
Abstract
Background
Plasma total homocysteine (tHcy) has been implicated in the development of cardiovascular disease, but the mechanisms remain unclear. Vitamin A (Vit-A) is involved in homocysteine metabolism and we therefore explored the potential interaction between plasma tHcy and serum Vit-A in relation to incident acute myocardial infarction.
Methods
Cox proportional hazards models were used to assess the prospective relationships between tHcy and acute myocardial infarction in 2205 patients from Western Norway undergoing elective coronary angiography for suspected stable angina pectoris. Results are reported as hazard ratio per standard deviation increase in log-transformed tHcy. An interaction term for tHcy × Vit-A was added to multivariate models including age, sex, smoking, apolipoprotein B fasting, statin and aspirin prescription and estimated glomerular filtration rate.
Results
Geometric mean (geometric standard deviation) age of the participants (64.3% men) was 62.3 (1.24) years. Plasma tHcy was higher among participants in the upper versus lower Vit-A tertile. During 7 (2.4) years of follow-up, 15.1% suffered an AMI. A significant association of plasma tHcy with AMI in the total study population was observed. When we stratified the population according to Vit-A tertiles, plasma tHcy was associated with acute myocardial infarction only in the upper Vit-A tertile (hazard ratio per SD: 1.25, 95% confidence interval: 1.04–1.53, pinteraction = 0.03).
Conclusions
The risk relationship between plasma tHcy and acute myocardial infarction was modified by serum concentrations of Vit-A in patients with suspected stable angina pectoris. This finding may clarify the relationship between tHcy and cardiovascular disease.
Introduction
The non-protein, sulphur-containing amino acid homocysteine is produced by intracellular transmethylation reactions where a methyl group is transferred from the universal methyl donor S-adenosylmethionine (SAM) to a methyl acceptor. 1 This reaction produces S-adenosylhomocysteine (SAH), which is readily hydrolysed to adenosine and homocysteine in a reversible reaction. In the circulation, homocysteine undergoes disulphide exchange reactions, forming symmetrical and mixed disulphides, which are collectively referred to as total homocysteine (tHcy). 2 Elevated plasma concentrations of tHcy have been linked to increased risk of cardiovascular disease (CVD) in observational studies, 3 findings that were recently suggested to depend on oxidative stress and inflammation. 4 However, tHcy-lowering treatment with B-vitamins did not improve prognosis in secondary prevention trials, and the potential underlying pathological mechanisms for the risk relationship of tHcy with CVD remain unclear. 5
Vitamin A (Vit-A) designates a class of fat-soluble compounds abundant in Western diets. 6 In target cells, retinol is a precursor for the major bioactive retinoid, retinoic acid (RA), which is a ligand for nuclear RA receptors. The role of Vit-A in CVD development is unclear, 7 but we have shown that serum Vit-A modified the risk association between lipid parameters and acute myocardial infarction in the same core population as the current study. 8 Moreover, expression of genes involved in synthesis of all-trans-RA is increased in some inflammatory conditions 9 and is promoted by mediators of oxidative stress and inflammation such as oxysterols. 10 This potentially increased synthesis of all-trans-RA may have metabolic ramifications for homocysteine. Circulating tHcy has been positively associated with Vit-A in an observational study, 11 and all-trans-RA is a potent activator of glycine N-methyltransferase (GNMT),12–14 which produces SAH and homocysteine under conditions of excess intracellular SAM. 15 GNMT is involved not only in the regulation of intracellular homocysteine concentrations, 16 but also in lipid metabolism 17 and cellular immune activation. 18
Taken together, the association of plasma tHcy with risk of CVD may be modified by Vit-A through several biological mechanisms. However, evidence is limited, predominantly experimental and little is known about this relationship in humans. The aim of this observational study among more than 2000 patients with suspected stable angina pectoris was to explore whether the relationship of plasma tHcy with risk of AMI was modified by serum concentrations of Vit-A.
Subjects and methods
A total of 4164 patients undergoing elective coronary angiography for suspected stable angina pectoris at Haukeland (n = 3413) and Stavanger (n = 751) University Hospitals, Norway, in the period 2000–2004 were enrolled in this study. In total, 61.8% (n = 2573) participated in the Western Norway B-Vitamin Intervention Trial (WENBIT) (clinicaltrials.gov: NCT00354081) and received either: 1) folic acid, vitamin B12 and vitamin B6, 2) folic acid and vitamin B12, 3) vitamin B6 or 4) placebo. 19 Subjects with missing data on plasma tHcy or serum Vit-A and those who received B-vitamin treatment (n = 1959) in the WENBIT were excluded, yielding a total of 2205 subjects available for the present study. Written informed consent was obtained from all participants and the study protocol was in accordance with the principles of the Declaration of Helsinki, and approved by the Regional Committee for Medical and Health Research Ethics, the Norwegian Medicines Agency, and the Norwegian Data Inspectorate.
Baseline data and biochemical analyses
CVD history and prescription of medications at baseline were self-reported and verified by hospital records. 19 Patients with diabetes were classified by previous diagnosis (type 1 or 2), having fasting or non-fasting serum glucose ≥ 7.0 or ≥ 11.1 mmol/L, respectively, or having baseline glycated haemoglobin > 6.5%. Definitions of smoking and severity of coronary artery disease as well as the calculation of glomerular filtration rate (eGFR) have been described previously. 20
Blood samples, mostly non-fasting (80%), were collected at baseline. Plasma and serum samples were stored at –80℃ until analysis. Plasma concentrations of tHcy were analysed using gas chromatography mass spectrometry, 21 whereas serum Vit-A (as all-trans retinol) 22 and neopterin 23 by liquid chromatography tandem mass spectrometry by BEVITAL AS (www.bevital.no). Serum concentrations of apolipoprotein B and C-reactive protein (CRP), and dietary Vit-A intake were measured as described previously.8,20
Follow-up and clinical endpoints
The participants were followed from baseline to the date of acute myocardial infarction (AMI) diagnosis or death, or to 31 December 2009 (the end of follow-up), whichever came first. AMI cases were ascertained via record linkage to national hospital discharge diagnoses obtained from the Cardiovascular Disease in Norway project (www.cvdnor.no) to 31 December 2009.24–26 The primary outcome was hospitalization or death attributed to AMI (coded I21, I22, I46.1, R96, and R98 according to the International Statistical Classification of Diseases 10th version). If more than one AMI event occurred in a participant during the follow-up period, only the first event was considered. An 11-digit personal identifier, unique to each Norwegian resident, was used to link baseline variables with study endpoints.
Statistical analysis
Due to non-normality, continuous variables are presented as geometric mean (gM) (geometric standard deviation (gSD)). Categorical variables are given as percentages (%). Baseline characteristics are presented for the total population and according to serum Vit-A tertiles. Trends across Vit-A tertiles were assessed with unadjusted ordinary least squares or logistic regression. Skewed variables were log-transformed before analyses. Survival analyses were carried out using Cox regression and reported as hazard ratios (95% confidence intervals (CIs)) per 1 SD log-transformed plasma tHcy in one model containing log-transformed tHcy (continuous), age (continuous) and sex (binary), and an additional model including additional adjustment for smoking (binary), statin prescription (binary), aspirin prescription (binary), fasting status (binary), eGFR (continuous) and apolipoprotein B (continuous). To assess the effect-modification by Vit-A, Vit-A (continuous), log-transformed tHcy (continuous) and their interaction term (Vit-A × tHcy) were added to the models. To assess the interaction in the presence of competing risks, we computed subdistribution hazard ratios from identical models based on the approach proposed by Fine and Gray. 27 To explore whether the results differed in patients with and without significant coronary stenosis, we evaluated the Vit-A × tHcy interaction in patients with 1–3 stenotic epicardial vessels as well as patients with no significant stenosis in models adjusted for age and sex. The assumption of proportionality was evaluated visually by log–log plots and quantitatively by calculating Schoenfeld residuals. To assess any non-linear relationships between tHcy and risk of AMI according to Vit-A tertiles, we constructed generalized additive model (GAM) dose–response curves based on the age- and sex-adjusted models in each Vit-A tertile. To visualize the interaction of log-transformed tHcy with Vit-A, we constructed an interaction plot. In brief, we plotted the hazard ratio of log-transformed tHcy against a given range of Vit-A (0–7 µmol/L), and thus illustrated how the association of log-transformed tHcy with AMI changes with increasing concentrations of Vit-A. We considered p-values < 0.05 significant. The statistical basis and R-codes for this procedure have been published. 28 Statistical analyses were carried out using the ‘base’, ‘survival’ and ‘cmprsk’ packages, whereas the GAM plot was created using the ‘mgcv’ package for R 3.0.2 (the R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Baseline characteristics for the total study population (N = 2205) with suspected stable angina pectoris.
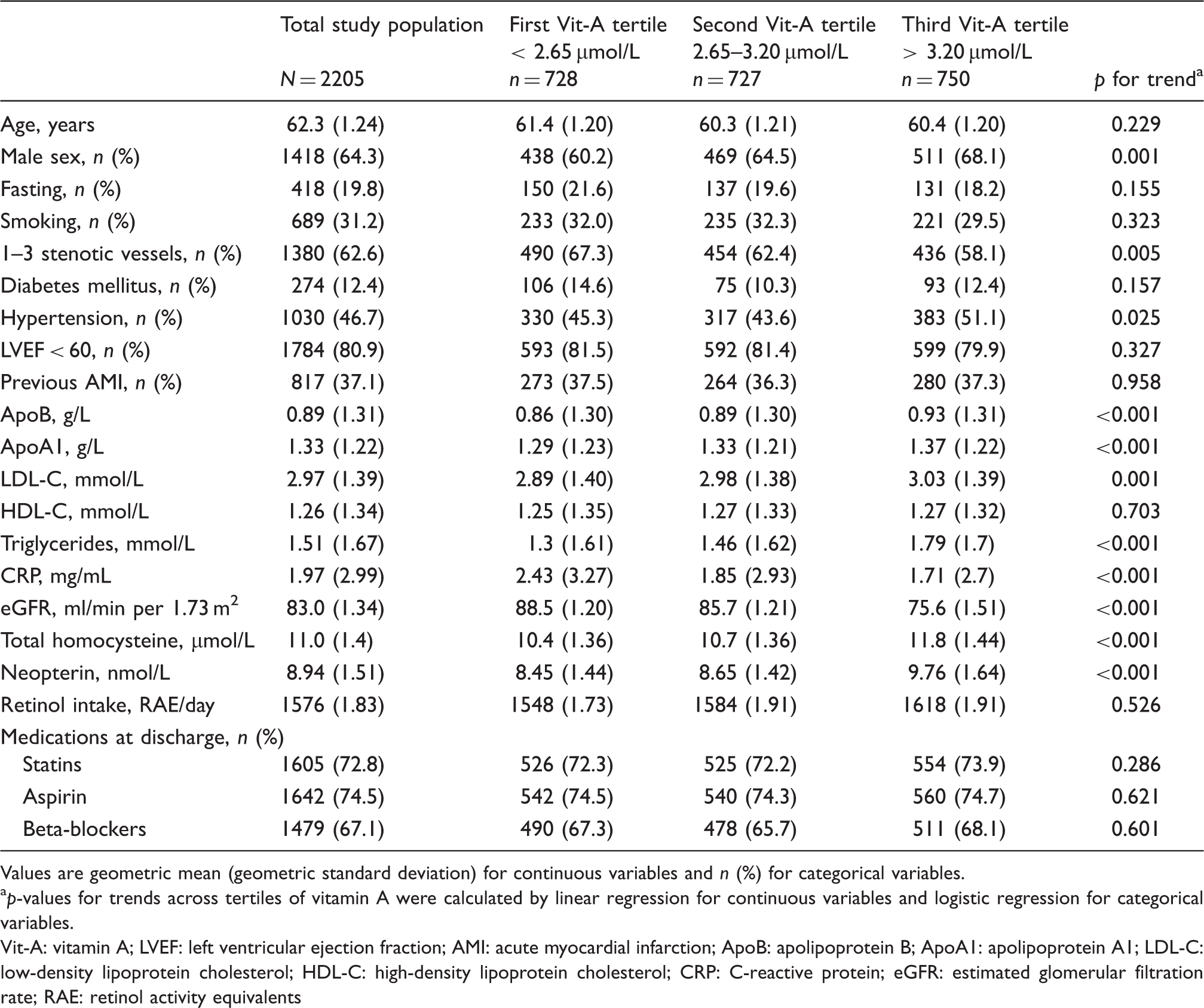
Values are geometric mean (geometric standard deviation) for continuous variables and n (%) for categorical variables.
p-values for trends across tertiles of vitamin A were calculated by linear regression for continuous variables and logistic regression for categorical variables.
Vit-A: vitamin A; LVEF: left ventricular ejection fraction; AMI: acute myocardial infarction; ApoB: apolipoprotein B; ApoA1: apolipoprotein A1; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; RAE: retinol activity equivalents
Association between plasma tHcy and AMI
tHcy-related risk of acute myocardial infarction in the total population. a
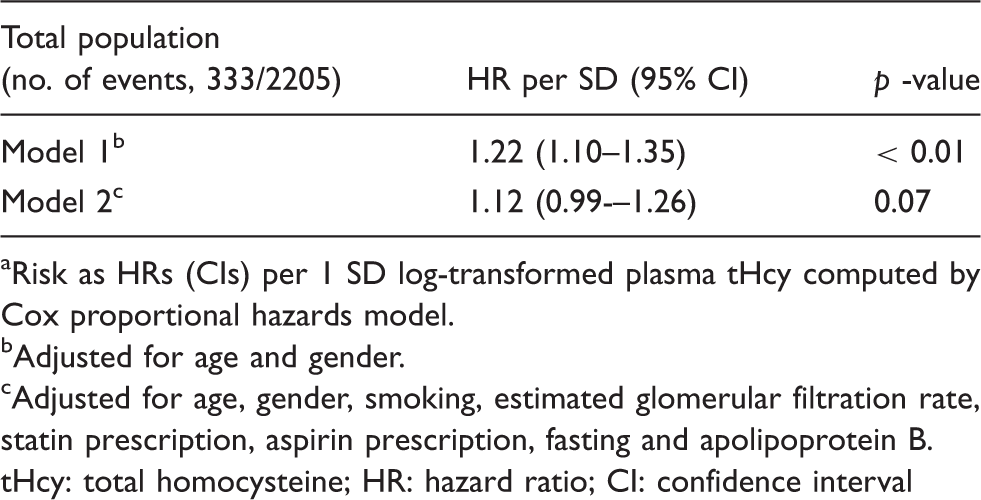
Risk as HRs (CIs) per 1 SD log-transformed plasma tHcy computed by Cox proportional hazards model.
Adjusted for age and gender.
Adjusted for age, gender, smoking, estimated glomerular filtration rate, statin prescription, aspirin prescription, fasting and apolipoprotein B.
tHcy: total homocysteine; HR: hazard ratio; CI: confidence interval
Interaction with Vit-A
Total homocysteine-related risk of acute myocardial infarction across tertiles of vitamin A. a
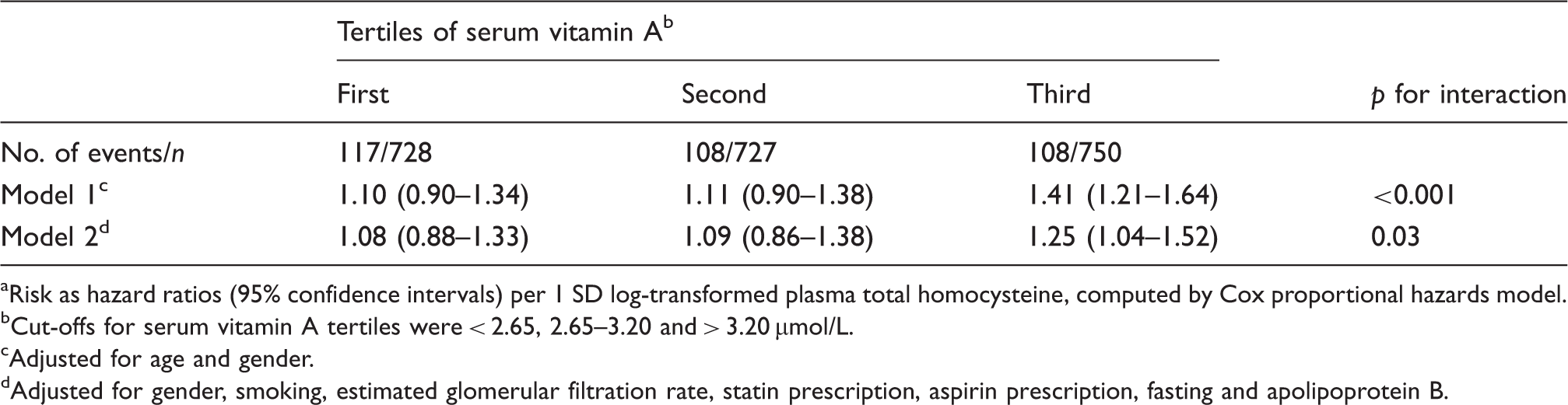
Risk as hazard ratios (95% confidence intervals) per 1 SD log-transformed plasma total homocysteine, computed by Cox proportional hazards model.
Cut-offs for serum vitamin A tertiles were < 2.65, 2.65–3.20 and > 3.20 µmol/L.
Adjusted for age and gender.
Adjusted for gender, smoking, estimated glomerular filtration rate, statin prescription, aspirin prescription, fasting and apolipoprotein B.
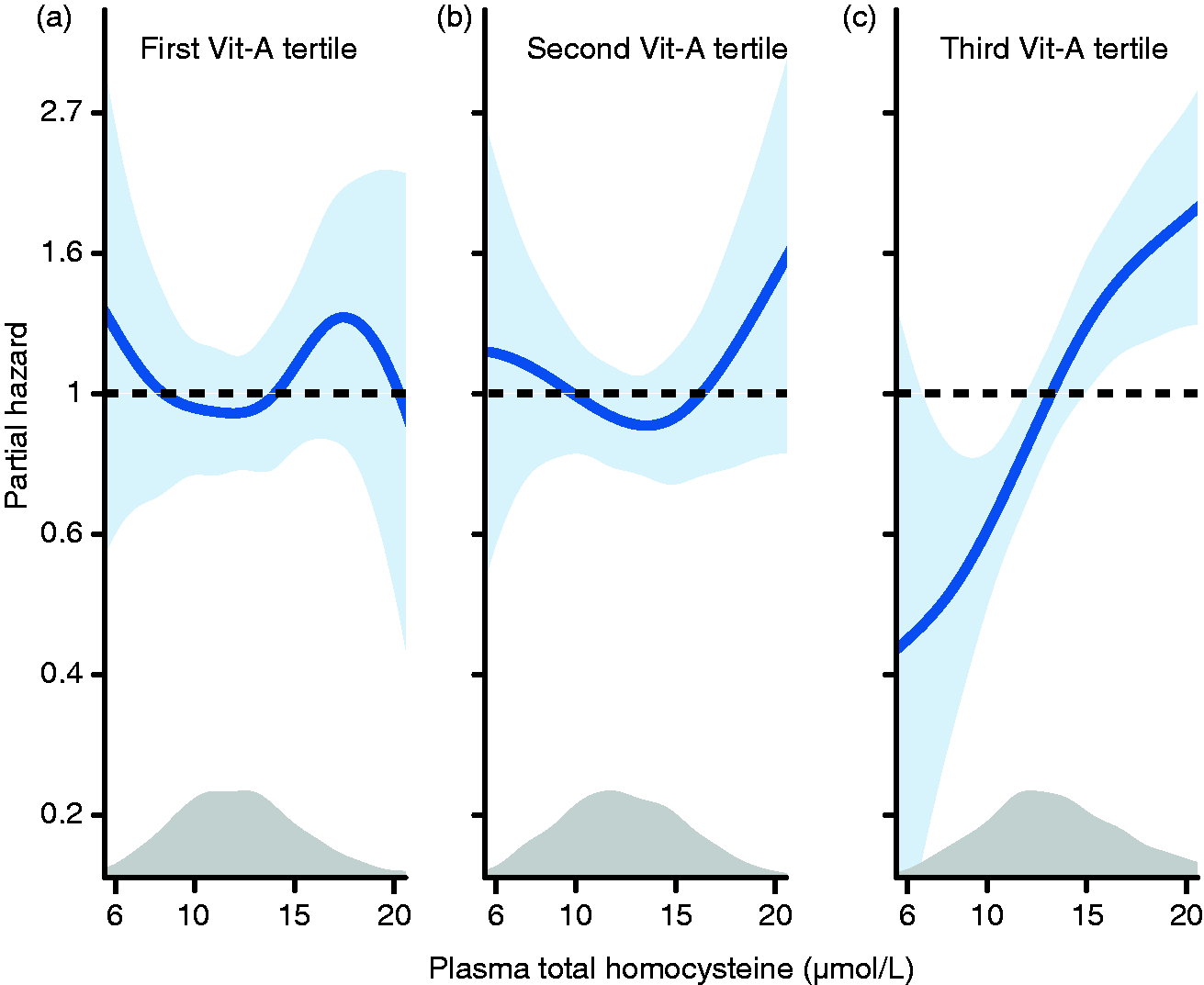
The dose–response relationship between log-transformed total homocysteine and acute myocardial infarctions in the first (a), second (b) and third (c) tertile of vitamin A computed by generalized additive models. Data are adjusted for age and sex. The blue shaded areas around the curve represent the 95% confidence intervals. Kernel distribution plots show the distribution of total homocysteine.

Illustration of the interaction between serum vitamin A and log-transformed total homocysteine on the continuous scale. The blue shaded areas around the curve represent the 95% confidence intervals.
Competing risks analysis
In total, 505 patients died, of which 274 (54.3 %) due to non-coronary causes. Based on this finding, we calculated subdistribution hazard ratios for having an AMI in the presence of non-cardiovascular mortality. The association of tHcy with AMI was generally unchanged in all multivariate models including the upper tertile of Vit-A (subdistribution hazard ratio: 1.24, 95% CI: 1.04–1.49, p for interaction = 0.03).
Interaction with Vit-A in patients with and without significant coronary stenosis
Total homocysteine-related risk of acute myocardial infarction across tertiles of vitamin A in patients with and without significant coronary stenosis at baseline angiography. a
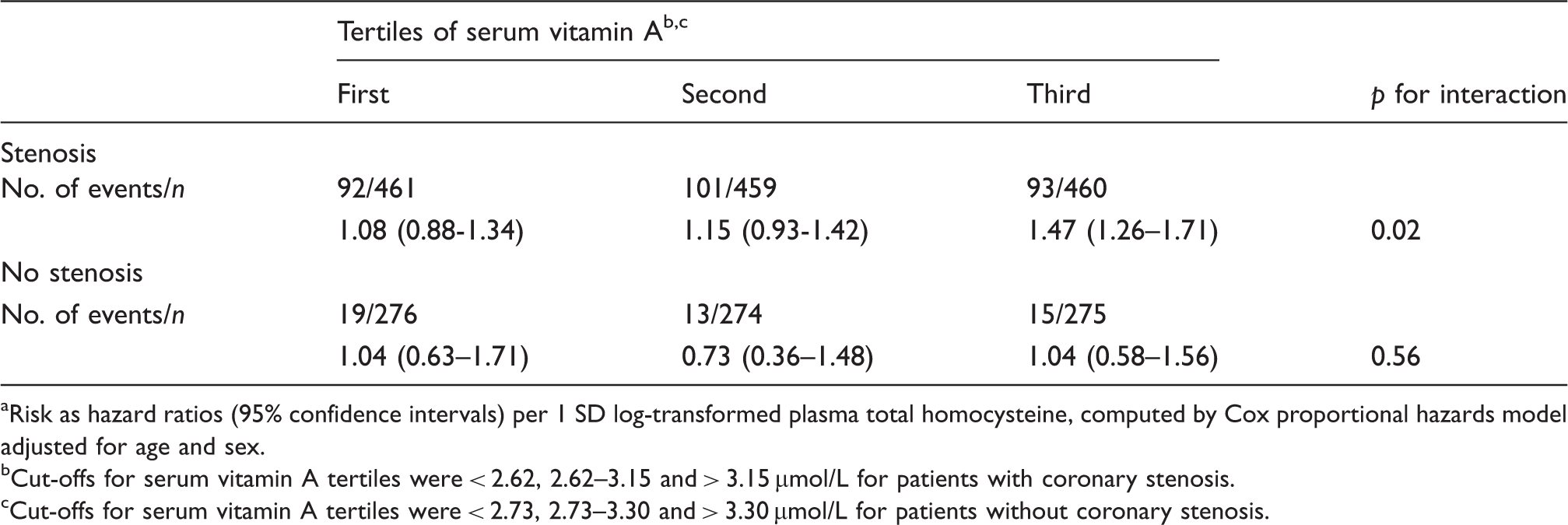
Risk as hazard ratios (95% confidence intervals) per 1 SD log-transformed plasma total homocysteine, computed by Cox proportional hazards model adjusted for age and sex.
Cut-offs for serum vitamin A tertiles were < 2.62, 2.62–3.15 and > 3.15 µmol/L for patients with coronary stenosis.
Cut-offs for serum vitamin A tertiles were < 2.73, 2.73–3.30 and > 3.30 µmol/L for patients without coronary stenosis.
Discussion
Principal findings
In this prospective study among more than 2000 patients with stable angina pectoris, we showed that plasma tHcy was higher in patients with elevated systemic Vit-A concentrations and that the association between tHcy and risk of AMI was primarily confined to patients in the highest tertile of serum Vit-A.
Homocysteine and Vit-A
Our findings are of interest considering our previously published results indicating effect modification by serum Vit-A on the association between traditional lipid parameters and incident CVD. 8 We also demonstrated a positive association between baseline plasma tHcy and serum Vit-A, which is in line with findings among overweight but otherwise healthy individuals. 11 Positive associations for Vit-A, 29 its transport protein retinol-binding protein 430 and cardiovascular endpoints has been reported from some prospective cohorts, but no interaction with other common risk factors have been reported. To our knowledge, epidemiological evidence on the interaction between tHcy and Vit-A with respect to incident AMI or CVD in general has not been assessed previously as far as we know.
Potential mechanisms
Experimental data on the interaction between homocysteine and Vit-A are limited, but possible mechanisms may include inflammation and lipid metabolism. Inflammatory conditions such as non-alcoholic fatty liver disease increase hepatic expression of genes involved in all-trans-RA synthesis. 9 Inflammatory markers such as oxysterols stimulate synthesis of all-trans-RA in the liver, 10 which in turn may affect homocysteine through induction of GNMT.13,15,31 Notably, GNMT plays a role in the production of interferon-γ, which drives synthesis of the macrophage-specific inflammatory marker neopterin.18,32 This pteridine has been related to risk of major cardiovascular events in humans 32 and potentiated tHcy-mediated risk of CVD in the same core population as the present study. 4 Neopterin was higher among patients with elevated Vit-A in the present study, and the tHcy-associated risk we observed in our study may reflect pro-inflammatory conditions that contribute to atherosclerosis. In contrast, CRP, which, unlike neopterin, is produced in the liver as part of the acute phase response 33 and is associated with aspects of CVD risk 34 and complications, 35 tended to be lower among patients with elevated Vit-A. Hence, the interaction between Vit-A and tHcy and the potential link with inflammation seems to relate to specific components of immune activation. This hypothesis needs further exploration in future studies.
Accumulation of cholesterol is crucial for atherosclerotic plaque progression and leads to foam cell formation from endothelial-derived smooth muscle like cells, 36 and may relate to impaired reverse cholesterol transport to high-density lipoprotein (HDL). 37 We recently showed that low concentrations of apolipoprotein A1 (apoA1), the major protein constituent of HDL, was associated with excess risk of cardiovascular events in patients with elevated Vit-A concentrations. 8 Homocysteine, partially produced by GNMT in the liver, accelerates hepatic clearance of HDL 38 and inhibits synthesis of apoA1 in the liver of mice and men with coronary heart disease. 39 Thus, homocysteine may exert detrimental effects on reverse cholesterol transport from atherosclerotic plaques and the dynamic exchange of cholesterol between HDL and low-density lipoprotein particles in the circulation by limiting HDL availability. However, this proposed mechanism is complicated by the demonstration that GNMT ablation in macrophages impaired reverse cholesterol transport, 37 indicating that the outlined mechanism involving Vit-A and GNMT may be tissue-dependent.
Taken together, we speculate that elevated Vit-A activity modifies the tHcy-associated risk of CVD. Notably, tHcy-associated risk among these patients may reflect immune activation and disrupted lipid metabolism. However, well-defined mechanistic studies are needed to explore this potential biological interaction in greater detail, and possibly with regard to different tissues.
Relevance
Recent dietary intake of Vit-A is not likely to affect the observed relationship as it does not affect serum Vit-A concentrations except in individuals with extreme excess or deficient intake. 40 Thus, the high circulating Vit-A levels may reflect metabolic disturbances, as has been shown in animal models. 41 Adjustment for important confounders such as kidney function, which is a determinant of both serum Vit-A 42 and plasma tHcy, 43 did not attenuate the interaction significantly. Although the interaction between tHcy and Vit-A appeared to be independent of other known risk factors, it is essential to replicate the findings in other studies.
In an attempt to explore whether the interaction differed according to the prevalence of coronary artery disease we stratified our patients based on the presence of significant coronary stenosis. We observed a significant interaction between tHcy and Vit-A in patients with 1–3 stenotic epicardial vessels, but not in patients without significant stenosis. These observations indicate that the interaction was confined to patients with more severe disease; however, the statistical power to detect the interaction in patients without coronary stenosis was weak (47 AMI events). These subgroup observations are exploratory but highlight the necessity of investigating this interaction in large and initially healthy cohorts.
Strengths and limitations
This study included a large and well-characterized population with established CVD. Given the high levels of circulating Vit-A compared with other populations,29,44 this cohort may have been particularly suitable for the current study objective. In contrast, the results reported in this study may not be generalizable to the general population because the patients were at increased CVD risk upon recruitment.
The majority of samples were drawn from non-fasting subjects, and tHcy has been found to be modestly increased following food intake,45–47 but adjustment for fasting state in the multivariate models did not alter the risk estimates significantly. The findings and proposed mechanisms are further complicated by the possibility that Vit-A concentrations do not necessarily reflect biological activity in tissues. Finally, as this study is of an observational nature, it does not allow for causal inference due to the possibility of residual confounding such as long-term use of high-dose supplements.40,48
Conclusions
The results from the present exploratory study suggest that the association of circulating concentrations of tHcy with incident AMI is confined to patients with elevated serum concentrations of Vit-A. These findings may shed light on the hitherto unclear relationship between tHcy and CVD. We speculate that tHcy-associated risk may reflect disturbed lipid metabolism and thus experimental and mechanistic studies are needed to elucidate this interaction in a biological system.
Footnotes
Author contribution
OKN conceived and designed the study; OKN, GFTS, ERP and PMU conducted the research; TO and KJV conducted the statistical analyses; ØM and PMU were responsible for measuring vitamin A in serum and tHcy in plasma; TO, KJV, GFTS, ERP, GST, RB, ID, PMU, HR and OKN interpreted the results; TO, KJV, GFTS, ERP, GST, RB, ID, PMU, ØM, HR and OKN wrote, critically revised and approved the final version of the manuscript.
Acknowledgements
The authors thank Tomislav Dimoski at the Norwegian Institute of Public Health for his contribution by developing the software necessary for obtaining data from Norwegian hospitals, and conducting the data collection and quality assurance of data in this project. We would also like to thank all study participants and study personnel for their invaluable contributions to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Advanced Research Program and Research Council of Norway; the Department of Heart Disease at Haukeland University Hospital; the Norwegian Foundation for Health and Rehabilitation; the Norwegian Heart and Lung Patient Organization; the Norwegian Ministry of Health and Care Services; the Western Norway Regional Health Authority; and the Institute of Medical Biosciences, University of Oslo.