
Abstract
Objective:
To provide a comprehensive overview of the diagnosis and management of temporomandibular disorders (TMDs) in patients with comorbid sleep-related conditions, specifically obstructive sleep apnoea (OSA) and sleep bruxism, while exploring their clinical interrelationships within an integrated dental care model.
Methods:
A narrative review of the existing literature was conducted to synthesise current evidence regarding the physiological and pathological links between sleep disordered breathing, neuromuscular jaw dysfunction, and nocturnal parafunctional habits.
Results:
This review demonstrates that TMD and sleep disorders are intrinsically linked, with sleep bruxism often acting as a potential protective mechanism for airway patency in OSA patients, while fragmented sleep exacerbates chronic TMD pain. Findings suggest that a “siloed” treatment approach often leads to sub-optimal outcomes. Conversely, an integrated diagnostic framework – utilising screening questionnaires alongside clinical TMD examinations – facilitates more accurate identification of these interrelated conditions.
Conclusion:
Effective management requires a shift from isolated dental interventions to a coordinated, interdisciplinary approach. By combining conservative measures, such as sleep hygiene and physiotherapy, with targeted therapies like mandibular advancement devices, dentists can significantly enhance oral rehabilitation success. Collaboration between dental professionals and medical sleep specialists is essential to ensure patient safety, optimise treatment sequencing, and improve the overall quality of life for patients presenting with this complex triad of disorders.
Keywords
Learning Objectives
To describe the clinical interrelationship between TMD, obstructive sleep apnoea, and sleep bruxism
To identify key history, examination findings, and screening tools for patients with suspected TMD and sleep-disordered breathing
To outline evidence-based management strategies for patients with coexisting TMD and sleep disorders
To explain why interdisciplinary collaboration is essential to optimise treatment sequencing, patient safety, and long-term outcomes in dental sleep medicine
Introduction
Temporomandibular disorders (TMDs) encompass a heterogeneous group of conditions affecting the temporomandibular joints (TMJs), masticatory musculature, and associated structures. Characterised by orofacial pain, joint sounds, and functional limitations, i.e. restricted jaw movement or difficulty chewing, TMD affects approximately one in 15 people in the UK, with a documented predilection for women and adults aged 20–40 years.1,2 Beyond local dysfunction, TMD is a primary driver of chronic orofacial pain, significantly diminishing patient quality of life. Sleep-related breathing disorders – most notably obstructive sleep apnoea (OSA) and sleep bruxism (SB) – are recognised as widespread conditions among adults, with a prevalence of about 12%. 3 OSA, defined by recurrent upper airway obstruction during sleep, leads to intermittent hypoxia and sleep disruption. With an estimated one billion adults affected globally, OSA is no longer a niche concern but a major contributor to fatigue, cardiovascular disease, cognitive decline, and metabolic dysfunction. 4 There is an increasing clinical recognition of the complex interplay between TMD and sleep disturbances. Patients with TMD frequently report poor sleep quality while those diagnosed with OSA or SB often present with secondary jaw pain or dysfunction. These conditions share a cluster of common risk factors, including age, chronic stress, and obesity which can create a cycle of exacerbation. For example, OSA-induced sleep fragmentation and intermittent hypoxia can lead to central sensitisation, effectively heightening pain sensitivity and worsening TMD symptoms. Conversely, persistent, high-intensity TMD pain can prevent patients from entering deep, restorative sleep stages, creating a feedback loop of fatigue and chronic pain. Notably, SB is frequently observed in OSA patients, with nearly half showing signs of bruxism, 4 suggesting a possible causal or adaptive relationship between airway obstruction and jaw activity. These interrelationships have profound implications for comprehensive dental management.
In complex cases, such as full mouth rehabilitations, failing to address OSA or SB can lead to mechanical restorative failure, persistent post-operative discomfort, and patient dissatisfaction. This article synthesises current evidence and clinical guidelines to provide a roadmap for the diagnosis and management of these coexisting conditions. It details diagnostic protocols and a spectrum of treatment modalities – from conservative cognitive-behavioural strategies and physiotherapy to advanced appliance therapy and surgical intervention – while reinforcing the necessity of interdisciplinary collaboration to optimise long-term patient outcomes.
Sleep bruxism (SB)
SB is defined as an involuntary rhythmic masticatory muscle activity (RMMA) characterised by clenching, grinding, bracing or thrusting of the mandible during sleep. 5 Clinical indicators of bruxism include masseteric hypertrophy, reported grinding or clenching by the patient, soft tissue indentations or trauma (e.g. cheek biting and tongue scalloping), and signs of occlusal wear or fracture of teeth or restorations. 6 While SB affects approximately 5–15% of the adult population, 7 its clinical manifestation differs significantly from awake bruxism (AB), which primarily involves sustained clenching. Research suggests that these are distinct entities, with patients rarely exhibiting both behaviours simultaneously.8,9 In healthy individuals, bruxism is no longer regarded strictly as a parafunctional habit or disorder, but rather as a behaviour that may act as a risk factor or potentially a protective mechanism for outcomes such as tooth wear and tooth or restoration fractures.10,11 The association between bruxism and TMDs remains complex. Current evidence does not support a definitive causal association between either form of bruxism and/or TMD.12 -15 While bruxism may contribute to TMD as part of a multifactorial aetiology, it is unlikely to initiate or sustain TMD symptoms in the absence of other contributing factors.
Obstructive sleep apnoea (OSA)
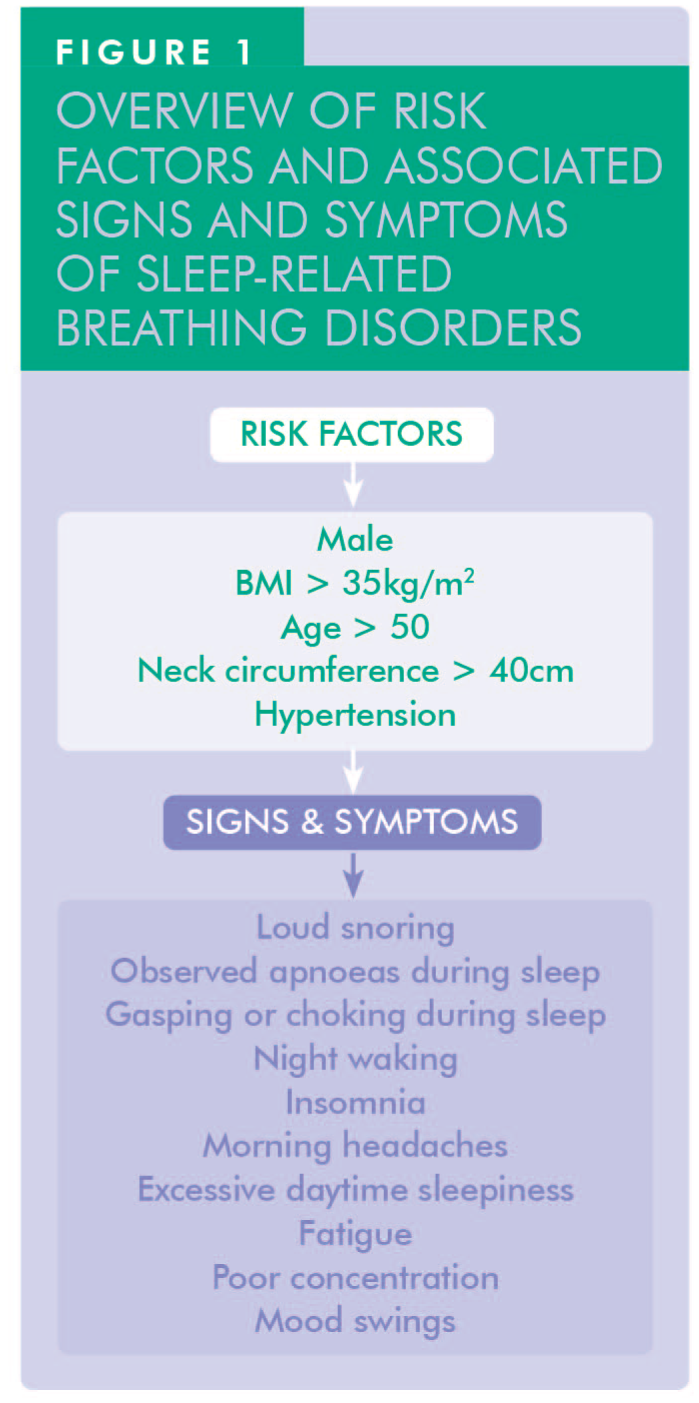
OSA is a common sleep-related breathing disorder linked to significant morbidity and mortality.16 -20 Despite its potentially life-threatening consequences, many individuals with OSA remain undiagnosed.21,22 Clinical evidence indicates that TMDs are significantly greater in the OSA population than in the general public.23 -25 Common symptoms that may indicate undiagnosed OSA include excessive daytime sleepiness, morning headaches, mood disturbances, impaired cognitive concentration, and reports from bed partners of gasping, choking, snoring, or breathing pauses during sleep. Given the life-threatening consequences of untreated OSA – including hypertension, cardiovascular disease, and metabolic dysfunction – it is incumbent upon dental clinicians to screen for ‘red flag’ symptoms during routine TMD evaluations (Figure 1).
TMD–sleep disorder interrelationship
The interrelationship between TMD and sleep disorders is well established.26 -31 Since poor sleep can heighten pain sensitivity and chronic TMD pain can disrupt sleep, a brief discussion about sleep habits should be part of the routine clinical evaluation. For patients showing signs of disturbed sleep, providing guidance or directing them to sleep hygiene strategies (the everyday habits and environmental adjustments that support good sleep) can support both symptom relief and overall treatment outcomes. Key elements of sleep hygiene strategies are a consistent sleep–wake routine, a quiet/comfortable sleep setting, and the avoidance of common disruptors (e.g. late caffeine/nicotine, alcohol near bedtime, long/late naps, high arousal before bed). 32 SB can overload the masticatory system, leading to muscle or joint pain, while TMD pain may disrupt sleep continuity. More recently, attention has turned to the links between TMD and OSA. 33 Systemic effects of OSA, such as increased pain sensitivity or delayed healing, may complicate TMD treatment. Risk factors like age, obesity, and stress are shared, and TMD, SB, and OSA commonly coexist. Dental practitioners should screen for overlapping conditions. Inappropriate appliance use can exacerbate events. For example, an occlusal appliance designed solely to treat TMD or protect against SB may allow for mandibular retrusion, potentially worsening undiagnosed OSA. This can lead to exacerbation of apnoeic events, while neglecting TMD in OSA patients, potentially leading to pain flares following oral appliance therapy. Conversely, initiating mandibular advancement device (MAD) therapy for OSA in a patient with pre-existing TMD can trigger acute pain flares if the joint and musculature are not properly stabilised beforehand.
Pathophysiological links: Underlying mechanisms of interaction
Arousal-linked bruxism 14
OSA is characterised by recurrent episodes of oxygen desaturation and sympathetic nervous system activation that precipitate cortical micro-arousals. These arousals may coincide with RMMA, which may function as a protective response to reopen the airway. However, repeated bruxism can overload the TMJs and contribute to pain and dysfunction.
Pain and sleep disruption 25
The relationship between TMDs and sleep quality is characterised by a sophisticated bidirectional influence, mediated by the autonomic nervous system and systemic inflammatory pathways. TMD pain can fragment sleep, while poor sleep quality – especially due to OSA – can increase inflammation and reduce pain thresholds. Clinical evidence demonstrates that successful treatment of OSA reduces TMD symptoms, most likely by improving overall sleep quality. 25
Shared arousal pathways 13
While bruxism and apnoeic events do not demonstrate a strict one-to-one correlation, both are fundamentally mediated by sleep arousals. RMMA and airway restoration often occur synchronously in response to nocturnal hypoxia. Current hypotheses suggest that bruxism may serve a compensatory role in maintaining airway patency via the co-activation of suprahyoid and genioglossus musculature, though this protective mechanism often incurs significant mechanical loading on the TMJs.
Craniofacial phenotypes 34
Skeletal Class II discrepancy, mandibular retrognathia, and a narrow oropharyngeal airway are synergistic risk factors for both OSA and TMD. Furthermore, nasal obstruction-induced mouth breathing necessitates a compensatory downwards and backwards rotation of the mandible; this alters muscular equilibrium and increases tension in the masticatory complex. Concurrently, bruxism-induced occlusal attrition can lead to a loss of vertical dimension, potentially encroaching on the functional airway space and complicating respiratory dynamics.
Neurochemical modulation 34
Shared neurochemical pathways – primarily involving dopamine and serotonin – regulate both autonomic arousal and descending motor control, potentially predisposing individuals to concurrent bruxism and chronic orofacial pain. Furthermore, chronic stress activates the hypothalamic–pituitary–adrenal (HPA) axis, elevating norepinephrine and cortisol levels; this driving force promotes sleep fragmentation and central pain sensitisation. These biochemical commonalities provide a robust rationale for integrating behavioural and psychological interventions into the comprehensive management of these comorbid conditions.
Diagnostic framework and examination protocols
Accurate diagnosis is essential for effective management of patients presenting with suspected TMD and sleep-related breathing disorders. Clinicians should employ a systematic clinical framework to evaluate the functional integrity of the stomatognathic system alongside validated screening metrics for sleep-disordered breathing.
As outlined in the sections below, comprehensive assessment may include the following:
history and symptom review
subjective assessment metrics
sleep diaries and screening
OSA screening questionnaires
airway and craniofacial examination
bruxism screening
History and symptom review
A systematic patient-centred history is the diagnostic cornerstone for managing comorbid TMD and sleep disorders. This phase must move beyond localised dental complaints to capture the broader physiological and behavioural landscape.
TMD symptomatology: Start with a detailed evaluation of primary complaints, specifically addressing jaw pain, stiffness, mechanical locking, or joint noises (clicking or crepitus). Document the chronicity (onset and duration) and aggravating factors, such as mastication or yawning, as well as the success or failure of any past interventions.
Referred pain and comorbidities: Map any associated discomfort, particularly temporal headaches or cervical tension, which often overlap with myogenic TMD.
Behavioural assessment: Systematically explore parafunctional habits, including diurnal (daytime) clenching, nail-biting, or occupational ‘bracing’ behaviours. Distinguishing between daytime muscle activity and nocturnal grinding is a critical step in differential diagnosis.
Sleep architecture screening: Transition to a ‘sleep history’ to assess subjective sleep quality. Key indicators include waking up ‘unrefreshed’, persistent daytime fatigue (somnolence), and chronic snoring. Clinicians should specifically inquire about bed-partner reports of witnessed nocturnal bruxism, gasping, or apnoeic pauses – symptoms that significantly increase the index of suspicion for OSA.
Subjective assessment metrics
Validated screening instruments, such as sleep diaries and standardised questionnaires, provide essential approximations of sleep quality derived from patient-reported outcomes. Although inherently subjective, these tools offer a low-cost, simple-to-use, longitudinal perspective on sleep-related behaviours and perceptions. Despite their subjectivity, these tools demonstrate high sensitivity – often exceeding 90% and ranging from 73% to 97.7% across studies. 35 Specificity is more variable, typically falling between 50% and 96%, but still offering clinically useful complementary data. 35
Sleep diaries 36
A sleep diary serves as a critical longitudinal tool, allowing clinicians to move beyond a single “snapshot” of patient experience to identify consistent behavioural patterns. Patients should be instructed to maintain a diary for one or two weeks to capture both weekday and weekend variability.
Core evaluative components include:
Sleep chronometry: Establishes the total “time in bed” (TIB).
Sleep latency: The duration required to transition from wakefulness to sleep. Latency consistently exceeding 30 minutes may indicate psychophysiological insomnia or heightened sympathetic arousal often seen in TMD patients.
Sleep quality: Nocturnal awakenings for tracking the frequency and duration of time awake after sleep onset.
Subjective rating: A simple Likert scale (1–10) for sleep restorative value, helping correlate ‘poor’ nights with morning jaw pain or stiffness flares.
Daytime function: Napping and somnolence – identifying “sleep debt” or excessive daytime sleepiness (EDS), which are primary indicators for an underlying sleep-disordered breathing condition.
Lifestyle and environmental modulators: Documenting intake timing of caffeine and alcohol. Particularly, alcohol acts as a muscle relaxant that can exacerbate airway collapse (OSA) while increasing RMMA (bruxism) during withdrawal phases.
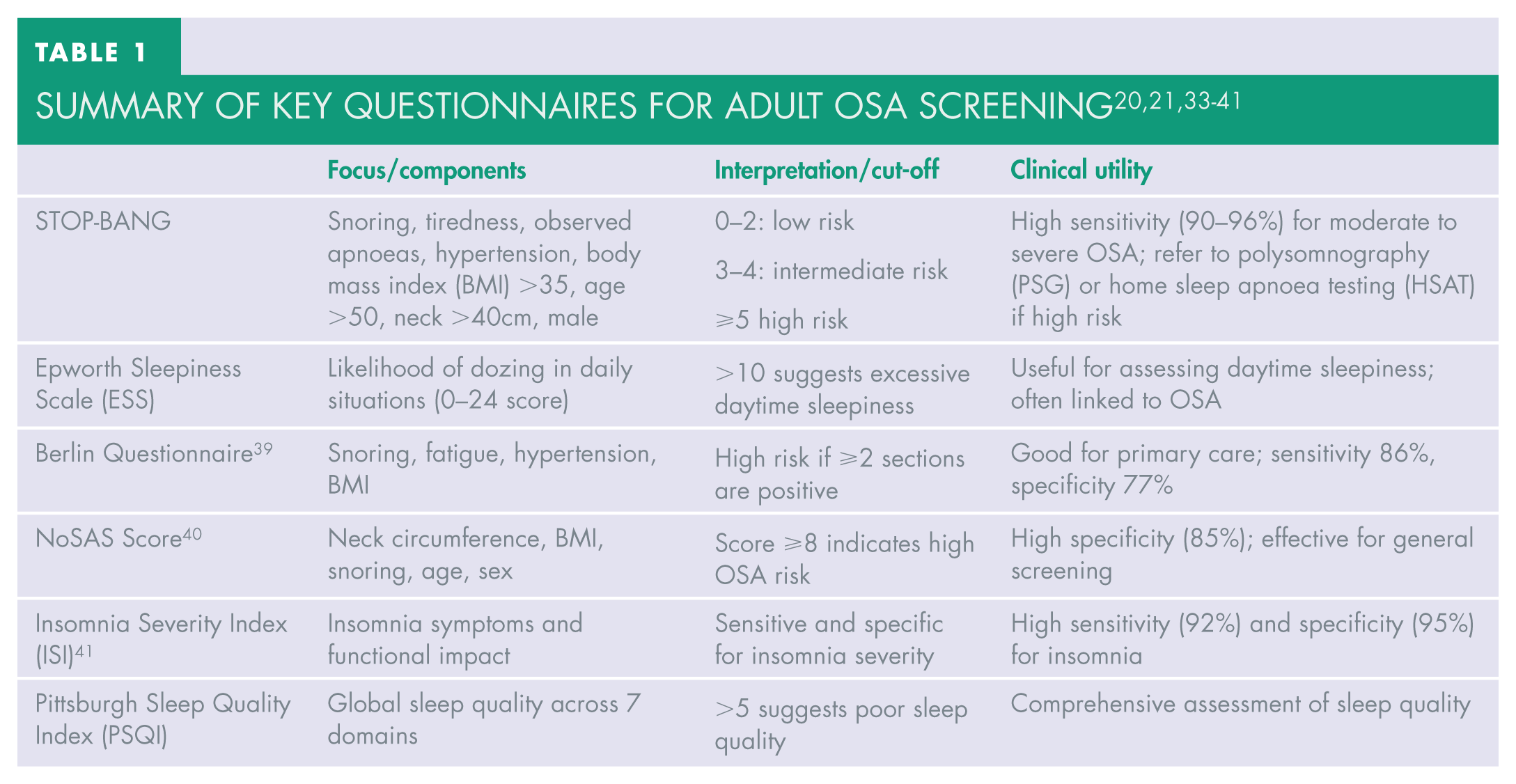
OSA screening questionnaires
Adult sleep screening
Table 1 summarises the most common screening questionnaires used in the diagnosis of OSA in adults.20,21,33 -41
Paediatric sleep screening
The paediatric sleep questionnaire (PSQ) is an effective parent-reported screening tool for identifying OSA in children. With 22 items, it offers strong diagnostic performance, showing sensitivity around 85% and specificity near 87%. 42
Airway and craniofacial examination
To examine the airway, a modified Mallampati classification (Figure 2) assessment should be performed with the patient sitting upright, mouth wide open, and tongue protruded without phonation:
Class I: Full visibility of soft palate, uvula, and tonsillar pillars
Class II: Soft palate and most of the uvula visible
Class III: Only the soft palate and base of uvula visible
Class IV: Only the hard palate visible
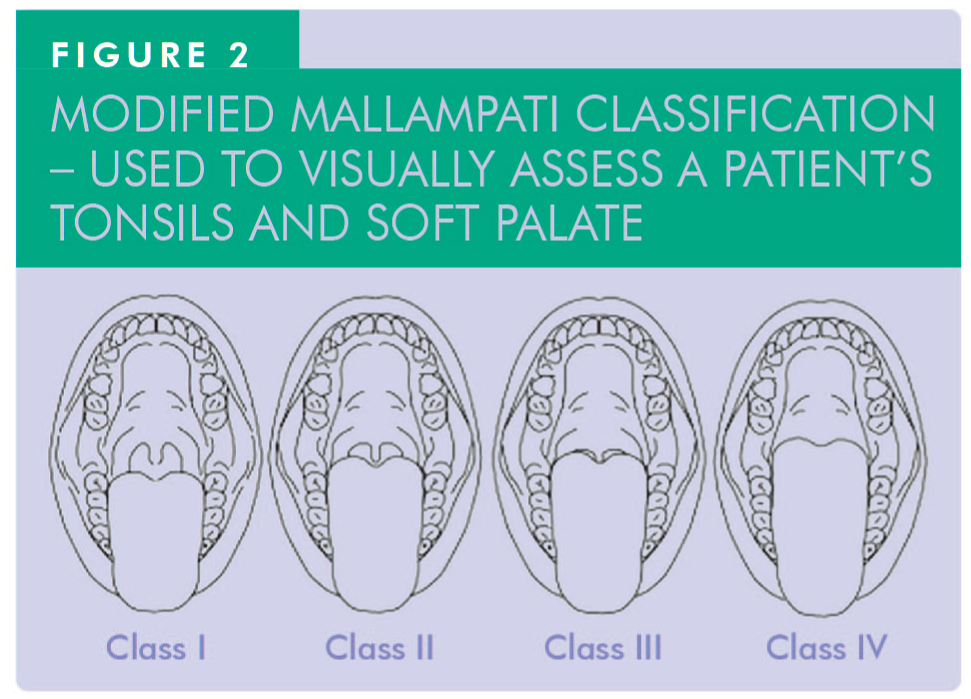
Classes III and IV suggest a crowded oropharynx and higher risk for OSA.43,44
Craniofacial morphological risk factors
Neck circumference: Measuring at the level of the cricothyroid membrane is a highly predictive metric for upper airway crowding. Values over 43cm in men or 41cm in women correlate strongly with increased OSA risk due to the mechanical load of adipose tissue on the pharyngeal wall. 45
Forward head posture: Patients often subconsciously adopt a forward head posture to compensate for a restricted airway. 46 This postural shift increases tension in the suprahyoid and masticatory muscles, often manifesting as myogenic TMD.
Airway obstruction markers
Nasal patency: Evaluate nasal patency, i.e. looking for septal deviation or nasal polyps as they can force a transition to chronic mouth breathing. 44
Tonsillar hypertrophy: Tonsillar size should be graded systematically. According to the modified Mallampati classification, grades 3 or 4 (where tonsils occupy >50% of the oropharyngeal space) can severely narrow the airway and are primary drivers of nocturnal obstruction. 47
Intra-oral indicators of crowding
Tongue scalloping: Indentations on the lateral borders of the tongue indicate a “discrepancy” between tongue volume and the available space in the mandibular arch.48,49 The scalloping suggests that the tongue is being pressed against the teeth – either due to macroglossia or a restricted, narrow oral cavity – making it highly likely to collapse into the oropharynx during sleep when muscle tone decreases.
Bruxism screening5,8
Clinical signs such as tooth wear, muscle hypertrophy, and linea alba support a diagnosis of bruxism. Additional confirmation can be obtained by systematic history-taking or validated questionnaires like the bruxism assessment questionnaire and standardised tool for the assessment of bruxism (STAB). Inquire directly: “Do you wake up with jaw soreness or tooth sensitivity?”; “Has anyone noticed you grinding your teeth at night?” A combination of subjective and objective signs supports a diagnosis of probable SB, as defined by the International Classification of Sleep Disorders. 50
Advanced sleep disorder diagnostics
When initial clinical screening – derived from patient history, physical examination, or validated questionnaires – indicates a significant risk for OSA, definitive diagnostic testing is mandatory. The gold standard is the overnight polysomnography (PSG) conducted in a controlled sleep laboratory environment. 51 This comprehensive assessment monitors a wide array of physiological parameters simultaneously, as outlined below:
Respiratory metrics: Continuous monitoring of nasal/oral airflow and thoracic/abdominal effort to distinguish between obstructive and central apnoeas.
Oximetry: Measurement of oxygen saturation (SpO2) to identify periods of intermittent hypoxia.
Neurological activity: Electroencephalography (EEG) to determine sleep architecture and identify micro-arousals.
Motor activity: Electromyography (EMG) to assess muscle tone and detect RMMA/bruxism.
In addition, the severity of OSA can be quantified by the below indices:52,53
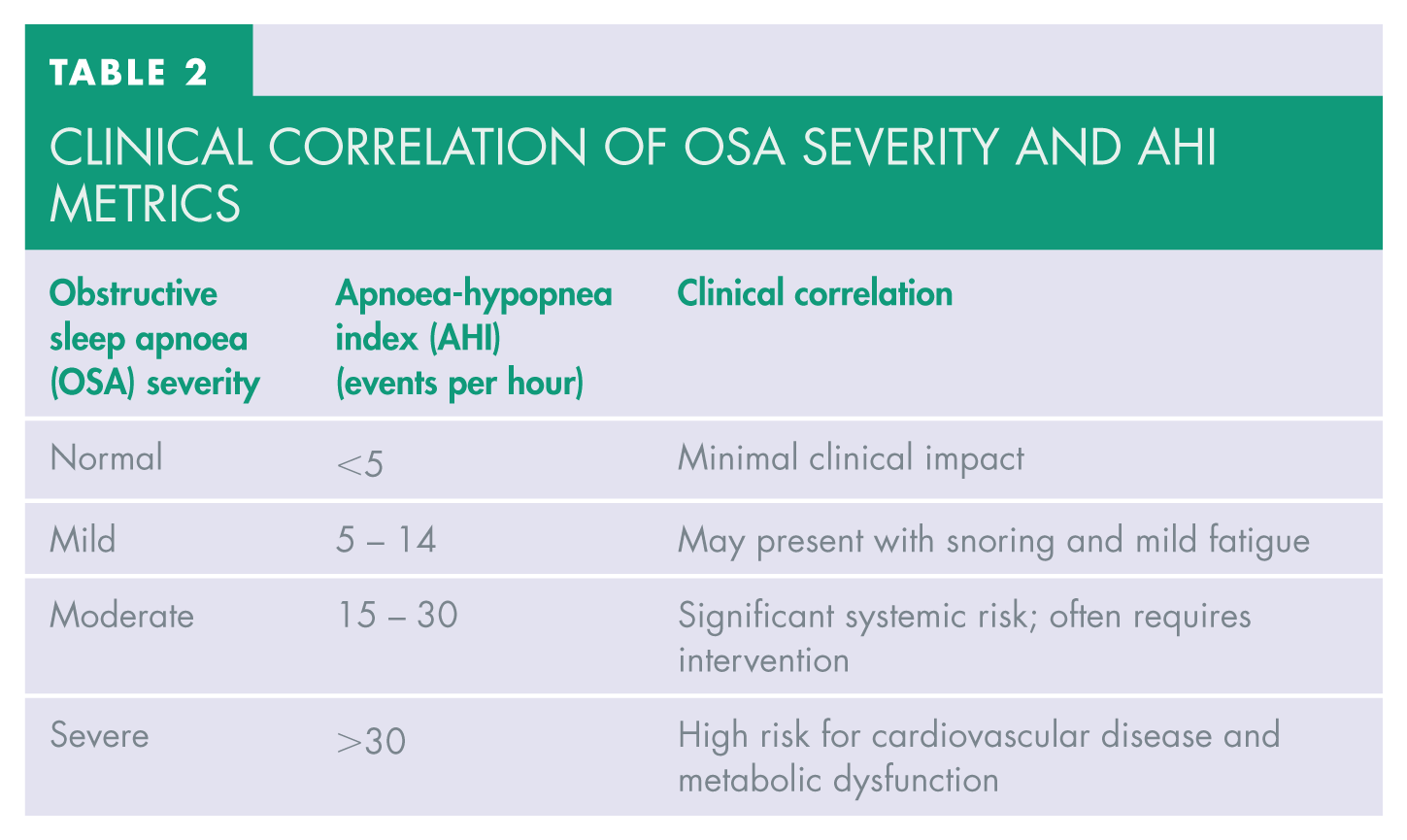
The apnoea-hypopnea index (AHI): The average number of apnoeic events (complete cessation of airflow) and hypophonic events (partial reduction in airflow) per hour of sleep. Table 2 illustrates the relationship between obstructive sleep apnoea severity, apnoea-hypopnoea index thresholds, and their associated clinical implications.
Oxygen desaturation index (ODI): The average number of times per hour that the blood oxygen level drops by a specific percentage (usually 3% or 4%) from the baseline.
Clinical correlation of OSA severity and AHI metrics
Clinical relevance for the Dental Team54 -62
Understanding the AHI metrics outlined in Table 2 allows the dental practitioner to communicate effectively with sleep physicians. For example, a patient with a “mild to moderate” OSA is often an ideal candidate for a MAD (also known as a mandibular advancement appliance [MAA]), whereas those in the “severe” category may typically require continuous positive airway pressure (CPAP) as a primary intervention.
Home sleep apnoea testing (HSAT) 51
HSAT is a viable alternative for many patients, measuring airflow, respiratory effort, oxygen saturation, and heart rate using a portable device. While HSAT (Figure 3) is less accurate in mild cases or in patients with comorbidities, it is widely used and can detect moderate to severe OSA.

Dental practitioners involved in sleep apnoea therapy (e.g. providers of MADs/MAAs) typically collaborate with sleep physicians or accredited sleep laboratories for testing as part of their structured referral network.
Adjunctive specialty consultations
Referral is often necessary:
ENT consultation: 51 For suspected anatomical airway obstruction, drug-induced sleep endoscopy (DISE) can identify specific sites of collapse during sleep, informing appliance design or surgical intervention.
Sleep Physician: The Sleep Physician is the medical lead in the multidisciplinary management of sleep-disordered breathing. Sleep Physicians conduct and interpret sleep studies, such as polysomnography or home sleep apnoea tests, determine the severity of OSA, and guide treatment selection, including CPAP, oral appliance (MAD/MAA) therapy, or surgical referral. For dental practitioners involved in sleep medicine, collaboration with sleep physicians is essential to ensure proper diagnosis, treatment planning, and follow-up – particularly when initiating or adjusting MADs. Sleep physicians also manage comorbidities such as insomnia, hypersomnia or parasomnias, which may influence treatment outcome.
Nutritionists and weight management specialists:54,55 In the multidisciplinary management of OSA, addressing the adiposity–airway link is fundamental. Excess body weight is a primary modifiable risk factor, as adipose tissue deposition in the neck and tongue directly compromises upper airway patency. Nutritionists and weight management specialists provide the behavioural and metabolic framework necessary for long-term respiratory improvement. Their role includes: 1. targeted interventions for sustainable reductions in body mass index (BMI); 2. dietary counselling; 3. behaviour modification; and 4. structured weight management plans. Evidence indicates that even modest weight loss (5–15%) can lead to a significant, clinically meaningful reduction in AHI and improve response to therapies such as oral appliances. 54
Effective management of patients with TMD and coexisting sleep disorders should be individualised, evidence-based, and multidisciplinary. Conservative, reversible treatments are preferred as first-line therapy. In cases where TMD, SB, and OSA coexist, the clinical priority is usually the airway. A “vicious cycle” exists where hypoxia drives bruxism, and bruxism drives TMJ pain. Resolving the respiratory disturbance often leads to a spontaneous reduction in myogenic symptoms.
Patient education and behavioural therapy
Empowering the patient through education and behavioural modification is a cornerstone of non-invasive therapy. The below strategies are useful for addressing psychosocial factors of TMD and the environmental triggers of sleep fragmentation.
Sleep hygiene and positioning 32
Optimising the sleep environment helps stabilise the autonomic nervous system, reducing the micro-arousals that trigger jaw clenching. In this respect, patients should be advised to maintain consistent sleep schedules, minimise light/noise, and avoid stimulants (caffeine) or heavy meals in the hours preceding sleep. For patients with “positional OSA” or primary snoring, side-sleeping can prevent the tongue and soft palate from collapsing posteriorly. Special pillows or “wearable” positional devices can be used to discourage the supine position and, consequentially, reduce apnoeic episodes. A weight reduction of 5–15% is clinically proven to reduce the AHI and improve systemic metabolic health. 54
Stress management and cognitive behavioural therapy56,57
Because stress drives the sympathetic “fight or flight” response and contributes to both bruxism and TMD pain, psychological health must be addressed in tandem with physical therapy.
Techniques such as diaphragmatic breathing and progressive muscle relaxation are effective in reducing AB and myofascial tension.
Cognitive behavioural therapy (CBT) is the “gold standard” for managing chronic pain and comorbid insomnia. It helps patients reframe their perception of pain and de-escalate the “catastrophising” that often leads to TMD chronicity. For patients with severe anxiety, refractory insomnia, or complex chronic pain, referral to a behavioural sleep medicine specialist is recommended.
Beyond mechanical appliances, functional rehabilitation and targeted pharmacotherapy play a vital role in stabilising the airway and reducing masticatory muscle strain. A summary of useful therapies is shown below.
Oropharyngeal (myofunctional) therapy
Myofunctional therapy involves a structured regimen of exercises designed to strengthen the tongue, soft palate, and pharyngeal wall muscles. Exercises for the tongue and pharyngeal muscles can reduce OSA severity by improving airway tone. They are recommended for mild to moderate OSA or as adjuncts to CPAP or oral appliance therapy.
Habit reversal for awake bruxism (AB)
While SB is largely autonomic, AB is often a semi-voluntary habit driven by stress or concentration. Habit-reversal techniques aim to increase the patient’s proprioceptive awareness. This includes biofeedback or simple “jaw relaxation reminders” (e.g. visual cues or smartphone apps) to encourage a “lips together, teeth apart” resting posture.
Pharmacotherapy is often utilised as an adjunct to behavioural and mechanical therapies, specifically to address the neurochemical drivers of pain and sleep fragmentation.
Muscle relaxants
In cases of acute myogenic TMD or severe nocturnal muscle guarding, skeletal muscle relaxants can be highly effective.
Bedtime use of agents such as cyclobenzaprine act centrally to reduce motor neuron activity, thus reducing muscle tension and improving sleep quality. These should be prescribed for short-term use only (usually two to four weeks). Prolonged use is discouraged to avoid dependency and to ensure the clinician does not mask symptoms of an underlying, untreated sleep-disordered breathing condition.
Antidepressants
These are used to modulate descending inhibitory pain pathways and stabilise sleep quality.
Low-dose tricyclic antidepressants (TCAs) such as amitriptyline (at bedtime) remain a mainstay for managing chronic myogenic TMD. They facilitate sleep consolidation and provide significant analgesic effects by increasing the availability of serotonin and norepinephrine in the central nervous system. Caution is needed in patients with confirmed or suspected OSA. Selective serotonin reuptake inhibitors (SSRIs) may worsen bruxism and are not usually beneficial for TMD pain. TCAs can reduce the muscle tone of the upper airway dilators and potentially lower the arousal threshold, which may exacerbate the frequency and duration of nocturnal hypoxic events.
SSRIs such as fluoxetine and sertraline are commonly prescribed for anxiety and depression. SSRIs are generally not beneficial for direct TMD pain management. Furthermore, they are well-documented to induce or worsen SB via “serotonin-induced” stimulation of the jaw-closing motor neurons, a phenomenon known as SSRI-induced bruxism.
Gastroesophageal reflux disease (GERD) and the “acid-arousal” link 59
The presence of GERD adds a layer of complexity to the TMD–sleep interface, often acting as a chemical trigger for nocturnal motor activity. In clinical practice, this is increasingly recognised as the “triple threat”: the co-occurrence of GERD, OSA, and SB.
The acid-arousal reflex: Nocturnal gastric acid refluxing into the oesophagus can trigger a protective “acid-arousal” response. This micro-arousal often stimulates RMMA as the body attempts to increase salivary flow – which is rich in bicarbonate to neutralise the acid (pH<4.0).
Synergy with OSA: The negative intrathoracic pressure generated during an apnoeic event can literally “pull” gastric contents into the oesophagus, making OSA a significant risk factor for nocturnal GERD.
Musculoskeletal impact: The systemic inflammatory state and frequent sleep fragmentation associated with GERD can lower pain thresholds, contributing to the chronicity of myogenic TMD symptoms.
Pharmacological adjuncts for OSA
Pharmacotherapy remains a secondary or adjunctive strategy rather than a primary treatment for the mechanical obstruction seen in OSA. For the dental practitioner, understanding these medications is vital for managing patients who are “partially responsive” to MADs. Nasal decongestants or intranasal corticosteroids (e.g. fluticasone) are frequently utilised to reduce nasal resistance. Improving the “nasal valve” function can lower the pressure required for CPAP and improve the efficacy of oral appliances by discouraging mouth breathing. In cases of residual excessive daytime sleepiness (REDS) – where the AHI is controlled but the patient remains fatigued – specialists may prescribe agents like modafinil or solriamfetol. It is critical to note that while a dental practitioner may recommend over-the-counter nasal aids, the prescription of wakefulness agents is strictly under the purview of a Sleep Physician or Neurologist.
Oral appliances and occlusal therapy60 -65
Oral appliances are central in managing TMD, bruxism, and OSA but must be selected carefully to avoid exacerbating coexisting conditions.
Stabilisation splints (Michigan/Tanner appliances)
Hard acrylic stabilisation splints protect teeth against tooth wear and reduce muscle activity and bruxism in TMD patients. While effective for many, traditional flat-plane splints may occasionally worsen OSA in susceptible individuals by increasing the vertical dimension without advancing the mandible. 64 They should be used cautiously in OSA patients; 65 an appliance design that maintains or slightly advances the mandibular position is preferable.
Mandibular advancement devices (MADs)
These custom-fabricated appliances (Figure 4) protrude the lower jaw, increasing posterior airway space and reducing OSA severity. By mechanically protruding the mandible, these devices also exert tension on the palatoglossus and other pharyngeal dilator muscles, effectively increasing the cross-sectional area of the upper airway and reducing soft-tissue collapse during sleep. They are effective in mild to moderate OSA and offer better patient compliance than CPAP. While short-term side effects (jaw discomfort, bite changes) are common, most resolve over time.
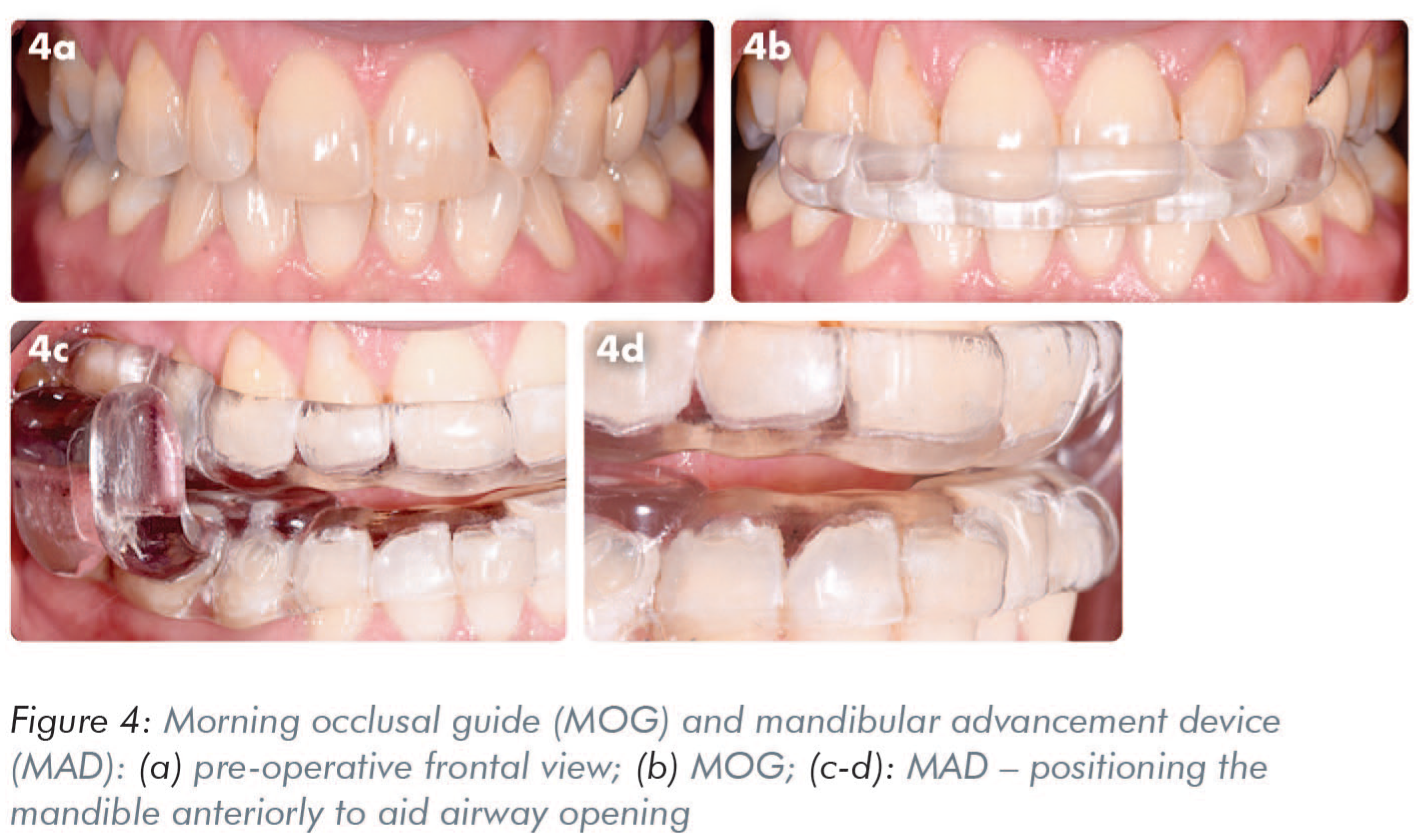
A morning occlusal guide (MOG) is a custom appliance fabricated in maximum intercuspation and worn briefly after removal of a MAD. Its purpose is to facilitate bite repositioning and help the patient return to their natural occlusion, reducing the risk of prolonged occlusal changes or discomfort. In patients with active TMD, stabilisation before MAD use may be helpful. Long-term monitoring of the TMJs, masticatory muscle health, and occlusal stability is paramount to ensure the airway benefits are not outweighed by musculoskeletal complications.
Combination therapy
In complex clinical cases where a single modality fails to achieve therapeutic goals, combination therapy offers a highly effective, multifaceted approach. By integrating dental and medical interventions, clinicians can optimise both respiratory outcomes and musculoskeletal protection. Patients with severe OSA and comorbid SB often require a dual-device approach, such as CPAP and a thin, hard-acrylic stabilisation splint which protects the dentition and restorations from the high-force loading of nocturnal grinding. 58 Coordination between providers is key to prevent appliance–mask interference.
Anterior bite planes (ABPs)
Also known as nociceptive trigeminal inhibition tension suppression system (NTI-tss) or “deprogrammers”, ABPs are small appliances that cover only the maxillary or mandibular anterior teeth, preventing the posterior teeth from occluding. While they serve a specific purpose in acute TMD management, they carry significant risks in the context of sleep-disordered breathing. They are best used only in the short-term. ABPs are strictly cautioned or contraindicated in patients with a high risk of OSA.
Orthodontic and surgical interventions67,68
For patients with underlying skeletal discrepancies (e.g. narrow palate, retrusive jaw), mechanical or functional orthodontic appliances may only provide symptomatic relief. The standard of care for these cases commonly involves combined intervention through definitive orthodontic or surgical means. Orthodontic expansion or orthognathic interventions may improve airway patency and air flow, and TMJ alignment. These should be coordinated within a multidisciplinary team.
Surgical options
For OSA, upper airway surgeries (e.g. septoplasty, tonsillectomy) may be considered based on the site of obstruction. Maxillomandibular advancement (MMA) surgery is highly effective for severe OSA and can simultaneously alleviate TMD in some cases. These procedures require careful case selection and interdisciplinary collaboration.
Monitoring and follow-up
Regular follow-up is critical. For TMD, reassess pain, appliance comfort, and functional changes. For OSA patients using oral appliances, follow-up sleep studies may be needed to confirm therapeutic benefit. Patient education should reinforce compliance and prompt reporting of any new or worsening symptoms. Long-term management should adapt to changes in weight, sleep quality, and TMJ condition. Evaluation of the oral appliance for structural integrity, loss of retention, or heavy wear facets is also important as these might indicate persistent high-force bruxism.
Conclusion
TMDs and sleep-related conditions such as OSA and SB are closely intertwined in clinical practice. Addressing this interplay is essential for effective management. For instance, jaw pain may persist if underlying sleep disturbances go unrecognised, while treating sleep apnoea without considering TMJ health may exacerbate TMD symptoms. This interconnection highlights the importance of a holistic, interdisciplinary approach. By integrating dental and sleep medicine perspectives, clinicians can optimise both oral health and overall well-being. This narrative review synthesises the current evidence into practical recommendations, but continued learning is vital as research into the TMD–sleep relationship evolves. Emerging therapies such as gene-based approaches for bruxism and neuromodulation for OSA may further refine treatment. In the meantime, applying evidence-based, collaborative care principles will help ensure safe and effective outcomes for patients with overlapping TMD and sleep disorders.