
Abstract
Aims
Few data are available on cardiovascular risk stratification in primary care patients treated for arterial hypertension. This study aimed at evaluating the cardiovascular risk profile of hypertensive patients included into the Swiss Hypertension Cohort Study according to the 2013 European Society of Hypertension/European Society of Cardiology Guidelines.
Methods
The Swiss Hypertension Cohort Study is a prospective, observational study conducted by the Centre for Primary Health Care of the University of Basel from 2006 to 2013. Patients with a diagnosis of arterial hypertension (office blood pressure measurement ≥140/90 mmHg) were enrolled. Office blood pressure measurement, cardiovascular risk factors, subclinical organ damage, diabetes mellitus, and established cardiovascular and renal disease were recorded at baseline and at an annual interval during routine consultations by general practitioners in Switzerland.
Results
In total, 1003 patients were eligible for analysis (55.6% male, mean age: 64.0 ± 13.2 years). At baseline, 78.5% of patients presented with either more than three additional cardiovascular risk factors, diabetes mellitus or subclinical organ damage, while 44.4% of patients had a high or very high overall cardiovascular risk. Cardiovascular risk factors and information about diabetes mellitus, established cardiovascular disease and renal disease were recorded mostly completely, whereas substantial gaps were revealed regarding the assessment of subclinical organ damage.
Conclusion
The present findings demonstrate that the majority of primary care patients with arterial hypertension bear a substantial number of additional cardiovascular risk factors, subclinical and/or established organ damage. This emphasizes the need for continuous cardiovascular risk stratification and adequate treatment of arterial hypertension in Switzerland.
Keywords
Introduction
Arterial hypertension is associated with increased morbidity and mortality.1–3 The Global Burden of Disease Study 2010 identified high blood pressure (BP) as the leading cardiovascular risk factor worldwide, followed by tobacco smoking, alcohol and drug use, diets low in fruits and high in sodium, high body mass index (BMI), high fasting plasma glucose, physical inactivity and high total cholesterol. 4 In Switzerland, 34.9% of the adult population had high BP in 2016. 5 Both systolic and diastolic BP correlate with the risk of stroke and coronary heart disease.2,6 Moreover, arterial hypertension plays a key role in the pathogenesis of heart failure, peripheral artery disease (PAD) and chronic kidney disease (CKD).7–10 According to the World Health Organization, cardiovascular diseases account for approximately 17 million deaths per year, representing one-third of global mortality. 11 Moreover, in 2011 an estimated 80% of health care costs in Switzerland (SFr64.6bn) were related to non-communicable diseases with a total of SFr10.3bn linked to cardiovascular diseases. 12
Besides the level of BP, the number of additional cardiovascular risk factors and the long-standing presence of diabetes mellitus, subclinical and established organ damage favour the development of cardiovascular diseases. The individual patient risk depends on the type and number of risk factors as well as on the extent of pathologic changes. 13 Careful risk stratification helps in understanding patients’ risk profile and guiding targeted treatment decisions. To date, few data are available on cardiovascular risk assessment in primary care patients treated for arterial hypertension. Two previous studies identified a high percentage (43% and 60%) of hypertensive patients in primary care as having a high or very high cardiovascular risk and emphasized the importance of global comprehensive cardiovascular risk stratification.14,15
Therefore, the aim of the present study was to evaluate the cardiovascular risk profile of hypertensive patients included into the Swiss Hypertension Cohort Study (HccH). Furthermore, the compliance of general practitioners (GPs) with the 2013 European Society of Hypertension/European Society of Cardiology (ESH/ESC) Guidelines, which were applicable when performing HccH, on cardiovascular risk stratification was assessed in order to identify potential gaps in the risk stratification process.
Methods
Study design and procedures
HccH is a prospective, observational study conducted from 2006 to 2013 by the Centre for Primary Health Care of the University of Basel, Switzerland. Eighty-seven GPs from 12 cantons of Switzerland (see Figure 1) enrolled a total number of 1003 patients and recorded data via an internet-based database. Data collection was done at baseline and annually thereafter during routine consultations. The study protocol was approved by the local ethics committee (Ethikkommission beider Basel (EKBB), ID: 52/05) and written informed consent was obtained from all patients prior to study entry.
Map of the cantons of Switzerland. Cantons participating in the Swiss Hypertension Cohort Study are marked in grey.
Study patients
Adult men and women (age ≥18 years) with an established diagnosis of arterial hypertension were eligible for enrolment into HccH. Inclusion criteria were antihypertensive treatment and/or mean through-sitting office BP measurement (OBPM) ≥140/90 mmHg. Diagnosis relied on the judgment of the treating physician, and treatment could be pharmacological and/or non-pharmacological (lifestyle modifications).
BP measurement
OBPM was based on the values measured at baseline. For every patient, a minimum of two BP readings were obtained in sitting position after at least 5 min of rest using calibrated aneroid or mercury sphygmomanometers or validated automatic devices, depending on availability. For risk stratification, BP was graded according to the 2013 ESH/ESC Guidelines. 13
Assessment of clinical data
GPs were requested to record demographic characteristics (age, sex, smoking history, weight, height and waist circumference) for each patient. Obesity was defined as BMI ≥30 kg/m2, while abdominal obesity was defined as waist circumference ≥102 cm in men and ≥88 cm in women. Furthermore, information on lifestyle modifications, antihypertensive drug therapy and concomitant treatments were documented. A laboratory screening for lipid and plasma glucose levels was conducted. Dyslipidaemia was defined as total cholesterol >4.9 mmol/L (190 mg/dL), or low density lipoprotein > 3.0 mmol/L (115 mg/dL), or high density lipoprotein < 1.0 in men (40 mg/dL) and <1.2 mmol/L in women (46 mg/dL), or triglycerides >1.7 mmol/L (150 mg/dL). Diabetes mellitus was considered if fasting plasma glucose levels were ≥7.0 mmol/L (126 mg/dL) on two repeated measurements, HbA1c was >7% (53 mmol/mol), or post-load plasma glucose values were >11.0 mmol/L (198 mg/dL). Mild CKD (defined as glomerular filtration rate (GFR) of 30–60 ml/min per 1.73 m2), microalbuminuria (albumin–creatinine ratio ≥2.26 mg/mmol or urinary protein dipstick test ≥2++), as well as signs of left ventricular hypertrophy (LVH) in electrocardiogram (ECG) (Sokolow–Lyon Index (SV1 + RV5/V6 ≥ 3.5 mV) or Cornell Voltage Product (RaVL + SV3 + 6 (in women)) × QRS-duration >244 mV*ms) and/or echocardiography (left ventricular mass index >115 g/m2 in men, >95 g/m2 in women) were considered as subclinical organ damage.13,16 Assessment of established cardiovascular and renal disease included coronary heart disease, stroke and transient ischaemic attack (TIA), myocardial infarction, congestive heart failure, PAD, and severe CKD with a GFR <30 ml/min per 1.73m 2 . 13
Cardiovascular risk stratification
Cardiovascular risk stratification was performed according to the 2013 ESH/ESC Guidelines taking into account all available individual patient data. Risk was categorized as low, moderate, high, or very high, corresponding to a 10-year risk for cardiovascular morbidity and mortality of <15%, 15–20%, 20–30%, or >30%, respectively.17,18
Data collection and management
The database used in HccH was developed by the Centre for Primary Health Care in cooperation with GPs and hosted by IBM SPSS Switzerland. Data entry was done by GPs participating in HccH via a password protected website (www.spss.serv.ch/IHAM/CaseManager). Anonymized data collection was ensured by using individual patient codes known by only the treating GP. Complete patient datasets were transferred via a secured channel to the study centre.
Statistics
Statistical analysis was performed using SPSS Version 22 (IBM SPSS Statistics). Discrete variables were expressed as number and percentage, continuous variables as mean and standard deviation (SD). Normal distribution of data was evaluated with the Shapiro–Wilk test, Q–Q Plot, histogram, skew and kurtosis. Mean comparisons between sexes and age groups were performed using Student’s t test or one-way analysis of variance, respectively Mann–Whitney U test or Kruskal–Wallis test, where applicable. Categorical variables were compared using the chi-squared test. Results were considered as statistically significant when a p-value of less than 5% was attained.
Results
Patient characteristics
Baseline characteristics of 1003 patients enrolled into the Swiss Hypertension Cohort Study.
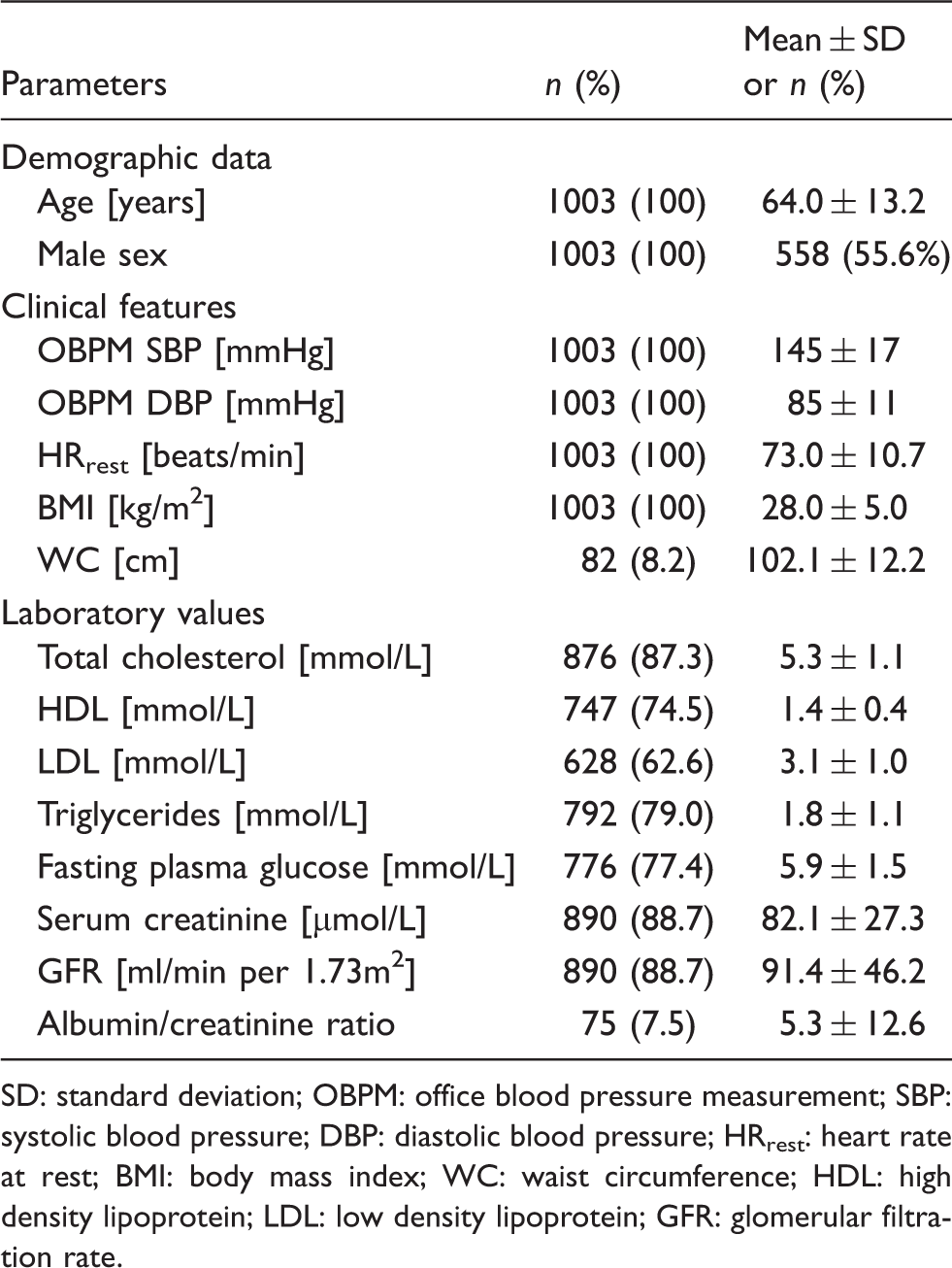
SD: standard deviation; OBPM: office blood pressure measurement; SBP: systolic blood pressure; DBP: diastolic blood pressure; HRrest: heart rate at rest; BMI: body mass index; WC: waist circumference; HDL: high density lipoprotein; LDL: low density lipoprotein; GFR: glomerular filtration rate.
BP categories
Hypertension grades based on office blood pressure measurement according to 2013 European Society of Hypertension/European Society of Cardiology Guidelines for the management of arterial hypertension (n = 1003).
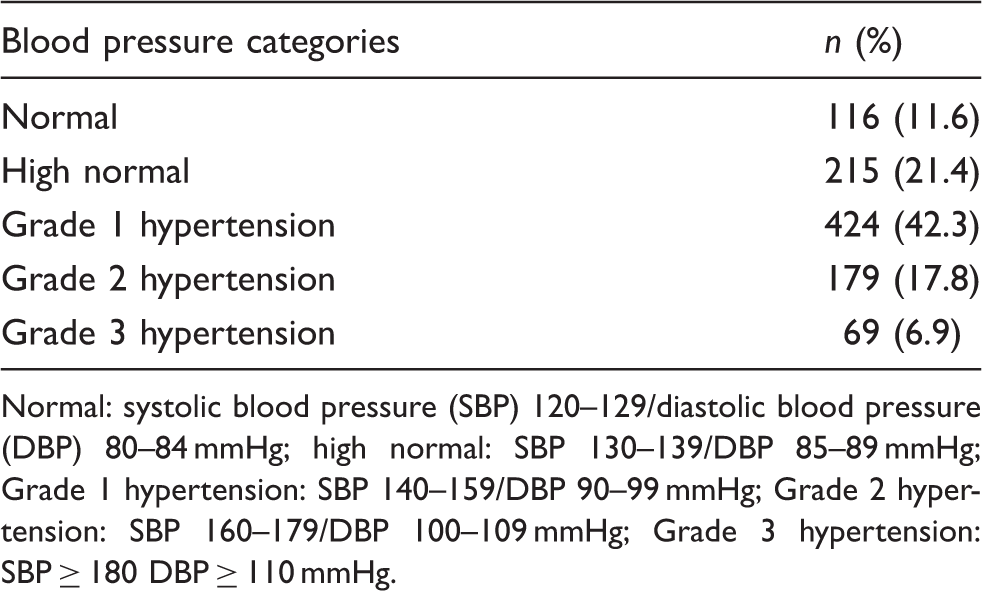
Normal: systolic blood pressure (SBP) 120–129/diastolic blood pressure (DBP) 80–84 mmHg; high normal: SBP 130–139/DBP 85–89 mmHg; Grade 1 hypertension: SBP 140–159/DBP 90–99 mmHg; Grade 2 hypertension: SBP 160–179/DBP 100–109 mmHg; Grade 3 hypertension: SBP ≥ 180 DBP ≥ 110 mmHg.
Cardiovascular risk stratification
Prevalence of CV risk factors, DM, and subclinical and established OD (n = 1003).
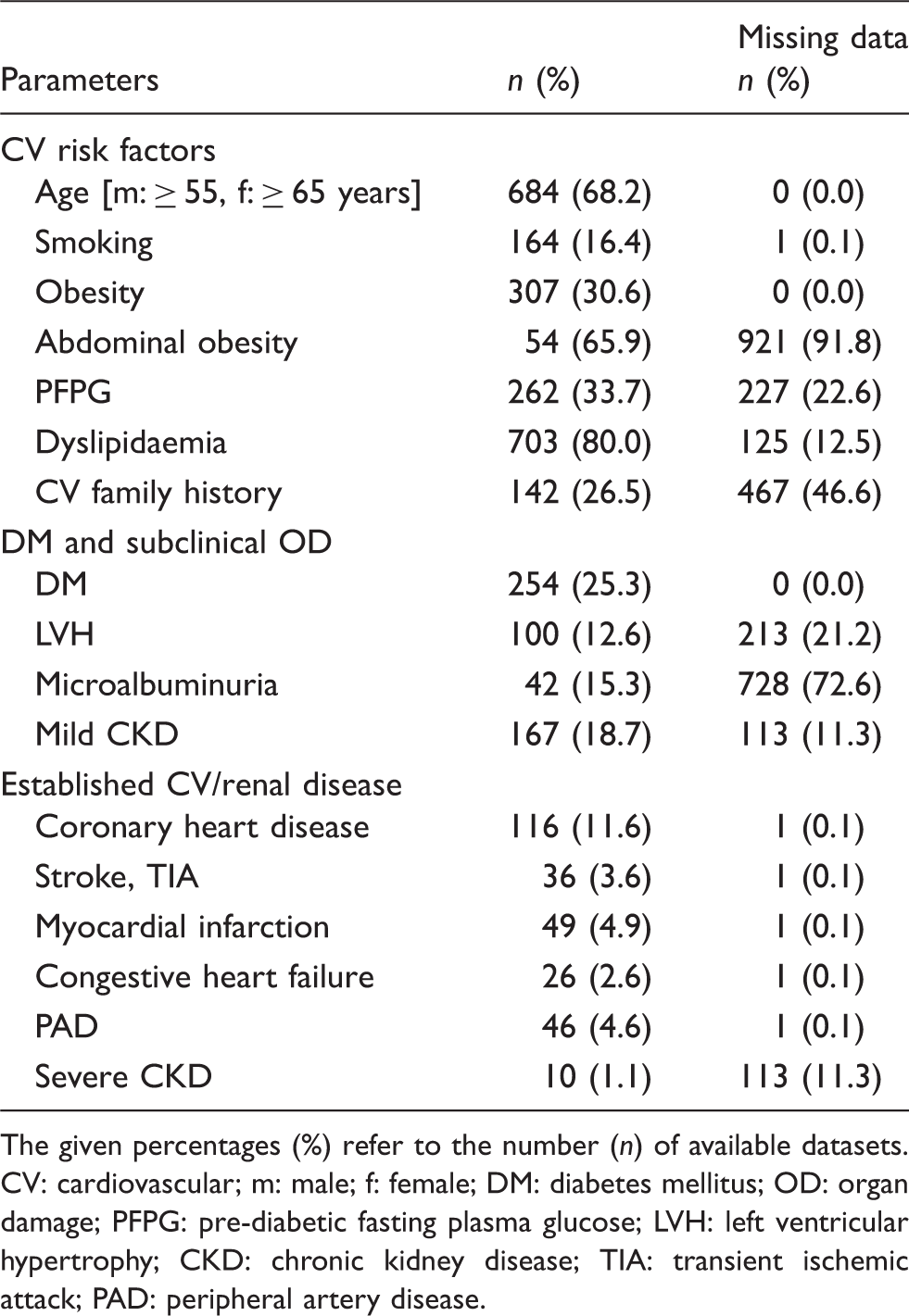
The given percentages (%) refer to the number (n) of available datasets.
CV: cardiovascular; m: male; f: female; DM: diabetes mellitus; OD: organ damage; PFPG: pre-diabetic fasting plasma glucose; LVH: left ventricular hypertrophy; CKD: chronic kidney disease; TIA: transient ischemic attack; PAD: peripheral artery disease.
Mean OBPM was significantly different in male patients, with 144/86 mmHg compared with female patients with 147/85 mmHg (p < 0.001). Evaluation of cardiovascular risk factors showed that men were significantly older and more often smokers (p < 0.001). Prevalence of obesity, dyslipidaemia, pre-diabetic fasting plasma glucose, diabetes mellitus and positive cardiovascular family history were comparable in both sexes. Regarding signs for subclinical organ damage, microalbuminuria was more frequent in male patients (p < 0.05), whereas the prevalence of mild CKD was significantly higher in females (p < 0.001). Coronary heart disease (p < 0.01) and myocardial infarction (p < 0.05) were significantly more common in male patients. Stroke, TIA, congestive heart failure and PAD did not differ between sexes, whereas severe CKD was more frequent in females (p < 0.05).
CV risk data by age category (n = 1003).
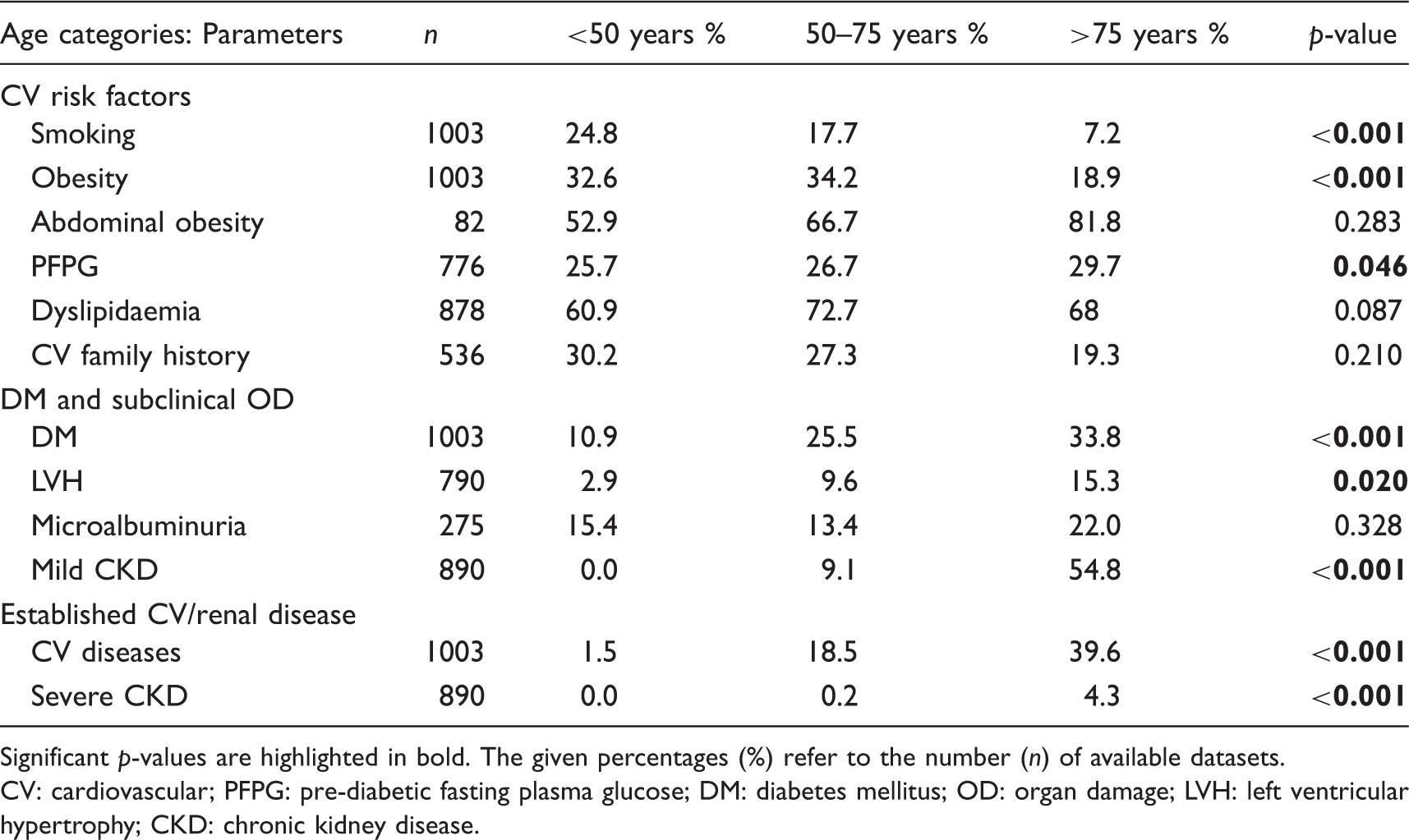
Significant p-values are highlighted in bold. The given percentages (%) refer to the number (n) of available datasets.
CV: cardiovascular; PFPG: pre-diabetic fasting plasma glucose; DM: diabetes mellitus; OD: organ damage; LVH: left ventricular hypertrophy; CKD: chronic kidney disease.
Cardiovascular risk profile
Only 1.7% of patients did not have any cardiovascular risk factors besides arterial hypertension, while 19.7% had one or two additional risk factors, and 27.3% had three or more risk factors (see Figure 2). In 29.9% of patients, subclinical organ damage, diabetes mellitus or mild CKD (stage 3) was found, and 21.3% had an established cardiovascular and/or renal disease. Taken together, 78.5% of patients included into HccH either had three or more CV risk factors, diabetes mellitus, and subclinical or established organ damage. Based on the 2013 ESH/ESC Guidelines taking into account BP grades at the time of enrolment, 11.1% of patients were at low or low-to-moderate cardiovascular risk, 9.4% at moderate risk, 23.5% at moderate-to-high risk, 27.7% at high or high-to-very-high risk and 16.7% at very high risk, indicating a high cardiovascular risk in the majority of patients (Table 5). High-to-very-high-risk patients were significantly older (p < 0.001) with a higher prevalence of obesity and pre-diabetic fasting plasma glucose (both p < 0.05) compared with patients at low-to-moderate cardiovascular risk.
This figure depicts the percentage of additional cardiovascular risk factors as categorized by the 2013 European Society of Hypertension/European Society of Cardiology Guidelines.
13
Assignment of CV risk category to 10-year risk for CV morbidity and mortality.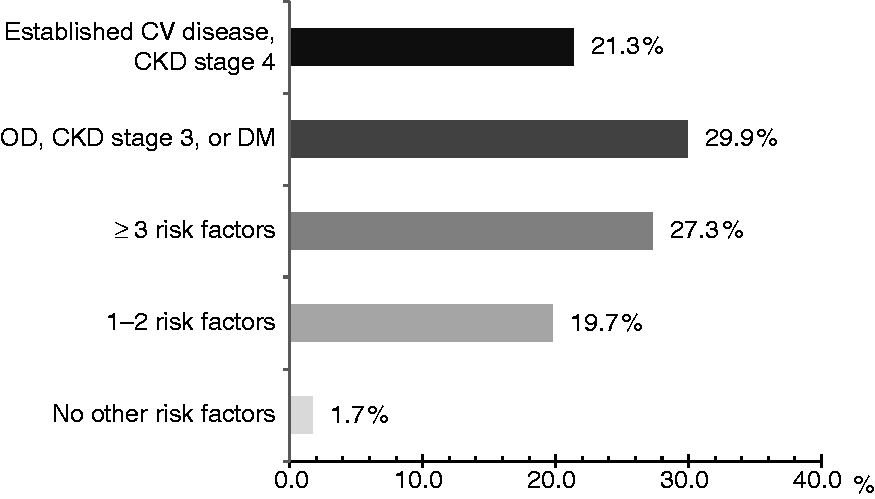

Discussion
The findings of this study investigating patients with arterial hypertension in Swiss primary care indicated that BP control (<140/90 mmHg) at the time of enrolment was low (33.0%) and that 44.4% of hypertensive patients had a high or very high overall cardiovascular risk, corresponding to a 10-year risk for cardiovascular morbidity and mortality of more than 20%. A high proportion of patients (78.5%) presented with either more than three cardiovascular risk factors, diabetes mellitus, subclinical or established organ damage. Information on sex, age, smoking status, BMI, diabetes mellitus and established cardiovascular diseases were collected mostly completely (all ≤ 0.1% missing data), whereas data collection was incomplete with regard to waist circumference (abdominal obesity), microalbuminuria and cardiovascular family history, which were recorded in only 8.2%, 27.4% and 53.4% of patients, respectively.
Cardiovascular risk profile
The low rate of controlled BP in this cohort emphasizes the need for comprehensive cardiovascular risk stratification and adequate treatment of arterial hypertension. Our results are largely comparable with those of the PRESCAP 2006 study performed in primary care centres in Spain, showing that approximately half of the patients treated for hypertension had a high (33.5%) or very high cardiovascular risk (18.4%). 19 The high prevalence of cardiovascular risk factors in our study is comparable with the findings of Barrios et al., who also demonstrated that age and dyslipidaemia were the most common cardiovascular risk factors in hypertensive patients in a primary care setting. 20 A population-based study has recently shown that obesity (50%), hypertension (47%) and hypercholesterolaemia (33%) are the leading cardiovascular risk factors in Switzerland, while smoking (13%) and diabetes mellitus (1.6%) were less prevalent than in our cohort. 21 Prevalence of established organ damage was consistent with other studies, showing that coronary heart disease was the most reported organ damage.19,20,22 Frequency of LVH as a sign of subclinical organ damage in hypertensive patients varies in the literature from 7.5% to 22.1%.22–24 In the present study, a prevalence of 12.6% for LVH was detected when taking into account either ECG or echocardiography. In this study, microalbuminuria was present in 15.3% of patients, which was comparable with other studies.23,25 Testing for microalbuminuria is not yet routinely performed in clinical practice, 26 although it is an established marker for subclinical organ damage according to the 2013 ESH/ESC Guidelines. 13 Dieterle et al. showed that urinalysis for detection of microalbuminuria affects therapeutic decisions, mainly in patients at low or moderate cardiovascular risk, where immediate drug treatment is indicated. 26 The inclusion of data on microalbuminuria increased the percentage of patients with high cardiovascular risk from 59.4% to 66.0%. Therefore, systematic testing for microalbuminuria is important for comprehensive diagnosis and risk assessment in patients with arterial hypertension.
Cardiovascular risk stratification and the impact of missing data
Hypertension management should be based on individual cardiovascular risk assessment. Therefore, comprehensive risk stratification is of great value. The present results showed that most cardiovascular risk factors were documented with high completeness. However, substantial gaps were found for the measurement of waist circumference, which was missing in 91.8% of patients, as well as for the assessment of cardiovascular family history, which was missing in 46.6% of cases. Diabetes mellitus was recorded in all patients and creatinine levels to evaluate GFR were determined in almost 90% of patients. In contrast, screening for subclinical organ damage, such as microalbuminuria or LVH, was performed inconsistently. On the other hand, documentation of established cardiovascular disease was largely complete, demonstrating that about every fifth hypertensive patient suffered from cardiovascular disease. Nevertheless, incomplete recording of data on subclinical organ damage seen in HccH indicates that cardiovascular risk might be substantially underestimated in patients with arterial hypertension. 27 Since cardiovascular risk affects both timing and selection of antihypertensive treatment, it is apparent that a more comprehensive approach for risk stratification could result in earlier and more targeted antihypertensive therapy, thereby beneficially affecting prognosis in these patients.
Implications for clinical practice
Increasing the number of parameters to determine overall cardiovascular risk in the individual patient is beneficial, but may also have its drawbacks. It is conceivable that the more risk factors are evaluated, the more accurate the risk estimate will be. However, the value of adding further risk factors to the risk stratification process may be limited by only minor incremental improvements with regard to the accuracy of risk estimates. 28 Furthermore, including a higher number of risk factors may result in a more complex, time-consuming and costly risk stratification process that may no longer be feasible in daily clinical practice. Therefore, besides statistical considerations the incremental benefit and cost-effectiveness of including additional risk factors in the risk stratification process need to be taken into account. 29 In this respect, the 2013 ESH/ESC Guidelines provide guidance on the selection of relevant and cost-effective screening tests. 13 However, the results of this study suggest that guidelines are not fully implemented in Swiss primary care yet. In particular, this applies to the awareness of the importance of comprehensive assessment of subclinical organ damage. Potential approaches may include targeted education activities and improved communication of guideline recommendations, as well as incentivizing GPs to integrate comprehensive risk stratification processes in daily practice. In addition, our data demonstrate that the assessment of physical activity is not an integral part of cardiovascular risk stratification in Switzerland. In view of recent publications demonstrating beneficial effects of regular physical exercise on the incidence of arterial hypertension as well as on BP control, particular importance should be attached to this topic. 30
Limitations
Several points should be considered as potentially limiting the interpretation and generalizability of the results of this study. Since decisions on patient recruitment as well as on the diagnosis of arterial hypertension, subclinical organ damage and comorbidities were at the discretion of the treating GP, a selection and inclusion bias cannot be completely excluded. In addition, cardiovascular risk in this cohort may have been underestimated due to numerous missing data. Nevertheless, baseline patient characteristics in this study were comparable with those found in previous studies. Moreover, being performed in a real-world setting, the results of this study adequately reflect the current situation and the challenges related to the management of arterial hypertension in Swiss primary care.
Conclusion
The HccH demonstrated a high rate of cardiovascular risk factors, subclinical organ damage and established cardiovascular and renal disease in primary care patients with arterial hypertension assessed in a cross-sectional approach. Despite treatment with either antihypertensive drugs and/or lifestyle modifications, almost half of the patients continued to have a high or very high overall cardiovascular risk. While cardiovascular risk factors, diabetes mellitus, and concomitant cardiovascular and renal disease were recorded with high completeness, screening for subclinical organ damage was incomplete, indicating that cardiovascular risk in primary care may be substantially underestimated. As a consequence, adequate measures should be taken to improve the process of cardiovascular risk stratification, since the detection of subclinical organ damage yields important information about cardiovascular risk and provides the basis for targeted antihypertensive treatment.
Footnotes
Author contribution
Authors AH and SBZ contributed equally to this manuscript. BM, PT, AZ and TD contributed to the conception or design of the work. All contributed to the acquisition, analysis, or interpretation of data for the work. AH, SBZ, JM and TD drafted the manuscript. SG, CG, BM, PT, JDL, AZ and TD critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The authors of this study would like to thank all participating GPs and in particular the physicians’ network of northwestern Switzerland for their highly appreciated support in patient recruitment. Part of this work was presented at the Annual Meeting of the Swiss Society of Internal Medicine 2015 in Basel, Switzerland. FM253: A Handschin, A Zeller, P Tschudi, B Martina, J Leuppi, T Dieterle. Cardiovascular risk profile and blood pressure control in treated hypertensive patients – an analysis from the Swiss hypertension cohort study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grants were received from the Swiss Society of Hypertension, Berne, Switzerland, Gottfried and Julia Bangerter-Rhyner-Foundation, Switzerland, Laboratory Rothen Basel, Switzerland, MSD Chibret AG Switzerland, Novartis Pharma Switzerland, Pfizer Pharma Switzerland, Robapharm Switzerland, Sandoz Pharma Switzerland, Sankyo Pharma Switzerland, and Spirig Pharma AG, Switzerland.