
Abstract
In patients with stable coronary artery disease, clinical outcomes are predominantly characterized by the consequences of atherosclerosis on the myocardium, but also by complications of atherosclerosis, notably recurrent acute coronary syndrome or stroke. Secondary prevention therapy is therefore key in this patient population. Intensification of secondary prevention therapy is possible, at the price of a therapeutic risk or a high cost, therefore justifying careful selection of patients with a high residual risk and low therapeutic risk. Two lines of therapy can be intensified, independently of each other, namely anti-thrombotics and lipid-lowering agents. Intensification of anti-thrombotic therapy is efficacious in terms of ischaemic events and cardiovascular mortality, but incurs an excess haemorrhagic risk. Patients aged over 65 years of age and those with a history of intra-cranial haemorrhage are not eligible for intensification of anti-thrombotic therapy. Conversely, patients with prior or recurrent myocardial infarction may benefit from this strategy, especially if they are current smokers or have diabetes mellitus. Intensification of lipid-lowering therapy can be achieved through an association of high-intensity statins with ezetimibe or PCSK9 inhibitors. This strategy engenders little risk, but the cost of PCSK9 inhibition is high, and should be considered based on the level of low-density lipoprotein cholesterol achieved with statin treatment at the maximal tolerated dose. In addition to this patient selection based on low-density lipoprotein cholesterol levels, the presence of diabetes or documented progression of atherosclerosis should be considered.
Keywords
Introduction
In patients with stable coronary artery disease, clinical outcomes are predominantly characterized by the consequences of atherosclerosis on the myocardium, namely left ventricular dysfunction, ventricular or atrial arrhythmias and disease progression, but also complications of atherosclerosis, notably recurrent acute coronary syndrome (ACS) or stroke. The PROSPECT study 1 showed that in the three years following an ACS, the risk of cardiovascular events was around 20%; half this risk was attributable to thrombotic complications at the angioplasty site, and the other half to complications of other atheromatous plaques. Before intensifying secondary prevention therapy, reinforcement of all possible lifestyle measures is of paramount importance. After this important first step, intensification of therapy is possible, by reinforcing antiplatelet therapy and by reducing the low-density lipoprotein cholesterol (LDL-C) level. The benefit to be gained from intensifying antithrombotic therapy goes hand in hand with an increase in the risk of bleeding, whereas intensifying lipid-lowering therapy engenders few side effects. However, both strategies can be envisaged, after careful evaluation of the ischaemic and bleeding risks as well as the risk of progression of atherosclerosis.
Residual risk in secondary prevention: individual predictors and scores
Individual factors
After ACS or stroke, the residual risk is time-dependent. The risk is highest during the first 12 months after an acute episode. Beyond one year, the event rate related to atherosclerosis seems to stabilize,2–5 but numerous other factors may enter into play, either individually or in combination, thereby modifying the residual risk,2,4,6,7 such as age,7,8 sex, 9 diabetes,7,10 left ventricular dysfunction and recurrent infarction,2,11 coexisting peripheral artery disease11,12 or stroke. 5 In addition to these clinical factors, other parameters also play a role, such as biological factors (renal failure13,14 or other biological markers15,16), genetic factors, 17 imaging findings such as the extent of vascular disease18–21 and, finally, the quality of secondary prevention therapy.4,7
Risk scores
Due to the large number of factors involved, the interactions between these factors and the relative weight of each in determining a patient’s risk, the use of risk scores is indispensable. Among the many scores developed to assess risk, the majority were designed for the acute phase.22–25 These scores are thus suboptimal for the chronic phase, even though certain scores have been validated up to one
26
and three years.
27
The updated version of the GRACE risk score was developed for a period ranging from discharge after ACS to six months, and showed satisfactory external validation up to three years.
28
Few risk scores have been developed specifically for secondary prevention in stable patients. The ischaemic risk score based on the population from the REACH registry (developed in 33,419 patients and validated in 16,270 patients) can be used for secondary prevention. The variables included in this score are age (in categories), smoking status, diabetes, extent of arterial disease (number of vascular beds affected), heart failure and treatment with statins and aspirin
29
(Figure 1).
Predictors of ischaemic (left panel) and haemorrhagic (right panel) events among patients with stable atherosclerosis. Data from the REACH registry, adapted from Wilson et al.
29
and Ducrocq et al.
60
In blue: predictors of ischaemic events. In red: predictors of haemorrhagic events. In green: predictors of both ischaemic and haemorrhagic events.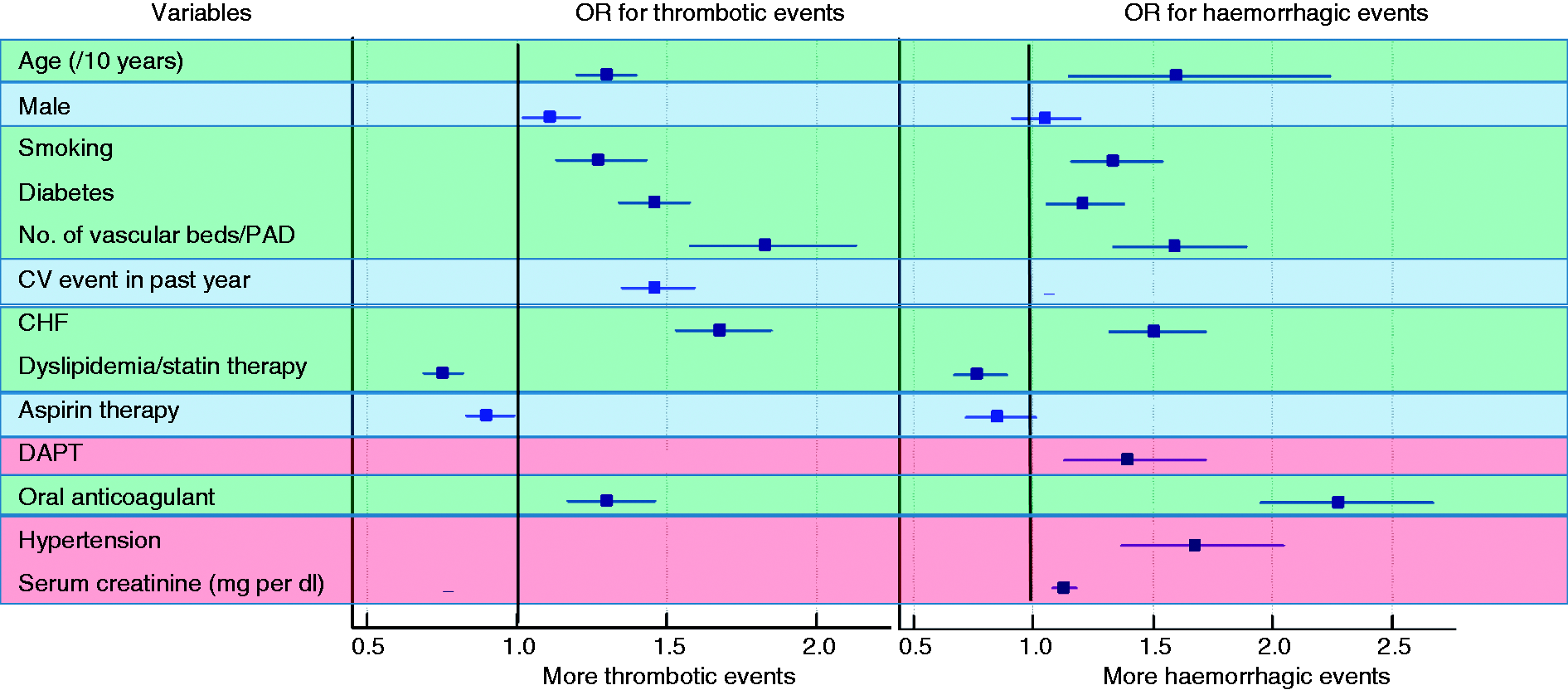
What is ‘aggressive’ secondary prevention treatment?
In the secondary prevention of atherosclerosis, optimal treatment has been well established for several years. In addition to correction of risk factors as well as lifestyle measures, guidelines recommend therapy combining antiplatelets, beta-blockers, angiotensin-converting enzyme inhibitors and statins, known under the acronym ‘BASI’.30–33 This is the cornerstone of treatment designed to suit the vast majority of patients, and there is little room for tailoring this treatment to meet the needs of individual patients. Yet, this standard secondary prevention therapy has evolved in recent years, with certain therapies called into question (notably, beta-blockers 31 ) and the advent of new molecules, in particular antiplatelet and lipid-lowering drugs. The universal ‘BASI’ approach has progressively been replaced by individually tailored treatment, especially for anti-thrombotic therapies34–37 and lipid-lowering therapy,38,39 with the potential to intensify lipid-lowering by using high-intensity statins, 38 by associating statins with other molecules such as ezetimibe 39 or by using PCSK9 inhibitors. 40
Variations in antiplatelet therapy
With the exception of patients who present allergy or intolerance (generally gastro-duodenal), treatment with aspirin is universally established as the cornerstone of secondary prevention therapy. 41 The first 12 months after an ACS constitute a period of high thrombotic risk, especially if revascularization was achieved by angioplasty with stent implantation. Further to the CURE 37 and COMMIT 42 studies, a combination of aspirin plus clopidogrel for one year was widely adopted and recommended by guidelines, except in patients at high risk of bleeding. During this 12-month period, antiplatelet therapy can be intensified by the use of other agents that are more potent than clopidogrel, without modifying the aspirin treatment. Beyond the first 12 months after ACS, it is potentially possible to prolong the dual antiplatelet therapy, with clopidogrel or other agents.
Dual antiplatelet therapy in the first 12 months after ACS
Antithrombotic therapy during the first year after an ACS can be intensified by replacing clopidogrel by either prasugrel 43 or ticagrelor. 34 Both these drugs have been shown to have net clinical benefit, despite an excess of bleeding events. The use of prasugrel is restricted to patients who undergo angioplasty and who have no prior history of stroke. In patients aged over 75 years or weighing less than 60 kg, the excess risk of bleeding as compared with clopidogrel is such that the net clinical benefit of prasugrel is nil. Ticagrelor has wider indications, including patients treated without percutaneous coronary intervention, that is, medically or by surgical revascularization, and there are no age or weight limits. The only patients not eligible for ticagrelor are those with a history of intra-cranial bleeding. A strategy of intensifying the standard antithrombotic combination of aspirin and clopidogrel with the addition of a direct oral anticoagulant (anti Xa) at low dose was tested in the ATLAS-ACS2 TIMI 51 study, with the use of rivaroxaban 2.5 or 5.0 mg twice daily. After an average follow-up of 13 months, rivaroxaban reduced the risk of the composite end point of death from cardiovascular causes, myocardial infarction or stroke, at the price of an increased risk of major bleeding and intracranial haemorrhage. 44 Therefore, secondary prevention therapy can be intensified in the first year after an ACS by replacing clopidogrel either with ticagrelor (except in patients with a history of ischaemic stroke) or with prasugrel (subject to the restrictions cited above). The addition of rivaroxaban at a dose of 2.5 mg twice daily is a potentially useful option that can be considered for patients at low haemorrhagic and high thrombotic risk.
Beyond the first 12 months after ACS or angioplasty, what is aggressive antithrombotic therapy, and which patients should have it?
Beyond the first year after an ACS or angioplasty with stent implantation, single antiplatelet therapy is the rule, generally using low-dose aspirin. 33 In a meta-analysis of 95,000 patients, aspirin was shown to reduce the relative risk of cardiovascular death by 21%. 45 As for the acute phase, antiplatelet therapy can be intensified, not by increasing the dose of aspirin above 100 mg/day, but rather by prolonging the duration of the dual antiplatelet therapy (DAPT), combining aspirin with clopidogrel or another antiplatelet agent.
Four clinical trials have tested the utility of DAPT beyond 12 months, testing associations of aspirin with one of clopidogrel, prasugrel, vorapaxar or ticagrelor.
The CHARISMA study included high-risk patients in primary prevention or (predominantly) secondary prevention, with 9478 of the 15,603 patients having suffered from documented infarction, stroke or peripheral arterial disease before inclusion.
46
Although the results did not find any significant benefit with the association of aspirin and clopidogrel compared with aspirin alone in the overall population, pre-defined subgroup analysis of secondary prevention patients showed a 17% reduction in relative risk of cardiovascular events with DAPT, without an increase in the risk of bleeding.
11
The ‘DAPT’ study confirmed a reduction of thrombotic complications with prolonged DAPT in patients undergoing angioplasty with implantation of an active stent (40% in the context of ACS), and treated for one year with DAPT without bleeding complications. In the intervention arm of the study, patients pursued DAPT for a further 18 months with either clopidogrel (63.5%) or prasugrel (34.7%). After the 18 additional months’ treatment, patients in this group had a reduction in thrombotic events,
47
albeit with an unexplained excess in mortality and a higher rate of bleeding complications. There was a statistically significant interaction (p = 0.03) between prasugrel and clopidogrel, suggesting that prasugrel yielded greater protection against major adverse cardiovascular events than clopidogrel. The use of vorapaxar, an inhibitor of the protease-activated receptor PAR-1, at a dose of 2.5 mg/day, on top of aspirin alone, or aspirin plus clopidogrel, for an average of 30 months, was tested versus placebo in the TRA-2P TIMI 50 study, in patients with a history of recent (<1 year) infarction or stroke.
48
The study was prematurely discontinued due to an excess of bleeding complications (moderate and severe bleeding, including intracranial haemorrhage), but the study nonetheless reported a reduction in cardiovascular mortality. The PEGASUS-TIMI 54 study compared ticagrelor versus placebo, in association with aspirin in patients aged over 50 years with a history of infarction (on average, 1.7 years prior) and presenting at least one additional high-risk feature (i.e. age > 65 years, diabetes, a second prior spontaneous myocardial infarction, multivessel disease or chronic renal dysfunction). After an average follow-up of 33 months, DAPT was associated with a reduction in thrombotic events at the cost of an increase in major bleeding, and there was a trend towards a reduction of cardiovascular mortality with the dose of 60 mg twice daily.
36
Age (above or below 75 years) was not shown to have an effect on the risk of bleeding at either the 60 mg twice daily or the 90 mg twice daily dose. The patients who seemed to yield the most benefit were those in whom the interval between myocardial infarction (MI) and randomization was the shortest.
49
Based primarily on the CHARISMA, DAPT and PEGASUS studies, the ACC-AHA guidelines published in 2016 stipulated that patients with previous MI may benefit from prolonged DAPT. 50
Dissociating the thrombotic risk from the haemorrhagic risk
A meta-analysis combining six randomized trials that evaluated the benefit of prolonged DAPT beyond one year in patients with MI (totalling 33,435 patients) found a relative reduction of 22% in major adverse cardiac events with prolonged DAPT, as well as a 15% reduction in cardiovascular mortality, albeit without a reduction in overall mortality, and at the price of a relative increase of 73% in major bleeding (Figure 2).
51
A Bayesian network meta-analysis including 31,666 patients showed that prolongation of DAPT beyond one year was associated with a 42% higher hazard ratio for bleeding, and an 18% higher hazard ratio for all-cause mortality, driven by a 49% higher hazard ratio for non-cardiac mortality, without any change in cardiovascular mortality, and despite a reduction in MI, stroke and stent thrombosis.
52
The CHARISMA, DAPT, PEGASUS and TRA2P studies suggest that patients with one or more previous MIs are consistently a population at high thrombotic risk who benefit from intensification of the antiplatelet therapy. Conversely, the higher bleeding risk associated with the more aggressive antithrombotic strategy obliges us to exclude patients at high haemorrhagic risk. Thus, although patients with a history of intracranial bleeding can easily be identified and excluded due to the potential risk of recurrence, other predictors of bleeding risk are more difficult to determine.
Meta analysis from six randomized trials comparing short versus prolonged dual antiplatelet therapy (adapted from Udell et al.
51
). Upper panel: odds ratios (and 95% confidence intervals) for major cardiovascular events. Lower panel: odds ratios (and 95% confidence intervals) for individual cardiovascular endpoints.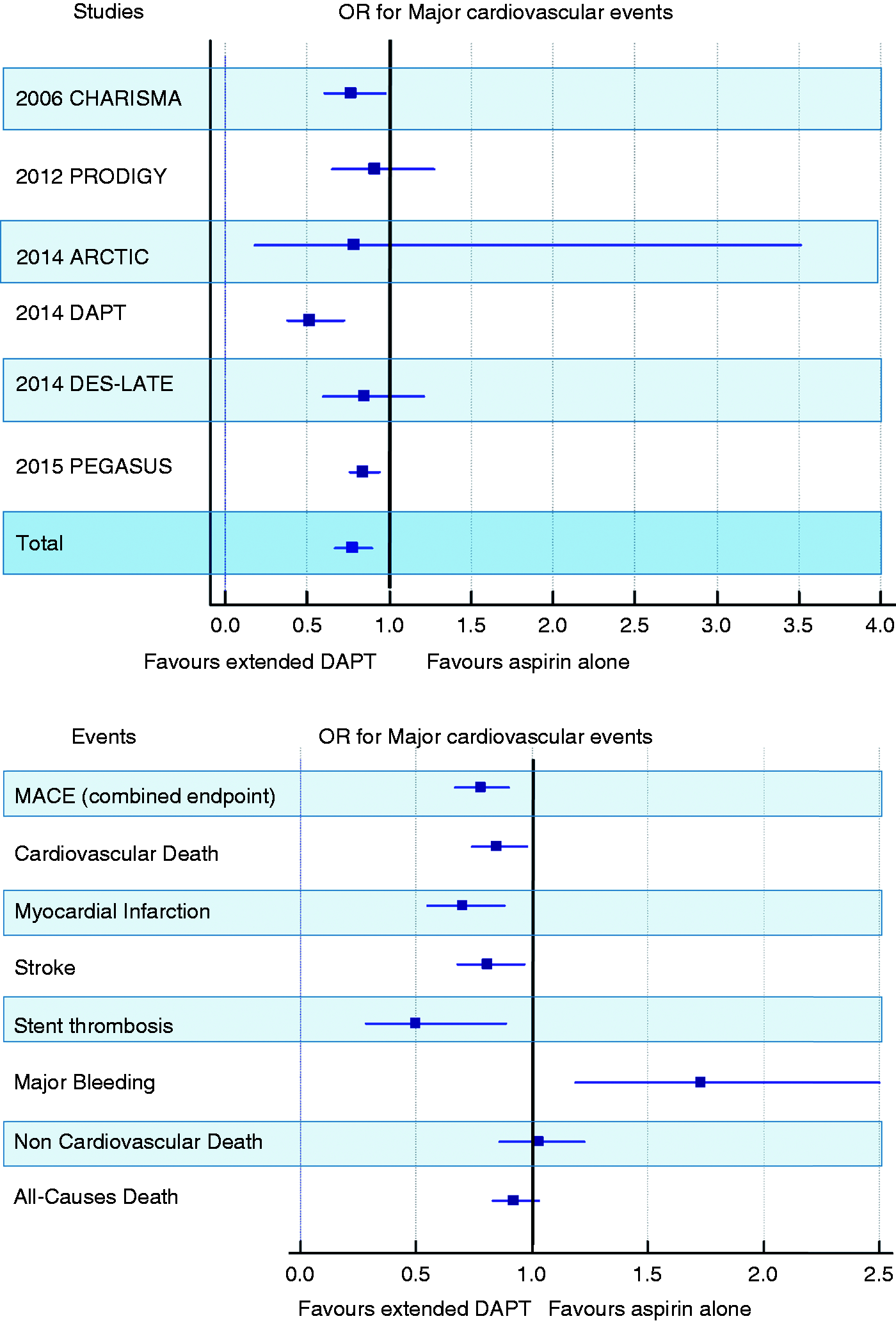
Estimating haemorrhagic risk
As with the estimation of ischaemic risk, several scores have been developed to evaluate the risk of bleeding, and most were designed for use in the acute phase,53–56 in the context of coronary angioplasty57,58 or in patients treated with vitamin K antagonists. 59 The predictors of bleeding retained in these scores include age, low body weight, renal failure, heart failure and anti-thrombotic treatment. One of the few scores developed in a cohort of patients with stable disease is the bleeding score from the REACH cohort, based on 68,106 patients included in the REACH registry and validated in 15,603 patients included in the CHARISMA study. 60 Age, peripheral arterial disease, congestive heart failure, diabetes, hypertension, smoking, antiplatelets, oral anticoagulants and hypercholesterolaemia were the nine items retained for the final score.
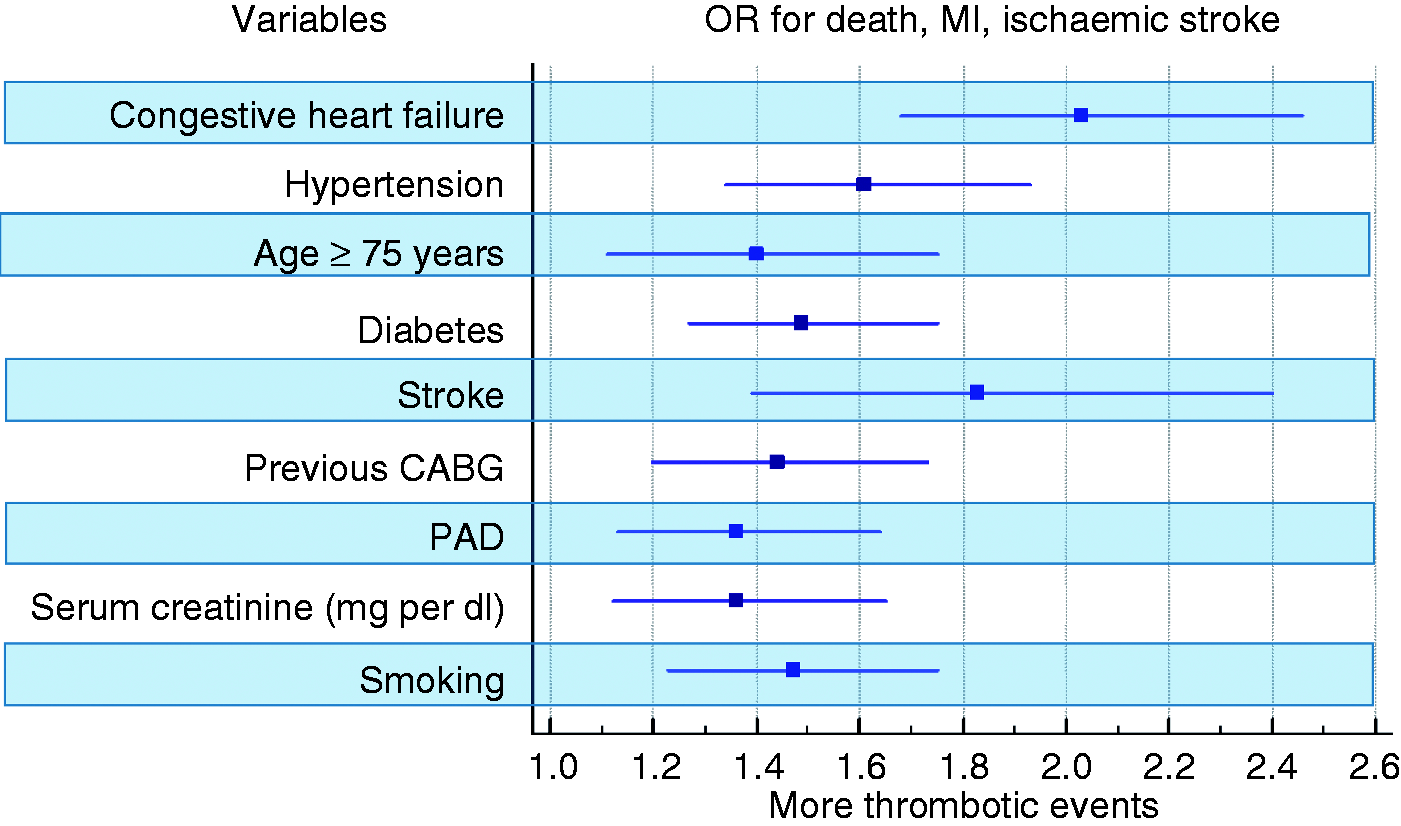
Sub-group analysis of patients with a history of MI in the TRA2P TIMI 50 study, including 17,779 patients, showed that in this population, the addition of vorapaxar reduced the risk of major adverse events by 20% after an average follow-up of 2.4 years (1.6% absolute risk reduction), with an excess of moderate and severe bleeding, including intra-cranial haemorrhage.
61
Analysis of stable patients in the placebo group who had a history of MI but no history of intra-cranial haemorrhage showed that patients at risk of an ischaemic event (death, MI or stroke) were those aged over 75 years and those with a history of peripheral, cerebral and coronary arterial disease, renal failure, diabetes and smoking
62
(Figure 3).
Factors associated with the risk of death, myocardial infarction and stroke by multivariate analysis in the placebo group of the TRA2P TIMI 50 study (adapted from Bohula et al.
62
).
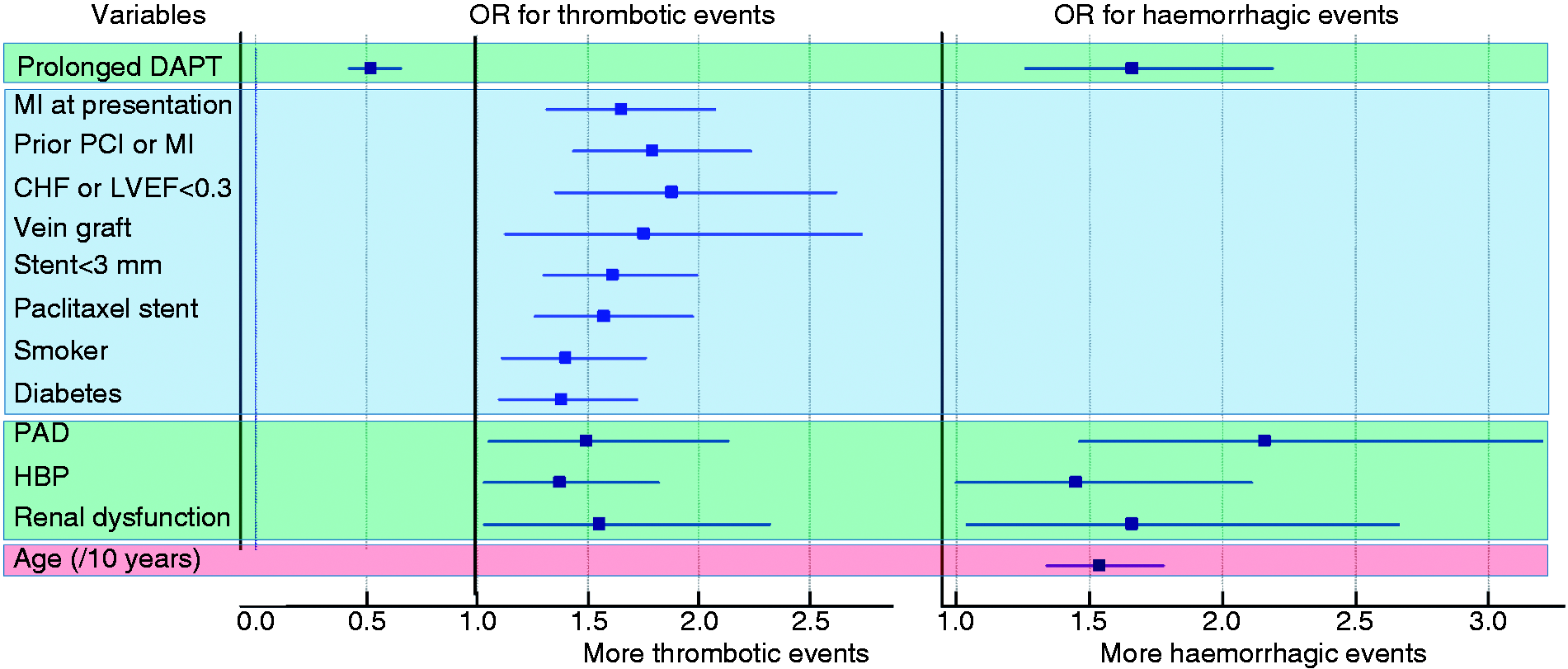
The comparison of the ischaemic and haemorrhagic scores from the REACH registry shows how difficult it is to dissociate these two types of risk. Age, renal failure, smoking status, heart failure and peripheral arterial disease are predictors of both thrombosis and bleeding. Only diabetes, lack of statins, and recent history of vascular events orient the profile towards ischaemic risk, while hypertension, renal dysfunction and prolongation of DAPT increase the bleeding risk (Figure 1). Similarly, the DAPT study enabled the construction of a score combining both thrombotic and haemorrhagic risk, in which only variables with discriminant capacity were retained (Figure 4). The main inclusion criterion in the DAPT study was that patients had to have been treated with antiplatelet therapy for at least one year without any bleeding complications. Age was found to be a predictor of bleeding, whereas a history of prior MI, heart failure, or diabetes, current smoking, implantation of multiple stents, stents of small diameter, taxol-eluting stents or stents placed on a vein graft were predictors of thrombotic events.
63
Although not strictly identical to the REACH score, the DAPT score does confirm certain factors as being of prime importance, and gives important pointers for patient selection (Figure 4).
Predictors of thrombotic (in blue), haemorrhagic (in red) and both thrombotic and haemorrhagic (in green) events in the DAPT population (adapted from Yeh et al.
63
).
What are the conclusions for the reinforcement of antithrombotic therapy?
Intensifying antiplatelet therapy is possible, either by modifying DAPT, or by replacing clopidogrel with a more potent agent (i.e. prasugrel 10 mg/day, or ticagrelor 90 mg twice daily, or rivaroxaban 2.5 mg twice daily). Beyond the first 12 months, intensification of antiplatelet therapy is possible by prolonging the prescription for DAPT, up to 30 months, using either clopidogrel 75 mg/day, or ticagrelor 60 mg twice daily, or rivaroxaban 2.5 mg twice daily.
Even when the prerequisite that the patient had no bleeding complication during the first year is respected, this reinforced DAPT regime reduces ischaemic events, but the increased haemorrhagic risk persists. Therefore, patient selection cannot be on the basis of previous MI alone, 50 but patients at high bleeding risk, such as those aged over 65 or those with prior intracranial bleeding, are not suitable candidates for this strategy and must therefore be excluded. Conversely, patients with a history of one or more prior MIs are potentially suitable candidates, and two additional criteria can also be taken into account, namely ongoing smoking, and diabetes, which in some studies were associated with higher thrombotic risk than bleeding risk.
Possible variations in lipid lowering therapy
Standard treatment, and achieving the target LDL-C value
Randomized and observational studies have successively shown that for secondary prevention, treatment with statins is beneficial, 64 regardless of the initial LDL-C value. 65 Furthermore, it has been shown that high-intensity statin therapy is preferable to low 38 or moderate intensity. 66 In both primary and secondary prevention, for every reduction of 1 mmol/l (38 mg/dl) in LDL-C, there is a 20% reduction in cardiovascular events per year, 67 justifying the recommendation for systematic treatment with high-intensity statins. 32 A target value of LDL-C <70 mg/dl (or a 50% decrease if the baseline LDL-C level is between 70 and 135 mg/dl) is recommended in the guidelines of the European Society of Cardiology in order to facilitate efficacy and compliance with treatment. Although the threshold of 70 mg/dl is not strongly supported by scientific evidence, it corresponds to the values found in studies that compared different intensities of statin treatment, and it is critical in clinical practice to have a fixed threshold to recommend in order to achieve better compliance. 68 The IMPROVE IT study tested two hypotheses, namely the benefit of adding ezetimibe to statin treatment after ACS over a prolonged duration; but also the idea of lowering LDL-C below the 70 mg/dl value. 69 In terms of LDL-C values, the IMPROVE IT study compared patients with an average LDL-C of 69 mg/dl versus those with an average value of 54 mg/dl, and showed that this additional reduction of 20% in LDL-C resulted in a 6% reduction in events over six years 39 (even reaching a reduction of 9%, if cumulative events are taken into account 70 ). The results of the FOURIER and SPIRE-2 trials confirm that treatment with a PCSK9 inhibitor yields a 50% to 60% reduction in LDL-C, and this reduction is associated with a corresponding decrease in major adverse cardiovascular events.40,71 The SPIRE trials were stopped early after the sponsor elected to discontinue the development of bococizumab owing in part to the development of high rates of antidrug antibodies observed in biological studies. The magnitude of reduction in clinical events per decrease of 1 mmol/l of LDL-C seems to be similar with PCSK9 inhibitors as with statins or ezetimibe. Importantly, the benefit of LDL-C reduction is observed for LDL-C levels far below 70 mg/dl, since patients in whom the LDL-C level on treatment was below 25 mg/dl had the greatest reduction in events. 40
In parallel to clinical criteria, the impact of the reduction in LDL-C has also been demonstrated in terms of progression or regression of the volume of atherosclerotic coronary plaque in studies using intravascular ultrasound. The REVERSAL 72 and GLAGOV studies, 73 as well as a meta-analysis, 74 have shown that the development of plaque volume within 12 to 24 months has a linear relation with the level of LDL-C achieved. An LDL-C value above 70 to 100 mg/dl is associated with plaque progression, whereas plaque regression of around 1% over 12 months is likely with LDL-C values between 36 and 70 mg/dl.72,73
In summary, the level of LDL-C achieved under treatment therefore identifies patients at risk and a greater reduction in LDL-C yields a greater reduction in events, without any clear lower threshold.
Patients with high residual risk, linked to LDL-C
Registry studies have shown in secondary prevention that the therapeutic target is achieved in only 28% of patients.
75
Three primary causes have been cited for this failure to achieve target LDL-C values: (1) insufficient efficacy of statins because of very high LDL-C levels, and this is particularly true in patients suffering from familial hypercholesterolaemia,
76
and also in poor responders to statin therapy;
77
(2) patients who are intolerant to statins, particularly because of muscle symptoms, and in whom treatment intensity has to be reduced, or even requiring treatment discontinuation;
78
and (3) patient non-compliance with treatment,
79
for which the predictive factors are well established. History-taking and LDL-C measurement generally make it possible to distinguish between these three causes, and each situation requires a specific management strategy:
For patients with elevated LDL-C values, and for those showing poor response to statin therapy, the addition of ezetimibe or a PCSK9 inhibitor should be considered.80–82 In the IMPROVE IT study, diabetic patients and those with prior coronary artery bypass graft
83
yielded a particular benefit from reduction of the LDL-C value below 70 mg/dl with ezetimibe. The mechanism of action of this improved efficacy in diabetics is related to their higher risk profile and a more favourable biological response.
82
If the LDL-C is still not at the desired target, despite a combination of highest tolerated statin dose plus ezetimibe, then PCSK9 inhibitors should be considered. Muscle intolerance should be verified by ensuring that symptoms improve when statin therapy is discontinued (even temporarily). In this case, statins can be re-introduced at a lower intensity and/or lower dose.
78
Patients at risk of intolerance are those who are initiating statin therapy for the first time, those with a personal or family history of muscle symptoms, elevation of muscle creatine kinase and those treated by simvastatin or atorvastatin. Conversely, well tolerated statin therapy for the previous three months or prescription of fluvastatin are factors that render muscle intolerance unlikely.
84
Premature discontinuation of secondary prevention treatments is frequent, and is not limited to statins only, but concerns all secondary prevention drugs.
79
Unwarranted discontinuation, often at the patient’s own initiative, of antiplatelet drugs
85
or statins is responsible for an excess of mortality and recurrent MI.86,87 Factors influencing non-compliance are mainly economic reasons, but also include younger age, male sex, lower socio-economic status, current smoking, and low body weight.
88
What are the conclusions for the reinforcement of lipid lowering therapy?
In the context of secondary prevention, all patients should have high-intensity statins, regardless of their baseline LDL-C level.32,78 Lipid-lowering therapy can be intensified by increasing the statin intensity where possible, or by adding ezetimibe or a PCSK9 inhibitor. A decision-making algorithm for optimizing lipid-lowering therapy in the context of secondary prevention after MI has recently been published, and considers that all patients after MI are at high risk as long as treatment has not reached the maximum tolerated dose, and it also allows for the possibility of adding ezetimibe if the LDL-C value remains above the target of 70 mg/dl. 89
LDL-C criteria for considering the use of a PCSK9 inhibitor, on top of maximally tolerated statins and ezetimibe treatment (adapted from Sabatine 93 ).
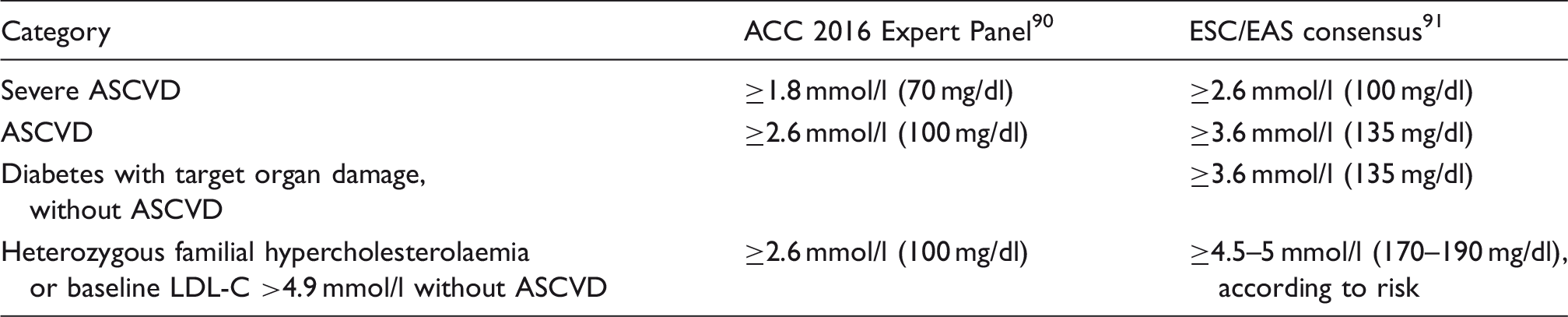
LDL-C: low-density lipoprotein cholesterol; ACC: American College of Cardiology: ESC/EAS: European Society of Cardiology/European Atherosclerosis Society; ASCVD: atherosclerotic cardiovascular disease
This treatment escalation does not appear to expose the patient to a risk of major adverse events, other than the risk of intolerance (mainly muscle symptoms), which is reversible and occurs at a frequency of around 10%. 84 To a lesser extent, there is a risk of development of diabetes, which is higher in pre-diabetic patients, and a low risk of intra-cranial haemorrhage. 67 Last but not least, there is no signal for cognitive decline with statins, ezetimibe and PCSK9 inhibitors, even at very low LDL-C levels, as shown by the results of the Ebbinghaus study. 92 However, it should be noted that in this study, the duration of exposure to PCSK9 inhibitors was quite limited.
Conclusion: what aggressive secondary prevention, and for whom?
Intensification of secondary prevention therapy is possible, at the price of a therapeutic risk or a high cost, therefore justifying careful selection of patients with a high residual risk and low therapeutic risk. Two lines of therapy can be intensified, independently of each other, namely antithrombotics and lipid-lowering agents. Intensification of antithrombotic therapy is efficacious in terms of ischaemic events and cardiovascular mortality, but incurs an excess haemorrhagic risk. Patients aged over 65 years of age, and those with a history of intra-cranial haemorrhage are not eligible for intensification of antithrombotic therapy. Conversely, patients with prior MI or recurrent MI may benefit from this strategy, especially if they are current smokers or have diabetes mellitus. Intensification of lipid-lowering therapy can be achieved through an association of high-intensity statins with ezetimibe or PCSK9 inhibitors. This strategy engenders little or no actual risk, but a high cost with PCSK9 inhibition, and therefore, its use should be considered based on the level of LDL-C achieved with statin treatment at the maximal tolerated dose. In addition to this patient selection based on LDL-C levels, the presence of diabetes or documented progression of atherosclerosis under treatment also identifies suitable candidates for treatment intensification.
Footnotes
Author contribution
FS and RC contributed to the conception of the work. All authors contributed to the acquisition, analysis and interpretation of literature data for the work. FS and FE drafted the manuscript. RC critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.