
Abstract
Genitourinary syndrome of menopause affects approximately 50% of women post-menopause and is under-reported. This review of the condition including established and newer treatment options aspires to empower clinicians to ask about symptoms and be more proactive in their management.
Keywords
This under-recognised condition affects approximately 50% of women post-menopause. 1 The case described highlights the importance of considering this diagnosis and asking the right questions, with the patients’ permission. Women are generally happy to respond, and less likely to volunteer information if not asked. In addition, many women under-report the extent of the problem and the impact that it has on them and their partner. Reluctance of women to volunteer concerns regarding the symptoms relating to vaginal health and sexual satisfaction is compounded by a reluctance of health-care professionals to address these issues. This may be, in part, due to lack of awareness as to how to treat the problem. Women should be asked routinely about symptoms of GSM, as many do not associate genital problems with menopause and are embarrassed to discuss them or ask for help. 2
Before I discuss Virginia (not her real name), I would like to consider GSM in more detail and draw attention to the current treatment options, many of which are relatively new.
GSM is comparatively new terminology, developed by consensus between the International Society for the Study of Women’s Sexual Health and the North American Menopause Society in 2014.
3
The new terminology recognises that all tissues in the genitourinary tract can be affected by lack of estrogen during the peri- and post-menopause. Women affected by GSM can have many symptoms (Box 1). The two most common are vaginal dryness and pain during sexual intercourse. GSM can be associated with bleeding, leading to invasive investigations. During this process, the focus often moves to exclusion of cancer rather than a treatable hormone deficiency. For some women, penetrative sexual intercourse may become impossible. Unlike other common menopausal symptoms, such as hot flushes and night sweats, which tend to improve with time, GSM is a chronic condition, with symptoms deteriorating over time in untreated women. Further research, with randomised controlled trials, is required for some of the newer therapeutic interventions described below, with a specific focus on sexuality.
4
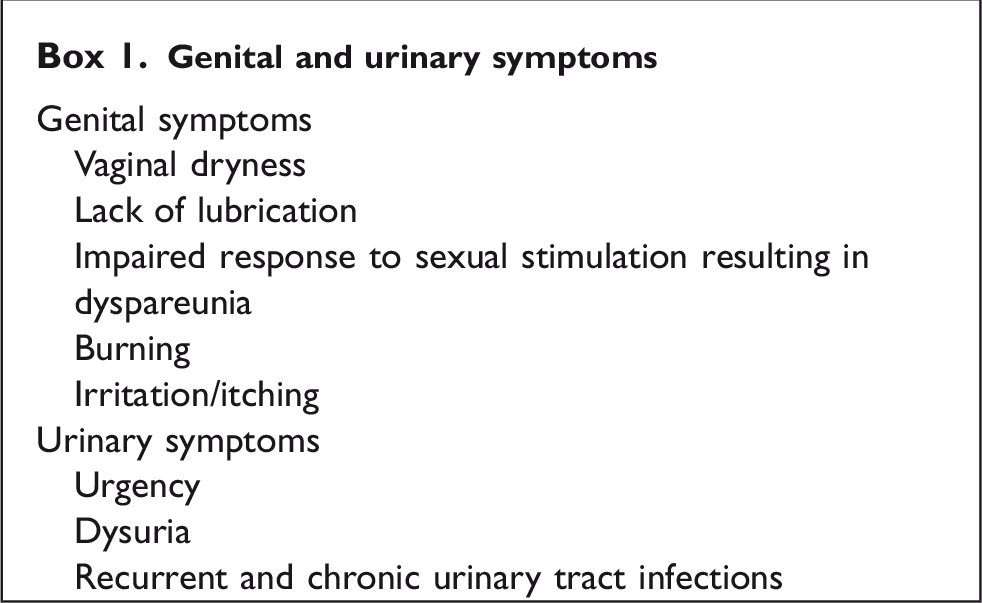
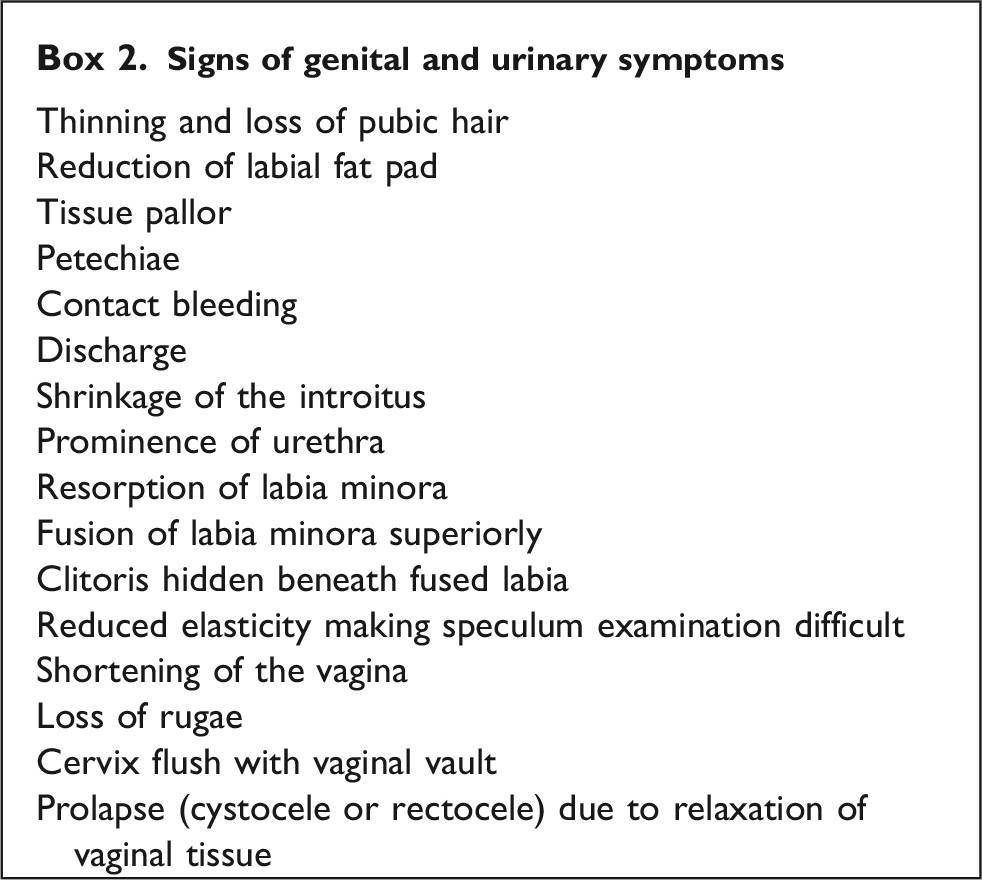
Affected women may have symptoms relating to the genital tract, urinary tract or both (Box 1). Possible signs are included in Box 2.
Sexual difficulties are particularly associated with shrinkage of the introitus, loss of elasticity and reduced lubrication.
A more objective evaluation of vulvovaginal atrophy depends on the measurement of vaginal pH, using low range pH paper (pH is increased) and assessment of vaginal maturation index (VMI) by taking a vaginal smear (increase in parabasal cells and reduction in superficial cells 5 ).
The optimal treatment for any condition is dependent on the correct diagnosis. For GSM, this will depend primarily on the history, but examination is important to avoid missing other conditions including significant pathology (genital dermatoses, lichen sclerosis et atrophicus, lichen planus and cancer) and also to confirm the physical findings associated with estrogen deficiency, listed in Box 2. Estrogen deficiency and the effect that this has on urogenital tissues is the underlying cause of GSM. The impact of lack of estrogen on tissue quality varies considerably between women. This possibly relates to pre-existing individual tissue quality, but further research is needed in this area. 6
Estrogen is necessary to maintain urogenital structure and function, including the production of mucous secretions. Lack of estrogen results in a decrease in blood flow, loss of glycogen and collagen with thinning of the vaginal epithelium. This alters the composition of the microbiome, reducing lactobacilli and increasing pH. Leucocytes are increased and can cause a discharge with irritation. Colonisation of vagina with pathogens such as Escherichia coli and Mobiluncus, in addition to causing inflammation, can predispose to urinary tract infection. 7
Treatment options
Available treatments include non-hormonal and hormonal options. Non-hormonal choices are particularly important for women with potential contraindications to the use of hormones; the most significant of which are hormone-dependent cancers, specifically breast and endometrial.
Non-hormonal
○ Vaginal lubricants
○ Vaginal moisturisers
○ Microablative fractional CO2 laser
○ Non- ablative photothermal Erbium:YAG – laser
○ Ospemifene (Selective Estrogen Receptor Modulator (SERM)). 8
Hormonal
Estrogen
○ Systemic – delivered orally, transdermally (patch or gel) or subcutaneously (implant)
○ Vaginal (systemically delivered estrogen is often too low dose to have a beneficial effect on the genital tissues). 9
Dehydroepiandrosterone (DHEA) – this is delivered vaginally on a daily basis. DHEA is metabolised within the vaginal mucosa, by a process known as intracrinology, to estrogen and testosterone. Testosterone, even in low dosage, delivered locally with no change in systemic levels, may have a beneficial effect on libido.
Virgina, a 56-year-old nulliparous woman, had seen many clinicians and undergone a number of invasive procedures, by the time she attended the menopause clinic. She was 10 years post-menopause. She had hormone replacement therapy (HRT) for five years, and this was stopped approximately five years before I first met her. The rationale for discontinuation of treatment was that she ‘had been on it for five years’. This unfortunate consequence of the Women’s Health Initiative (WHI) study has been redressed by NICE CG 23, which clearly states that there is no mandatory stopping point in relation to HRT and that length of use should be determined by an on-going individualised risk assessment.
A retired lawyer, she was in good general health, taking the following medication for minor conditions – Pantoprazole (reflux), Oxytetracycline (rosacea), Movicol (constipation). She had a history of endometriosis. She did not smoke or drink excessive amounts of alcohol and had no personal or family history of breast cancer or venous thromboembolism.
The original referral to gynaecology (in another area) in January 2018, due to post-menopausal bleeding (continual spotting in association with suprapubic discomfort/urge incontinence), resulted in investigations including bimanual examination (normal), transvaginal ultrasound (normal uterus/endometrium), endometrial sampling (non-diagnostic due to insufficient tissue) and hysteroscopy (normal). No treatment was provided, despite the observation that the vagina and cervix were atrophic. Follow-up ultrasound scan was requested as a result of a coincidental finding of an ovarian cyst (Ca125 normal, as was repeat ultrasound scan four months later). When seen in a general gynaecology clinic in May 2018, a small speculum was passed and a cervical smear test was taken (normal). The introitus was described as tight, and bimanual examination was not possible at that time due to discomfort. No other mention was made in relation to any of the features of vulvovaginal atrophy listed in Box 2 above. Vagifem 10 µg daily for two weeks, and then twice weekly was initiated, in addition to samples of ‘Yes’ products and further review was arranged. During this consultation, Virginia enquired about laser treatment to improve tissue quality. She was told by the doctor seeing her that they had not really heard much about it, but that they would get in touch with her and her GP once they had looked into it. Later documentation confirmed an unsuccessful response to twice weekly Vagifem and consideration was being given to recommencing systemic HRT. This resulted in referral to the menopause service.
In the menopause clinic, Virginia was diagnosed with GSM. Vaginal estrogen was changed to Estring, delivering 7.5 µg estradiol daily and she was also commenced on Estradiol gel (and Utrogestan for endometrial protection) to see whether this might improve libido. Clearly, GSM and libido are not separate issues, and Virginia demonstrates the complexities associated with patient management in relation to sexual problems. Initially, she said that sexual intercourse had been uncomfortable for a few years. When first seen in the menopause service, she said that she and her husband had not had sex for two years. Prior to having CO2 laser therapy (Mona Lisa Touch®) privately, she had extended this to four years. It was likely longer and lack of sexual contact is a problem for both partners. Virginia used Estring, which provided continuous local oestrogen therapy, for six months prior to her first CO2 laser treatment in March 2019. The recommendation is for three to five treatments four to six weekly initially, followed up with 12 monthly treatments for an indefinite period of time. However, there are no long- term data to support current recommendations.10–13 Laser therapy is not available on the NHS and treatments are expensive, averaging £700.00 per treatment. Many women with the potential to benefit will be unable to afford this option. In Virginia’s case, there was complete resolution of the signs of atrophy, which included tissue pallor, petechiae, contact bleeding, resorption of the labia minora, loss of rugae, cervix flush with vaginal vault, shrinkage of the introitus and prominence of the urethra.
The addition of testosterone gel improved the desire for sex, but this was countered by a huge element of fear, preventing any attempt at penetration. My plan now, with Virginia’s consent, is to refer her to our specialist pelvic floor physiotherapist for support with pelvic floor relaxation and vaginal dilators and also for psychosexual counselling if required (the waiting time in six months). 5
This tale from the clinic highlights a number of important points:
Vaginal bleeding is a common presentation in post-menopausal women and whilst it is important to exclude cancer, treatment of other commoner conditions, like GSM should not be forgotten. Management should include access to all newer treatment options, as some women have a suboptimal response to vaginal estrogens, even when used in higher doses, out-of-product license. Randomised controlled trials using sham laser are needed to prove efficacy of laser therapy. 14
An optimal outcome is likely to involve a multidisciplinary team, including well-informed medical staff, a specialist pelvic floor physiotherapist and a psychosexual counsellor. Managing the brain through therapy is as important as reversing the architectural defects resulting from estrogen deficiency.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.