
Abstract
Objective:
The Joint Committee of Surgical Training guidelines for the award of a Certificate of Completion of Training in urology were updated in 2015. In 2015, we published operative logbook data from Certificate of Completion of Training in urology applications in 2010–2012 in line with the original 2011 guidelines. This study reviewed a contemporary cohort against the 2015 guidelines and this previous cohort to evaluate whether the number of trainees achieving these requirements had changed.
Materials and methods:
All Certificate of Completion of Training in Urology application logbooks from March 2014–October 2015 (77 in total, 2015 cohort) were reviewed and compared to 154 logbooks in 2010–2012 (2012 cohort).
Results:
There was a significant increase (p<0.05) in the percentage of trainees achieving indicative exposure in 10 domains in the 2015 cohort according to the updated guidelines. Percentage increases included male lower urinary tract symptoms procedures from 68.2% to 88.3%, transurethral resection of bladder tumour from 64.3% to 89.6%, paediatric urology from 1.9% to 23.4%, female incontinence from 9.7% to 33.8% and andrology from 9.1% to 42.9%. There were significant reductions (p<0.01) in mean operative numbers for transurethral resection of bladder tumour and male lower urinary tract symptoms procedures from 184 to 162 and 187 to 161, respectively. One trainee in the 2015 cohort achieved requirements in all 17 domains and 55% failed to meet the requirement in ⩾5 domains.
Conclusions:
While an increasing number of trainees currently meet Joint Committee of Surgical Training expectations, some domains remain at low levels. Despite this, no trainee to date has not been awarded a Certificate of Completion of Training as a direct consequence of this, but this could become a possibility in the near future, and it is the responsibility of Local Education Training Boards and trainees to ensure that indicative numbers are both achievable and achieved.
Keywords
Introduction
In July 2015, the Joint Committee on Surgical Training (JCST) and the Specialty Advisory Committee (SAC) in urology issued updated guidelines for the award of a Certificate of Completion of Training (CCT) in urology. The previous iteration of the guidelines, published in 2011, included a list of operative procedures for which higher surgical trainees (ST3+) in urology were expected to achieve a minimum exposure, termed the indicative number. We have previously published data on a cohort of UK and Irish trainees from 2010–2012, 1 which demonstrated significant variance from the JCST expectations with >75% achieving indicative numbers in five domains according to the 2011 guidelines, increasing to >80% in eight domains using the 2015 guidelines. The 2015 guidelines reduced the expected operative exposure in the domains of transurethral resection of bladder tumour (TURBT), procedures for male lower urinary tract symptoms (LUTS), nephrectomy, cystectomy, female incontinence and paediatric urology. There was an increase in the expected number of flexible cystoscopies from 200 to 300 and changes in the expected competency from level 3 to 4 for ureteroscopy, and from level 3 down to 2 for nephrectomy. The 2015 guidelines also stratified inguinoscrotal surgery into scrotal procedures, inguinal orchidectomy and adult circumcision, resulting in an increase from 15 to 17 operative domains for which indicative numbers apply. Full details are shown in Table 1.
Expected levels of competency in procedures in 2011 and 2015 according to the Joint Committee on Surgical Training (JCST) guidelines.
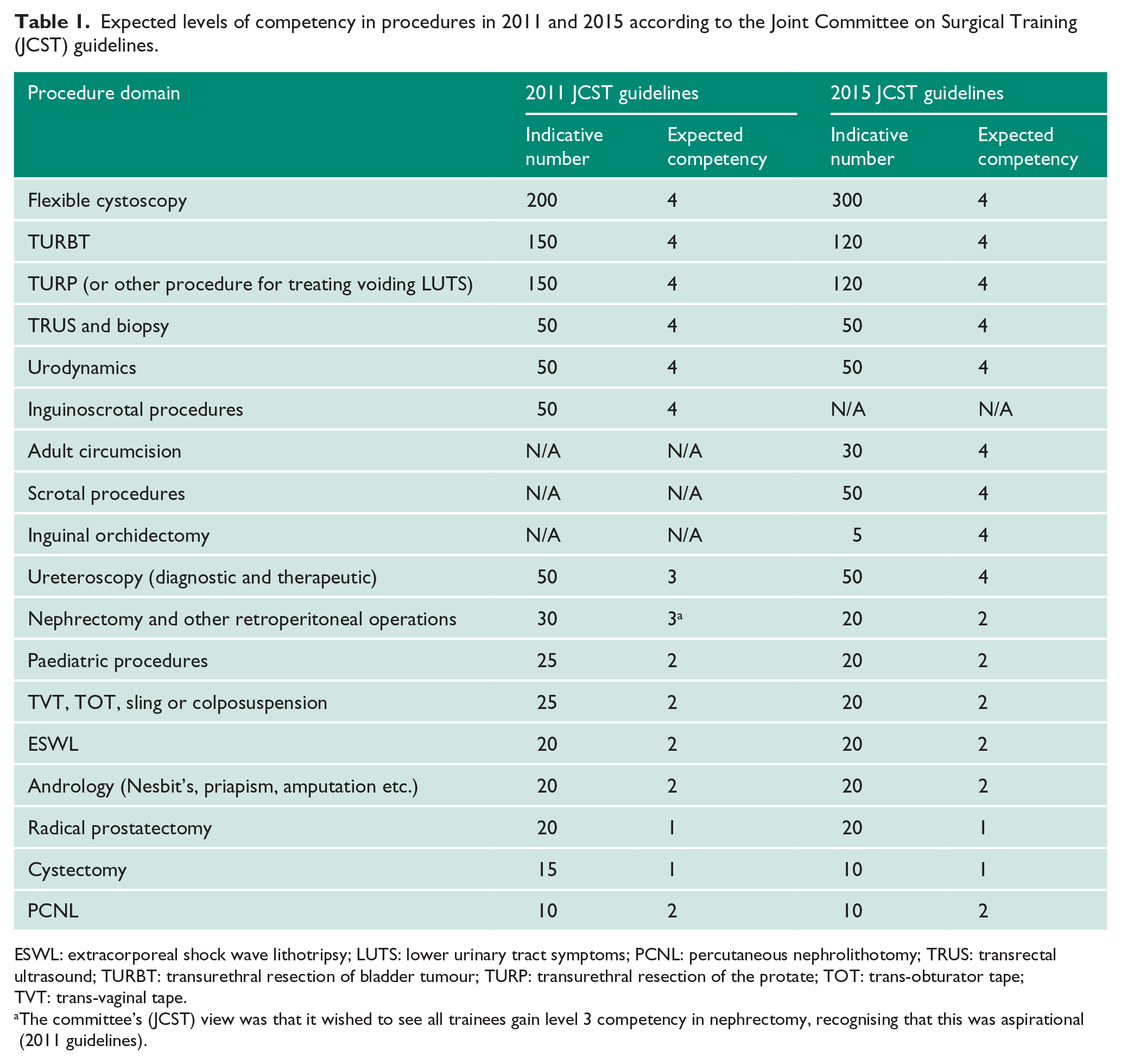
ESWL: extracorporeal shock wave lithotripsy; LUTS: lower urinary tract symptoms; PCNL: percutaneous nephrolithotomy; TRUS: transrectal ultrasound; TURBT: transurethral resection of bladder tumour; TURP: transurethral resection of the protate; TOT: trans-obturator tape; TVT: trans-vaginal tape.
The committee’s (JCST) view was that it wished to see all trainees gain level 3 competency in nephrectomy, recognising that this was aspirational (2011 guidelines).
Current trainees are highly cognisant of the JCST requirements on indicative numbers, as the introduction coincided with their commencement on the specialist training programme, and the guidelines have formed part of their annual review of competence progression (ARCP). This would not have been the case for the previous cohort of trainees, who were coming to the end of their training when indicative numbers were introduced. For the current cohort of trainees, there is an expectation to achieve the requirements of the JCST. This study aimed to review the operative exposure of a contemporary cohort of trainees against the current JCST guidelines, and to compare the exposure of the previous cohort to establish whether the number of trainees achieving these requirements had changed, and if they were not being achieved where the deficits exist.
This information should be of interest to current trainees, in order to assess how they compare nationally, and to consultant urologists to help support their trainees fulfil these requirements. It will also inform the SAC where current trainees stand in meeting the requirements, guide future review of indicative numbers, areas where changes need to be made to the curriculum and how it is delivered.
Methods
All logbooks submitted to the SAC in urology to support applications for a CCT in urology between March 2014–October 2015 were obtained (the 2015 cohort). Using a standardised proforma, data was extracted on operative exposure during training in the operative domains defined from both the 2011 and 2015 JCST guidelines. All operative exposure in each domain was combined to give total operative exposure, irrespective of the degree of consultant supervision. Identification of paediatric procedures, other than where a separate paediatric logbook was submitted, was problematic. In an attempt to overcome this, a pragmatic decision was made to include ligation of patent processus vaginalis, orchidopexy (other than for twisted spermatic cord) and hypospadias surgery as paediatric procedures for those trainees who did not submit separate logbooks. Procedures observed by the trainee, or where the level of supervision was undefined, were excluded.
Operative exposure in the 2015 cohort was then compared to that achieved by the previously published cohort of 154 trainees 1 (the 2012 cohort). Total operative exposure for each comparable domain was compared between cohorts using a Mann-Whitney U test and the proportion of trainees meeting the JCST minimum requirements for each domain was compared using Fisher’s exact test. Statistical analysis was performed using Graph Pad Prism (La Jolla, California, USA) and significance was set at p<0.05.
Results
Logbook data on 77 trainees was available covering a period of 20 months, from March 2014–October 2015. Only 10 (12.9%) of the 2015 cohort submitted a separate logbook for paediatric procedures, of which nine met the minimum requirement of 20 procedures. When comparing the two cohorts, there was a significant increase in operative exposure (p<0.05) for flexible cystoscopy, transrectal ultrasound (TRUS) and biopsy, inguinoscrotal procedures, ureteroscopy, nephrectomy, extracorporeal shock wave lithotripsy (ESWL), female incontinence surgery, paediatric procedures and andrology (Table 2). This was contrasted by a significant reduction (p<0.05) in mean exposure to male LUTS procedures from 187 (range 67–486) to 161 (range 102–266) and TURBT from 184 (range 16–512) to 162 (range 67–311). There were no significant changes in mean exposure for cystectomy, radical prostatectomy or percutaneous nephrolithotomy (PCNL).
Comparison of the two cohorts operative exposure and achievement of the Joint Committee of Surgical Training (JCST) guidelines on indicative numbers.
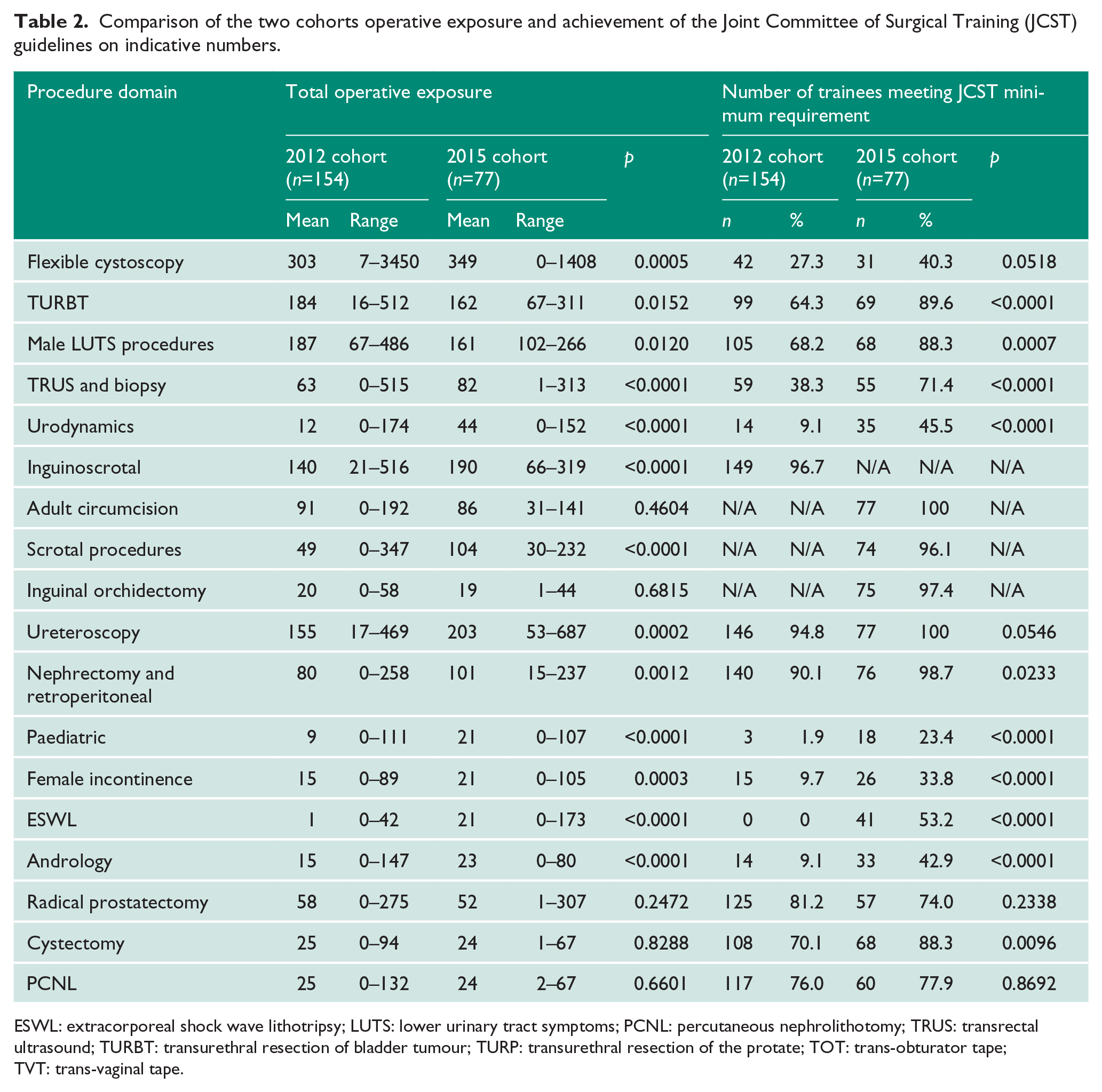
ESWL: extracorporeal shock wave lithotripsy; LUTS: lower urinary tract symptoms; PCNL: percutaneous nephrolithotomy; TRUS: transrectal ultrasound; TURBT: transurethral resection of bladder tumour; TURP: transurethral resection of the protate; TOT: trans-obturator tape; TVT: trans-vaginal tape.
Despite the reduction in exposure to male LUTS procedures and TURBT, the proportion of trainees meeting the minimum indicative number increased significantly from 68.2% to 88.3% for male LUTS procedures and 64.3% to 89.6% for TURBT. However, this was due to the lowering of the indicative numbers for both procedures by 20% from 150 to 120, as similar numbers would have achieved the indicative numbers using the 2011 guidelines at 62.3% and 67.5% respectively. There was no significant change in the proportions for PCNL or radical prostatectomy.
Significant improvements in the proportion of trainees meeting expectations were seen in all other comparable domains with absolute increases of 18.2% for cystectomy, 24.1% female incontinence procedures, 33.1% TRUS and biopsy, 33.8% andrology, 36.4% urodynamics, 53.2% ESWL and 21.5% paediatric procedures. For TRUS and biopsy, andrology, urodynamics and ESWL this reflected a genuine improvement (p<0.0001), as there were no changes to indicative numbers. For the four other domains where there was a reduction in indicative numbers (paediatric procedures, female incontinence, cystectomy and nephrectomy) more trainees in the 2015 cohort achieved these even with the original guidelines, therefore the increase in trainees meeting the requirements was not due to a lowering of standards.
Despite these increases, the overall proportion of trainees reaching the minimum requirement in the 2015 cohort remained below 75% for eight out of 17 domains. The proportion of trainees who met the expected requirement was 74% for radical prostatectomy, 71.4% TRUS and biopsy, 53.2% ESWL, 45.5% urodynamics, 42.9% andrology, 40.3% flexible cystoscopy, 33.8% female incontinence and 23.4% paediatric procedures.
The mean operative exposure for inguinoscrotal surgery increased from 140 (range 21–516) to 190 (range 66–319) cases, representing twice the expected requirement for circumcision, scrotal procedures and inguinal orchidectomy combined. The same pattern was also seen for nephrectomy and ureteroscopy with means of 101 (range 15–237) and 203 (range 53–687) cases respectively, representing five-fold and four-fold the expected requirement. It is notable that these five procedure domains are also the only ones where >95% of trainees met the minimum requirement. The relationship between mean exposure and the proportion of trainees achieving the minimum requirements is shown in Figure 1.
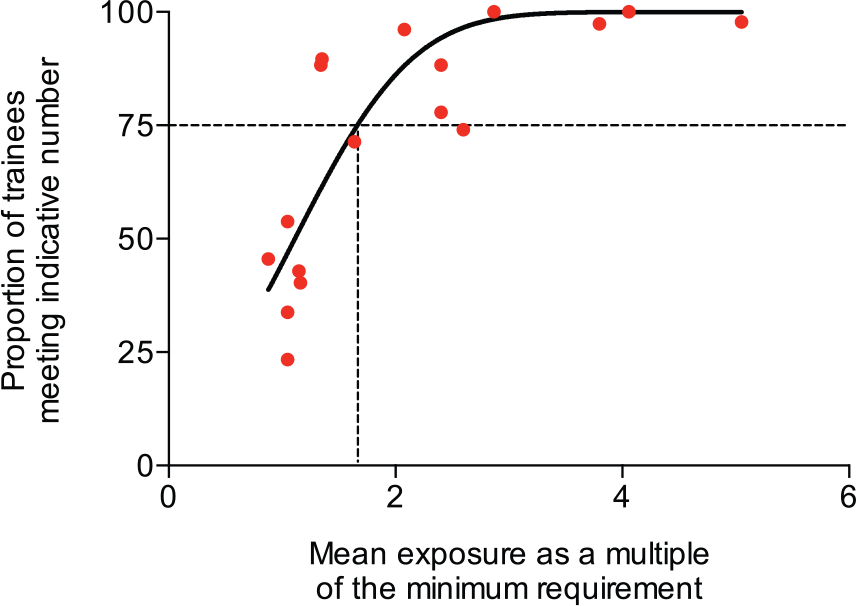
The relationship between mean exposure and the proportion of trainees achieving the minimum requirements.
The number of trainees failing to meet the requirements in multiple domains was very high. Only one trainee in the 2015 cohort met the JCST minimum requirement in all 17 domains and 54.5% of trainees failed to meet the requirements in five or more domains (Figure 2). Overall, in the 2015 cohort >75% trainees achieved indicative numbers in nine out of 17 domains compared to the 2012 cohort who achieved only five out of 15 domains.
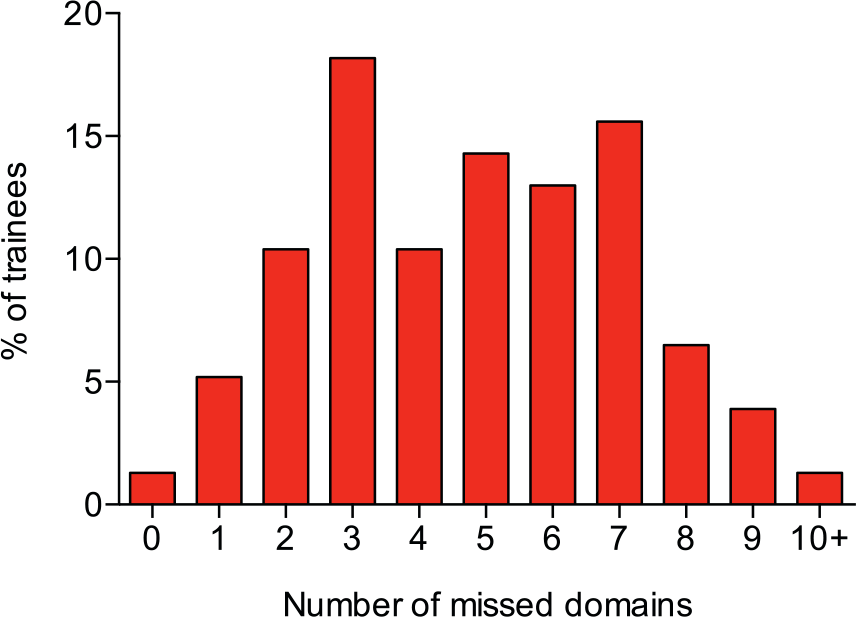
The number of trainees failing to meet the requirements in multiple domains.
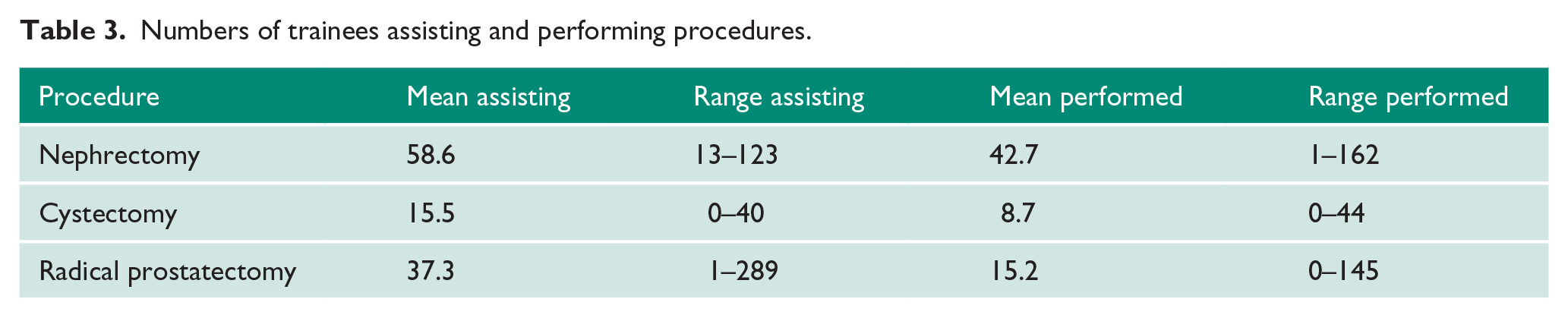
A single surgeon can undertake the vast majority of urological procedures without the need for an assistant. Exceptions to this are nephrectomy, cystectomy and radical prostatectomy. Analysing procedures performed as the primary surgeon or assistant demonstrated that the mean number of nephrectomies undertaken by trainees as the primary surgeon is high, at 42.7. The mean total experience for radical prostatectomy was also markedly greater than the minimum requirement at 52, although this was comprised of a majority of assisting with a mean of 37.3 cases (Table 3).
Numbers of trainees assisting and performing procedures.
Discussion
Indicative numbers in UK surgical training are a key metric used in the ARCP process and CCT application. We have previously published data on a cohort of trainees, 1 demonstrating a very wide spectrum of operative exposure and a large disparity between JCST expectations and trainee achievement. The current study has demonstrated a clear improvement in the proportion of trainees meeting requirements in a number of domains with >75% of trainees in 2015 cohort achieving indicative numbers in nine out of 17 domains compared to five out of 15 in the 2012 cohort.
Proponents may argue that this improvement indicates that indicative numbers have driven up standards, by ensuring that trainee experience is aligned to the curriculum, rather than being the result of opportunistic exposure. However, this improvement is not completely explained by improved surgical training or increased awareness of the requirements by trainees. For a number of the domains (TURBT and male LUTS procedures) it is due only to a reduction in the indicative number. The continued reduction in mean exposure to male LUTS procedures and TURBT follows a decade-long trend previously noted between the 2012 cohort and data published in 2012 by Gill et al. on a six-year cohort of trainees from 2004–2009. 2 These data demonstrate sustained reductions in mean numbers of both male LUTS procedures, at 189, 187 and 161, and TURBT, at 190, 184 and 162, in the Gill et al. data, for the 2012 and 2015 cohorts respectively. The reduction in exposure to TURBT and male LUTS procedures is not explained by a reduction in the number of procedures being performed nationally. HES (Hospital Episode Statistics) data for England reports little change between 2005/2006 and 2014/2015, with 40,107 and 40,206 TURBTs and 25,451 and 23,418 transurethral resections of the prostate (TURPs) respectively. 3 Length of training may be influencing the data, which has reduced from six to five years over this time period. Another factor may be the increasing utilisation of weekend operating and non-NHS care providers, which do not typically provide training opportunities.
We suggest that for investigative and outpatient procedures, including flexible cystoscopy, urodynamics, ESWL and TRUS, the rise in exposure may be driven by increased recording efficiency as a corollary to the established role of indicative numbers. However, the improvement in recorded andrology and female incontinence surgery more likely reflects a true increase in exposure, which is welcome. Changes in paediatric urological surgery exposure were more difficult to examine, as in both cohorts the majority did not include separate logbooks for paediatric surgery. Although there was an improvement in indicative numbers, it is likely that we have underestimated true exposure.
The majority of trainees will not undertake nephrectomy or radical prostatectomy in consultant practice, due to sub-specialisation and centralisation of cancer services. Current mean operative exposure for nephrectomy stands at over 100 cases and for radical prostatectomy almost 40 cases as an assistant. This disparity between expectation and exposure indicates that for the majority of trainees their time in training is not being optimally utilised. With over half of trainees failing to meet operative requirements in >5 domains, training must focus more on the requirements of the curriculum rather than service provision.
Once trainees have achieved the required indicative number and competency for a domain, they should be given opportunities or priority for placements to gain experience in the remaining required domains to ensure they meet all requirements. It is not expected that trainees work on one domain at a time but on multiple domains available to allow broad experience, and then focus on particular areas of need, continuing to gain experience in domains where the indicative number is reached – as this is a minimum requirement – there is no limit on operative experience.
Urology training is changing, with a trend towards training the majority of new consultants as generalists, to meet the population demands following the Shape of Training Review. 4 There are only a small number with subspecialist training sufficient to embark on subspecialty practice without a further period of dedicated training such as post-CCT fellowship or mentoring during the consultant post, as this is not expected nor a requirement for CCT. There is a silent acceptance of this, as clearly reflected in the competency levels for indicative numbers since their introduction, as for cystectomy and radical prostatectomy the competency level is 1 (has observed), and for andrology, female urology, paediatric urology, PCNL and ESWL level 2 (can do with assistance). In addition, with the 2015 guidelines, nephrectomy has been reduced from level 3 to 2. Furthermore, the indicative numbers for nephrectomy, cystectomy, female urology and paediatric urology have all been reduced. It therefore raises the question whether further formal assessment of indicative numbers and competency levels should be applied for those undergoing subspecialist training, as exists in other surgical specialties such as general surgery where the final two years are dedicated to subspecialty training with specific indicative numbers and competency levels, in addition to those for all trainees. 4 In addition, the effects of reduction in training requirements and exposure in pelvic and abdominal surgery may significantly impact upon the provision of emergency urological care in district general hospitals, and how we overcome this is not clear.
For trainees to achieve expected exposure requires individual departments to be undertaking sufficient numbers of the procedures in question. Whilst this may be the case for the majority of procedures, there is evidence for paediatric urology and female incontinence that most trainee placements are unlikely to provide the exposure required. 5 Our data also suggests that it is an oversimplification to assume that if the ratio between the total number of specific procedures in a Local Education Training Board (LETB) and the total number of trainees exceeds the minimum requirement all trainees should achieve the minimum standard. Our data indicates that the total number of procedures available to trainees may need to be three times the minimum requirement for all trainees in a LETB region, and twice that for 75% to reach the minimum. This is explained by competing activities such as annual leave, study leave and on-call commitments. A concerted effort on behalf of the LETB to match trainees to placements that address their deficiencies may result in both an increase in the proportion of trainees achieving minimum operative exposure and a reduction in training opportunities for trainees who have already achieved the required competence.
Irrespective of the issues described, the introduction of indicative numbers has led to increasing recorded numbers of procedures within the majority of operative domains. Individual learning curves vary and there are not fixed numbers of procedures undertaken that lead to the acquisition of competency, but there is a strong relationship between surgeon experience and patient outcomes. 6 It may therefore be correct that certification guidelines should include minimum operative exposure.
Conclusion
Overall, this data has shown significant improvements in the number of trainees meeting indicative numbers, but whether competency levels are met is beyond the scope of this article. However, there are still a large number of domains with significant deficiencies. Such deficits are not confined to a small number of trainees, with the majority having been demonstrated to be below expectations in a large number of domains. Despite this failure to achieve the requirements, no trainees to date have been denied the award of CCT as a result. Indicative numbers are here to stay, and with trainees now coming through who were appointed after their introduction, there will be little if any scope for non-compliance and those not complying run the risk of not being awarded a CCT at the end of training. Trainees alone cannot be held accountable for their lack of operative experience, therefore the onus is both on the LETBs to further examine the delivery of surgical training to facilitate achievement of these requirements, and the trainees to achieve them.
Footnotes
Acknowledgements
The authors would like to thank Megan Warde from the JCST for her assistance with this work.
Conflicting interests
KO’F was chair of the Urology SAC between 2010–2012. TT was chair of the Urology SAC between 2013–2016. RR was a previous chair of Senior Urological Registrars Group (SURG). JD and EL have held the positions of Secretary and Treasurer of SURG.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
RR.
Contributorship
RR, KO’F and TT conceived the study. RR researched the literature. RR, JD and EL performed the data collection. JD and RR performed the data analysis. RR wrote the first draft of the manuscript. EL wrote the second and third draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.