
Abstract
The temporomandibular joint (TMJ) is a uniquely complex, bi-articular joint that enables both rotational and translational mandibular movement. Joint sounds, such as clicking and crepitation, are among the most common clinical findings associated with temporomandibular disorders (TMDs) and frequently cause patient concern. Understanding the underlying anatomy of the TMJ, its fibrocartilaginous surfaces, articular disc morphology, and complex muscular attachments is essential to diagnosing the origin of these joint sounds. This article outlines the anatomy and clinical relevance of the TMJ to help clinicians adopt a conservative, evidence-based approach to the assessment of joint sounds, recognising that most are benign and self-limiting, while ensuring accurate diagnosis of sounds suggestive of internal derangement or degenerative change.
Keywords
Learning Objectives
To describe the key anatomical structures of the temporomandibular joint (TMJ)
To differentiate between common types of TMJ sounds and understand their underlying anatomical and biomechanical causes
To recognise the clinical significance of TMJ sounds and distinguish benign joint noises from those associated with internal derangement or degenerative joint disease
Introduction
The temporomandibular joint (TMJ) is a multi-functional joint which allows articulation of the mandible with the cranial bones. In dentistry we encounter symptoms and issues relating to its supporting structures, the most common of which is joint sounds such as “clicking” and “crepitation”.
TMJ anatomy
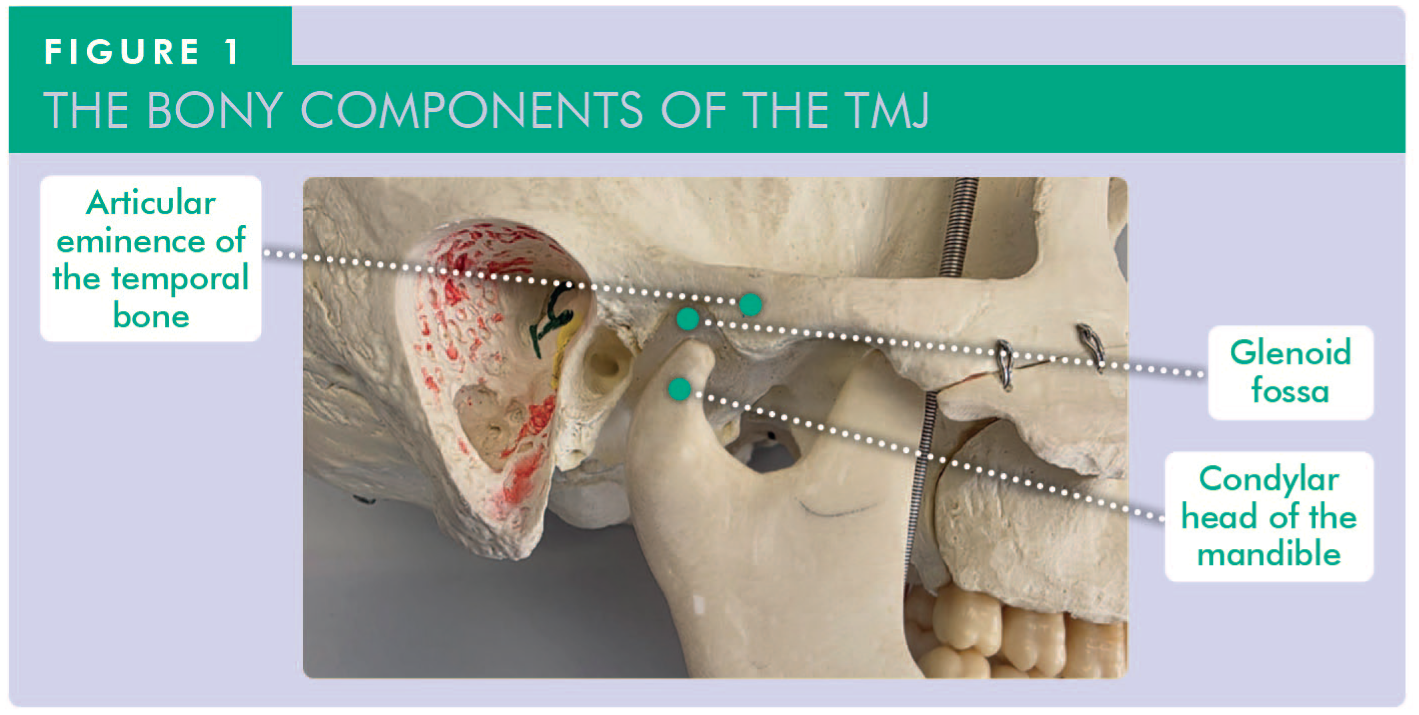
To understand patients’ symptoms and correctly diagnose their issues, it is essential to understand the anatomy of the TMJ. The bony components of the TMJ are comprised of the glenoid fossa and articular eminence of the temporal bone, and the condylar head of the mandible (Figure 1).
Translational and rotational movements occur at the TMJ. Uniquely, each movement is affected by the contralateral TMJ as the mandible is bi-articular making it distinctive among joints of the body as mandibular movements occur simultaneously in two joints. Additionally, the bony components articulate indirectly with each other via an intermediary articular disc made of fibrocartilage. The bony articular elements are also unique as they are also covered by fibrocartilage rather than hyaline cartilage. 1 The movements of the mandible at the TMJ are essential for swallowing, mastication and speech.
The articular disc is concave posteriorly and convex anteriorly; the concave section covers the condylar head. The anterior extension of the articular disc attaches superiorly to the articular eminence of temporal bone and inferiorly to the anterior margin of the condyle. 2 Medially and laterally the disc attaches to the joint capsule and the poles of the condylar head. There are two attachment points of the posterior extension of the disc, a superior and inferior. The superior attachments are the posterior wall of the glenoid fossa and squamotympanic suture, the inferior attachment is the neck of the mandibular condyle posteriorly.
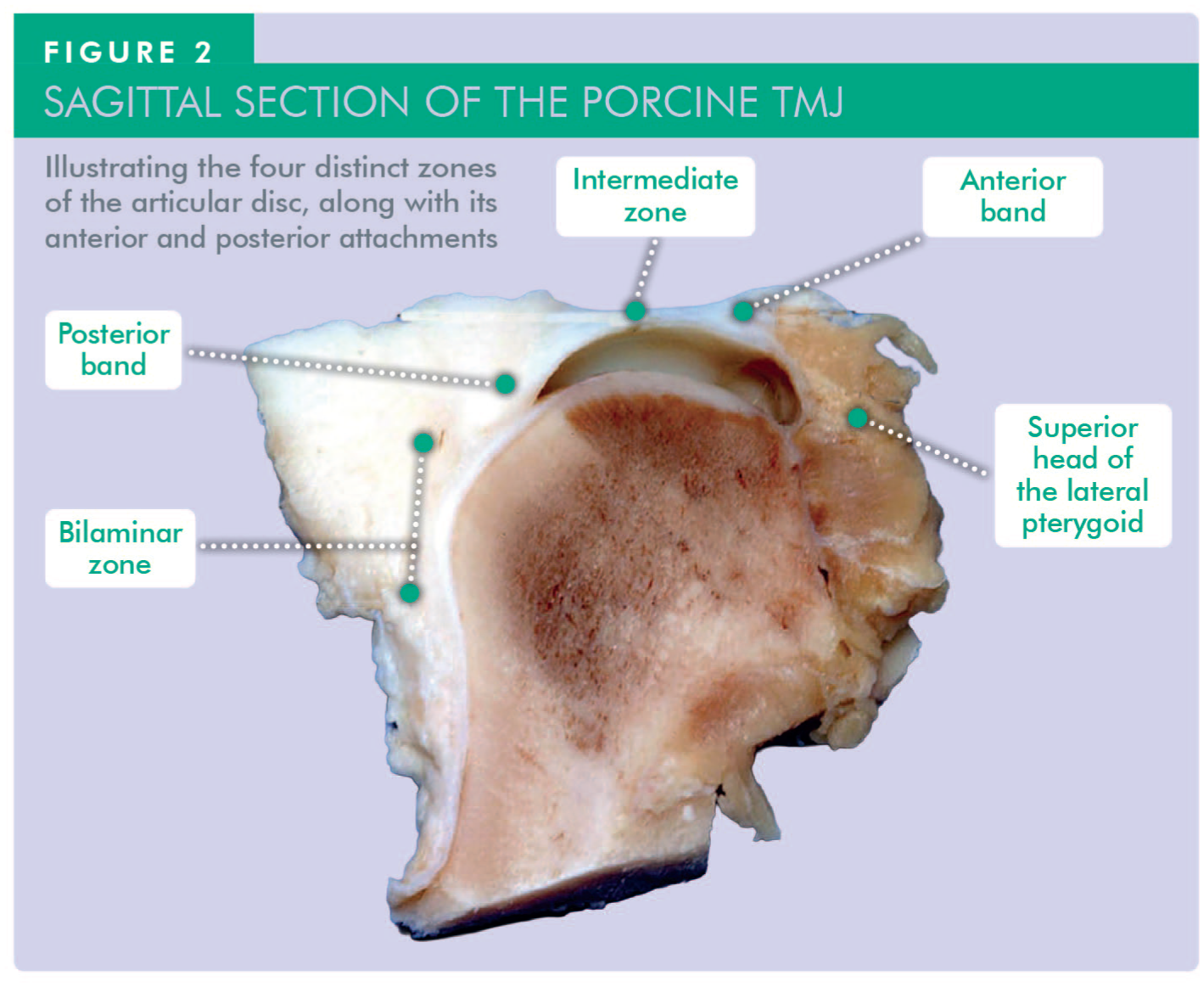
There are four clear transverse ellipsoidal zones of the disc: the anterior band, the intermediate zone, the posterior band, and the bilaminar zone. 3 The anterior band is moderately thick yet narrows anteroposteriorly. The intermediate zone, which is both narrow and the thinnest of the transverse zones, sits between the anterior and posterior bands. The posterior band is the thickest and widest zone of the disc, anteroposteriorly. Finally, the bilaminar zone has two layers of different composition: the upper layer (or stratum) is elastic and attaches to the posterior wall of the glenoid fossa and squamotympanic suture; the lower stratum is fibrous and attaches to the neck of the mandibular condyle posteriorly. 3 When the mandible is in the resting (postural) position, the posterior zone separates the two bony elements of the TMJ. As the condyle translates anteriorly onto the articular eminence, the intermediate zone and then anterior band separate the bony elements. The anterior extension of the articular disc appears to show direct attachment of muscle fibres from the superior head of the lateral pterygoid in studies; however, this remains debated 4 (Figure 2).
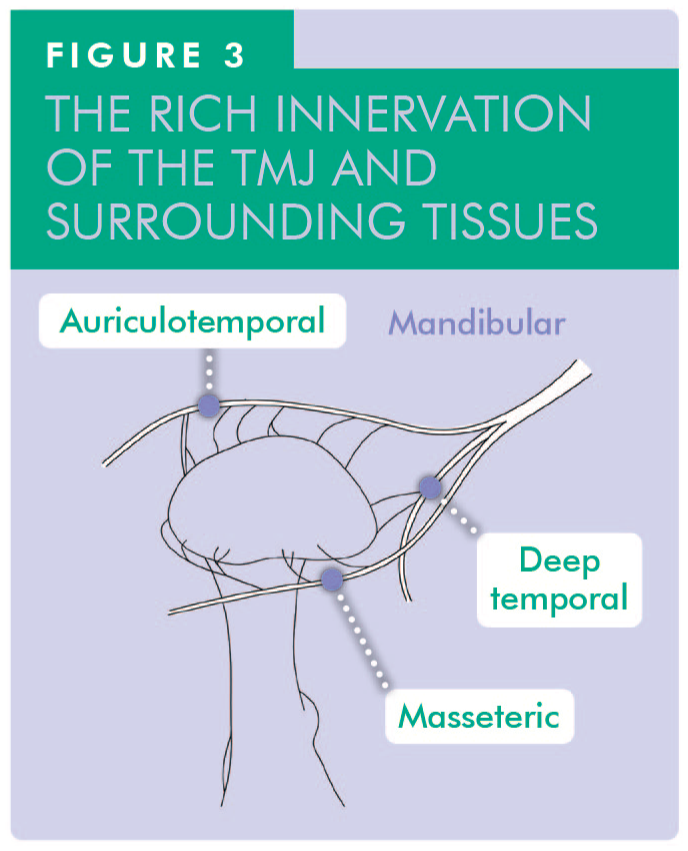
There is no direct innervation of the articular disc itself, but there is rich innervation of the surrounding joint capsule. This is derived from the auriculotemporal branch of the mandibular division (V3) of the trigeminal nerve. This nerve wraps around the capsule anterolaterally starting from the posterior medial aspect of the condylar head and gives off small branches into the joint capsule. The masseteric and posterior deep temporal nerves are also involved in additional innervation of the joint capsule especially the anteromedial aspect of the capsule as seen in some papers, though there is variation present between individuals (Figure 3). 5
Understanding the mechanism behind joint sounds
TMJ sounds are common clinical observations that often alarm patients. While these joint sounds are not always pathological, they may indicate an underlying functional disturbance within the joint complex.
What causes the “click”?
The most common cause of TMJ clicking is disc displacement with reduction (DDwR).
The disc is normally pulled forwards by the superior head of the lateral pterygoid muscle, and the posterior attachment to the squamotympanic fissure, which is elastic. This allows stretching of the posterior portion of the disc; thereby allowing it to remain interposed between the two bony components of the joint at all phases of movement. During closure of the mouth, the reverse process occurs and the elastic recoil of the posterior part of the bilaminar zone of the disc helps to pull it back into place.
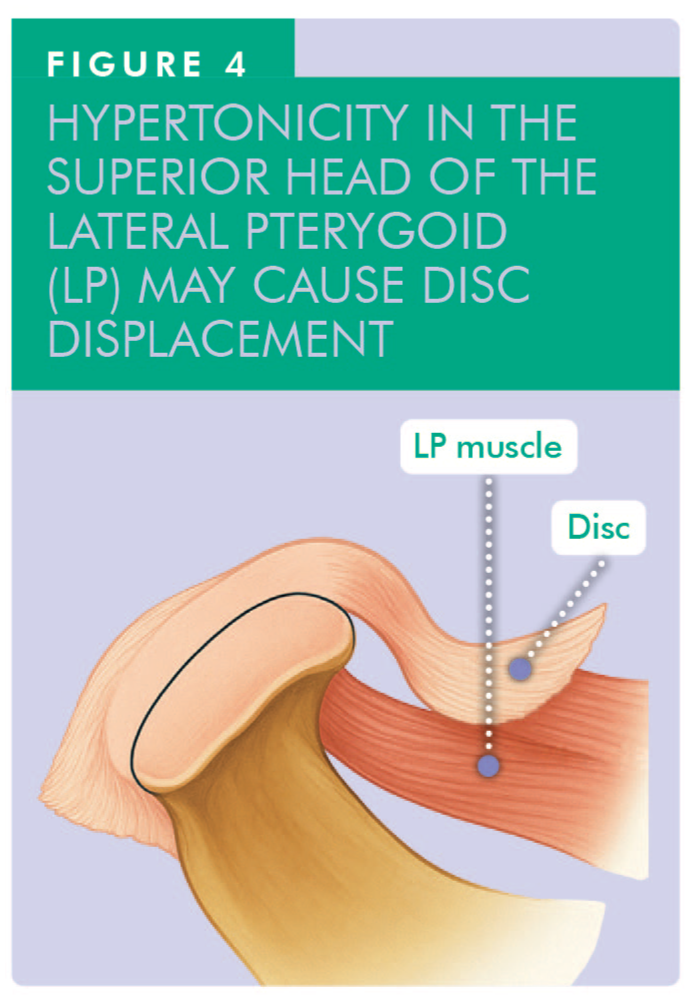
If the joint is overloaded in any way, there is a tendency for an increased tonicity in the lateral pterygoid muscle, and this tends to pull the disc forwards. This muscle overactivity may stem from habits such as clenching or grinding (Figure 4). 6
An early- or mid-opening cycle click is commonly caused by disc displacement. If the intra-articular disc is displaced, then the patient can usually open to 15−20mm without causing a click. This is a consistent range of measurement due to the rotational condylar movement but as the translation phase starts, the head of the condyle slides forwards and encounters the disc in the displaced position and it impacts against the thicker posterior band of the disc. Friction is then built up until the head of the condyle “jumps past” this portion of the disc which causes an audible release of energy, which is the click sound. 2
The closing click tends to be softer than the opening click, as it is more of a passive movement when the disc repositions.
Another explanation for a late-opening click could be subluxation, when the disc is not displaced at the commencement of mouth opening, but the click occurs because of the condylar head moving considerably further than the disc and thereby attaining a displaced position.
Different proposed mechanisms involve disrupted synovial fluid dynamics. Abnormal disc–condyle alignment may trap synovial fluid, creating pressure that is released audibly when movement restores normal flow.7,8
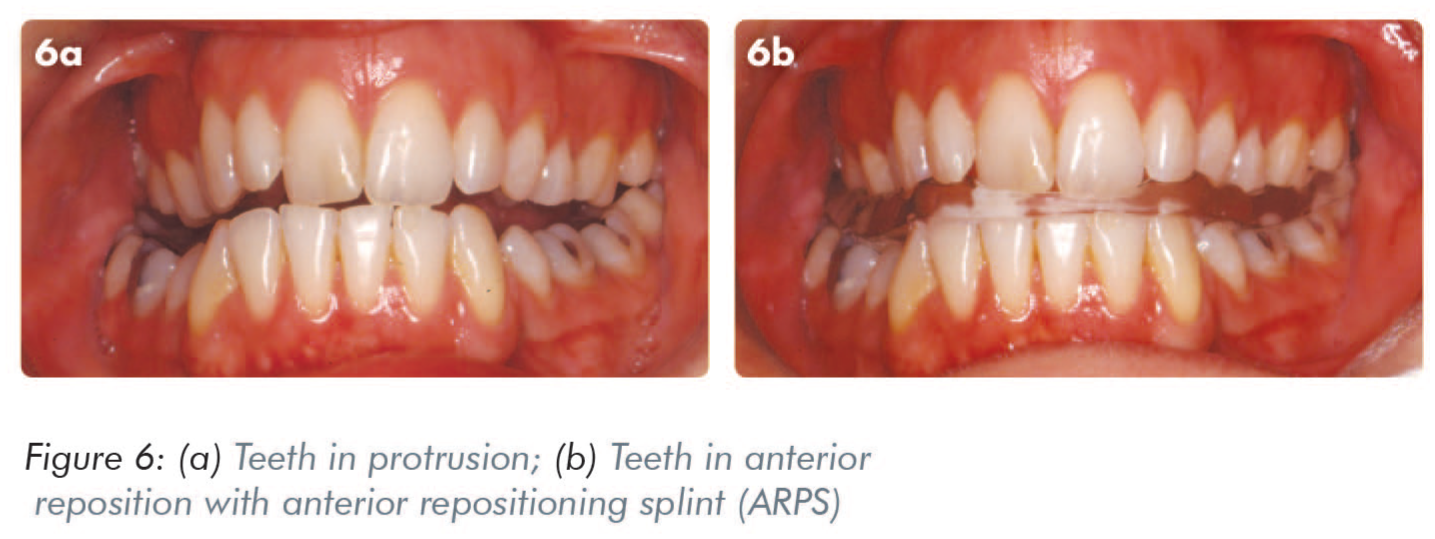
Interestingly, this clicking often disappears when the mandible is postured forward, such as when using an Anterior Repositioning Splint (ARPS). This forward shift re-establishes disc-condyle congruence and normalises joint mechanics.
When do TMJs click?
It is important for the clinician to be aware of this and differentiate between a true internal derangement and a click associated with facial arthromyalgia, as the treatment will vary between the two diagnoses – treatment that might be applicable for one would have little chance of success with the other. 2
Clicking associated with myofascial pain
Parafunctional habits, especially nocturnal bruxism, can elevate muscle tone in the superior pterygoid muscle during Rapid Eye Movement (REM) sleep, drawing the disc anteriorly. On waking, the disc may remain displaced, and clicking often occurs with the first few jaw movements. As muscle tension subsides through the day, the disc may reposition and return to its normal anatomical and functional position, owing to the elastic pull of the posterior part of the disc, and the clicking typically fades as the day goes on. However, it can recur during periods of high function and increased muscle tension, such as chewing. 8
Disc displacement with reduction (DDwR)
This presentation is typified by a consistent, usually painless click during both opening and closing movements, a pattern referred to as “reciprocal clicking”. The opening click tends to be louder due to the active force required to reposition the disc, while the closing click is softer and more passive in nature.
It is important to differentiate between the two types of clicks based on the patient’s history as this will directly affect the treatment plan.
Characteristics of TMJ clicks
Note should be made of whether the click is painful or painless, single or multiple, and early or late in the opening/closing cycle.7 -9
Early clicks (at the start of opening) often reflect mild disc displacement.
Late clicks (near maximum opening) may indicate more advanced displacement or even subluxation, where the condyle overshoots the disc.
Multiple clicks during one movement cycle can point to disc instability or, more rarely, disc perforation.
Persistent clicking throughout the day is more consistent with internal derangement and may warrant further clinical investigation.
Jaw deviation and TMJ clicks
Jaw deviation during opening is often caused by unilateral disc displacement. As the condyle on the affected side meets resistance from the displaced disc, the mandible may deviate laterally to overcome the obstruction. Once the disc is recaptured, the jaw usually returns to the midline.
Clinical assessment
Initial evaluation of TMJ clicking includes:
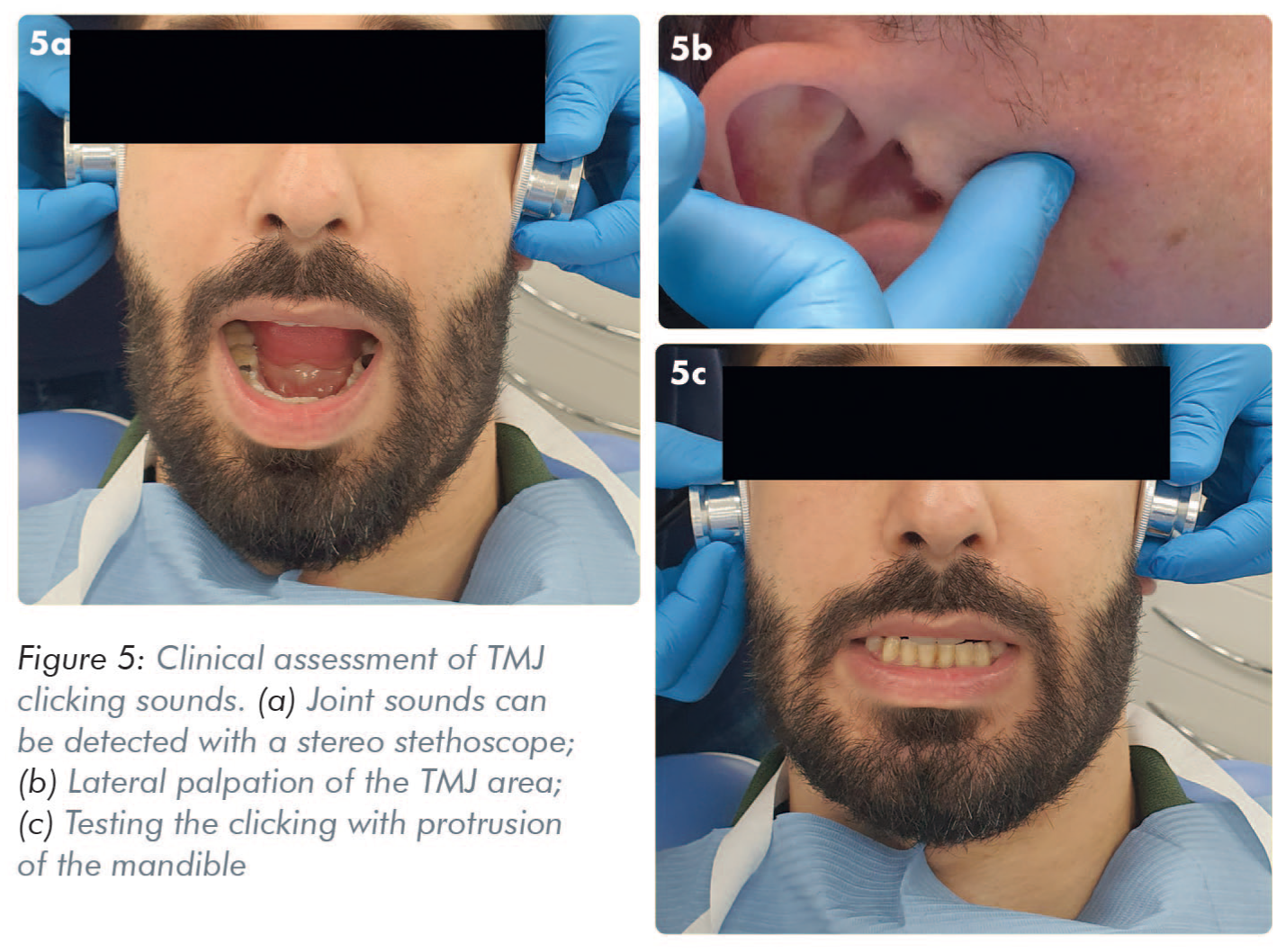
Auscultation with a stethoscope or listening tube (Figure 5a)
Palpation around the joint area (Figure 5b). The lateral aspect of the TMJ is palpated by pressing gently over the immediate preauricular area, both at rest and during mandibular motion (opening, closing, protrusion, and lateral excursions)
Mandibular protrusion tests, to assess how altering jaw position affects the clicking (Figure 5c)
These non-invasive techniques often provide enough information for diagnosis and management planning.
Does a TMJ click require treatment?
A TMJ click does not always require treatment. Many patients with clicking TMJs do not need intervention, particularly if the sound is painless and does not impair function. If a patient presents with a painless click that is completely symptom free, there is no pain and there never has been any experience of locking, there may be no need to treat the condition. Periodic clinical monitoring, however, is advisable to ensure the condition remains stable and does not progress. 2
When not to treat
Conservative clinical monitoring is appropriate if the patient:
experiences a painless, intermittent click
has no history of jaw locking
maintains full range of motion
is not socially affected by the sound
When to treat
Intervention is warranted if:
the click is painful
locking occurs
the noise causes embarrassment or social concern
In these cases, an ARPS is often the treatment of choice.
Anterior repositioning splints (ARPS): mechanism and protocol
The chairside test involves asking the patient initially to open their mouth, protrude the lower jaw and then close their mouth (Figure 5c). On subsequent opening and closing movements, the patient is asked to keep the mandible forwards with the incisors in an edge-to-edge relationship and the “click” should disappear. 9 In some patients (e.g. those with a Class II skeletal relationship and/or a Class II division 1 occlusal relationship) it may not be necessary to attain an edge-to-edge occlusal position. If the click is heard on a protrusive mandibular movement, record this position as the one to work to. If protrusion eliminates the click, this is indicative that an ARPS would have a high chance of success. When the patient postures forwards onto their incisor teeth the head of the condyle projects downwards and forwards so that the displaced disc assumes a more normal “functional” relationship to the head of the condyle. Opening and closing from this position without causing the click thereby eliminates trauma to the disc and the natural elasticity of the posterior part of the disc gradually repositions it.10 -12
An ARPS works by posturing the mandible forwards, allowing the disc to realign with the condyle and eliminating mechanical interference (Figure 6).
Testing for suitability
Ask the patient to:
Open fully, protrude the jaw, then close.
Repeat opening and closing in this protruded position.
If the click disappears, the patient is likely to respond well to ARPS therapy. In Class II division 1 patients, even a slight protrusion may be effective.
Treatment protocol
The patient should wear the splint 24 hours/day for around 12 weeks. The splint may be worn continuously, including during eating, unless otherwise advised by the clinician. A soft diet is recommended during the first few weeks of splint therapy to minimise discomfort and allow adaptation.
Follow with a gradual weaning period.
After splint withdrawal, the mandible returns to its normal occlusion.
If successful, the disc remains in place and the click resolves.13 -16
ARPS therapy has a success rate of approximately 85% in cases where clicking occurs during vertical opening. 17 Clicking during lateral jaw movements is more difficult to treat and less responsive to this approach.17 -22
Crepitation
The other, less commonly encountered joint sound is crepitation (or crepitus), which is a crunching or grating sound. It is usually indicative of degenerative joint disease, such as osteoarthrosis, psoriatic arthritis or rheumatoid arthritis (RA). The clinician should be aware that RA rarely, if ever, presents in the TMJ as being the first joint affected and the patient would normally have a pre-existing history of RA in other joints.
When associated with osteoarthrosis, crepitus may be present with or without pain. It is indicative of degeneration of the joint surfaces, either of the condyle, of the fossa or of the intra-articular disc itself. It may indicate surface friction due to lack of synovial fluid or high viscosity because of pressure applied by abnormal activity.
Radiographic findings may or may not be present (Figure 7). 22
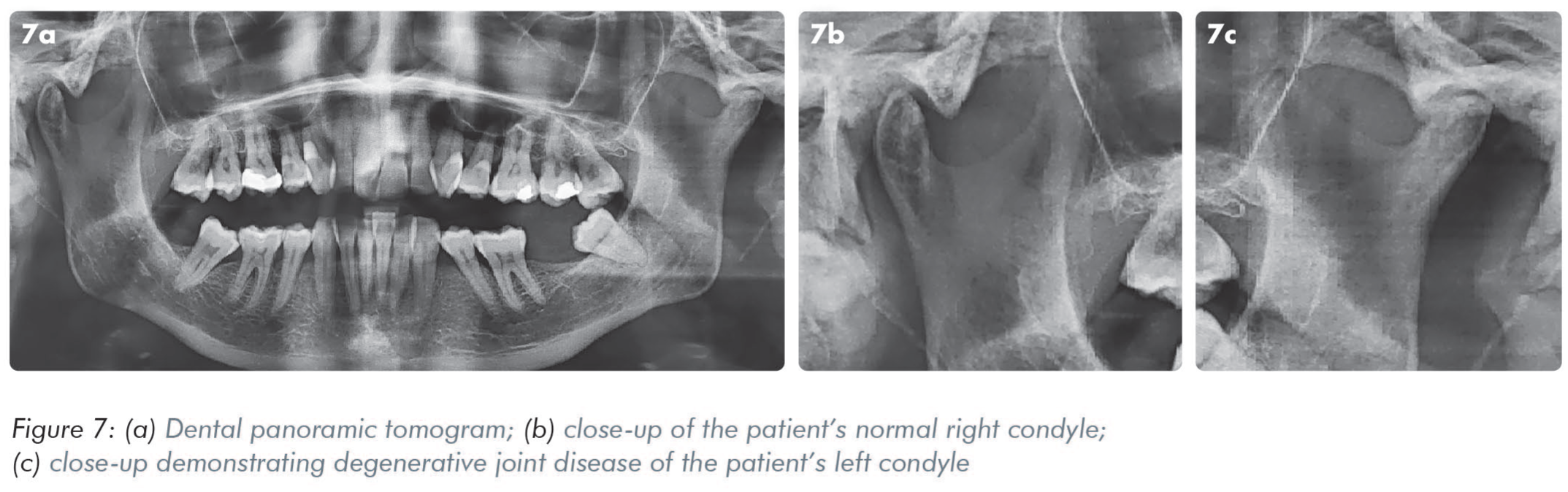
The joint sound of crepitation is managed in a different way to clicking joint sounds. When a patient presents with recently-developed crepitation, the chances are that it will persist for a period of up to 9−12 months. The TMJ, however, does retain the capacity to repair and remodel throughout life. The undifferentiated germinative mesenchyme cell layer can be stimulated by irritation. The direct effect of this, in response to degenerative joint disease, is for the head of the condyle to reshape, remodel and resurface. This reparative cycle can take anything from 18 months to three years to occur. Occlusal splints may help in avoiding continuous pressure on articular surfaces made by bruxism, allowing synovial membrane to secrete enough quantity with appropriate quality of synovial fluid.23 -26
Conclusion
TMJ clicking is often a benign and self-limiting symptom. However, persistent, painful or functionally disruptive clicking, especially in the context of DDwR, may require targeted treatment. Anterior repositioning splints remain a valuable tool in managing these cases. Accurate assessment of the click’s timing, quality, and associated symptoms is essential for effective diagnosis and treatment planning.
Crepitation in the TMJ is a less common but significant clinical finding, often associated with degenerative joint conditions such as osteoarthrosis, psoriatic arthritis or RA. While not always accompanied by pain or radiographic changes, crepitus typically signals joint surface deterioration. Importantly, the TMJ retains a remarkable capacity for repair through remodelling of the condyle and surrounding structures.
Clinicians should adopt a patient and supportive approach, recognising the potential for natural joint adaptation and improvement over time.