with Internet, and implanted cardiac device (ICD, pacemaker) are additional exclusion criteria.
Intervention
Patients randomised to intervention will undergo six months of telemonitored guidance followed by six months without telemonitoring. The mCR programme involves a home-based programme in which patients are supplied with a heart rate belt to wear while exercise training and a smartphone/application (app) with a data subscription from MobiHealth BV. The wireless connected heart rate belt measures the heart rate of the patient during the activity and the data are subsequently transferred to the smartphone app by a Bluetooth connection. Through this app, patients are able to measure and register physical activity, heart frequency and intensity (BORG scale) and can monitor progress. The patient has access to a MobiHealth Rehabilitation secured web portal where data are presented and compared to their personal goals for activities. The research team (typically a CR nurse or physiotherapist) also has access to the web portal to monitor progress of participants, advise on rehabilitation approach and stimulate compliance at regular intervals described below.
Patients are instructed to exercise while wearing the heart rate monitor for a minimum of five days per week for at least half an hour at an individually selected level of intensity and self-chosen type of activity. The outcomes of the CPET on the first visit (T0) will guide the individual heart rate zones. A personal guideline regarding the intensity and frequency for the self-chosen activity for the patient is entered once at the start of the study by the researcher/nurse. During training sessions, the patients wear the heart rate monitor and select on their smartphone the type of activity they are going to perform from a predefined list (cycling, running, walking, home trainer, gardening, etc.). After finishing the exercise, patients enter the rate of perceived exertion for the training session (6–20 BORG score). Accordingly, the duration, intensity (based on the heart rate zones) and BORG score of each training/activity are collected by the smartphone and transferred to a secured website where both patient and researchers/nurses involved in the study can view the results.
The aim of mCR is to improve the self-management skills, stimulate patients to exercise independently and increase self-confidence. During the first month patients receive weekly individual coaching and feedback on their training results by telephone, in the second month they will be coached every two weeks, and in months 3–6 one monthly call will be held. For the individual coaching the motivational interviewing method is used. The concept of motivational interviewing evolved from experience in the treatment of problem drinkers. 12 Motivational interviewing is a directive, client-centred counselling style for eliciting behaviour change by helping people to explore and resolve ambivalence. Researchers involved in the RCT have received training on motivational interviewing during the initiation visit. Furthermore, a standard operating procedure for the individual coaching is used in order to ensure a similar mode of operation. 13 At the end of the first six months, the patients are asked to return the heart rate monitor and smartphone. In the subsequent six months until the end of the study patients will receive no further coaching or feedback.
Patients randomised to the control group will not receive any form of CR. During the 12-month study period both groups will receive locally defined standard patient care.
Randomisation
Before randomisation patients will receive oral and written information and sign a consent form. Patients will be randomised 1:1 to active intervention or control by a centralised computerised allocation system, applying an algorithm that prevents the care providers and/or the investigators from predicting the outcome of the randomisation process. It is not possible for the full research team to be blinded towards the allocation but centres are instructed to have CPET performed by personnel not knowing the randomisation outcome and to inform patients afterwards on the randomisation outcome.
Study endpoints, baseline and follow-up assessments
The patient assessment and measurements will be performed at baseline (T0), six months (T1) and end of follow-up at 12 months (T2) (Figure 2, Table 4).
Overview of assessments in European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE) randomised controlled trial (RCT). CR: cardiac rehabilitation; CVD: cardiovascular disease; MACE: major adverse cardiovascular event; mCR: mobile telemonitoring guided CR. Overview of data acquisition for European study on effectiveness and sustainability of current cardiac rehabilitation programmes in the elderly (EU-CaRE) randomised controlled trial (RCT). BMI: body mass index; CR: cardiac rehabilitation; ECG: electrocardiogram; mCR: mobile telemonitoring guided CR. Routine practice. Between T1 (6 months) and T2 (12 months) monitoring of care utilisation and registration of events is by monthly telephone calls with the participant.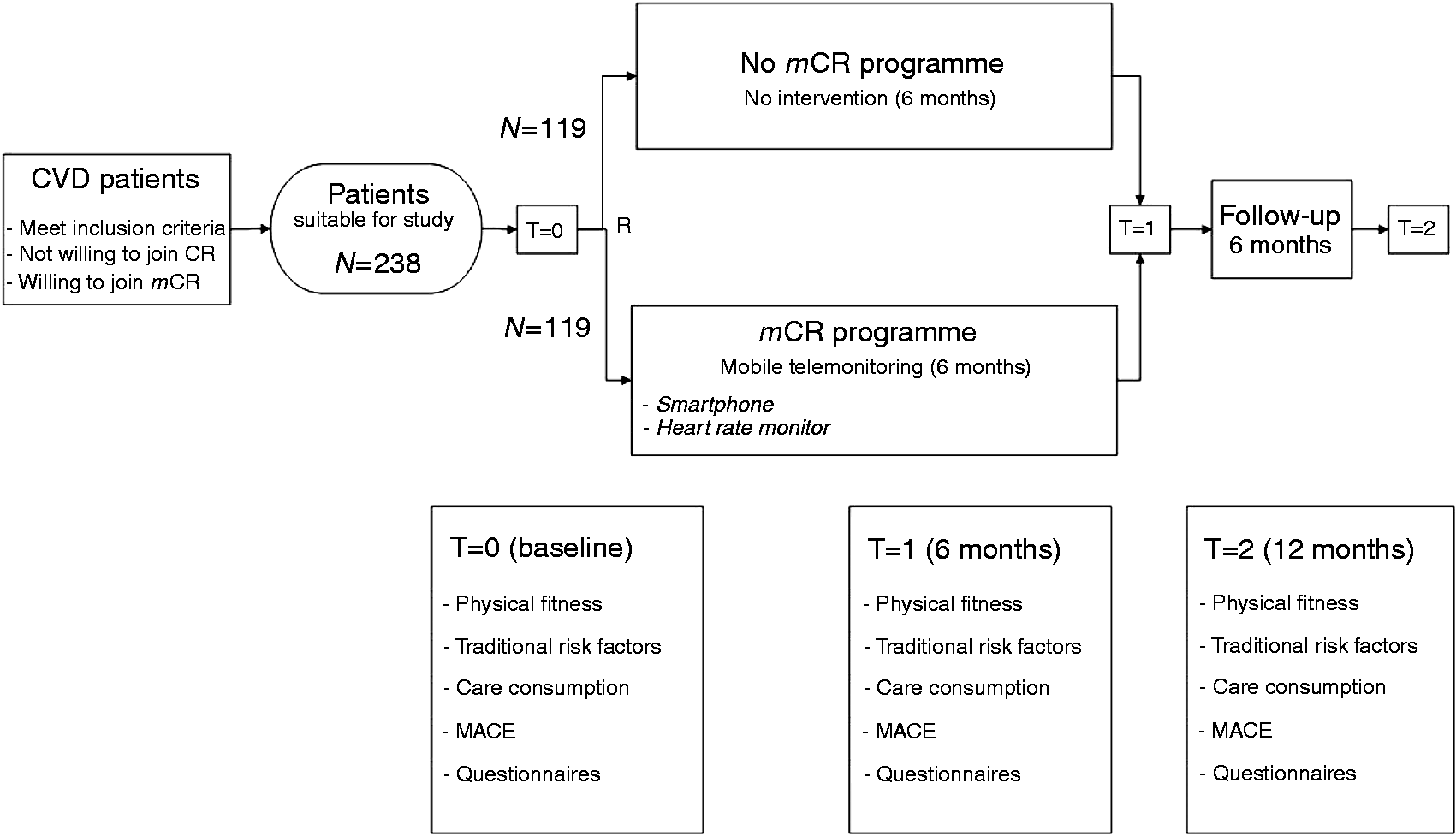

Physical fitness defined as VO2peak is currently the best predictor for sustained patient health outcomes and change in peak oxygen uptake (VO2peak) derived from CPET at six months compared to VO2peak from baseline, was chosen as primary endpoint.14,15
Secondary endpoints are changes in the following conventional CVD risk factors: lipid profile, hemoglobine A1c (HbA1c), renal function, lean body mass, blood pressure and smoking habits; changes in depression score assessed by: PHQ-9 questionnaire; anxiety score assessed by GAD-7 questionnaire, and Quality of Life assessed by SF-36v2 Physical Component Summary Score and Mental Component Summary Score and MACEs, a composite of all-cause mortality, near sudden cardiac death and hospital admission for cardiovascular disease. MACEs will be registered and/or collected by monthly telephone calls with the participants throughout the study period.
Care utilisation will be expressed as costs per patient based on clinical admission days, emergency and outpatient clinic visits, GP visits for cardiac-related complaints or issues, cardiac-related radiology/physiology, nuclear or laboratory tests and other cardiac interventions. For each country cost prices per activity will be assessed and for each patient the cardiac problem-related costs can be calculated.
The patient-related data that will be collected are the same as in the observational. Additional to that, the following data will be registered: number of training sessions, logged volume and intensity of training sessions and patient compliance to the programme. Full compliance will be defined as fulfilling the planned exercise session with mCR for at least 30 min, five days per week.
Patients can leave the study at any time for any reason if they wish to do so without any consequences. Patients will not be replaced after withdrawal from the study. Drop-outs from the study will be registered as well as their reason for drop-out. They will be encouraged to participate in follow-up visits and will be included in intention to treat analyses. Patients who experience a new event will receive normal follow-up.
Sample size calculation and projected statistical analyses
For the randomised tele-monitoring trial, the sample size calculation is based on the expected difference in increase in level of 3.0 ml/kg/min between the control and intervention group with an estimated standard deviation of 5 ml/kg/min in the intervention group and 6 ml/kg/min in the control group. Assuming 80% power and a 5% two-sided significance level (a = 0.05), the sample size (n) required to achieve a probability of 80% of detecting a difference in an increase level between two independent groups is n = 55 per randomisation group. Since this is a multi-centre study in different countries, we will use an adjustment based on the estimated intraclass correlation coefficient (ICC) for the study centres to calculate the sample size. An ICC of 0.05 is used in the sample size calculations. After adjustment for the ICC, the sample size in n = 83 per randomisation group. Based on 30% withdrawal we aim for a group size of n = 119 per randomisation group (n = 238 in total). Five centres will participate in the RCT so we will aim at including 48 patients per centre. As this is a cooperative trial, centres may recruit more patients than this recruitment goal. When one centre starts to dominate enrolment, however, recruitment might need to be capped. The total sample size (n = 238) would be sufficient to detect a clinically and physiologically relevant change in peak oxygen consumption, despite a 30% dropout.
The primary endpoint of the RCT is the change in VO2peak level between baseline and six months and the null hypothesis that there is no difference in mean change in VO2peak level between the two groups. Group comparison will be by linear mixed models with the intervention as a fixed effect, the effect of centre on the outcome modelled with a random effect and adjustment for baseline value of VO2peak. A two-sided p-value of less than 0.05 will be considered to be statistically significant. Similar analyses will be performed for effects at 12 months and for the secondary outcomes. This analysis allows for missing values. Missing values will be analysed in order to determine whether they systematically differ between groups or are related to baseline value. In this case multiple imputation methods will be used to calculate parameter estimates as a sensitivity analysis.
Group comparison will be by linear mixed models with the intervention as a fixed effect, the effect of centre on the outcome modelled with a random effect and adjustment for baseline value of VO2peak. A two-sided p-value of less than 0.05 will be considered to be statistically significant. Similar analyses will be performed for effects at 12 months and for the secondary outcomes.
The cumulative incidences of the composite endpoint MACEs and the elements from which it is constituted will be presented by intervention group and plotted in Kaplan-Meier survival curves for one year of follow-up. We will test for differences in hazard rates between the mCR and control group using Cox regression analysis allowing the baseline hazard functions to differ between centres.
Cost-effectiveness analyses
The economic method of evaluation is a cost-benefit analysis. The two main benefits are survival and quality of life. Survival will be measured by the surrogate endpoint VO2peak, a reliable predictor for mortality, and quality of life will be represented by the difference in two composed scores between T2 (the end of follow-up) and T0 (enrolment): Physical Component Summary Score and Mental Component Summary Score.
All costs with regard to the cardiological diagnostic and therapeutic process from the moment of inclusion in the study until the end of follow-up will be included. The cost categories that are examined are all direct costs within and outside the health care system. Direct costs in healthcare comprise GP consultations, admission days, outpatient visits, and diagnostic and therapeutic activities. The direct non-medical costs include travel and time costs of the patient and in relation to visits to the doctor and health care institutions. Medication is not included in the analysis, because all patients receive normal cardiology care. For the assessment of volume all observations registered in the e-CRF will be used. All activities performed during one outpatient visit or admission period are considered to be one patient visit to the hospital. Confounders may have a large impact on the results and uncertainty in measurement. For this reason, a sensitivity analysis will be performed.
Data management
The gathered data are entered into an electronic case record form and managed by a Contract Research Organisation (CRO) (diagram) responsible for the data management, monitoring of participating centres and quality of data; this includes full source data verification for at least the first five included patients per centre and 10% of the other included patients. At the end of the project all data will be integrated in a data warehouse, and made query free and available for statistical analysis.
Discussion
Even as the global incidence and mortality from CHD is declining, the burden of elderly patients suffering from chronic CHD is increasing in Europe. 1 In this light, CR is of particular importance. The quality of life of CVD patients is significantly impaired, especially in the elderly, due to several factors including high risk of recurrence of events, hospital admission, physical disability, co-morbidity and general frailty. With physical limitations, social limitations, and unstable health, many CHD patients become anxious or depressed. These factors render elderly CHD patients, more than half of whom are women, more vulnerable not only in terms of recurrent events but also in terms of maintaining ability to lead an independent life. Yet paradoxically, uptake of CR remains poor, particularly in the elderly. Practical barriers, like distance, insufficient transportation infrastructure, mobility problems and lack of social support are proven to be factors for low participation. With the objective of contributing significantly to a solution, the EU-CaRE consortium hopes that by adding novel components to existing CR there will be increased success.
The current project aims to address these issues by targeting the challenges related to CVD and ageing. EU-CaRE compares existing CR programmes in the elderly as well as an innovative mobile tele-monitoring guided CR focusing on sustainability, (cost-) effectiveness and participation grade. The study will map the current practice and effectiveness of CR and through this identify characteristics of successful CR. This will contribute to the understanding of the predictors for effectiveness of individual CR components, provide the evidence base to redesign and improve CR and allow tailoring of CR delivery towards the elderly.
mCR technology
Smartphone apps are becoming increasingly popular among physicians, patients and general public. The majority of these apps are general health and fitness apps that both facilitate the tracking of health parameters by private users, and provide users with basic health and fitness-related information as well as guidance. There is, however, very little evidence for the effectiveness of mobile health apps and as a consequence very little experience on how to best evaluate these apps: especially when the use of an app is combined with individual coaching as in the EU-CaRE RCT. The mCR technology that will be used in this project, has recently been tested in addition to conventional CR in a pilot study at Isala Zwolle in the Netherlands. The outcomes are being evaluated. Recently, Frederix et al. showed that the addition of cardiac tele-rehabilitation to conventional centre-based CR proved to be more effective and efficient than centre-based CR alone. 16 Cardiac tele-rehabilitation reduced the number of readmissions during the follow up period from 22.9% to 10.1%, an average cost reduction of €564 per patient and an increased quality of life. In the EU-CaRE RCT patients will receive mCR who would otherwise not have received CR at all. Little is known about the effects of mCR in comparison to no CR instead of being added to conventional centre-based CR. mHealth solutions could develop more cost-effective CR, avoid unnecessary hospital visits and develop truly patient-centred CR programmes. The technology could facilitate patient long-term compliance by the capacity to personalise programmes, facilitate communications and monitor patient status, drug adherence and physical activity during long periods. Also, mHealth may overcome barriers related caused by lack of mobility by providing home-based programmes. Small studies have investigated the effectiveness of home-based CR (not based on mHealth technology), with guidance in the residential environment, compared with centre-based CR. These findings have generally been non-inferior and have indicated increased participation rates.8,9 The implementation of the mHealth in a multinational, multicentre trial will overcome the weaknesses of single-centre trials and is a major strength of the study. Use of mCR represents an opportunity to increase participation and adherence in elderly patients.
Strengths and weaknesses
The strengths of the project include the prospective nature, the detailed assessment of patients, the focus not only on the effect of the intervention but also on causes of non-referral and non-adherence. A weakness is that due to the organisation of CR, e.g. referral to different CR centres due to health insurance coverage and lack of registries of CHD patients eligible for CR, the actual number of patients eligible for CR may not be accurately recorded in all centres. Thus the true uptake may be overestimated. Further, for ethical and practical reasons the information gathered on patients not referred to CR or who decline is limited and important predictors of CR uptake may not be registered (e.g. related to socioeconomic factors, co-morbidity or social network). The additional strength of the RCT is the randomised setting and the focus on the compliance and adherence to mCR.
The aim of the RCT was to test an intervention in patients who currently receive no CR and thus includes only patients who have declined regular centre-based CR. This design was chosen to ensure that patients were not deprived of an evidence-based multidisciplinary intervention. However, this also introduces a bias in the study since the results will only be applicable to a sub-group of the patients eligible for CR. A further weakness may be that mCR is focused on exercise training and patients do not achieve the benefit of multidisciplinary programme as provided in the standard CR.
Conclusion
The EU-CaRE project is aimed to provide the evidence base for the development of more effective CR interventions, and for enhanced uptake, adherence and compliance in the elderly population. EU-CaRE RCT in its turn hopes to provide proof that mCR is a valuable alternative for elderly population who opt out of current CR offers.
With this study, we hope to identify barriers in the entire chain of events that leads to successful CR, whether these barriers are structural barriers, relate to referral and the organisation of the CR programme, relate to the implementation of the programmes or to patient characteristics. By comparing the elements implemented in experienced CR enters in different parts of Europe and the effects these have on the success of CR we may learn from each other. We further hope to identify patient groups that may need particular attention in terms of improved referral, adherence and effect of intervention.
Footnotes
Acknowledgements
The authors wish to acknowledge MobiHealth BV (Zwolle, The Netherlands) for the smartphone/application with data subscription and the web-portal used in EU-CaRE RCT.