
Abstract
Background:
The association between chronic beta-blocker treatment and haemodynamics at admission in patients with ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention is not well studied. We investigated the impact of chronic beta-blocker treatment on the risk of cardiogenic shock and pre-shock at admission in patients with ST-segment elevation myocardial infarction treated by primary percutaneous coronary intervention.
Methods and results:
A total of 4907 patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention were included in the study. A total of 1148 patients (23.3%) were on chronic beta-blocker treatment. Cardiogenic shock was observed in 264 patients (5.3%). Pre-shock was defined as a shock index (the ratio of heart rate and systolic blood pressure) of 0.7 or greater, and was observed in 1022 patients (20.8%). The risk of cardiogenic shock in patients with chronic beta-blocker treatment was not increased (adjusted hazard ratio (HR) 0.97, 95% confidence interval (CI) 0.65–1.46, P=0.90). Chronic beta-blocker treatment was also not associated with an increased risk of pre-shock (adjusted HR 0.86, 95% CI 0.68–1.07, P=0.19). Also after propensity score matched analysis, there was no increased risk of cardiogenic shock or pre-shock in patients with chronic beta-blocker treatment (respectively HR 0.97, 95% CI 0.61–1.51, P=0.88 and HR 0.82, 95% CI 0.65–1.06, P=0.12).
Conclusion:
In ST-segment elevation myocardial infarction, chronic beta-blocker treatment is not associated with an increased risk of cardiogenic shock or pre-shock.
Introduction
Beta-blockers are widely used, with several indications in the treatment of cardiovascular disease, including stable angina, hypertension, arrhythmias and heart failure. Apart from the favourable effects, beta-blockers may have negative effects on haemodynamics. 1 In the acute phase of ST-segment elevation myocardial infarction (STEMI), left ventricular function may be severely depressed, leading to an increased risk of heart failure and mortality. 2 There has been concern about early beta-blocker use in patients with STEMI. 1 However, several studies have suggested beneficial effects of early administration of beta-blockers in patients with STEMI.3–5 Recently published data have shown that early beta-blocker administration did not result in increased cardiogenic shock (CS) at admission. 6 However, the effect of chronic beta-blocker treatment on admission haemodynamics in STEMI is still unclear. We investigated the risk of chronic beta-blocker treatment on either CS or pre-shock in patients with STEMI, treated by primary percutaneous coronary intervention (PCI).
Methods
Data for this study are from the prospective cohort of patients with STEMI at the Isala Heart Centre, Zwolle, The Netherlands, from January 2005 to December 2011. To avoid double inclusion, only the first recorded admission for STEMI was included. Patients were diagnosed with STEMI if they had chest pain of more than 30 minutes duration and electrocardiographic changes with ST-segment elevation greater than 2 mm in at least two precordial or greater than 1 mm in the limb leads. Prior to the primary PCI procedure, all patients received 300–500 mg of aspirin intravenously, a P2Y12 blocker (either 600 mg of clopidogrel or 180 mg of ticagrelor), and 5000 international units of unfractionated heparin. Ischaemic time was calculated from symptom onset to first balloon inflation. Patients with out-of-hospital cardiac arrest were not included in this analysis.
Definitions
The primary endpoint of this study was CS at admission. This was defined as a systolic blood pressure less than 90 mmHg for at least 30 minutes, clinical signs of pulmonary congestion and end-organ hypoperfusion (cool extremities, altered mental status, or a urine output of <30 ml/hour). 2 The secondary endpoint of this study was pre-shock, which was defined as a shock index (SI) of 0.7 or greater.7,8 SI was defined as the ratio of heart rate and systolic blood pressure on hospital admission. Coronary angiographic flow was determined in accord with the classification system of the Thrombolysis in Myocardial Infarction (TIMI) study group.
Statistics
Statistical analysis was performed with the Statistical Package for the Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA). Continuous data are presented as mean ± standard deviation or median (interquartile range 25–75) for non-normal distributed variables; whereas discrete data are given as absolute values and percentages.
To define potential confounders, we compared baseline characteristics between patients with and without chronic beta-blocker treatment. We assessed the risk of CS and pre-shock at admission in both patient groups. Stratified analyses were performed to assess the prognostic importance in subgroups and to investigate potential effect modification. To demonstrate the independent predictive value of chronic beta-blocker treatment on CS and pre-shock, multivariable analyses were performed, using a binary logistic regression analysis model, adjusting for age, gender, previous myocardial infarction (MI), previous PCI, previous coronary artery bypass grafting (CABG), hypertension, infarct-related vessel (left main, left anterior descending, ramus circumflex, right coronary artery), multivessel disease and year of hospitalisation. A P value of 0.05 was determined as significant.
We also performed a propensity analysis for receiving a beta-blocker. A propensity score matched multivariable analysis was performed to assess the risk of CS and pre-shock in both patient groups.
Results
A total of 4907 patients were included in the current analysis. A total of 1148 patients (23.3%) were on chronic beta-blocker treatment. Baseline characteristics and a comparison between patients who were on chronic beta-blocker treatment and those who were not are summarised in Table 1. In short, patients with pre-admission beta-blocker use were older and more often female. Furthermore, they more often had a history of hypertension or MI.
Baseline characteristics of patients with and without chronic beta-blocker treatment.
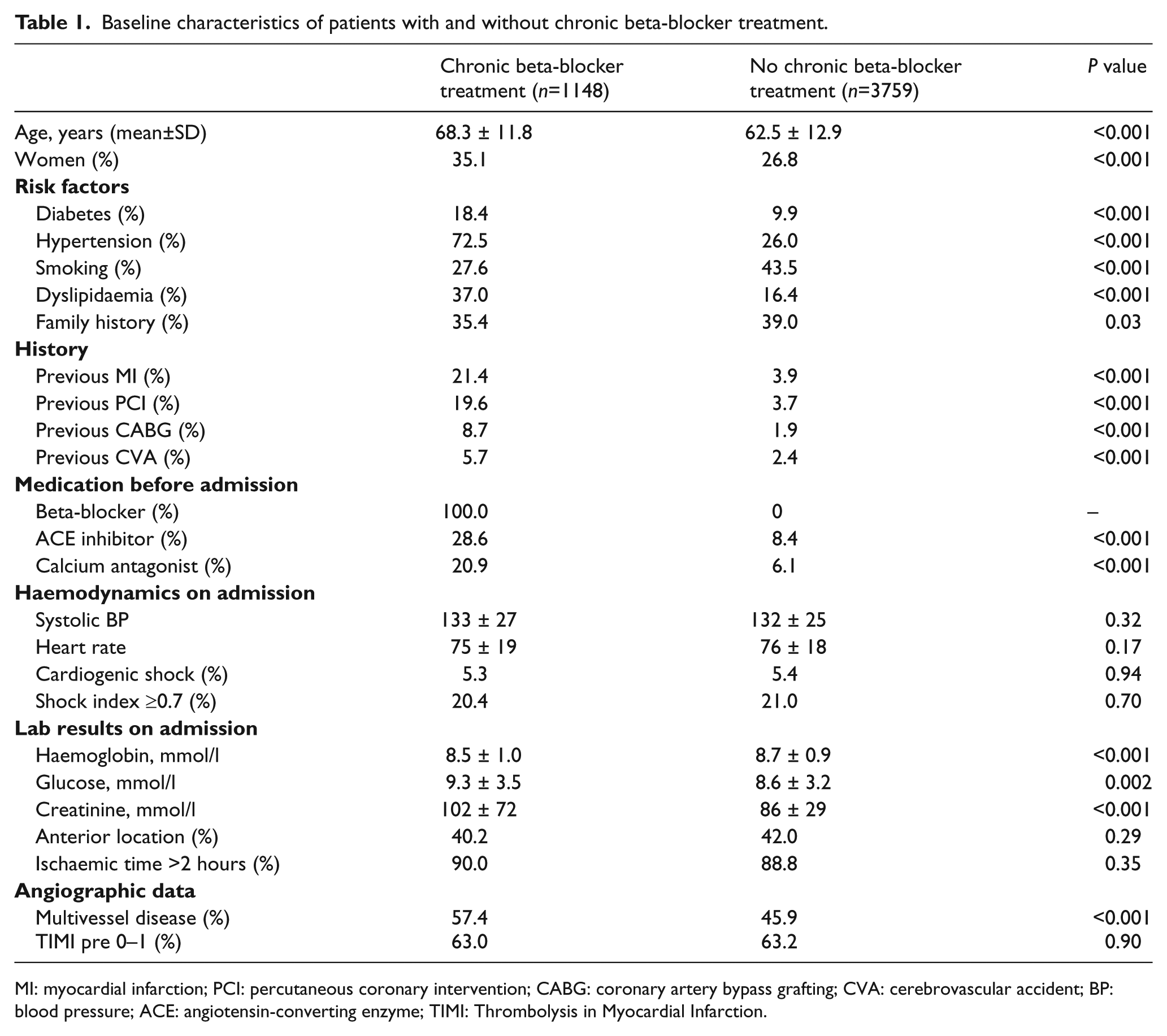
MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; CVA: cerebrovascular accident; BP: blood pressure; ACE: angiotensin-converting enzyme; TIMI: Thrombolysis in Myocardial Infarction.
A total of 264 patients (5.3%) had CS on admission. Differences in baseline variables between patients with and without CS are summarised in Table 2. Patients with CS more often had multivessel disease and an occluded infarct-related vessel (TIMI score pre-PCI of 0–1) and less often had anterior wall location. There was no difference in beta-blocker treatment in patients with and without CS.
Baseline characteristics of patients with and without cardiogenic shock on admission.
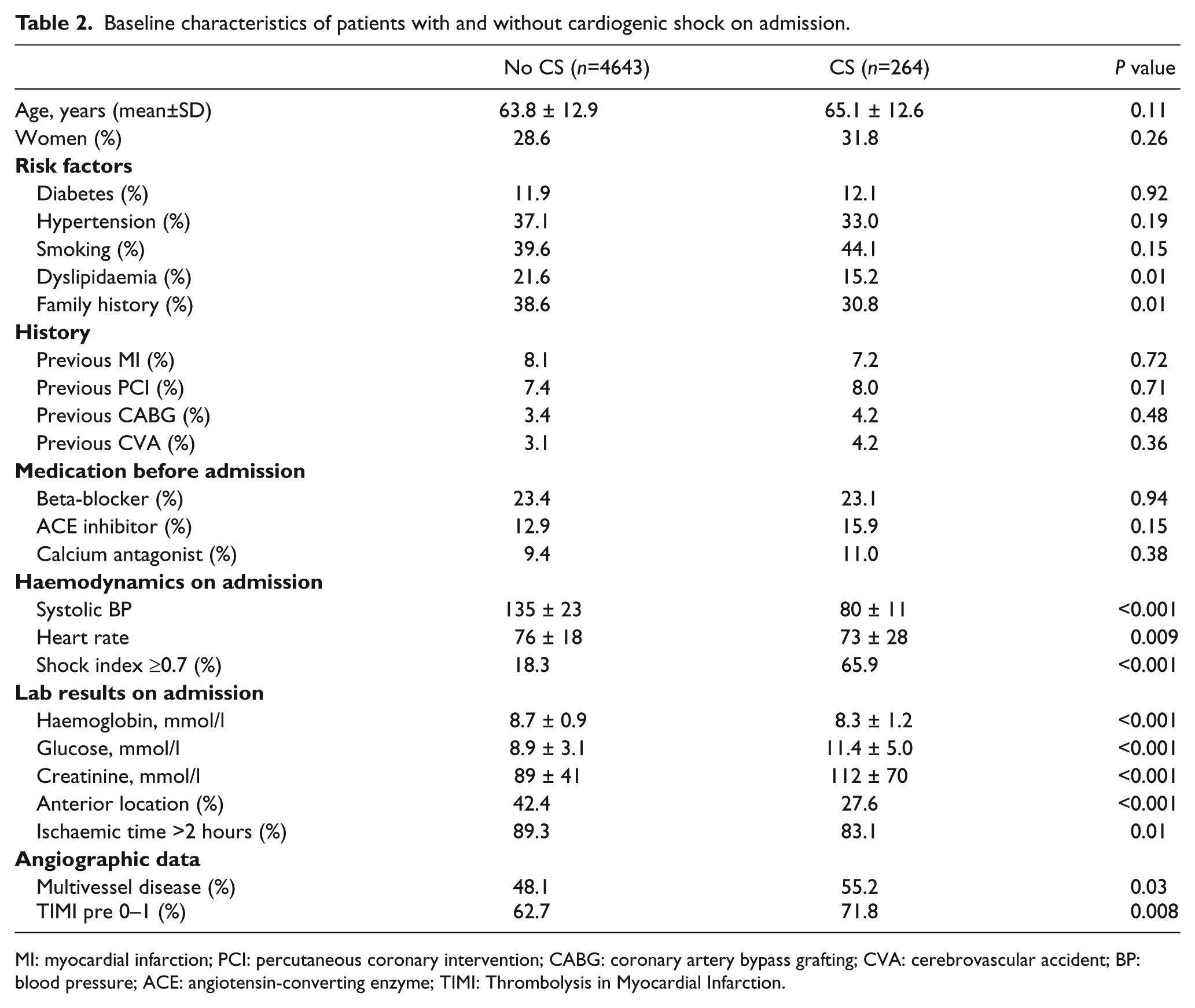
MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; CVA: cerebrovascular accident; BP: blood pressure; ACE: angiotensin-converting enzyme; TIMI: Thrombolysis in Myocardial Infarction.
A total of 1022 patients (20.8%) were in pre-shock (SI ≥0.7). Differences between patients with and without pre-shock are summarised in Table 3. There was also no difference in beta-blocker treatment in patients with and without SI of 0.7 or greater. Patients with SI of 0.7 or greater more often had diabetes mellitus and anterior infarct location.
Baseline characteristics of patients with and without pre-shock (SI ≥0.7) on admission.
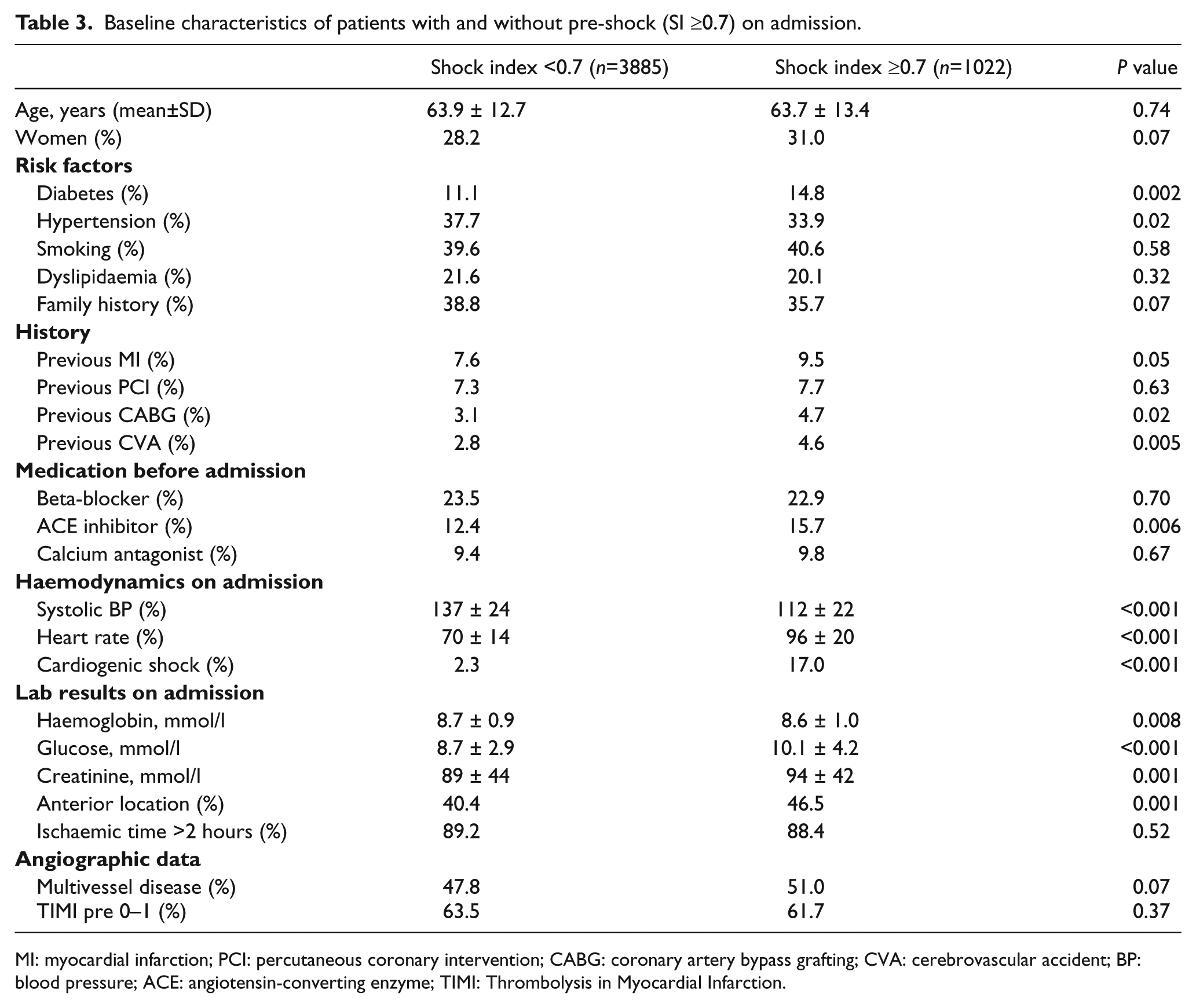
MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; CVA: cerebrovascular accident; BP: blood pressure; ACE: angiotensin-converting enzyme; TIMI: Thrombolysis in Myocardial Infarction.
After univariable analyses, the risk of CS in patients with chronic beta-blocker treatment was comparable to those without chronic beta-blocker treatment, odds ratio (OR) 1.0 (95% confidence interval (CI) 0.7–1.3). Also, the risk of pre-shock was identical in patients with chronic beta-blocker treatment, OR 1.0 (95% CI 0.8–1.1). The results of stratified analyses are summarised in Figures 1 and 2. There was no subgroup of patients with chronic beta-blocker treatment with an increased risk of CS. In patients with previous CABG, chronic beta-blocker treatment was associated with a reduced risk of CS. However, this concerned a very small group of patients. There was no subgroup of patients with chronic beta-blocker treatment with an increased or reduced risk of pre-shock.
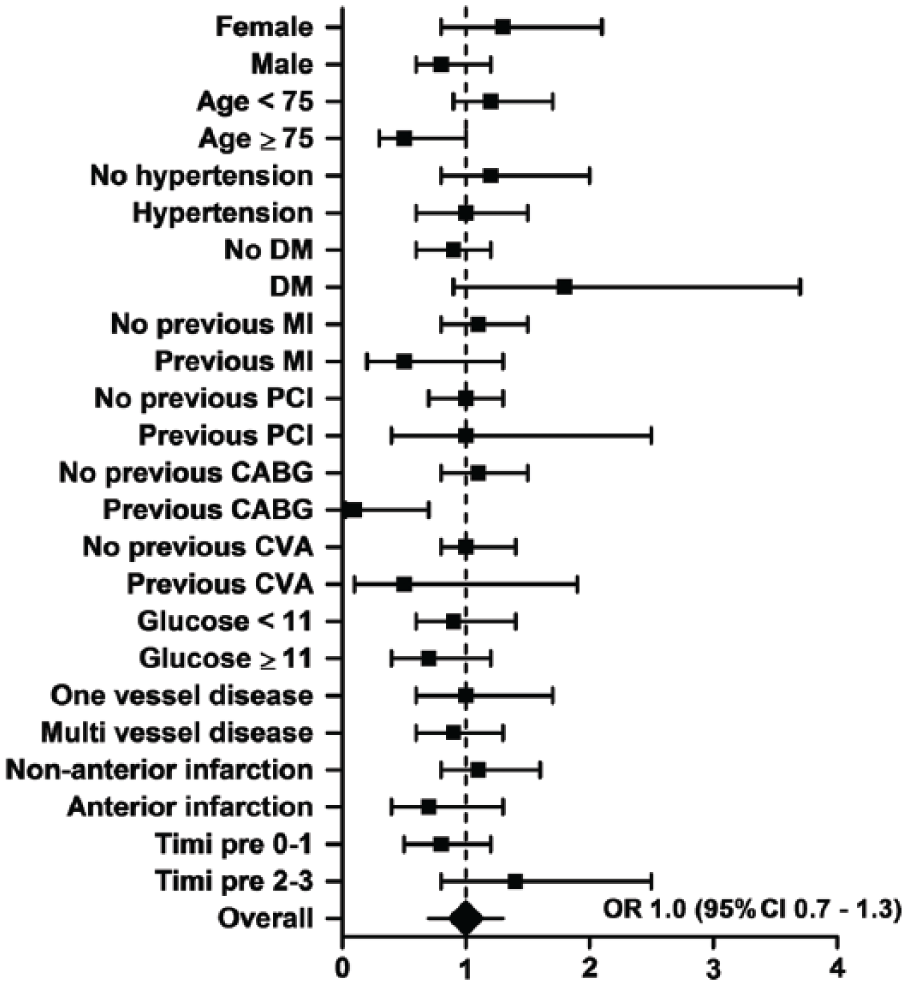
Risk of cardiogenic shock in patients with chronic beta-blocker use.
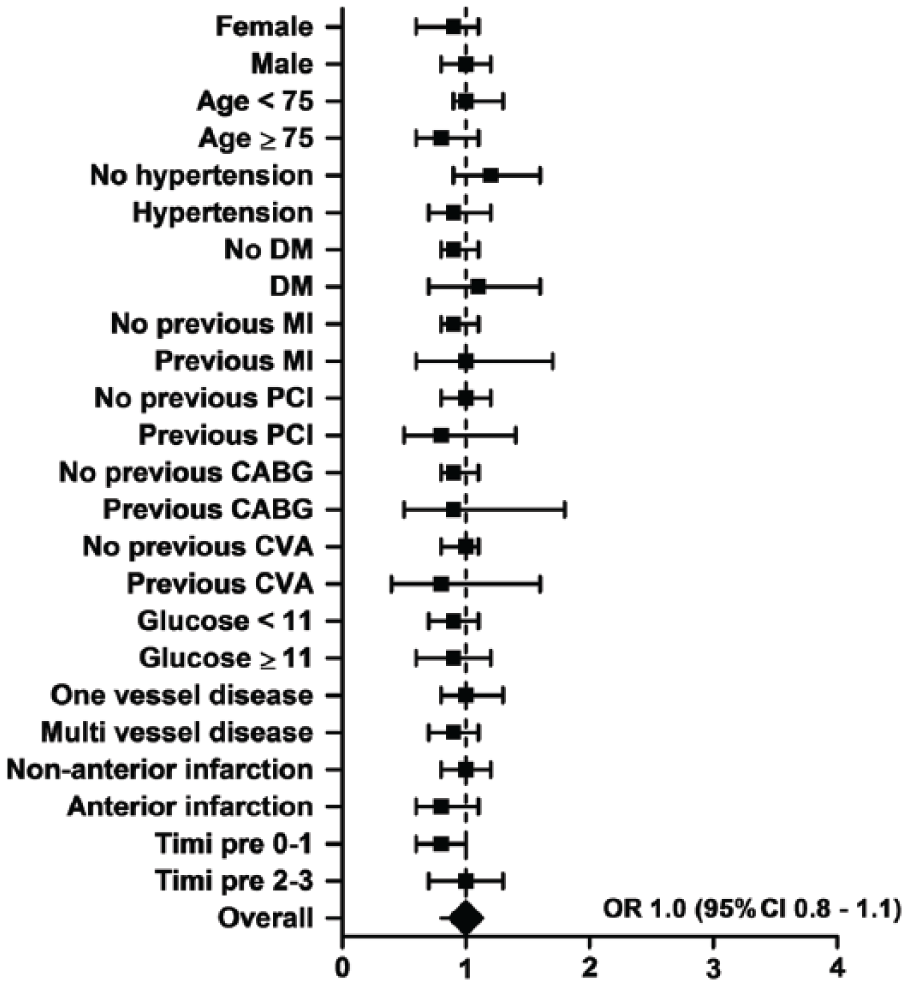
Risk of pre-shock in patients with chronic beta-blocker use.
Multivariable analyses were performed to adjust for potential confounders. After adjusting for age, gender, previous MI, previous PCI, previous CABG, hypertension, infarct-related vessel, multivessel disease and year of hospitalisation, there was no impact of chronic beta-blocker treatment on the risk of CS at admission (hazard ratio (HR) 0.97, 95% CI 0.65–1.46, P=0.90). Chronic beta-blocker treatment was also not associated with a reduced or increased risk of pre-shock (HR 0.86, 95% CI 0.68–1.07, P=0.19).
After propensity score matched multivariable analysis, there was still no impact of chronic beta-blocker treatment on the risk of CS or pre-shock at admission (respectively HR 0.97, 95% CI 0.61–1.51, P=0.88 and HR 0.82, 95% CI 0.65–1.06, P=0.12).
Discussion
In this large registry of patients with STEMI treated by primary PCI, there was no evidence of deteriorated haemodynamics on admission in patients on chronic beta-blocker treatment.
In our study, anterior MI was significantly less present in patients with CS. However, the presence of inferior MI was significantly higher in patients with CS versus without CS (respectively 49.4% vs. 38.9%, P=0.001), suggesting right ventricular involvement or atrioventricular-nodal block or vasovagal reactions. This also explains the lower heart rate in CS patients versus patients without CS. Although in general patients with inferior wall MI have a better prognosis, those who have hypotension and right ventricular involvement may have a poor prognosis. 9
Comparison with previous studies
Beta-blockers reduce mortality when administrated after MI.10,11 They also decrease the incidence of recurrent MI, recurrent ischaemia and life-threatening arrhythmias and improve left ventricular remodeling. Therefore, the use of beta-blockers constitutes a class I indication in clinical guidelines.12–14 However, the effects of early beta-blocker administration on admission haemodynamics in STEMI patients had been studied poorly until recently. In the COMMIT trial, 1 the prevalence of recurrent MI or ventricular fibrillation was significantly lower in patients treated with beta-blockers before admission. However, this was counterbalanced by a 1.1% increase in cardiogenic shock. Based on this trial, it was suggested that it might be more prudent to start beta-blockers only after a patient’s haemodynamic condition has stabilised after acute MI. However, in COMMIT reperfusion was performed with thrombolytics, and patients scheduled for PCI were even excluded. Furthermore, the dose of beta-blockers may have been too high in COMMIT, especially in selected patients with low blood pressure.
An older study suggested a reduced risk of mortality in patients taking beta-blockers before admission, but that study was performed in patients who were not treated by primary PCI. 15
In the era of primary PCI the effect of beta-blocker treatment before admission has been analysed in a limited number of studies.3,6,16,17 In an observational study, STEMI patients treated by primary PCI showed that elevated admission heart rate was associated with a long-term increase of all-cause mortality, and beta-blocker therapy reduced mortality in patients with elevated admission heart rate. 4
The METOCARD-CNIC trial used the same beta-blocker scheme as in the COMMIT trial in anterior STEMI during transportation to the PCI centre. The authors showed that early intravenous beta-blockers reduced infarct size and improved left ventricular ejection fraction, with no excess of adverse events or CS. 17 In the recently published Early-BAMI trial, 6 early metoprolol administration did not reduce infarct size, but also did not increase adverse events such as CS. However, these trials focused on the effect of beta-blockers on infarct size and left ventricular function. Our study focused on chronic beta-blocker treatment and its effect on admission haemodynamics in STEMI patients.
Strengths and limitations
We studied the independent prognostic importance of chronic beta-blocker treatment on the risk of CS and pre-shock at admission in STEMI patients. The strength of this study is the large STEMI cohort and the addition of a propensity score matched analysis. Also, the cohort studied is comparable to other STEMI cohorts.
Our study, however, also has some limitations. Our study was a retrospective cohort study. A major limitation is that we had no data about left ventricular function in most patients. We had no data on the use of inotropics before admission, although this medication is rarely given in the ambulance. We had also no data on type, dose and duration of beta-blocker treatment before admission.
Clinical implications
Beta-blockers are drugs with multiple actions on the heart. Blockade of β1 receptors results in a reduction of myocardial oxygen demand by the reduction of heart rate and myocardial contractility. In the context of acute MI, which represents a state of reduced oxygen supply to the affected portion of the heart, these effects may be beneficial. But there is debate as to whether pre-reperfusion administration of intravenous beta-blockers may reduce infarct size as compared with post-reperfusion administration, and whether this will be safe, without increasing the risk of CS. In the current era of primary PCI, the METOCARD-CNIC trial showed reduced infarct size and increased left ventricular ejection fraction in anterior wall STEMI patients without signs of heart failure treated with early intravenous metoprolol.5,17 However, that single study had a limited sample size, was not blinded, not placebo controlled, and included a selected patient group. The recently published Early-BAMI trial has a larger sample size in which beta-blocker administration before primary PCI was studied in all patients with STEMI, with a double blinded, placebo controlled design. 6 The trial did not show a reduction in infarction size, but did reduce the incidence of malignant arrhythmias in the acute phase and was not associated with an increase in adverse events. Our study shows that chronic beta-blocker use did not increase the incidence of CS or pre-shock at admission in STEMI patients. These results support the Early-BAMI trial with respect to haemodynamics.
Conclusion
In STEMI patients treated by primary PCI, chronic beta-blocker treatment is not associated with an increased risk of CS or pre-shock at admission.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.