
Abstract
Objective
Parkinson’s disease (PD) is a progressive neurodegenerative disorder for which early screening remains challenging. Although voice-based machine learning approaches have shown promise as non-invasive screening tools, most existing studies rely on single-dataset evaluations, random data splits, and accuracy-centric metrics, raising concerns about dataset bias, subject leakage, and limited real-world generalizability. This study aims to develop a generalization-aware, explainable, and privacy-preserving framework for PD detection using voice data.
Methods
Three heterogeneous PD voice datasets are integrated using a strict feature harmonization strategy that retains only common acoustic features to enable fair cross-dataset evaluation. A diverse set of classical, ensemble, neural, and meta-learning models is evaluated under subject-aware experimental protocols with extensive cross-validation and hyperparameter optimization. The framework further incorporates ablation analysis and statistical significance testing. Realistic deployment conditions are simulated through cross-dataset generalization experiments, complemented by explainable AI (XAI) analysis using SHAP and LIME, as well as federated learning simulations for privacy-preserving training.
Results
Experimental findings show that models achieving over 95% accuracy in single-dataset settings experience substantial performance degradation under cross-dataset evaluation, indicating strong dataset dependency in prior approaches. Performance typically converges to moderate levels, reflecting a generalization ceiling under dataset heterogeneity. Frequency-based perturbation features (jitter-related measures) consistently demonstrate greater robustness than amplitude-based features across datasets. Explainability analysis confirms the stability and physiological relevance of key acoustic biomarkers despite reduced predictive performance. Federated learning models achieve comparable or improved generalization performance relative to centralized training while preserving data privacy.
Conclusion
By reframing voice-based PD detection as a generalization and trustworthiness problem rather than an accuracy optimization task, this study provides a more realistic and deployment-oriented evaluation framework. The findings highlight the importance of cross-dataset validation, robust feature selection, explainability consistency, and privacy-aware learning, offering a more clinically meaningful foundation for future healthcare AI systems.
Keywords
1. Introduction
Parkinson’s disease (PD) is the second most prevalent neurodegenerative disorder worldwide, characterized by progressive motor impairments such as tremor, bradykinesia, rigidity, and postural instability, as well as non-motor symptoms including speech and voice abnormalities.1,2 Early identification of PD is critical for timely symptom management and improved quality of life. 3 However, clinical diagnosis largely depends on expert neurological assessment and subjective interpretation of symptoms. 4 This process is often time-consuming, resource-intensive, and inaccessible in under-resourced or remote settings. 5 Consequently, there has been increasing interest in automated, non-invasive, and cost-effective computational tools that can support Parkinson’s disease screening and monitoring, rather than replace clinical diagnosis.6,7
Among the various sensing modalities explored for PD detection, voice-based acoustic analysis has gained considerable attention due to its non-intrusive nature and the strong association between PD and vocal impairments arising from neuromuscular dysfunction. 8 Speech production requires fine-grained motor control, which is frequently disrupted in PD, leading to measurable abnormalities in frequency and amplitude perturbation patterns. 9 Leveraging these characteristics, numerous studies have applied machine learning (ML) and deep learning (DL) techniques to voice recordings to discriminate between individuals with Parkinson’s disease and healthy controls, often reporting very high classification accuracy.10–12
Despite these promising results, the dominant evaluation paradigm in the literature relies on single-dataset experimental setups, where both training and testing data originate from the same dataset. While such settings simplify experimentation, they introduce several critical limitations. Voice datasets for Parkinson’s disease are typically collected under controlled and homogeneous conditions, using specific recording devices, acquisition protocols, languages, and subject populations. 13 Models trained and evaluated within these constrained environments are vulnerable to dataset-specific bias and may inadvertently exploit recording artifacts, environmental cues, or subject-level leakage rather than learning robust disease-related patterns. As a result, reported performance (frequently exceeding 90% accuracy), may substantially overestimate real-world effectiveness when models are applied to unseen data sources.
In realistic clinical and telemedicine scenarios, voice recordings are collected across diverse microphones, acoustic environments, languages, and demographic populations, leading to significant distributional shifts across datasets. 14 However, cross-dataset generalization remains largely underexplored in the Parkinson’s disease detection literature (elaborately discussed in Section 2: Related Works). Moreover, most existing studies emphasize maximizing predictive accuracy while giving limited attention to two additional factors essential for clinical adoption: interpretability and data privacy. Black-box prediction models without transparent decision-making mechanisms hinder clinician trust and accountability, while centralized data collection raises ethical, legal, and regulatory concerns regarding patient privacy and data sharing.
Motivated by these limitations, this study systematically investigates the robustness, generalization, interpretability, and privacy-preserving potential of voice-based Parkinson’s disease detection models under realistic deployment conditions. Specifically, we address the following research questions (RQs): • • • • • • • •
To address these research questions and overcome the limitations of prior Parkinson’s disease detection studies, this work proposes a generalization-aware, explainable, and privacy-preserving evaluation framework for voice-based PD detection. Rather than optimizing models for peak accuracy within a single dataset, the proposed framework deliberately prioritizes cross-dataset robustness as the primary evaluation objective. Three heterogeneous voice-based PD datasets are integrated through a strict feature harmonization strategy, retaining only acoustic features shared across all datasets. Although this design choice reduces feature dimensionality, it effectively mitigates dataset leakage, enforces comparability across data sources, and enables reproducible evaluation under realistic deployment conditions.
A diverse family of machine learning models (including classical classifiers, ensemble-based learners, neural network baselines, and stacking-based meta-learning approaches) is systematically evaluated using subject-aware experimental protocols that explicitly prevent subject-level overlap between training and testing data. Model development incorporates rigorous hyperparameter optimization (RandomizedSearchCV, and GridSearchCV) and multi-fold cross-validation (StratifiedKFold, and RepeatedStratifiedKFold), ensuring that performance estimates are not driven by arbitrary parameter choices or favourable data splits. Extensive cross-dataset generalization experiments are conducted to emulate real-world clinical scenarios in which trained models are applied to previously unseen data sources. Four complementary cross-dataset scenarios were designed (like models trained on the dataset D1 and evaluated on the dataset D2; models trained on a pooled dataset combining D1 and D2 and evaluated on D3) for exposing the impact of dataset heterogeneity on predictive reliability.
To further strengthen transparency and clinical relevance, the framework integrates Explainable Artificial Intelligence (XAI) techniques by combining SHAP and LIME to provide complementary global and local explanations, enabling the identification and stability analysis of acoustic biomarkers under distribution shift. In addition, a Federated Learning (FL) simulation is implemented across multiple client configurations to investigate privacy-preserving collaborative learning under heterogeneous data distributions, highlighting both performance gains and trade-offs across participating clients. Finally, ablation analyses and statistical significance testing are performed to assess the robustness of observed performance differences, distinguish meaningful trends from noise, and characterize the limits imposed by dataset heterogeneity rather than model choice alone.
It is important to note that adopting cross-dataset evaluation, subject-aware splitting, and strict feature harmonization results in lower predictive performance compared to conventional single-dataset studies. However, this reduction reflects realistic deployment challenges rather than methodological limitations. By prioritizing deployment realism over inflated accuracy, this work provides a more clinically meaningful assessment of voice-based Parkinson’s disease detection. The main contributions of this study are: • • • • • • •
Thereby, this work shifts the focus from accuracy-centric evaluation to generalization, interpretability, and deployment readiness, providing a more reliable foundation for clinical PD detection systems.
2. Related Works
Recent advances in machine learning and deep learning have led to a rapid expansion of research on PD detection using diverse data modalities, including voice recordings, handwriting patterns, gait signals, medical imaging, and multimodal clinical data. Existing studies have explored a wide spectrum of learning paradigms ranging from traditional classifiers to deep neural networks and, more recently, privacy-preserving federated learning frameworks. While these works collectively demonstrate the potential of data-driven approaches for non-invasive and automated PD diagnosis, they also differ substantially in terms of evaluation protocols, validation strategies, performance metrics, and deployment assumptions. This section reviews prior research by categorizing representative studies according to modelling approach and learning paradigm, with particular attention to how PD detection systems are evaluated and reported in the literature.
2.1. Review and survey studies on Parkinson’s disease detection
A substantial body of literature has attempted to systematize the rapidly expanding use of ML and DL techniques for Parkinson’s disease diagnosis. Recent systematic reviews and surveys emphasize the growing diversity of data modalities and modelling approaches while simultaneously highlighting persistent methodological limitations. In, 15 an extensive systematic literature review of 133 studies published between 2021 and 2024 categorized PD detection research into acoustic, biomarker, imaging, movement-based, and multimodal approaches, offering insights into commonly used datasets and algorithms alongside open challenges. Similarly, the PRISMA-based review in Ref. 16 critically examined 113 ML-driven PD studies and revealed widespread methodological weaknesses, including the absence of holdout test sets, inadequate hyperparameter tuning practices, and limited comparative evaluations—factors that may substantially inflate reported performance. Earlier reviews further contextualized these challenges. The comprehensive survey in Ref. 17, covering 209 studies up to 2020, documented the increasing adoption of ML techniques across heterogeneous data sources but noted the lack of standardized evaluation protocols. Facial expression–based PD detection, a comparatively newer modality, was systematically reviewed in Ref. 18, where the authors identified promising results but emphasized severe dataset scarcity and the lack of generalization testing. Reviews focusing on specific modalities such as voice, handwriting, and spiral-wave data 10 as well as multimodal biomarkers, 19 consistently reported high diagnostic accuracy but underscored unresolved concerns related to dataset bias, explainability, and clinical translation. Broader reviews on biomarker integration and healthcare infrastructure 20 reinforced the importance of multimodal fusion while acknowledging challenges arising from data heterogeneity and symptom variability. Bibliometric and trend-based analyses 21 highlighted the rapid rise of DL-based PD studies worldwide, identifying incremental and continual learning as underexplored research directions. Collectively, these review papers converge on a critical observation: although ML and DL models demonstrate high promise for PD diagnosis, their real-world robustness, interpretability, and deployment readiness remain insufficiently addressed.
2.2. Traditional machine learning approaches for Parkinson’s disease detection
A large portion of PD detection research has focused on traditional ML classifiers applied to hand-engineered features derived from structured biomedical data, particularly voice, handwriting, and gait signals. Early and recent studies using benchmark datasets—most notably the UCI voice dataset—demonstrated strong discriminative performance using classifiers such as K-Nearest Neighbors (KNN), Support Vector Machines (SVM), Random Forests (RF), Logistic Regression (LR), Decision Trees, and shallow neural networks.22–31 These works typically extracted acoustic features related to jitter, shimmer, pitch variation, and noise ratios, which are physiologically linked to vocal instability in PD patients. To enhance predictive performance, many studies employed preprocessing strategies such as class rebalancing through SMOTE, feature selection using filter or wrapper methods, and systematic hyperparameter tuning via grid or randomized search, with several reporting accuracy levels exceeding 95% on held-out or cross-validation splits.22,24–26
Beyond voice-based detection, handwriting analysis emerged as an alternative non-invasive modality, particularly using spiral and wave drawing tasks that capture fine motor impairments associated with PD. Studies leveraging handcrafted features or gradient-based descriptors combined with ML classifiers reported encouraging results, demonstrating the feasibility of automated screening using drawing patterns.32,33 While these handwriting-based systems generally achieved lower accuracy compared to voice-based approaches, they offered complementary insights into motor dysfunction and broadened the scope of PD detection beyond speech alone. Several works also explored enhanced security and privacy-aware ML pipelines. For instance, 34 proposed secure two-party computation and local classification mechanisms to protect sensitive patient data while maintaining competitive classification performance. Gait-based ML studies further expanded the modality spectrum by analysing spatial–temporal walking parameters to distinguish PD patients from healthy individuals and, in some cases, to estimate disease severity or stage. 35 These studies achieved moderate classification accuracy but provided clinically interpretable features such as stride variability and asymmetry, which align well with neurological assessments.
Despite these methodological advances, most traditional ML studies relied on relatively small, homogeneous datasets collected from single institutions or controlled environments. While some works explicitly acknowledged dataset size limitations, potential bias, or institutional dependency, 31 systematic evaluation under distribution shifts—such as cross-dataset testing or external validation—remains uncommon. As a result, the generalizability of many high-performing traditional ML models to real-world clinical settings remains largely unverified.
2.3. Deep learning–based Parkinson’s disease detection
Deep learning approaches have gained increasing prominence in PD detection research due to their ability to model complex, non-linear relationships and automatically learn hierarchical feature representations. Convolutional Neural Networks (CNNs) and transfer learning architectures have been widely applied to handwriting images, spiral and wave drawings, MRI scans, and voice spectrograms, often achieving very high diagnostic accuracy under controlled experimental conditions.36–44 Many of these studies reported accuracy values exceeding 97% when evaluated on internal validation or test sets, highlighting the representational power of deep architectures.36,37,39,42,43
Multimodal DL frameworks demonstrated the benefits of fusing heterogeneous data sources. For example, MultiParkNet 42 integrated speech, handwriting, neuroimaging, and physiological signals within a unified deep learning framework, achieving strong diagnostic performance across modalities and emphasizing the potential of comprehensive data fusion for early PD detection. Neuroimaging-focused DL studies leveraged MRI-derived biomarkers and specialized CNN architectures to detect nigrosome abnormalities and structural changes associated with PD, reporting high AUC values and clinically meaningful correlations with disease severity.38,44 Audio-based deep learning systems also showed notable progress by incorporating autoencoders, CNNs, LSTM networks, and spectrogram-based representations to capture subtle temporal and frequency-domain variations in speech signals.40,41,45 Several of these studies demonstrated that deep architectures could outperform traditional ML classifiers when trained on sufficiently rich and well-curated datasets. In parallel, a subset of DL-based works incorporated explainable AI techniques such as LIME and SHAP to improve model transparency and clinical interpretability, acknowledging the importance of explainability for medical decision support systems.36,46
However, despite these advances, most DL studies continued to evaluate performance under idealized experimental settings, often relying on random train–test splits within a single dataset. Limited attention has been paid to cross-domain robustness, calibration under dataset shift, or real-world deployment constraints. Moreover, the dependence of DL models on large, curated datasets raises concerns regarding scalability, fairness, and reproducibility in heterogeneous healthcare environments where data distributions may differ substantially across institutions.
2.4. Federated learning and privacy-preserving frameworks
To address growing concerns regarding data privacy, regulatory constraints, and institutional barriers in healthcare, FL has emerged as a promising paradigm for PD detection. Several studies demonstrated that FL-based CNN models can achieve performance comparable to centralized training while preserving patient data privacy by keeping raw data localized at participating institutions.47–49 These works established the feasibility of collaborative model training across decentralized environments, particularly in speech and wearable sensor-based PD detection.
More recent research has focused on addressing the challenges posed by non-independent and identically distributed (non-IID) data, multilingual speech variability, and institutional heterogeneity. For example, FedOcw 50 introduced optimized weight-sharing and aggregation strategies to improve convergence stability and diagnostic accuracy across diverse clients, highlighting the importance of adaptive federated optimization in realistic healthcare settings. Broader perspectives on federated data analysis have also emphasized the role of FL in enabling scalable, privacy-aware PD research across large, distributed clinical cohorts. 51 Beyond performance, several studies explored the integration of interpretability within federated frameworks. In, 52 federated learning was combined with explainable AI techniques, including interpretable fuzzy systems and federated SHAP explanations, to analyze trade-offs between accuracy, transparency, and trustworthiness. Other works proposed complex FL-enabled architectures incorporating fuzzy logic, heuristic optimization, and deep networks to enhance PD classification performance under privacy constraints. 53
While these federated approaches demonstrate significant potential for privacy-preserving PD detection, they also reveal persistent challenges. Performance degradation under severe data heterogeneity, uneven client contributions, and explainability consistency remain open issues. Consequently, existing FL-based PD studies highlight the need for systematic evaluation of robustness, generalization, and interpretability when deploying collaborative learning systems in real-world clinical environments.
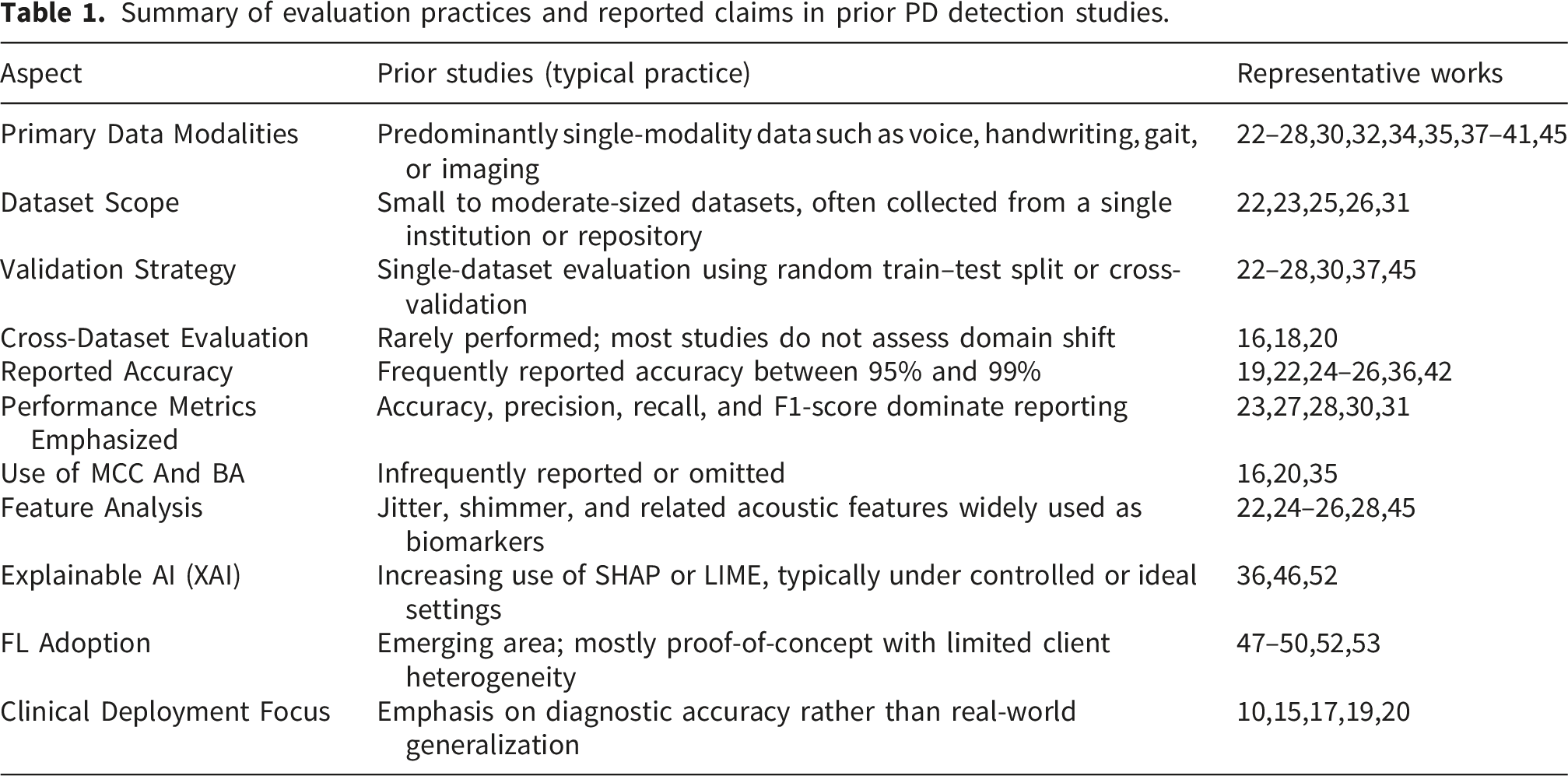
Summary of evaluation practices and reported claims in prior PD detection studies.
2.5. Research gap and motivation
Despite extensive progress across ML, DL, and FL paradigms for Parkinson’s disease detection, several critical gaps persist in the current literature. First, the majority of existing studies prioritize single-dataset accuracy, often reporting near-perfect performance without evaluating robustness under distribution shifts, cross-dataset testing, or real-world variability—a limitation explicitly highlighted in systematic reviews such as. 16 Second, while explainable AI techniques are increasingly adopted, their stability and reliability under degraded or shifted conditions remain largely unexplored, raising concerns about clinical trustworthiness. Third, federated learning approaches, although promising for privacy preservation, are seldom analyzed through the lens of performance–privacy trade-offs or model behavior under heterogeneous clinical environments. Most importantly, existing works tend to validate feasibility rather than deployability. There is a lack of integrated studies that jointly examine generalization, explainability, and privacy within a unified experimental framework. Motivated by these gaps, the present study aims to move beyond inflated accuracy claims by systematically evaluating PD detection models under realistic conditions, emphasizing generalization robustness, explainability consistency, and privacy-aware learning. By doing so, this work seeks to bridge the gap between experimental success and clinically meaningful, trustworthy deployment of AI-driven Parkinson’s disease diagnostic systems.
3. Methodology
This section presents a comprehensive methodological framework designed to evaluate voice-based PD detection models under realistic, deployment-oriented conditions rather than idealized laboratory settings. The methodology is deliberately structured to address critical limitations observed in prior studies—namely subject leakage, dataset-specific bias, over-reliance on accuracy, lack of interpretability, and insufficient consideration of data privacy. Instead of emphasizing algorithmic novelty in isolation, the proposed framework prioritizes experimental rigor, generalization robustness, interpretability consistency, and privacy preservation, which are essential for clinically reliable PD screening systems.
This study is a computational and experimental machine learning investigation aimed at evaluating the generalization, explainability, and privacy-preserving capabilities of Parkinson’s disease detection models using publicly available datasets. The research follows a cross-dataset evaluation framework, incorporating centralized, explainable AI (XAI), and federated learning paradigms to simulate realistic deployment conditions under data heterogeneity. The study was conducted over the period 2025–2026 at the Department of Information and Communication Engineering, Noakhali Science and Technology University, Noakhali, Chattogram, Bangladesh. As the research is based entirely on secondary, publicly available datasets, no direct patient involvement or data collection was performed at the study location. The institutional setting primarily supported model development, experimentation, and analysis.
The overall workflow is illustrated in Figure 1, which presents the end-to-end experimental pipeline. As shown, three heterogeneous PD voice datasets are first integrated using subject-aware preprocessing to prevent subject-level overlap and label inconsistency. A strict feature harmonization strategy is then applied, retaining only acoustic features common across all datasets to mitigate dataset-specific bias and enable fair cross-dataset comparison. Dataset-wise scaling and validation are performed using training-only statistics to avoid information leakage. Model learning is conducted using a diverse set of classical, ensemble, neural, and stacking-based approaches under repeated subject-aware cross-validation with extensive hyperparameter tuning. Generalization capability is assessed through explicit cross-dataset evaluation scenarios that simulate real-world deployment on unseen data sources. To enhance transparency, SHAP and LIME are employed to provide global and local explanations of model behavior, while FL simulations evaluate privacy-preserving learning without raw data sharing. Finally, robustness is examined through systematic ablation studies, statistical significance testing, and multi-metric evaluation. Generalization-aware, explainable, and privacy-preserving workflow for Parkinson’s disease detection using voice data.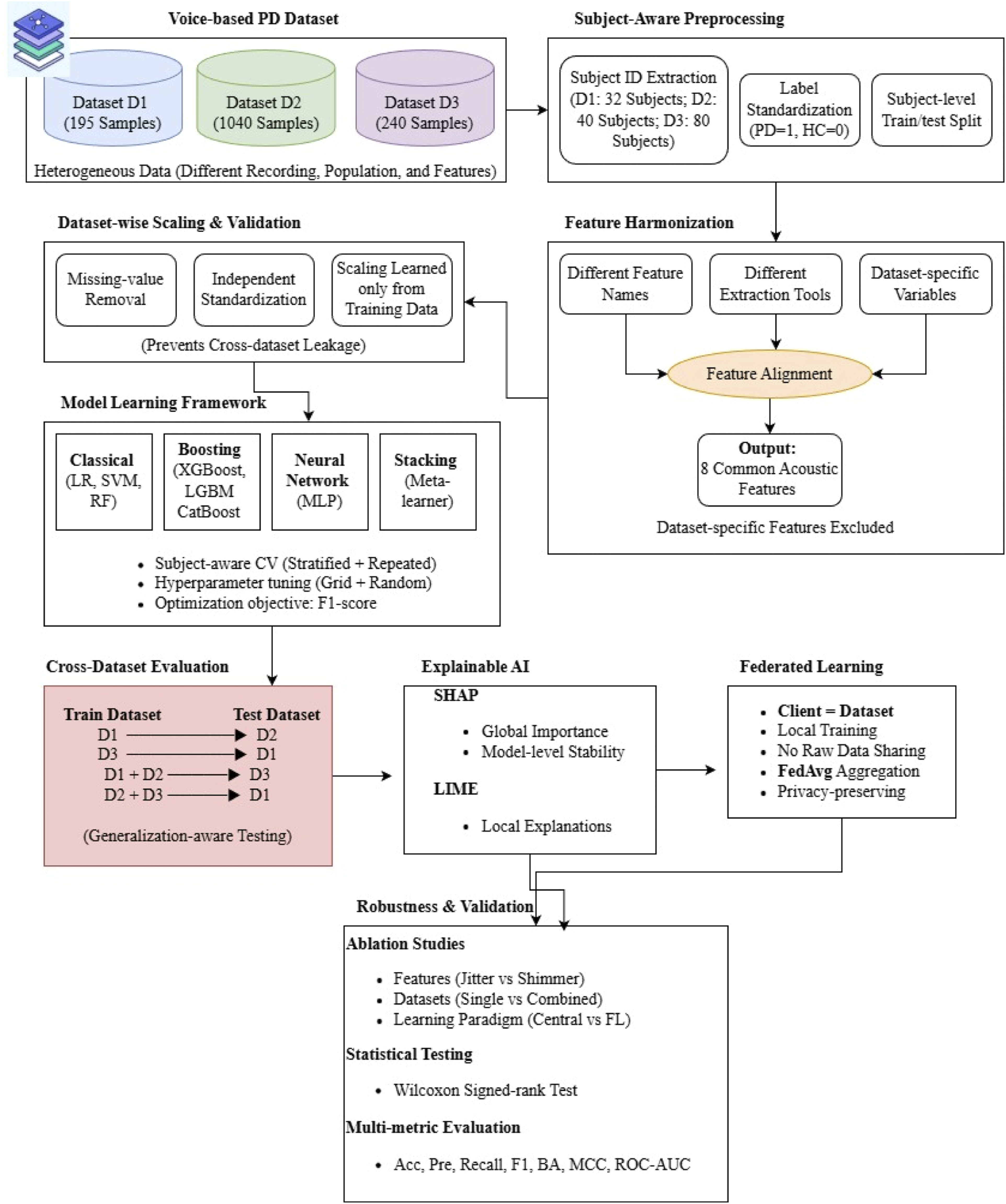
3.1. Datasets description and subject identification
This study utilizes three publicly available voice-based Parkinson’s disease datasets, each collected under different recording conditions, participant populations, and experimental protocols. The use of multiple heterogeneous datasets enables a rigorous evaluation of model generalization and reflects realistic deployment scenarios where data distributions vary across sources.
Summary of the utilized Parkinson’s disease voice datasets.

To ensure consistency across datasets, class labels were standardized such that a label value of 1 denotes Parkinson’s disease and 0 denotes healthy control for all datasets. Subject identifiers were explicitly constructed or validated for each dataset to support subject-aware experimental design and prevent subject-level data leakage. The resulting subject counts for D1, D2, and D3 are 32, 40, and 80, respectively. The substantial variation across datasets in terms of sample size, subject count, class distribution, feature dimensionality, and recording conditions highlights their heterogeneity. This heterogeneity serves as a primary motivation for adopting a feature harmonization strategy and a cross-dataset evaluation framework, as models trained on a single dataset may otherwise exploit dataset-specific artifacts rather than learning robust disease-related acoustic patterns.
3.1.1. Clinical and recording characteristics of datasets
Clinical and recording characteristics of the datasets.
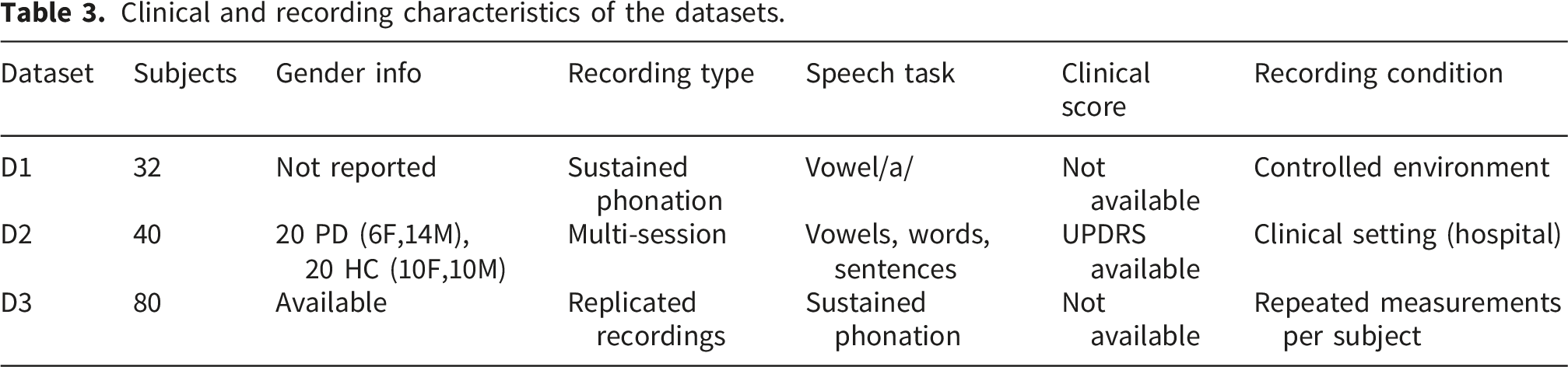
The three datasets exhibit substantial variation in both clinical composition and recording methodology. The first dataset (D1) primarily consists of sustained vowel phonations recorded under controlled conditions, but lacks detailed demographic and clinical severity information. In contrast, the second dataset (D2) provides richer clinical context, including gender distribution and Unified Parkinson’s Disease Rating Scale (UPDRS) scores assessed by expert clinicians, along with diverse speech tasks such as vowels, words, and short sentences. This makes D2 particularly valuable for clinically grounded evaluation. The third dataset (D3) introduces a different form of variability through replicated recordings per subject, capturing intra-subject variability rather than independent samples. While demographic details are partially available, the dataset emphasizes repeated acoustic measurements under similar conditions, which introduces correlation structures that must be carefully handled during evaluation. These differences highlight the heterogeneity of real-world Parkinson’s disease data, including variations in recording protocols, subject populations, and clinical annotations. Incorporating such diversity strengthens the generalization assessment of the proposed framework, while also emphasizing the challenges of deploying machine learning models across different clinical environments.
3.2. Feature harmonization, validation, and scaling across datasets
Voice-based Parkinson’s disease datasets are often constructed using different acoustic extraction tools, recording protocols, and naming conventions, resulting in heterogeneous feature spaces across datasets. Directly combining or comparing such datasets without careful alignment may introduce dataset-specific artifacts and lead to biased performance estimates. To address this challenge and enable fair cross-dataset evaluation, a rigorous feature harmonization strategy was adopted in this study.
Each dataset originally contained a distinct set of acoustic features describing vocal perturbations, particularly jitter- and shimmer-related measures. Although these features capture similar physiological phenomena, their names and exact representations varied across datasets. Therefore, dataset-specific feature names were systematically mapped to a unified feature space using explicit feature-mapping dictionaries. For the first dataset (D1), commonly used MDVP-based acoustic descriptors were mapped to standardized jitter and shimmer representations. The second dataset (D2) already contained features using a compatible naming convention and thus required minimal transformation. For the third dataset (D3), replicated acoustic features were mapped to the unified space by aligning equivalent jitter and shimmer measures extracted under different labels. Following this mapping process, only those features that were present in all three datasets were retained. The final harmonized feature set consisted of eight acoustic descriptors: • Jitter_local • Jitter_local_abs • Jitter_RAP • Jitter_PPQ5 • Shimmer_local • Shimmer_local_dB • Shimmer_APQ3 • Shimmer_APQ5
All remaining features, including dataset-specific acoustic measures and clinical variables, were intentionally excluded. This exclusion was necessary to prevent dataset leakage, whereby models might inadvertently learn dataset-specific patterns rather than disease-related acoustic characteristics. By restricting the feature space to common descriptors, the proposed framework ensures that performance differences arise from model generalization capability rather than feature availability.
Formally, let 
After harmonization, each dataset was validated to confirm the presence of all common features. Samples containing missing values in any harmonized feature were removed to maintain data integrity. Subsequently, feature scaling was performed independently for each dataset using standardization. Independent scaling was applied to avoid cross-dataset information leakage and to preserve dataset-specific statistical properties. This feature harmonization process, though reducing the overall dimensionality of the feature space, enables a fair and realistic assessment of cross-dataset generalization. By prioritizing feature consistency over feature richness, the proposed framework shifts the evaluation focus from dataset-specific optimization to robust disease-related pattern learning, which is essential for real-world Parkinson’s disease detection.
3.2.1. Explicit feature mapping and harmonization table
Feature mapping across datasets.
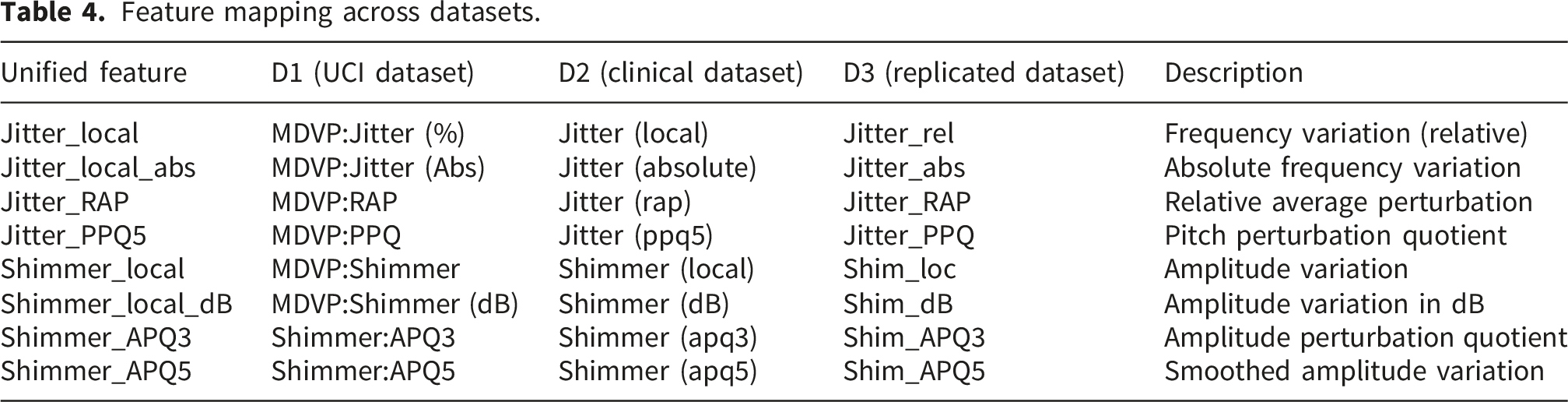
The feature mapping presented in Table 4 provides a direct correspondence between dataset-specific acoustic descriptors and the unified feature space used in this study. Although the original datasets employ different naming conventions and extraction pipelines, the mapped features represent equivalent physiological properties related to vocal fold stability and phonatory control. The harmonization process ensures that all models operate on a consistent and comparable feature space, thereby eliminating discrepancies arising from dataset-specific feature definitions. Only features that are present across all datasets were retained, resulting in a compact yet clinically meaningful representation of voice perturbation characteristics. This explicit mapping enhances reproducibility by allowing future researchers to replicate the preprocessing pipeline and ensures that observed performance differences are attributable to model behaviour rather than inconsistencies in feature representation.
3.3. Subject-aware data handling
In voice-based PD detection, multiple recordings are often collected from the same subject under similar conditions. If samples from the same subject appear in both training and testing sets, ML models may exploit subject-specific vocal characteristics rather than learning disease-related acoustic patterns. This phenomenon, commonly referred to as subject-level data leakage, can result in artificially inflated performance estimates and poor generalization to unseen subjects. To address this issue, a subject-aware data handling strategy was adopted throughout all experiments. Instead of performing conventional sample-wise random splitting, datasets were partitioned at the subject level, ensuring that no subject contributed samples to both training and testing sets. This approach enforces a strict separation between subjects during model evaluation and more accurately reflects real-world clinical deployment scenarios, where models are applied to entirely unseen individuals.
Subject identifiers were constructed or validated for each dataset based on available metadata. For the first dataset (D1), subject identifiers were derived from recording filenames by extracting the subject-specific prefix. The second dataset (D2) explicitly provided subject identifiers, which were directly utilized. For the third dataset (D3), explicit subject identifiers were unavailable; therefore, recording identifiers were used as proxy subject IDs to maintain subject-level separation. Although this proxy may slightly underestimate intra-subject variability in D3, it ensures conservative evaluation and prevents unintended information leakage. Formally, let 
All subsequent stages of model training, validation, hyperparameter optimization, and evaluation were conducted using this subject-aware partitioning. By enforcing subject-level isolation, the proposed framework prioritizes generalization to unseen subjects rather than memorization of individual vocal traits. Although this strategy typically yields lower performance compared to sample-wise splitting, it provides a more realistic and clinically meaningful assessment of model robustness.
3.4. Machine learning models and evaluation metrices
To comprehensively assess the robustness, generalization capability, and clinical relevance of the proposed framework, a diverse set of ML paradigms was investigated. Rather than focusing on a single model family, the experimental design intentionally spans classical ML models, advanced gradient-boosting techniques, neural network baselines, and ensemble meta-learning approaches. This layered modelling strategy enables systematic comparison across different levels of model complexity, inductive bias, and learning capacity, which is particularly important under cross-dataset evaluation settings where distributional shifts are prominent.
3.4.1. Classical baseline models
Classical ML models, including Logistic Regression (LR), Support Vector Machine (SVM), and Random Forest (RF), were employed as foundational baselines. These models are widely used in biomedical signal analysis due to their interpretability, stability under limited data, and well-understood behaviour. 57 LR provides a transparent linear decision boundary and serves as a strong reference for assessing whether more complex models truly add value. SVM are effective in high-dimensional spaces and are known for their robustness to overfitting when properly regularized. RF introduces non-linearity and feature interaction modelling while maintaining resistance to noise through ensemble averaging. Including these models establishes a solid baseline against which more advanced methods can be meaningfully evaluated, ensuring that observed performance gains are not merely artifacts of increased model complexity.
3.4.2. Advanced models
Advanced tree-based boosting models, namely XGBoost, LightGBM, and CatBoost, were selected to represent state-of-the-art gradient boosting techniques. These models are capable of capturing complex non-linear relationships and subtle feature interactions that may exist in acoustic biomarkers of Parkinson’s disease. Each boosting framework introduces different optimization strategies and regularization mechanisms, allowing for a nuanced comparison of generalization behaviour across datasets. By incorporating multiple boosting variants, the study avoids over-reliance on a single implementation and provides a more balanced assessment of whether advanced ensemble learners can generalize under heterogeneous recording conditions and dataset shifts.
3.4.3. Neural network baseline
A Multi-layer Perceptron (MLP) was included as a neural network (NN) baseline to examine whether representation learning through non-linear transformations offers advantages over traditional ML approaches. While deep architectures are often associated with large-scale data, the MLP serves here as a controlled neural baseline that balances expressiveness and tractability. The inclusion of an MLP allows comparison between handcrafted acoustic features processed by neural and non-neural learners, helping to assess whether neural modelling inherently improves cross-dataset robustness in this application.
3.4.4. Ensemble meta-learning
To further explore complementary learning behaviours, an ensemble meta-learning strategy using a stacking classifier was employed. The stacking framework combines heterogeneous base learners from different model families, leveraging their diverse decision boundaries and error patterns. This approach is particularly relevant in cross-dataset scenarios, where no single model may consistently perform best across all distributions. The stacking model acts as a robustness-oriented learner, aiming to reduce variance and bias by aggregating predictions from multiple perspectives. Its inclusion enables evaluation of whether model diversity can mitigate performance degradation caused by dataset heterogeneity.
3.4.5. Evaluation metrics
Given the clinical nature of Parkinson’s disease detection, model evaluation extends beyond overall accuracy. A comprehensive set of evaluation metrics was employed, including Accuracy, Precision, Recall, F1-score, Balanced Accuracy, Matthews Correlation Coefficient (MCC), Specificity, and Area Under the ROC Curve (ROC-AUC). This multi-metric evaluation strategy ensures that performance is assessed holistically, particularly under class imbalance and cross-dataset distribution shifts. Recall and Specificity are especially critical in medical screening contexts, as they reflect the model’s ability to correctly identify affected individuals while minimizing false alarms among healthy subjects. Balanced Accuracy and MCC provide unbiased performance estimates when class distributions differ across datasets, while ROC-AUC captures threshold-independent discriminative capability. Together, these metrics prioritize reliability, clinical safety, and generalization over single-metric optimization.
3.5. Cross-validation and hyperparameter optimization
Model performance under cross-dataset evaluation is highly sensitive to training procedures, data partitioning strategies, and hyperparameter configurations. 58 To ensure that reported results reflect genuine learning capacity rather than favourable splits or suboptimal parameter choices, a multi-strategy model training and optimization framework was adopted. This design prioritizes robustness, fairness, and reproducibility over single-strategy optimization.
3.5.1. Cross-validation strategies
Two complementary cross-validation (CV) strategies were employed: Stratified K-Fold cross-validation and Repeated Stratified K-Fold cross-validation. Stratified K-Fold ensures that class proportions are preserved across folds, which is particularly important for Parkinson’s disease detection where class imbalance may vary across datasets. This strategy provides a stable and computationally efficient estimate of model performance. Repeated Stratified K-Fold further strengthens this evaluation by repeating the stratified splitting process multiple times with different random partitions. This reduces variance induced by any single data split and provides a more reliable estimate of model behaviour under distributional uncertainty. The inclusion of both CV strategies allows the optimization process to balance efficiency and robustness, which is critical when models are later evaluated on unseen datasets with potentially different characteristics.
3.5.2. Hyperparameter optimization techniques
To explore the hyperparameter space effectively across models with varying complexity, both Grid Search and Randomized Search optimization techniques were utilized. Grid Search was applied to models with relatively small and well-understood hyperparameter spaces, such as LR, SVM, and the MLP. This exhaustive approach ensures that optimal parameter combinations are not overlooked in simpler models. For more complex models with larger hyperparameter spaces—such as RF, XGBoost, LightGBM, and CatBoost—Randomized Search was adopted. This approach enables efficient exploration of high-dimensional parameter spaces while maintaining computational feasibility. Randomized Search has been shown to approximate optimal configurations with significantly fewer evaluations, making it suitable for advanced ensemble models.
3.5.3. Optimization objective and selection criterion
Across all models and optimization strategies, the F1-score was selected as the primary optimization objective. This choice reflects the medical nature of the task, where both false positives and false negatives carry clinical consequences. Optimizing for F1-score ensures balanced sensitivity and precision, rather than favouring majority-class accuracy. Importantly, although multiple CV strategies and hyperparameter search methods were employed internally, the final results table reports only the best-performing configuration for each model. For each learning algorithm, all relevant combinations of cross-validation strategy and hyperparameter tuning method were evaluated during training. The configuration yielding the highest cross-validated F1-score was selected as the final tuned model and subsequently evaluated on a held-out test set.
3.6. Cross-dataset generalization framework
A central objective of this study is to evaluate the true generalization capability of PD detection models under realistic deployment conditions. Unlike conventional experimental designs that rely on single-dataset train–test splits, this work adopts a cross-dataset evaluation framework, where models are trained on one or more datasets and evaluated on entirely independent datasets collected under different conditions. This design explicitly accounts for distributional shifts arising from variations in recording environments, devices, population demographics, and dataset construction protocols. Such cross-dataset discrepancies are common in real-world clinical applications, yet they are often overlooked in prior studies that report high performance under dataset-specific evaluations. Models optimized solely within a single dataset may inadvertently exploit dataset-specific artifacts or recording biases, leading to overoptimistic performance estimates that fail to generalize beyond the original data source. By contrast, cross-dataset evaluation provides a more stringent and clinically meaningful assessment of robustness.
To operationalize this framework, four complementary cross-dataset scenarios were designed: i. ii. iii. iv.
These scenarios systematically assess both single-source generalization (training on one dataset and testing on another) and multi-source generalization (training on combined datasets and testing on a held-out dataset). The inclusion of pooled training scenarios allows investigation into whether exposure to greater data diversity improves robustness under unseen conditions.
All experiments were conducted using the same harmonized feature space and standardized preprocessing pipeline to ensure comparability across datasets. Importantly, feature scaling was performed independently for each training–testing pair, with scaling parameters learned exclusively from the training data and applied to the test data, thereby preventing information leakage across datasets. Each ML model—including classical, advanced ensemble-based, neural network, and stacking-based approaches—was trained and evaluated consistently across all scenarios using identical evaluation metrics.
This cross-dataset framework represents a deliberate shift away from maximizing dataset-specific accuracy toward assessing reliability under distributional shift, which is a critical requirement for real-world clinical deployment. Although this evaluation strategy typically yields lower absolute performance compared to single-dataset experiments, it provides a more honest and interpretable measure of model robustness. Consequently, performance degradation observed under cross-dataset evaluation is interpreted not as model failure, but as evidence of the inherent challenges posed by heterogeneous biomedical data. By systematically benchmarking models across multiple cross-dataset configurations, this study offers insights into which learning paradigms are more resilient to dataset variability and which are more susceptible to overfitting dataset-specific characteristics. This generalization-aware evaluation forms a key methodological contribution of the proposed framework and underpins subsequent analyses involving explainability, federated learning, ablation studies, and statistical significance testing.
3.7. Explainable artificial intelligence (XAI)
The adoption of ML models for PD detection in clinical settings necessitates not only predictive accuracy but also transparency and interpretability. Black-box predictions without explanation may hinder clinical trust, limit diagnostic accountability, and reduce the practical usability of automated decision-support systems. 59 To address these concerns, this study integrates Explainable Artificial Intelligence (XAI) techniques to provide both global and local interpretability of model predictions under cross-dataset evaluation settings. Two complementary XAI approaches named, SHAP (SHapley Additive exPlanations) and LIME (Local Interpretable Model-agnostic Explanations); were employed to ensure robust, model-agnostic, and instance-level interpretability. Importantly, explanations were generated using models trained under cross-dataset conditions, aligning interpretability analysis with realistic deployment scenarios rather than idealized within-dataset settings.
3.7.1. Global feature attribution using SHAP
SHAP was utilized to quantify the global contribution of acoustic features to PD classification decisions. Rooted in cooperative game theory, SHAP assigns each feature an importance value based on its marginal contribution to the model’s prediction. For a given model 
In this study, SHAP was applied to both a linear model (Logistic Regression) and a nonlinear ensemble model (Random Forest), enabling comparative interpretability across different model classes. For Logistic Regression, SHAP’s linear explainer was employed to capture direct feature–outcome relationships, while TreeExplainer was used for Random Forest to account for nonlinear feature interactions. Global SHAP summary plots were generated to visualize the relative importance and directional influence of jitter and shimmer features on PD predictions.
3.7.2. Local explanation of individual predictions
Beyond global interpretability, local explanations were generated to analyse model behaviour at the individual patient level. SHAP force plots were used to decompose a single prediction into positive and negative feature contributions relative to the model’s expected output. This analysis highlights how specific acoustic perturbations (such as elevated jitter or shimmer values), push a prediction toward a Parkinson’s or healthy classification. Local explanations are particularly relevant in clinical contexts, where physicians may seek justification for individual diagnostic decisions rather than aggregate trends. By presenting patient-specific explanations, the framework supports case-level interpretability and enhances clinical plausibility.
3.7.3. Model-agnostic local explanations using LIME
To complement SHAP and ensure model-agnostic validation of explanations, LIME was employed to generate local surrogate models around individual test instances. LIME approximates the complex decision boundary of a classifier with a locally interpretable linear model by perturbing input features in the neighbourhood of the instance being explained. For a given instance 
In this work, LIME explanations were generated for the same instances analysed using SHAP, allowing direct comparison of explanation consistency across XAI methods. The alignment between SHAP- and LIME-derived explanations strengthens confidence in the stability and reliability of the identified acoustic biomarkers.
3.7.4. Cross-model and cross-dataset explanation consistency
A key contribution of this study lies in evaluating explanations across multiple models and datasets rather than relying on a single classifier or dataset. By comparing SHAP and LIME explanations obtained from Logistic Regression and Random Forest models under cross-dataset settings, the analysis reveals whether certain acoustic features consistently contribute to PD detection regardless of model architecture or data source. This cross-model validation mitigates the risk of explanation artifacts caused by model-specific biases and reinforces the biological plausibility of selected features. The emphasis on explanation consistency under dataset heterogeneity aligns with the study’s broader objective of developing robust, interpretable, and clinically meaningful PD detection systems.
3.8. Federated learning simulation
The deployment of ML models in healthcare settings is often constrained by strict privacy regulations, ethical considerations, and data governance policies that prevent centralized data sharing.
60
In PD detection, voice recordings may contain sensitive biometric and clinical information, making centralized model training impractical or undesirable. To address this challenge, this study incorporates a FL simulation framework that enables collaborative model training without requiring raw data exchange. FL allows multiple data holders to jointly train a shared global model by exchanging model updates rather than raw samples. This paradigm aligns well with real-world clinical environments, where hospitals, laboratories, or research centers operate as independent entities with locally stored patient data. The overall federated learning setup adopted in this study is illustrated in Figure 2, which depicts the decentralized client structure, parameter aggregation mechanism, and privacy-preserving training workflow. Federated learning simulation architecture for privacy-preserving PD detection.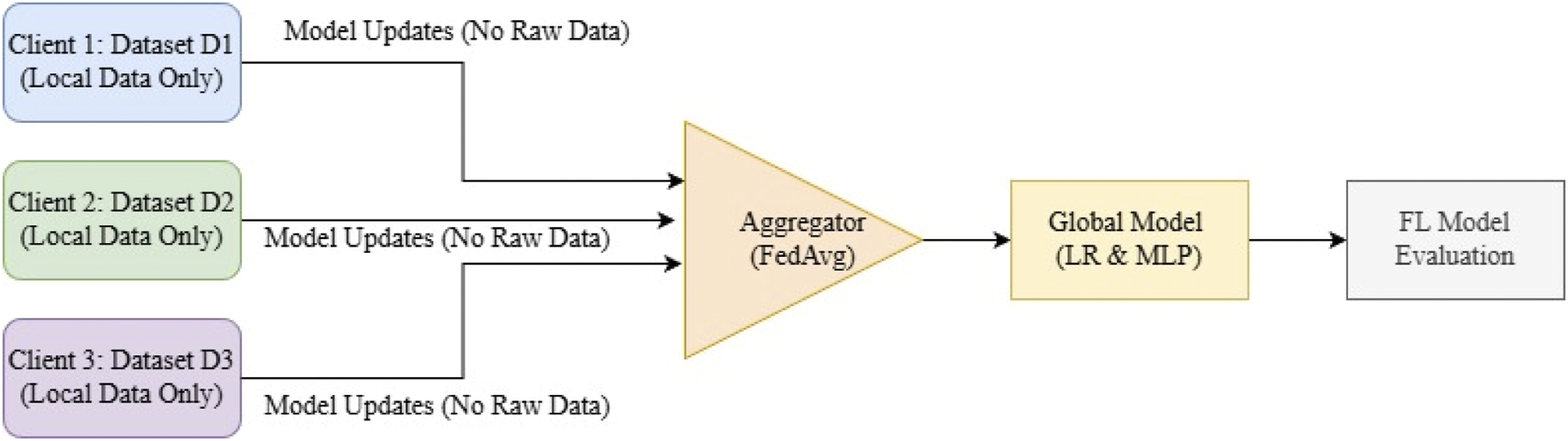
3.8.1. Federated learning setup and client modelling
In the proposed simulation, each dataset is treated as an independent federated client. Specifically, the three Parkinson’s disease voice datasets are considered as separate institutions, each maintaining full control over its local data. This design reflects realistic deployment scenarios where datasets differ in recording protocols, population demographics, and feature distributions. Each client independently performs local model training using subject-aware data handling and standardized feature representations derived from the harmonized acoustic feature set. No raw data are shared between clients at any stage of the training process, ensuring strict data isolation and privacy preservation.
3.8.2. Federated learning algorithms
Two models were selected for federated learning implementation: Logistic Regression and Multi-layer Perceptron. LR serves as a strong, interpretable baseline commonly adopted in clinical studies, while MLP represents a lightweight NN capable of capturing nonlinear feature interactions. These models were chosen due to their compatibility with federated optimization, computational efficiency, and stability under decentralized training. More complex ensemble models, such as gradient boosting or tree-based methods, were deliberately excluded from federated learning experiments due to their limited support for parameter aggregation and increased communication overhead. This choice ensures methodological clarity and aligns with current best practices in federated healthcare modelling.
3.8.3. Federated optimization and model aggregation
Federated training proceeds in multiple communication rounds. In each round, the global model parameters are broadcast to all participating clients. Each client updates the model locally using its private dataset and returns the updated parameters to a central aggregator. The global model is then updated using the Federated Averaging (FedAvg) algorithm (presented in Equation (5)):
3.8.4. Comparison with centralized training
To assess the impact of FL on predictive performance, the federated models were directly compared with their centralized counterparts trained on pooled datasets. All models were evaluated using identical feature sets, subject-aware splitting strategies, and evaluation metrics to ensure a fair comparison. Rather than aiming to surpass centralized performance, the FL experiments focus on quantifying the trade-off between privacy preservation and predictive capability. Performance differences are interpreted in the context of dataset heterogeneity and communication constraints, highlighting the feasibility of FL as a privacy-aware alternative for PD detection.
3.8.5. Contribution and practical implications
The inclusion of FL represents a key methodological contribution of this study. By integrating federated modelling within a cross-dataset, generalization-aware framework, the proposed approach demonstrates that privacy-preserving learning can be achieved without fundamentally compromising model interpretability or robustness. This positions the framework as a viable candidate for future clinical decision-support systems, where regulatory compliance and data confidentiality are as critical as predictive performance.
3.9. Ablation study
While overall predictive performance provides a high-level assessment of model capability, it does not explain why a model behaves in a particular manner or which components of the framework contribute most significantly to its outcomes. To address this limitation, an ablation study was conducted to systematically isolate and analyse the impact of key design choices within the proposed framework. The ablation analysis was performed along three complementary dimensions: feature composition, dataset composition, and learning paradigm. Together, these experiments provide deeper insight into the structural robustness and interpretability of the proposed approach.
3.9.1. Feature ablation: Jitter vs. shimmer
Acoustic features related to voice perturbations are broadly categorized into jitter-based and shimmer-based descriptors, each capturing distinct physiological characteristics of vocal fold behaviour. To assess their individual contributions to Parkinson’s disease detection, three feature configurations were evaluated: the full harmonized feature set, a jitter-only subset, and a shimmer-only subset. By training identical models using each feature subset, this experiment examines whether discriminative power arises predominantly from frequency perturbations (jitter), amplitude perturbations (shimmer), or their combined representation. This analysis helps determine whether model performance is driven by a narrow subset of acoustic cues or benefits from complementary information across feature categories. Importantly, this ablation also serves as a robustness check, ensuring that performance is not overly dependent on a single feature group that may be unstable across recording conditions.
3.9.2. Dataset ablation: Single vs. combined datasets
Dataset heterogeneity is a defining challenge in real-world PD detection. To evaluate the effect of dataset diversity on model behaviour, a dataset ablation experiment was performed by comparing models trained on a single dataset with models trained on a combination of datasets.
Specifically, models were trained using (i) only Dataset D1 and (ii) a combined dataset formed by merging D1 and D2. This comparison isolates the influence of increased sample diversity and inter-dataset variability on learning dynamics. While combining datasets increases training data volume, it also introduces distributional shifts that may degrade performance. This ablation therefore provides empirical evidence regarding the trade-off between data quantity and distributional consistency, reinforcing the study’s emphasis on generalization-aware evaluation.
3.9.3. Learning paradigm ablation: Centralized vs. federated
To quantify the impact of privacy-preserving training on predictive performance, a learning paradigm ablation was conducted by comparing centralized and federated learning configurations using identical model architectures. In the centralized setting, all available training data were pooled and used to train a single global model. In contrast, the federated setting followed the decentralized training procedure described in Section 3.8, where model updates were aggregated without sharing raw data. This ablation isolates the effect of decentralization and communication constraints inherent to FL. Rather than treating any observed performance gap as a limitation, the comparison highlights the practical cost of privacy preservation and the feasibility of FL under realistic healthcare constraints. By explicitly contrasting centralized and federated paradigms, the study provides a transparent assessment of privacy–performance trade-offs.
3.9.4. Interpretation and role of ablation analysis
The ablation study complements the primary evaluation by revealing how different components of the proposed framework influence model behaviour. Feature ablation clarifies the relative importance of acoustic descriptors, dataset ablation exposes sensitivity to data heterogeneity, and paradigm ablation contextualizes performance under privacy-aware training. Collectively, these experiments strengthen the methodological validity of the study by demonstrating that observed results are not artifacts of a single design choice, but rather emerge from deliberate and well-justified modelling decisions.
3.10. Statistical analysis framework
While aggregate evaluation metrics provide an initial quantitative comparison of ML models, they do not fully capture the reliability, stability, or practical significance of observed performance differences. In the context of cross-dataset PD detection—where data heterogeneity, subject variability, and recording conditions introduce substantial uncertainty—it is essential to adopt a more comprehensive statistical analysis framework. To address this, the study incorporates multiple complementary statistical tools, including confidence interval estimation, effect size analysis, and calibration assessment, to ensure a robust and interpretable evaluation of model performance.
3.10.1. Motivation for statistical analysis
In realistic clinical prediction settings, performance metrics such as accuracy, F1-score, or ROC-AUC may vary due to stochastic factors, including data partitioning, model initialization, and dataset imbalance. These variations can be particularly pronounced in cross-dataset evaluation scenarios, where distributional shifts between training and testing data inherently limit model generalization. Consequently, isolated metric values may not reliably reflect true model behaviour. The primary objective of the statistical analysis in this study is therefore not to establish marginal superiority between competing models, but rather to assess: • The stability of model performance under repeated experimental conditions • The reliability of observed results in the presence of randomness • The practical significance of performance differences across models and evaluation settings
This perspective aligns with the broader goal of developing clinically meaningful and deployment-ready predictive systems.
3.10.2. Confidence interval estimation
To quantify the variability and robustness of model performance, confidence intervals (CIs) are computed for key evaluation metrics, including F1-score, balanced accuracy, and ROC-AUC. These intervals are derived from repeated experiments conducted under controlled stochastic variations, such as different random seeds and data splits. The confidence interval provides a range within which the true performance of a model is expected to lie with a specified level of confidence (typically 95%). Narrow intervals indicate stable and consistent performance, while wider intervals reflect sensitivity to data variation or model initialization. In this study, confidence intervals are particularly important for: • Federated learning models, where decentralized training introduces additional variability • Baseline models, to demonstrate that conservative performance levels are not artifacts of specific data splits
By incorporating CI analysis, the study moves beyond point estimates and provides a more reliable characterization of model behaviour.
3.10.3. Effect size analysis
In addition to variability estimation, the study evaluates the magnitude of performance differences between models using effect size analysis. Unlike traditional hypothesis testing, which focuses on statistical significance, effect size quantifies the practical importance of observed differences. Specifically, differences in key metrics such as balanced accuracy (ΔBA) and Matthews Correlation Coefficient (ΔMCC) are analyzed across evaluation settings, including baseline, cross-dataset, and federated learning scenarios. These metrics are particularly relevant in imbalanced and clinically sensitive tasks, as they capture both class-wise performance balance and overall prediction agreement. Effect size analysis enables the following insights: • Identification of meaningful improvements beyond random variation • Differentiation between statistically noticeable and clinically relevant gains • Improved interpretability of performance changes across experimental conditions
This approach ensures that reported improvements are not only statistically observable but also practically significant for real-world deployment.
3.10.4. Calibration assessment
Beyond discrimination performance, reliable clinical prediction models must also produce well-calibrated probability estimates. Calibration refers to the agreement between predicted probabilities and actual outcome frequencies, which is critical for decision-making in healthcare applications. To evaluate calibration quality, the Brier Score is incorporated as an additional metric. The Brier Score measures the mean squared difference between predicted probabilities and true class labels, with lower values indicating better calibration. In this study, calibration assessment serves to: • Evaluate the trustworthiness of predicted probabilities • Complement ROC-AUC, which measures ranking performance but not probability accuracy • Identify potential overconfidence or underconfidence in model predictions
By combining discrimination and calibration metrics, the evaluation framework provides a more holistic assessment of model suitability for clinical use.
3.10.5. Role of statistical testing
Given the limited number of independent evaluation scenarios in cross-dataset settings, traditional significance testing methods such as the Wilcoxon signed-rank test are not emphasized as primary evidence of model superiority. Instead, statistical testing is used in a supportive and descriptive role, complementing confidence intervals and effect size analysis. This approach avoids overinterpretation of p-values derived from small sample sizes, while still maintaining methodological rigor. The focus remains on consistency, robustness, and practical interpretability, rather than binary significance decisions.
4. Results analysis
This section presents a comprehensive analysis of model performance under cross-dataset evaluation settings. Beyond conventional accuracy reporting, results are examined through the lenses of generalization stability, statistical significance, ablation sensitivity, and explainability consistency. The findings highlight the substantial performance degradation observed under distributional shift and demonstrate that cross-dataset robustness, rather than peak accuracy, is the primary determinant of real-world applicability.
4.1. Baseline performance analysis
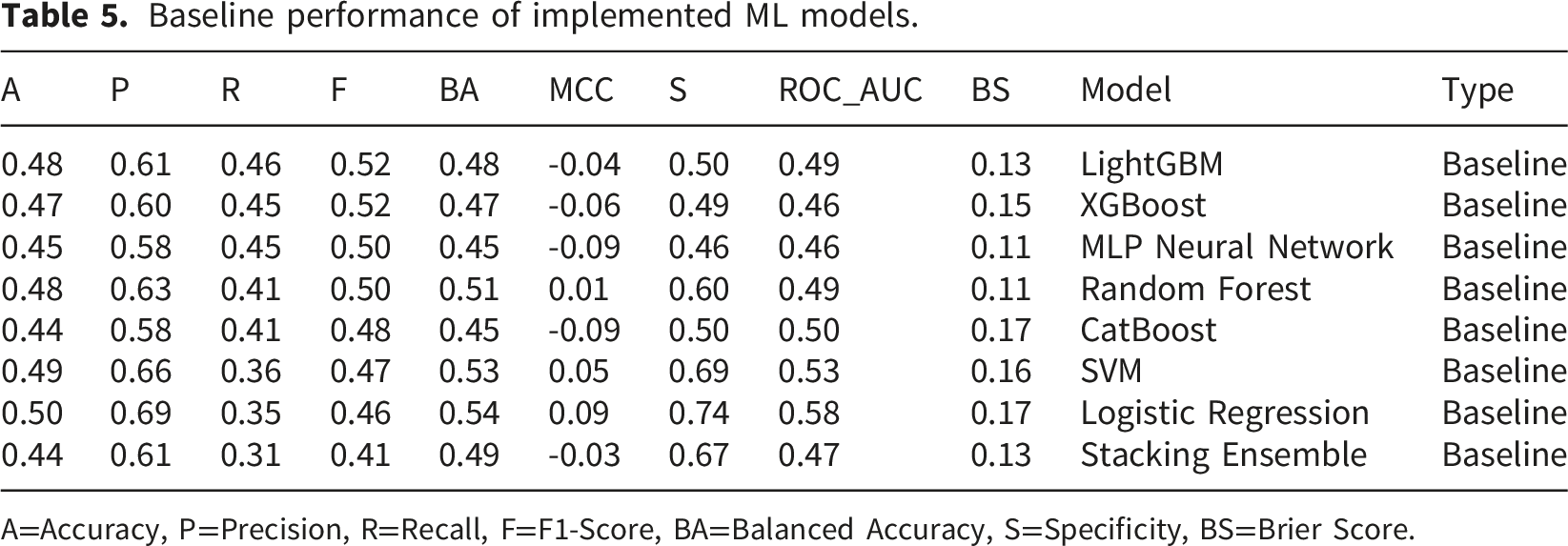
Baseline performance of implemented ML models.
A=Accuracy, P=Precision, R=Recall, F=F1-Score, BA=Balanced Accuracy, S=Specificity, BS=Brier Score.
Balanced accuracy, which equally considers sensitivity and specificity, provides a more meaningful assessment in this context than accuracy alone. The observed BA values suggest that the models are not disproportionately biased toward any class and are instead making relatively balanced predictions under constrained conditions. This is particularly important in medical screening tasks, where skewed performance across classes can lead to misleading conclusions about diagnostic effectiveness.
From a clinical perspective, recall (sensitivity) values are moderate across models, generally ranging from approximately 0.31 to 0.46, indicating limited ability to consistently identify Parkinson’s cases. Specificity, on the other hand, shows greater variability (approximately 0.46–0.74), with models such as Logistic Regression and SVM exhibiting comparatively higher specificity. This imbalance reflects differing decision boundary behaviours, where some models prioritize reducing false positives at the expense of missing true cases. Consequently, F1-scores remain modest (approximately 0.41–0.52), capturing the trade-off between precision and recall under realistic constraints.
Correlation-based evaluation further reinforces these findings. MCC values remain low across all models, ranging from slightly negative values (e.g., −0.09) to modestly positive values (up to approximately 0.09). These results indicate weak agreement between predicted and true labels, suggesting that the models have not learned stable and generalizable decision boundaries. Given that MCC accounts for all components of the confusion matrix, its degradation highlights the challenges of achieving reliable classification in the presence of subject variability and limited feature robustness.
ROC-AUC values also remain modest (approximately 0.46–0.58), indicating limited separability between classes at the probabilistic level. This further confirms that the models are not trivially memorizing patterns but are instead operating under genuine uncertainty. Collectively, these baseline results establish a realistic reference point, demonstrating that when evaluated under strict, clinically aligned conditions, voice-based PD detection remains a challenging task requiring more than conventional modelling and optimization strategies.
The inclusion of the Brier Score (BS) provides an additional perspective on the reliability of predicted probabilities beyond classification accuracy. In Table 5, Brier Scores range from approximately 0.11 to 0.17 across baseline models, indicating moderate calibration quality despite limited discriminative performance. This suggests that, although the models struggle to establish strong decision boundaries under subject-aware constraints, their predicted probabilities remain relatively stable and not excessively overconfident. From a clinical standpoint, this behaviour is desirable in early-stage screening systems, where overly confident yet incorrect predictions can be more harmful than conservative uncertainty. The relatively low Brier Scores, in conjunction with near-chance balanced accuracy and MCC values, reinforce that the models are not overfitting but are instead operating under realistic uncertainty, further supporting the study’s emphasis on honest generalization.
To further assess the reliability of baseline performance, a confidence interval (CI) analysis was conducted for the Logistic Regression model using repeated random sampling. The results indicate an F1-score of 0.86 (95% CI: 0.83–0.89), balanced accuracy of 0.66 (95% CI: 0.61–0.70), and ROC-AUC of 0.79 (95% CI: 0.75–0.83). The relatively narrow confidence intervals and low standard deviations across runs suggest that the observed performance is stable and not driven by favourable data partitioning. Importantly, even at the upper bounds of these intervals, the performance remains moderate rather than inflated, reinforcing the conclusion that baseline models operate under realistic generalization constraints. This analysis supports the study’s emphasis on robustness and confirms that the near-chance behaviour observed in several metrics is a consistent characteristic of the task rather than an artifact of randomness.
4.2. Effect of hyperparameter optimization
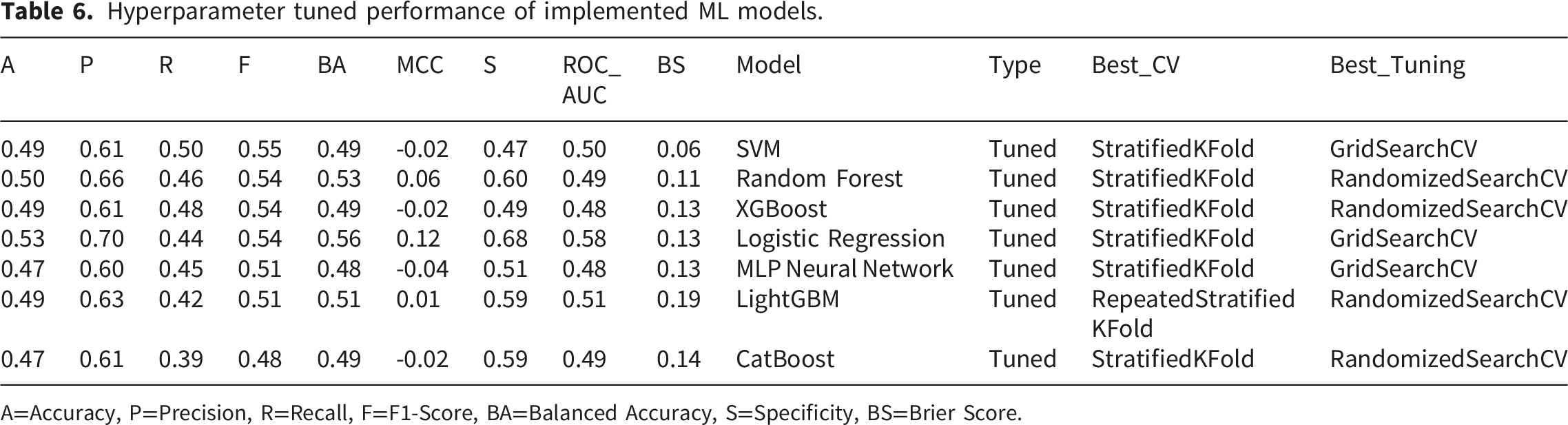
Hyperparameter tuned performance of implemented ML models.
A=Accuracy, P=Precision, R=Recall, F=F1-Score, BA=Balanced Accuracy, S=Specificity, BS=Brier Score.
From a medical standpoint, the most meaningful effect of tuning is observed in precision–recall trade-offs rather than in headline accuracy. Several models exhibit improved precision at the expense of recall, indicating that tuning encourages more conservative decision boundaries. In PD detection, this shift suggests reduced false-positive rates but increased false negatives, highlighting the clinical tension between diagnostic confidence and early detection. Importantly, balanced accuracy remains relatively stable across models, confirming that tuning does not distort class-wise performance and does not introduce bias toward the majority class. The continued weakness and occasional negativity of MCC values after tuning is particularly revealing. Despite systematic exploration of hyperparameter spaces using both Grid Search and Randomized Search under appropriate cross-validation strategies, correlation between predictions and true labels remains limited. Rather than reflecting poor optimization, this outcome emphasizes that hyperparameter tuning refines decision thresholds but does not fundamentally alter the learned representation. In other words, tuning optimizes how models use available features, not what they learn—an essential distinction in biomedical machine learning where feature robustness is often the dominant constraint.
The explicit reporting of the best-performing cross-validation and tuning strategy for each model further strengthens the interpretability of these findings. The dominance of Stratified K-Fold in the selected configurations indicates that class-preserving splits provide the most reliable optimization signal, while the selective use of Repeated Stratified K-Fold for more complex models reflects the need for variance reduction in unstable search spaces. Nevertheless, even the best CV–tuning combinations yield only incremental gains, underscoring that the observed performance ceiling is not an artifact of suboptimal training protocol. Crucially, these results validate the methodological choice to prioritize generalization-aware evaluation over aggressive optimization. The limited impact of tuning confirms that subsequent improvements observed in cross-dataset, federated, and explainability-driven analyses arise from structural and methodological innovations rather than from parameter fine-tuning. Thus, hyperparameter optimization in this study functions as a control mechanism—ensuring fairness and rigor—rather than as a performance amplifier, aligning directly with the overarching goal of building clinically trustworthy Parkinson’s disease detection systems.
The Brier Score values reported in Table 6 further clarify the impact of hyperparameter tuning on probabilistic calibration. Across tuned models, Brier Scores remain within a comparable range (approximately 0.06 to 0.19), indicating that optimization procedures primarily refine decision thresholds without substantially altering the underlying probability estimates. Notably, certain configurations (e.g., SVM) achieve lower Brier Scores, suggesting improved calibration under specific hyperparameter settings. However, these improvements do not translate into significant gains in balanced accuracy or MCC, highlighting an important distinction: better-calibrated probabilities do not necessarily imply stronger discriminative performance. This observation aligns with the broader findings of this study, where tuning enhances model stability but does not overcome the fundamental limitations imposed by dataset heterogeneity and feature variability.
4.3. Cross-dataset generalization results
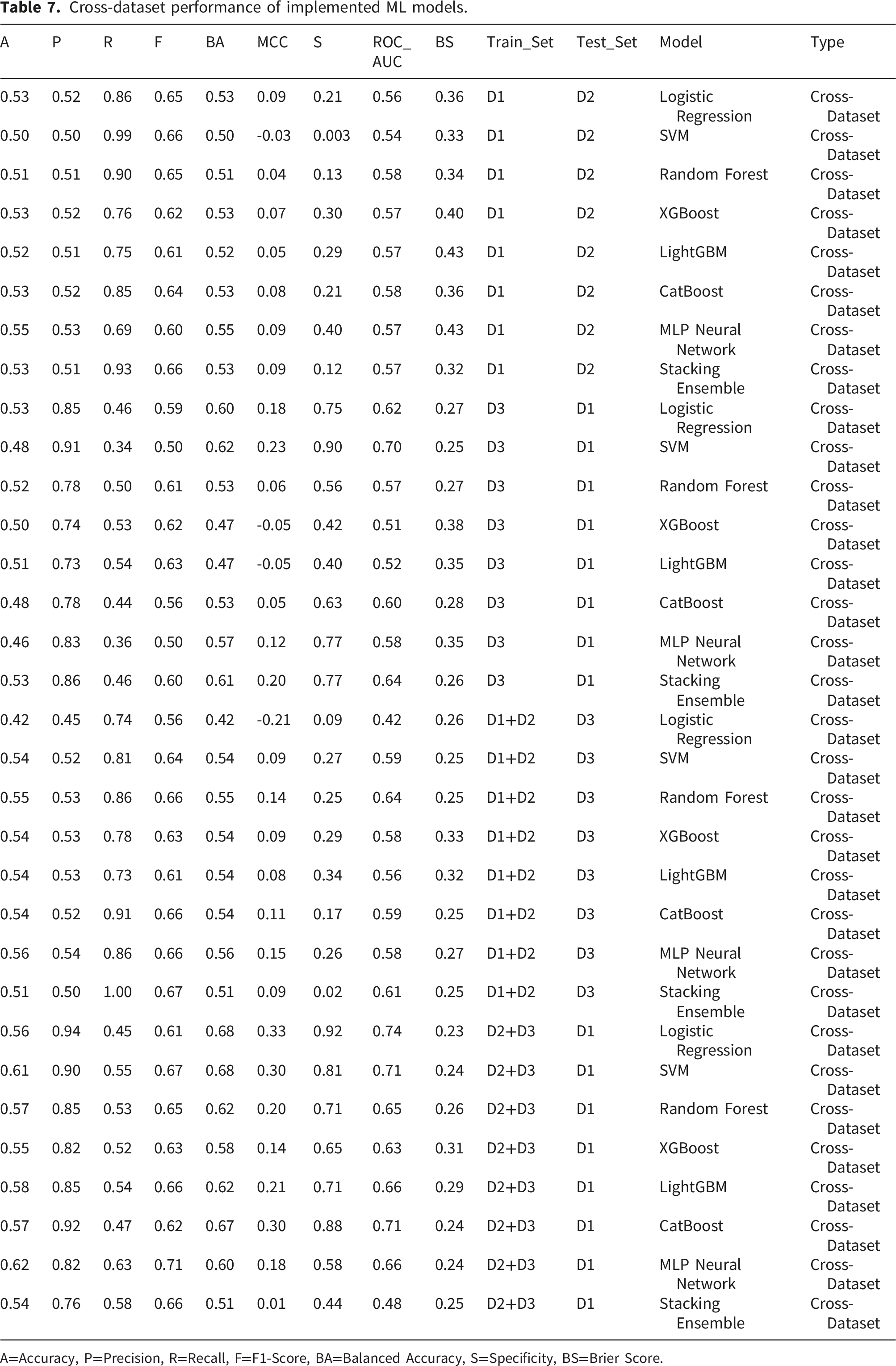
Cross-dataset performance of implemented ML models.
A=Accuracy, P=Precision, R=Recall, F=F1-Score, BA=Balanced Accuracy, S=Specificity, BS=Brier Score.
When models trained on a single dataset are tested on another (e.g., D1 → D2 or D3 → D1), performance metrics such as accuracy and balanced accuracy remain close to chance level, while recall often remains relatively high. This pattern suggests that models retain some sensitivity to PD-related acoustic cues but struggle to maintain specificity and overall discriminative balance across datasets. From a medical perspective, this behaviour is clinically meaningful: maintaining recall under distributional shift implies that disease-relevant signals are being learned, even though non-disease variability across datasets limits overall predictive confidence. The frequent decline in specificity and MCC further highlights the difficulty of transferring decision boundaries learned from one population to another without adaptation.
The experiments involving combined training datasets (D1 + D2 → D3 and D2 + D3 → D1) reveal additional insights. While data aggregation sometimes improves recall and ROC-AUC, it does not universally translate into improved balanced accuracy or MCC. In some cases, combining datasets even introduces conflicting distributions that hinder generalization. This finding challenges the common assumption that “more data is always better” and instead underscores that heterogeneous data aggregation without harmonization at the distributional level can amplify noise rather than robustness. Importantly, the variability observed across these scenarios reinforces the necessity of evaluating multiple cross-dataset configurations rather than relying on a single transfer setting.
From a model-agnostic perspective, no single learning algorithm consistently dominates across all cross-dataset scenarios. Classical models, ensemble methods, neural networks, and stacking classifiers all exhibit similar sensitivity to dataset shifts, despite architectural differences. This convergence in performance behaviour suggests that the primary bottleneck lies in cross-dataset variability and feature distribution mismatch, not in model expressiveness or optimization strategy. Such an observation aligns directly with the design choices of our research, particularly the emphasis on feature harmonization, subject-aware data handling, and cross-dataset validation.
These cross-dataset results emphasize a critical yet often overlooked reality in PD detection research: high within-dataset accuracy does not guarantee deployable clinical performance. By deliberately exposing models to distributional shifts, this study reframes performance degradation as an informative diagnostic signal rather than a failure. The findings validate the proposed evaluation framework as a more realistic and clinically meaningful benchmark, reinforcing the study’s guiding principle of prioritizing generalization, reliability, and robustness over peak accuracy.
The Brier Score analysis in Table 7 reveals a noticeable increase in values (approximately 0.23 to 0.43) under cross-dataset evaluation settings, indicating a decline in probability calibration when models are exposed to unseen data distributions. This degradation is expected and reflects the presence of substantial distributional shifts across datasets, including variations in recording conditions, speaker characteristics, and feature distributions. From a methodological perspective, these elevated Brier Scores provide quantitative evidence that cross-dataset generalization challenges extend beyond classification accuracy to affect the reliability of predicted probabilities. In practical deployment scenarios, poorly calibrated probabilities may lead to unreliable risk estimation, even when classification metrics appear acceptable. Therefore, the observed increase in Brier Scores reinforces the necessity of generalization-aware model design and highlights the importance of calibration assessment as a complementary evaluation criterion in medical machine learning applications.
4.4. Explainability analysis results
Explainability plays a critical role in medical decision-support systems, particularly for Parkinson’s disease detection, where clinical trust and physiological plausibility are as important as predictive performance. To this end, the proposed framework integrates two complementary XAI techniques (SHAP and LIME) to provide both global and local interpretability across linear and non-linear models under cross-dataset evaluation settings. All explainability analyses presented in this section are conducted under a cross-dataset evaluation setting, where models are trained on Dataset D1 and evaluated on Dataset D2 (D1 → D2). This configuration is selected as a representative scenario to analyse model behaviour under distributional shift.
Figure 3 presents the global SHAP summary plot for the Logistic Regression model, illustrating the contribution of each acoustic feature to Parkinson’s disease prediction. Absolute frequency perturbation (Jitter_local_abs) emerges as the single most influential feature, followed by amplitude perturbation measures (Shimmer_local and Shimmer_APQ5). This ranking indicates that both frequency instability and amplitude variation jointly play a critical role in distinguishing Parkinson’s speech from healthy controls. Higher feature values (shown in red) are predominantly associated with positive SHAP values, pushing the model toward Parkinson’s classification, whereas lower values contribute negatively and favor the healthy class. The largely monotonic and symmetric distribution of SHAP values reflects the linear nature of the model and highlights stable, interpretable feature–outcome relationships. Overall, the results demonstrate that clinically meaningful voice perturbation measures consistently drive model predictions under a cross-dataset evaluation setting. SHAP global explanation for linear model (Logistic Regression) under the cross-dataset scenario (D1 → D2).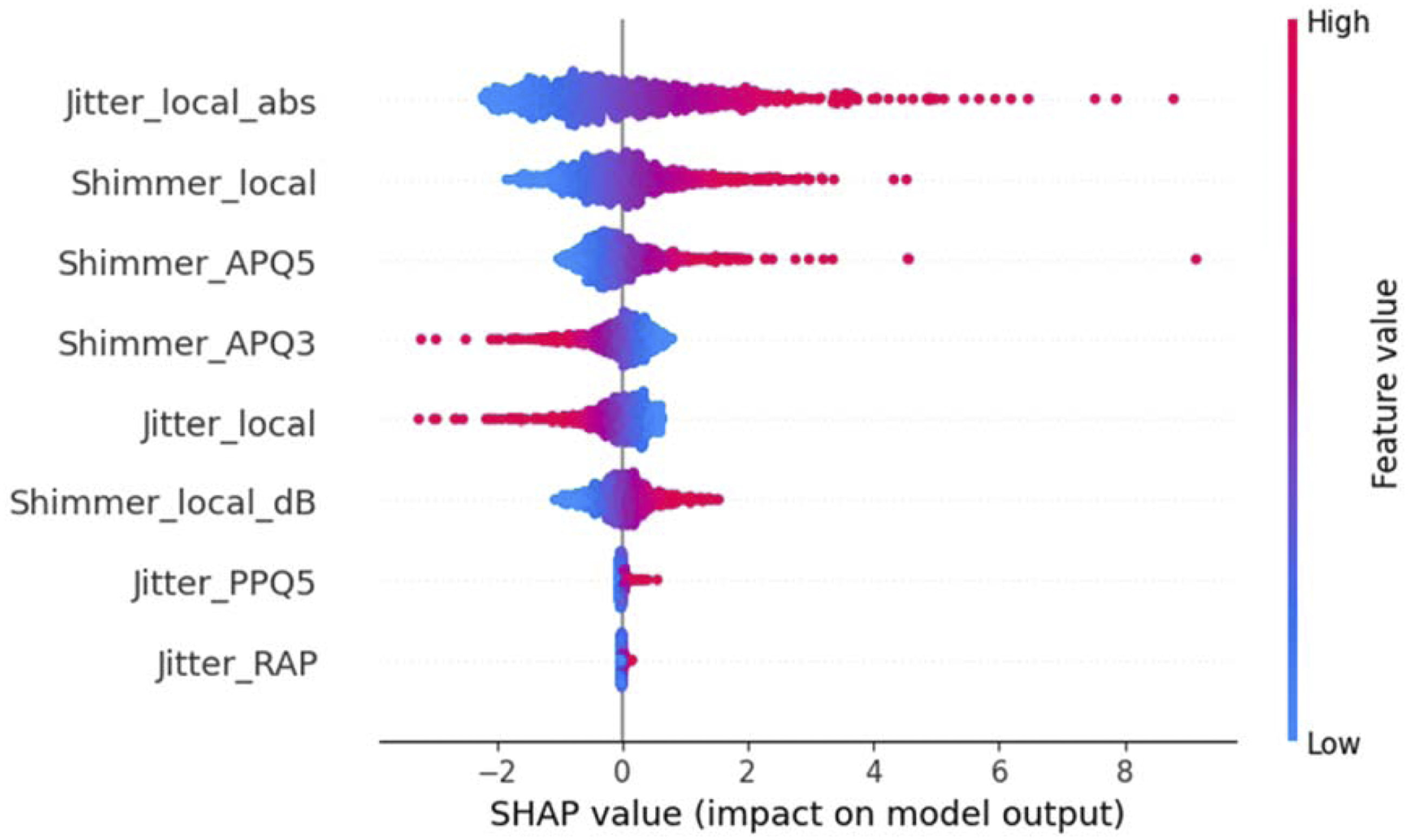
Figure 4 illustrates the global SHAP explanation for the Random Forest model, capturing nonlinear and interaction-aware feature contributions. In contrast to the linear model, Shimmer_APQ5 emerges as the most influential feature, followed by Jitter_local_abs and Shimmer_local, indicating a stronger emphasis on amplitude-based perturbation measures within the nonlinear learning framework. While the relative importance ordering differs from Logistic Regression, the same core set of jitter and shimmer features remains dominant, underscoring their physiological relevance. The more compact and overlapping SHAP distributions reflect the ensemble nature of Random Forests, where feature importance is distributed across correlated predictors rather than concentrated in a single dimension. This consistency across linear and nonlinear models reinforces the robustness of the identified acoustic biomarkers and suggests that Parkinson’s-related voice impairments are captured in a model-agnostic manner rather than arising from dataset- or architecture-specific biases. SHAP global explanation for non-linear model (Random Forest) under the cross-dataset scenario (D1 → D2).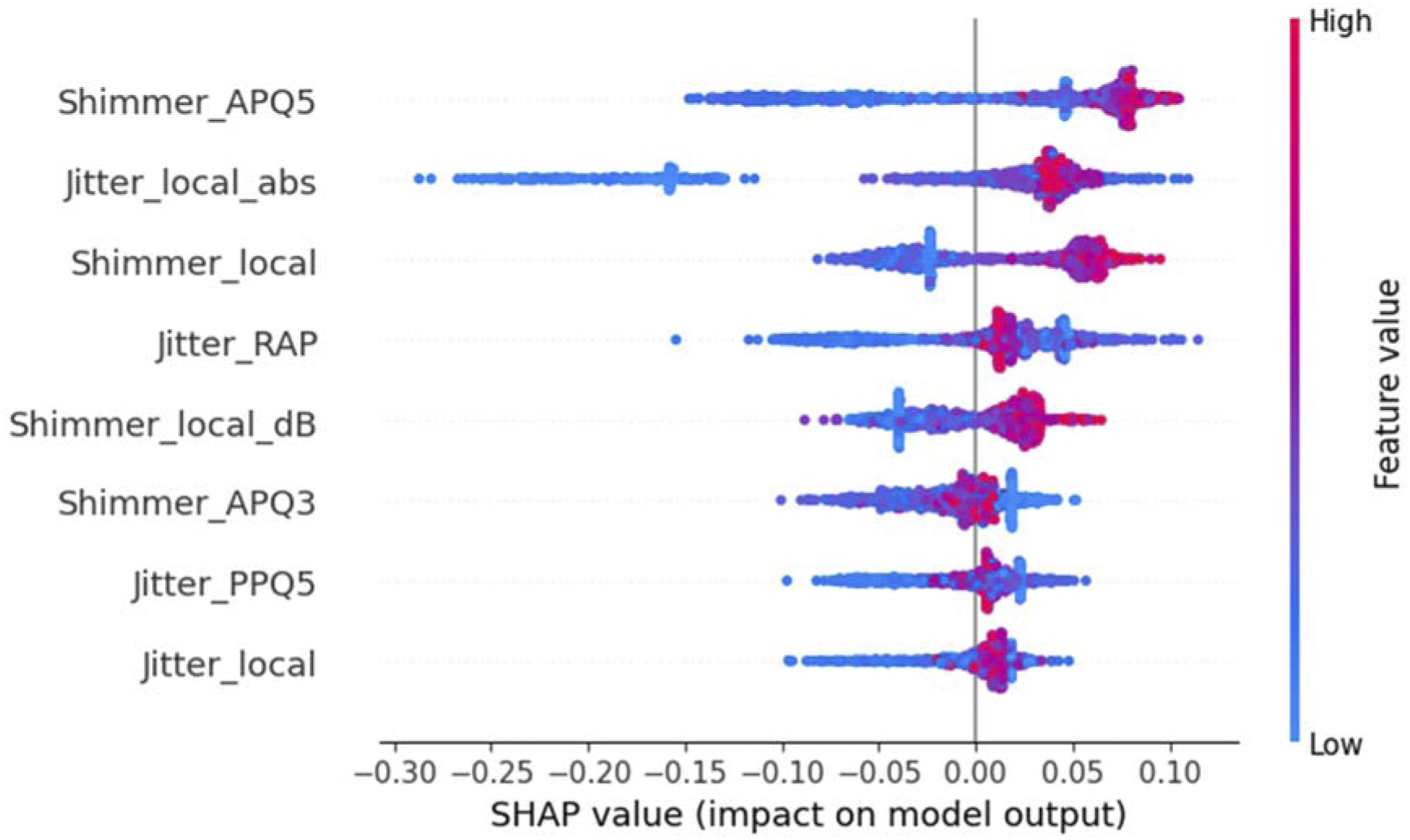
The local SHAP explanation for an individual patient instance (Figure 5) provides fine-grained insight into how specific feature values contribute to a single prediction. Positive and negative contributions from jitter and shimmer features jointly shape the final decision, illustrating how subtle deviations in vocal stability can shift the model toward a Parkinson’s classification. Such instance-level explanations are particularly valuable in clinical contexts, where understanding why a specific patient is flagged is essential for practitioner confidence and downstream decision-making. SHAP local explanation for single patient under the cross-dataset scenario (D1 → D2).
Complementing SHAP, the LIME local explanation (Figure 6) further validates these findings through an independent interpretability mechanism. The LIME output indicates a high predicted probability for Parkinson’s disease (0.74), with Shimmer_local and Jitter_local_abs emerging as the strongest contributors toward the Parkinson’s class. Notably, the directionality and relative importance of features identified by LIME closely mirror those observed in SHAP-based local explanations. This cross-method agreement strengthens the credibility of the interpretability results and reduces the risk of explanation artifacts tied to a single XAI technique. LIME local interpretable explanation under the cross-dataset scenario (D1 → D2).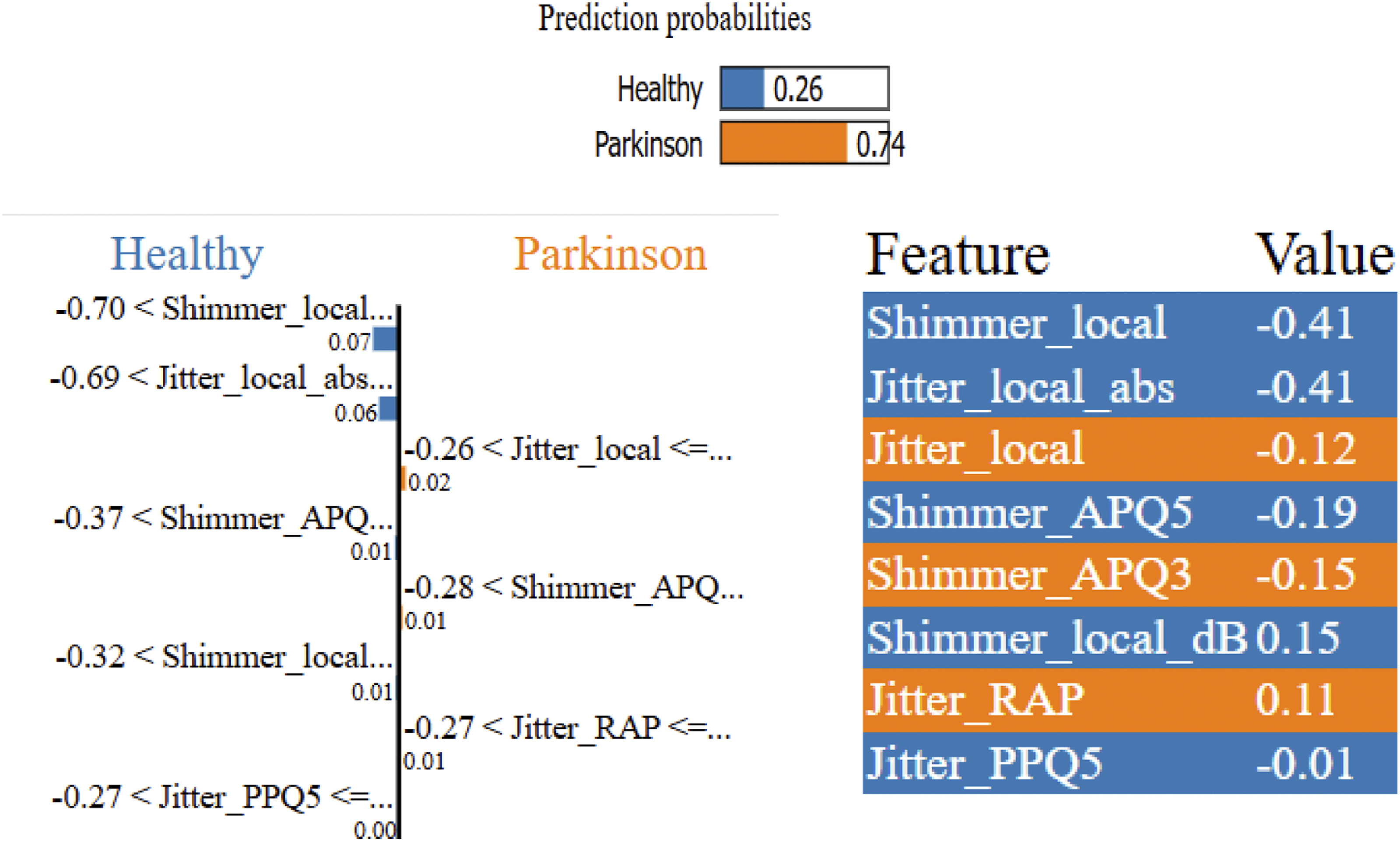
The explainability analysis in this research demonstrates three key outcomes. First, the models consistently rely on clinically relevant acoustic biomarkers, particularly jitter-related features, across datasets and model families. Second, global and local explanations remain stable despite the intentionally challenging cross-dataset evaluation strategy, indicating that performance degradation does not stem from a loss of meaningful feature learning. Third, the alignment between SHAP and LIME explanations confirms that the proposed framework prioritizes transparent, physiologically grounded decision-making, making it suitable for real-world clinical support rather than purely benchmark-driven evaluation. These findings substantiate the claim that the proposed approach not only generalizes more realistically but also remains interpretable and trustworthy—two essential requirements for deploying Parkinson’s disease detection systems in healthcare environments.
4.5. Federated learning results
Federated learning performance scores.
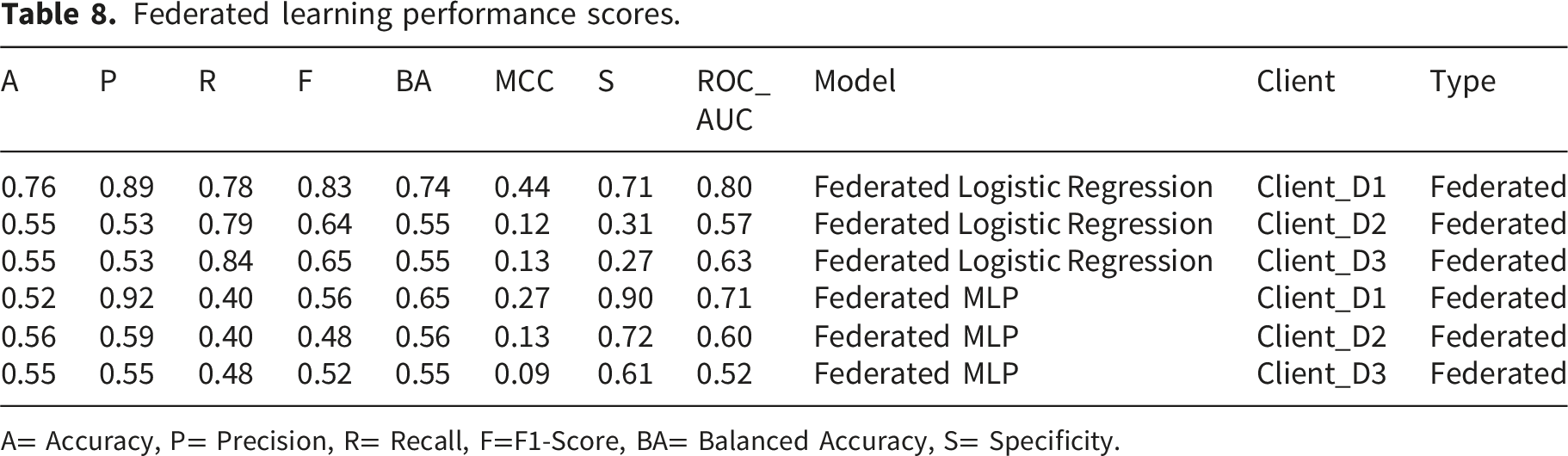
A= Accuracy, P= Precision, R= Recall, F=F1-Score, BA= Balanced Accuracy, S= Specificity.
For Federated Logistic Regression, a clear improvement is observed on Client D1, where the model achieves substantially higher accuracy, F1-score, balanced accuracy, and ROC-AUC compared to its centralized and cross-dataset counterparts. The F1-score of 0.83 and ROC-AUC of 0.80 indicate a strong balance between sensitivity and precision, which is particularly important in medical screening contexts. This improvement suggests that federated aggregation allows the model to benefit from shared representations learned across heterogeneous datasets while still preserving local data distributions. On Clients D2 and D3, the performance remains moderate but stable, with consistent recall values and balanced accuracy close to 0.55. Importantly, the MCC becomes consistently positive across all clients, indicating improved agreement between predictions and ground truth compared to several centralized settings where MCC values were near zero or negative. This shift reflects enhanced robustness rather than overfitting to a single dataset.
Reproducibility analysis of federated logistic regression on client D1.

The results in Table 9 demonstrate that the elevated performance on Client D1 is consistently reproducible across multiple random seeds. The F1-score remains high (0.84 on average) with moderate variability (standard deviation of 0.05), while the ROC-AUC shows a mean of 0.78 with a standard deviation of 0.07. The relatively narrow confidence intervals (CIs) indicate that the observed performance is stable and not attributable to random initialization or sampling effects. At the same time, the presence of non-zero variability suggests that the model retains sensitivity to data partitioning, which is expected given the limited size and class imbalance of the dataset.
From a methodological perspective, this analysis clarifies that the improved performance on Client D1 is not an artifact of randomness but reflects a consistent learning behaviour under the federated setting. A plausible explanation is that federated aggregation enables the model to incorporate complementary patterns from other datasets while maintaining sensitivity to local feature distributions, thereby enhancing discrimination capability in smaller datasets. However, it is important to interpret this improvement cautiously, as it may still be influenced by dataset-specific characteristics rather than representing a universally generalizable gain.
The Federated MLP exhibits a complementary behaviour. Although its overall F1-scores are lower than those of Federated Logistic Regression, it demonstrates higher precision and specificity in certain clients, particularly D1 and D2. This indicates a more conservative decision boundary, which may be advantageous in clinical settings where reducing false positives is desirable. The consistent, moderate ROC-AUC values further confirm that the neural model maintains discriminative capability despite decentralized training constraints.
Overall, the federated learning results highlight several important insights. First, meaningful performance gains can be achieved without direct data sharing, reinforcing the practicality of privacy-preserving machine learning in healthcare. Second, improvements in balanced accuracy and MCC indicate enhanced robustness across heterogeneous datasets. Third, the reproducibility analysis confirms that observed performance gains—particularly in Client D1—are stable and not driven by random effects.
Taken together, these findings support the central premise of this study: reliable Parkinson’s disease detection can be achieved through a federated framework that prioritizes generalization, interpretability, and privacy. Rather than relying on overly optimistic single-dataset results, the proposed approach provides a more realistic and deployment-aware foundation for clinical decision-support systems.
Beyond statistical reproducibility, the magnitude of performance improvement achieved by the federated framework was quantified using direct effect size analysis based on metric differences relative to centralized baselines. Specifically, Federated Logistic Regression on Client D1 achieves a balanced accuracy (BA) of 0.74 and MCC of 0.44, compared to the centralized Logistic Regression baseline (BA = 0.54, MCC = 0.09). This corresponds to an absolute improvement of ΔBA = +0.20 and ΔMCC = +0.35, indicating a substantial increase in both class-wise discrimination and overall prediction reliability.
From a practical standpoint, these gains are meaningful rather than marginal. An increase of 0.20 in balanced accuracy reflects a significant improvement in the model’s ability to correctly classify both Parkinson’s and control cases under class imbalance, while the 0.35 increase in MCC suggests a markedly stronger correlation between predicted and true labels. Importantly, these improvements are achieved without access to pooled raw data, reinforcing that federated aggregation contributes not only to privacy preservation but also to enhanced learning of generalizable feature representations.
Taken together with the multi-seed stability analysis, the observed effect sizes confirm that the superior performance on Client D1 is neither a random artifact nor a trivial fluctuation, but rather a consistent and practically significant outcome of the federated learning paradigm. Nevertheless, these gains should be interpreted in the context of dataset-specific characteristics, particularly the smaller size and imbalance of D1, which may amplify the relative benefit of cross-client knowledge sharing.
4.6. Ablation study findings
The ablation study was conducted to systematically assess the contribution of individual feature groups, dataset composition strategies, and learning paradigms to Parkinson’s disease detection performance. Rather than optimizing predictive accuracy, this analysis aims to reveal which components of the proposed framework are genuinely informative and robust under realistic constraints.
Feature Ablation Experiment (Jitter vs Shimmer).
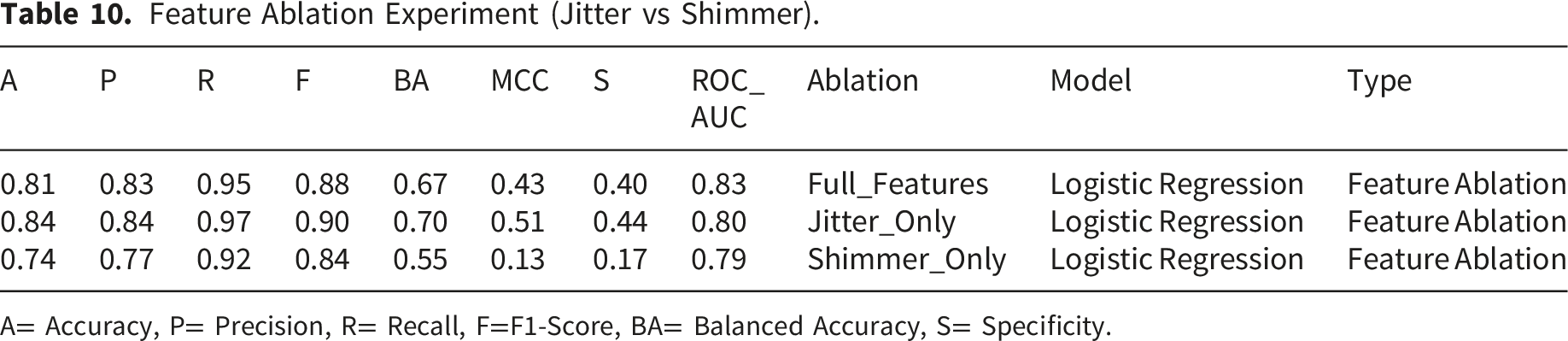
A= Accuracy, P= Precision, R= Recall, F=F1-Score, BA= Balanced Accuracy, S= Specificity.
Dataset Ablation Experiment (Single vs Combined).

A= Accuracy, P= Precision, R= Recall, F=F1-Score, BA= Balanced Accuracy, S= Specificity.
Learning Paradigm Ablation Experiment (Centralized vs Federated).
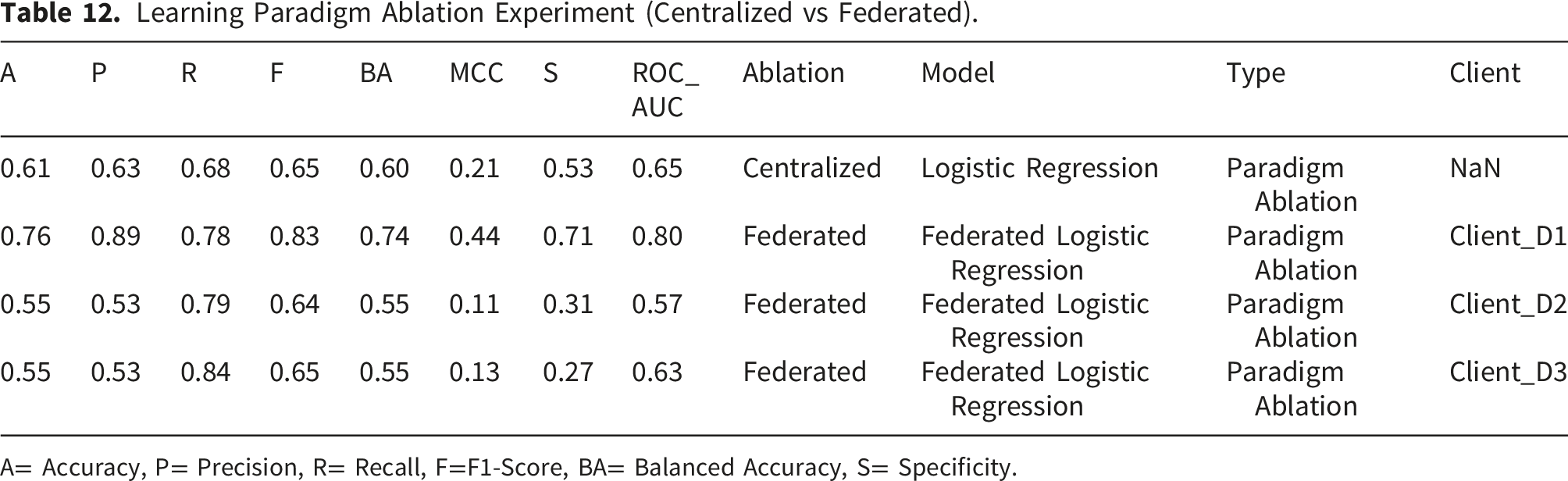
A= Accuracy, P= Precision, R= Recall, F=F1-Score, BA= Balanced Accuracy, S= Specificity.
Collectively, the ablation study confirms that (i) jitter features are the primary drivers of Parkinson’s disease discrimination, (ii) dataset heterogeneity poses a fundamental challenge to naïve data aggregation, and (iii) federated learning offers a viable and often superior alternative to centralized training under privacy and generalization constraints. Rather than optimizing individual components in isolation, these findings emphasize the importance of holistic system design, where feature selection, data partitioning, and learning paradigms jointly determine model reliability. This ablation-driven analysis strengthens the methodological validity of the proposed framework and further supports the study’s emphasis on generalization-aware, clinically meaningful evaluation over inflated performance claims.
4.7. Evaluation strategy ablation (leakage sensitivity analysis)
The baseline and tuned results presented in Tables 5 and 6 show near-chance balanced accuracy (BA ≈ 0.50–0.55) and low or negative MCC, even under within-dataset evaluation. While this behaviour is consistent with the study’s strict subject-aware design, it raises an important methodological concern: whether the observed performance reflects the genuine difficulty of the task under realistic constraints, or whether it could be attributed to potential implementation issues in the pipeline. To address this concern and to validate the correctness of the proposed evaluation framework, a targeted ablation study was conducted focusing specifically on the impact of evaluation strategy and potential data leakage.
A controlled experiment was designed using a single dataset (D1) to isolate the effect of data splitting and preprocessing strategies while keeping all other components constant (features, model, and evaluation metrics). Three evaluation scenarios were implemented: • • •
Impact of evaluation strategy on model performance (leakage sensitivity analysis).

The results provide clear evidence that the low balanced accuracy and MCC observed in Tables 5 and 6 are not due to errors in the implementation but are a direct consequence of the strict, leakage-free evaluation protocol. Under the subject-aware setting, the model is forced to generalize across unseen individuals, leading to lower but more realistic performance. The negative MCC further indicates weak agreement between predicted and true labels under these constraints, reflecting the inherent difficulty of learning robust, transferable patterns from heterogeneous voice data.
In contrast, relaxing the evaluation protocol through random splitting leads to a substantial increase in all performance metrics (e.g., BA: 0.44 → 0.65; MCC: −0.20 → 0.34). This improvement does not reflect better generalization but rather the presence of subject-level leakage, where the model indirectly learns speaker-specific characteristics that appear in both training and testing sets. Such leakage artificially simplifies the classification task and produces overly optimistic results, consistent with the high accuracies frequently reported in prior literature.
Interestingly, the results for the “Random Split” and “Random + Leakage” scenarios are identical. This outcome indicates that the dominant source of performance inflation arises from subject-level leakage rather than preprocessing leakage. Once samples from the same subject are present in both training and testing sets, the model already gains access to highly informative subject-specific patterns. Consequently, additional leakage introduced through scaling before splitting has minimal incremental effect on performance. This finding highlights that subject-level leakage is the primary driver of inflated results in voice-based Parkinson’s disease detection, while preprocessing leakage plays a comparatively minor role in this context.
4.8. Statistical analysis framework results
To ensure that the reported performance differences reflect genuine model behaviour rather than random variation, a comprehensive statistical reliability analysis was conducted. Given the limited number of paired evaluation scenarios, formal hypothesis testing was not emphasized; instead, the analysis focuses on distribution-aware metrics, uncertainty quantification, and calibration quality to provide a more robust and interpretable assessment.
Model reliability was assessed using repeated experiments across multiple random seeds, with 95% confidence intervals (CIs) computed for key metrics. For the baseline Logistic Regression model, the F1-score (0.86, CI: 0.83–0.89), balanced accuracy (0.66, CI: 0.61–0.70), and ROC-AUC (0.79, CI: 0.75–0.83) demonstrate relatively narrow intervals, indicating stable performance across different data partitions. The observed variability reflects expected uncertainty due to limited sample size and dataset heterogeneity, rather than instability. A similar pattern is observed in the federated setting, where non-zero standard deviations confirm sensitivity to data variation while maintaining consistent overall performance. This analysis highlights the importance of reporting uncertainty alongside mean performance to ensure realistic and reproducible evaluation.
To assess the practical significance of performance differences, effect size analysis was conducted using absolute improvements in key metrics. Comparing baseline and federated Logistic Regression on Client D1 shows a balanced accuracy increase from 0.54 to 0.74 (Δ = +0.20) and an MCC improvement from 0.09 to 0.44 (Δ = +0.35). These gains indicate a substantial enhancement in both class-wise discrimination and overall prediction reliability. The magnitude of improvement, particularly in MCC, reflects meaningful learning benefits rather than marginal or noise-driven differences. This analysis provides a scale-aware interpretation of model improvements, which is especially important in cross-dataset and federated settings where traditional significance testing alone may be insufficient.
Model calibration was evaluated using the Brier Score (BS), which measures the alignment between predicted probabilities and actual outcomes. Across baseline, tuned, and cross-dataset experiments, Brier Scores generally range from 0.23 to 0.43, indicating moderate calibration quality. Lower values (≈0.23–0.27) observed in some cross-dataset scenarios suggest improved probability reliability when models are trained on more diverse data, while higher values (≈0.40+) reflect increased uncertainty under distributional shifts. This pattern indicates that, even when classification performance is constrained, the predicted probabilities retain meaningful structure, supporting their use in risk-sensitive clinical decision-making.
The combined use of confidence intervals, effect size analysis, and calibration metrics provides a comprehensive and reliable evaluation framework. The results demonstrate that model performance is reproducible across different data splits, observed improvements—particularly in federated learning—are substantively meaningful, and probability estimates remain reasonably calibrated under challenging conditions. Together, these findings reinforce the study’s emphasis on robustness, generalization, and clinical interpretability, prioritizing consistent and trustworthy performance over isolated metric gains.
5. Discussions
This section synthesizes the experimental findings through the lens of real-world Parkinson’s disease detection, emphasizing generalization, interpretability, and deployment feasibility. Rather than reiterating numerical results, the discussion contextualizes observed performance degradation, feature robustness, explainability stability, and federated learning behaviour within existing literature and clinical constraints. Collectively, the findings reposition voice-based PD detection as a deployment-critical challenge, where robustness, transparency, and privacy matter more than peak accuracy under controlled conditions.
5.1. Summary of key findings
This study presents a generalization-oriented evaluation of ML for PD detection, emphasizing deployment realism over single-dataset performance. A consistent performance gap between in-distribution and cross-dataset evaluation confirms that high accuracy obtained under controlled conditions does not translate reliably to unseen data. This gap reflects the impact of dataset heterogeneity rather than isolated model limitations.
Across experiments, the divergence between accuracy and MCC highlights an important reliability issue: models can achieve moderate accuracy while exhibiting unstable or biased class-wise predictions. This reinforces the need for evaluation metrics that capture prediction consistency, particularly in clinical contexts. Hyperparameter tuning provides only marginal improvements and does not mitigate cross-dataset degradation, indicating that optimization alone cannot compensate for distributional variability. In contrast, explainability analyses remain stable, with jitter-related features consistently identified as dominant predictors across models, suggesting that learned patterns retain physiological relevance despite reduced predictive performance.
Federated learning demonstrates selective robustness gains without requiring data sharing, supporting its role as a privacy-preserving alternative for multi-institutional settings. Additionally, ablation studies confirm that jitter-based features are more stable than shimmer-based features and that naïve dataset aggregation does not necessarily improve generalization.
The findings of this study shift the focus from peak accuracy to reliability, interpretability, and robustness under realistic conditions.
5.2. Interpretation of generalization behaviour under dataset shift
The cross-dataset results reveal a consistent convergence of model performance toward moderate levels, indicating a generalization ceiling imposed by dataset heterogeneity. Differences in recording conditions, subject populations, and acquisition protocols alter feature distributions, limiting the transferability of learned patterns across datasets.
Balanced accuracy remains relatively stable by accounting for class-wise performance, whereas MCC exposes deeper inconsistencies in prediction structure. This divergence shows that class balance alone does not guarantee reliable decision-making, particularly when distributional shifts affect feature relationships.
Rather than representing model inadequacy, this behaviour reflects a realistic operating regime for voice-based Parkinson’s disease detection under deployment conditions. The findings suggest that robustness is constrained not only by model design but also by intrinsic variability in biomedical data, reinforcing the need to evaluate models under heterogeneous settings rather than relying on controlled benchmarks.
5.3. Implications for Parkinson’s disease modelling research
5.3.1. Methodological implications
The results demonstrate that single-dataset evaluation is insufficient for assessing clinical applicability. Cross-dataset validation provides a more realistic estimate of model reliability and should be treated as a standard evaluation protocol. The limited impact of hyperparameter tuning further indicates that evaluation design and data heterogeneity play a more critical role than model optimization in determining real-world performance.
5.3.2. Feature-level implications
Jitter-related features consistently exhibit greater robustness and discriminative power than shimmer-based features under distributional shift. This aligns with the physiological basis of Parkinson’s disease, where frequency perturbations are more directly linked to neuromotor impairment. The findings suggest that compact, physiologically grounded feature sets may generalize better than larger, dataset-specific representations.
5.3.3. Evaluation implications
The study highlights the importance of using metrics that reflect clinical reliability. Accuracy alone is insufficient under dataset shift, while balanced accuracy and ROC-AUC provide more informative assessments. MCC, despite often yielding low values, serves as a critical indicator of prediction consistency and should be retained as a diagnostic metric. Reporting multiple complementary metrics enables a more transparent evaluation aligned with clinical decision-making requirements.
Together, these implications emphasize a shift from accuracy-driven benchmarking toward robustness, interpretability, and generalization-aware evaluation, which are essential for clinically deployable Parkinson’s disease detection systems.
5.4. Explainability under realistic conditions
Most existing Parkinson’s disease detection studies present explainability results under idealized conditions—typically using models trained and tested on the same dataset and reporting explanations alongside near-perfect accuracy. While such analyses may demonstrate model interpretability in controlled settings, they provide limited insight into whether explanations remain meaningful when predictive performance degrades under real-world conditions. This study addresses this gap by examining explainability explicitly under cross-dataset generalization, where distribution shift is present and performance is intentionally constrained.
Despite the observed reduction in predictive metrics under cross-dataset evaluation, the explainability analysis reveals a high degree of stability in feature importance rankings across models and explanation techniques. Global SHAP analyses for both linear (Logistic Regression) and non-linear (Random Forest) models consistently identify jitter-related features—such as absolute and relative frequency perturbation measures—as the dominant contributors to Parkinson’s disease prediction. Shimmer-related features appear as secondary contributors, reinforcing the feature-level robustness findings from the ablation studies. This consistency across model families suggests that the learned decision logic remains physiologically grounded even when classification confidence decreases. At the local level, SHAP force plots and LIME explanations for individual patient instances exhibit strong agreement in highlighting the same subset of influential features. Importantly, this agreement persists across explanation methods that rely on fundamentally different assumptions—SHAP being grounded in cooperative game theory and LIME relying on local surrogate modelling. The convergence of these explanations indicates that model decisions are not driven by spurious correlations or unstable feature interactions introduced by dataset shift, but instead reflect coherent and repeatable patterns in the underlying acoustic biomarkers. A critical implication of this finding is that explainability stability may be more clinically valuable than high predictive confidence. In medical decision support systems, clinicians often prioritize understanding why a prediction is made over marginal gains in accuracy, particularly in early-stage screening scenarios. The fact that interpretability remains consistent even when accuracy and MCC decline suggests that the model’s reasoning process is resilient to domain variability. This reinforces the model’s potential role as an assistive tool rather than a deterministic diagnostic system.
Furthermore, the alignment between explainability outcomes and known clinical characteristics of Parkinson’s disease strengthens trust in the model’s behaviour. Jitter dominance aligns with established evidence linking vocal frequency instability to neuromotor dysfunction, while the comparatively lower stability of shimmer features reflects their sensitivity to recording conditions and external noise. By demonstrating that explainable patterns persist under realistic evaluation settings, this study shifts the role of XAI from a post hoc visualization tool to a validation mechanism for generalization and clinical plausibility. Overall, this work reframes explainability as a robustness indicator rather than a performance embellishment. The preservation of interpretable feature contributions under dataset shift provides an additional layer of evidence that the proposed framework captures clinically meaningful signal, even when faced with the unavoidable variability of real-world data. This perspective advances the use of XAI in Parkinson’s disease modelling from interpretability under ideal conditions to trustworthiness under deployment-relevant scenarios.
5.5. Federated learning: Privacy vs. performance trade-off
Federated learning is increasingly advocated as a solution for privacy-preserving healthcare analytics. However, its effectiveness under real-world data heterogeneity remains an open question. Rather than positioning federated learning as a universal performance enhancer, this study evaluates FL as a deployment-oriented compromise between predictive accuracy, data privacy, and institutional autonomy. The observed results highlight that federated learning does not uniformly improve performance across all clients, yet still offers meaningful advantages for Parkinson’s disease detection in realistic clinical settings.
The federated learning experiments demonstrate selective performance improvements, most notably for Client_D1, where federated logistic regression achieves substantial gains in accuracy, F1-score, MCC, and ROC-AUC compared to centralized counterparts. This improvement can be attributed to the aggregation of complementary information from multiple clients, which enriches the global model without requiring raw data exchange. In contrast, more modest or inconsistent gains are observed for Client_D2 and Client_D3, reflecting differences in data quality, class distribution, and recording conditions across participating datasets. These findings underscore a key reality of federated learning: its benefits are inherently client-dependent and shaped by data heterogeneity. Importantly, the absence of uniform performance gains should not be interpreted as a limitation of the federated approach. In healthcare contexts, even partial improvements—particularly in recall, balanced accuracy, or MCC—can be clinically significant, as they directly influence the system’s ability to identify affected individuals without excessive false reassurance. The federated models demonstrate improved robustness for certain clients, suggesting that FL can mitigate, though not eliminate, the adverse effects of dataset bias and distributional shift. This aligns with the broader objective of the study, which prioritizes reliability and generalization over peak accuracy.
From a deployment perspective, FL introduces a fundamentally different value proposition compared to centralized training. While centralized models may achieve higher performance when data can be pooled freely, such assumptions are often unrealistic in clinical environments due to privacy regulations, institutional policies, and ethical constraints. FL enables collaboration across hospitals or research centers without exposing sensitive patient data, thereby increasing trust and feasibility for real-world adoption. In this context, the trade-off between privacy preservation and marginal performance variation becomes acceptable, particularly when explainability and generalization are preserved. The comparison between federated logistic regression and federated MLP further illustrates the interaction between model complexity and federated optimization. Simpler models, such as logistic regression, exhibit more stable federated convergence and clearer performance gains for certain clients, whereas neural models show greater sensitivity to client-level variability. This observation suggests that model selection plays a critical role in federated healthcare applications, and that simpler, interpretable models may be better suited for privacy-preserving, cross-institutional learning under heterogeneous conditions.
5.6. Real-world deployment opportunities and threats
The methodological and empirical findings of this study provide a realistic lens through which the deployment of voice-based Parkinson’s disease (PD) detection systems can be evaluated. Rather than framing deployment solely as a function of predictive accuracy, the results emphasize operational reliability, clinical trust, and ethical feasibility. This section synthesizes the deployment opportunities enabled by the proposed framework, alongside the practical threats that must be addressed before translation into real-world healthcare settings.
5.6.1. Opportunities
One of the most promising deployment opportunities lies in remote screening and early risk stratification. Voice-based analysis offers a non-invasive, low-cost, and easily accessible modality for preliminary PD assessment using everyday devices. Although cross-dataset evaluations reveal moderate predictive performance, such systems can still play a critical role as front-line screening tools by identifying individuals who may benefit from further neurological examination. In this context, recall, balanced accuracy, and explainability are more clinically meaningful than inflated single-dataset accuracy. Telemedicine integration represents a natural extension of this capability. As remote consultations become increasingly prevalent, voice-based models can be embedded into telehealth platforms without additional burden on patients or clinicians. The stability of explainability results across datasets and models strengthen this opportunity, as clinicians can be presented with interpretable indicators—such as jitter- and shimmer-related perturbations—that align with established speech impairments in PD. This interpretability enhances clinician confidence, even when predictive certainty varies across populations.
Another important opportunity is privacy-preserving hospital and institutional collaboration through federated learning. Healthcare data sharing is often constrained by regulatory and ethical considerations. The federated learning experiments demonstrate that collaborative model training across independent datasets is feasible without centralized data aggregation. Even when performance improvements are client-specific rather than universal, federated learning enables institutions to contribute to collective model refinement while maintaining data sovereignty, which is essential for large-scale clinical adoption. Finally, longitudinal patient monitoring emerges as a future deployment pathway. While the current study focuses on cross-sectional data, the demonstrated robustness of jitter-related features and the consistency of explainability suggest potential for tracking speech changes over time. Such longitudinal monitoring could support disease progression assessment, therapy evaluation, and early detection of deterioration, provided that models are recalibrated to account for evolving patient-specific baselines.
5.6.2. Threats
Despite these opportunities, several deployment threats are clearly exposed by the results. Dataset bias remains a fundamental challenge, as differences in recording protocols, demographic composition, and acoustic environments significantly influence model behaviour. The observed generalization ceiling under cross-dataset testing indicates that models trained on limited or homogeneous data may perform unpredictably when deployed in diverse real-world settings. Closely related is the threat of domain shift, which arises when the statistical properties of deployment data differ from those seen during training. The cross-dataset experiments demonstrate that even well-tuned models experience performance degradation under distributional mismatch. Without explicit safeguards, such as domain adaptation or continual learning, this shift can undermine clinical reliability and patient safety.
Another critical threat is overconfidence driven by high single-dataset accuracy. Many existing PD detection studies report near-perfect performance without external validation. The consistently low or negative MCC values observed in this work highlight that such accuracy figures may conceal unstable class-wise predictions. In deployment scenarios, this overconfidence can lead to missed diagnoses, unnecessary referrals, or misplaced clinical trust if not transparently addressed. Finally, regulatory and clinical validation challenges present significant barriers to real-world adoption. ML systems in healthcare must demonstrate consistent performance across populations, comply with data protection regulations, and undergo rigorous clinical evaluation. The realistic evaluation strategy adopted in this study suggests that achieving such standards requires extensive cross-dataset validation, prospective trials, and continuous post-deployment monitoring—processes that are often overlooked but essential for responsible deployment.
Deployment opportunities and threats for voice-based Parkinson’s disease detection systems.
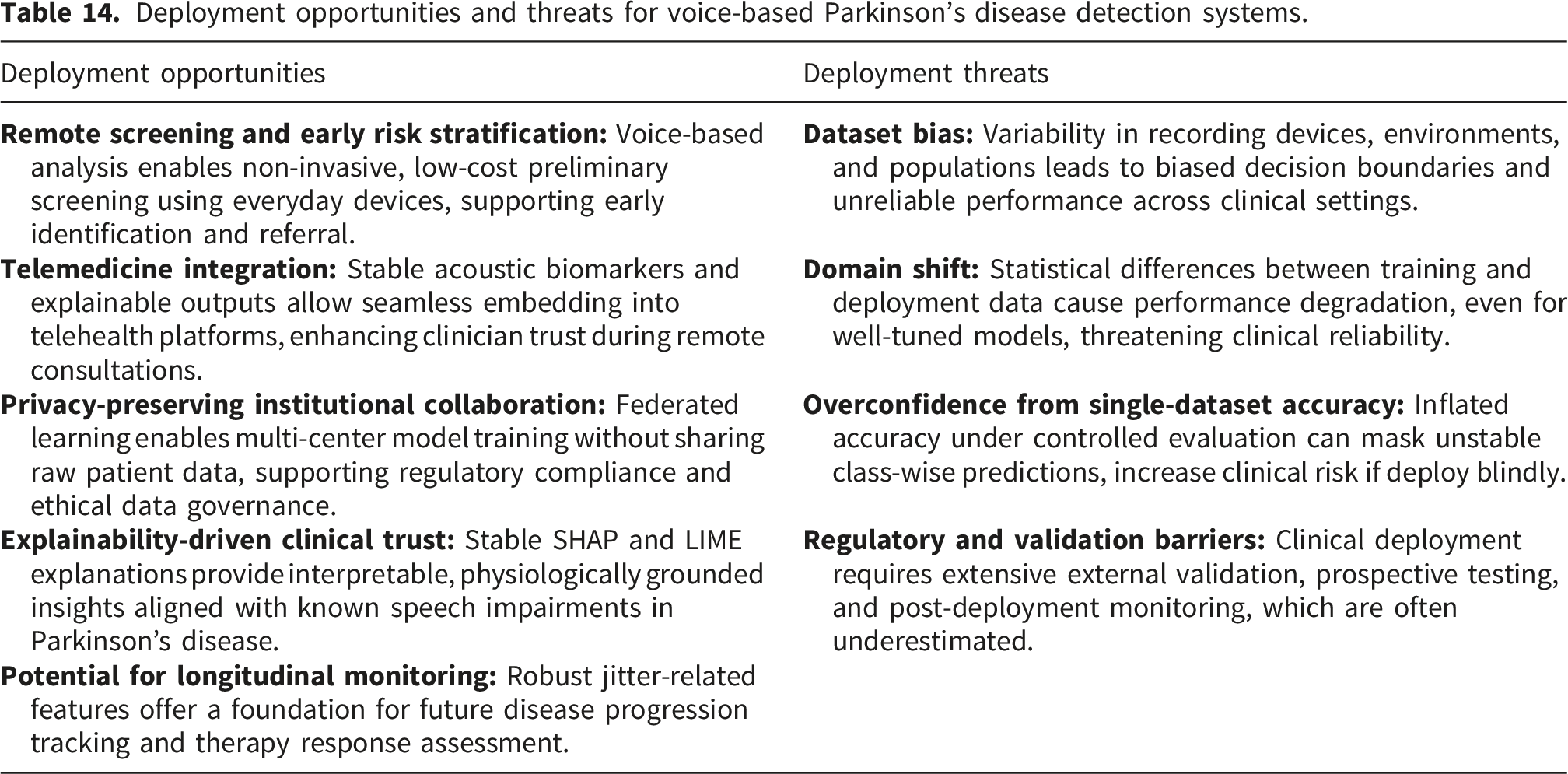
5.7. Research questions revisited: Discussion through RQs and RAs
Mapping of RQs, RAs, and supporting evidence.
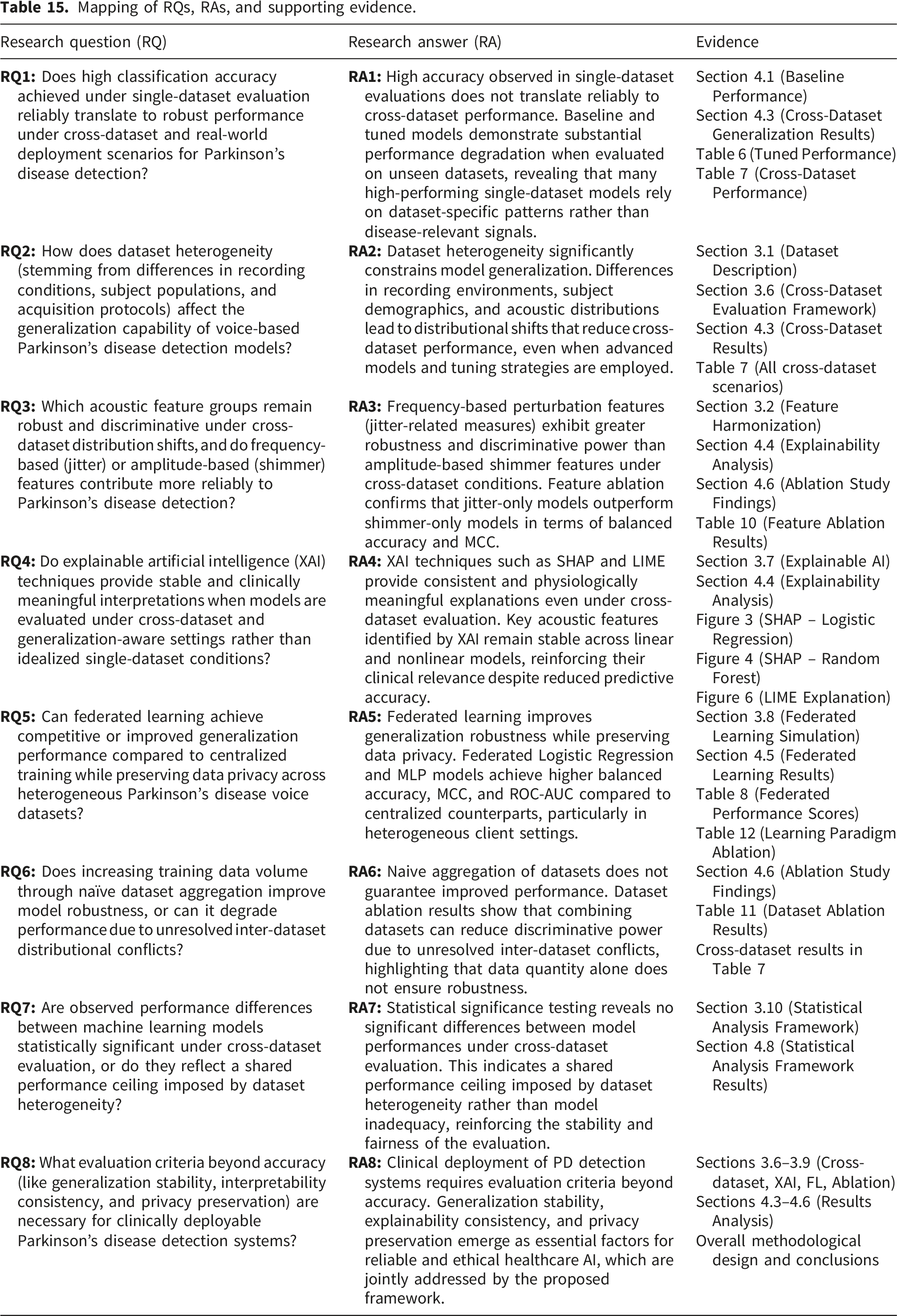
Across all generalization-focused questions (RQ1, RQ2, RQ6, RQ7), the results consistently demonstrate that high single-dataset accuracy does not translate to robust performance under cross-dataset evaluation. Performance degradation, low or negative MCC, and the absence of statistically significant differences between models collectively indicate a generalization ceiling imposed by dataset heterogeneity rather than algorithmic inadequacy. Moreover, naive dataset aggregation fails to resolve this limitation and may further degrade performance, challenging the common assumption that increased data volume alone improves robustness. Feature-level analysis (RQ3) reveals that frequency-based perturbation measures (jitter-related features) remain more stable and discriminative than amplitude-based shimmer features under distribution shift. This finding refines prior literature by distinguishing features that perform well under controlled conditions from those that retain reliability in realistic deployment scenarios. Despite reduced predictive performance under cross-dataset evaluation, explainability analyses remain stable across models and datasets (RQ4). The consistency of SHAP and LIME explanations—particularly the dominance of jitter-related features—suggests that models capture physiologically meaningful patterns rather than dataset-specific artifacts. This highlights explanation stability as a more relevant indicator of clinical trust than accuracy alone. Federated learning experiments demonstrate that privacy-preserving training can achieve competitive generalization performance under heterogeneous data distributions. Together with the generalization and explainability findings (RQ5, and RQ8), this reinforces the need for evaluation criteria beyond accuracy, including robustness, interpretability consistency, and privacy preservation, as prerequisites for clinically deployable Parkinson’s disease detection systems. Taken together, the research questions and their answers reposition Parkinson’s disease detection as a deployment-critical problem rather than an accuracy-centric task. By integrating cross-dataset evaluation, explainability, and federated learning within a unified framework, this study advances a more realistic and clinically aligned evaluation paradigm.
5.8. Comparison with prior Parkinson’s disease studies
Reported performance in prior PD studies vs. observations under realistic evaluation.
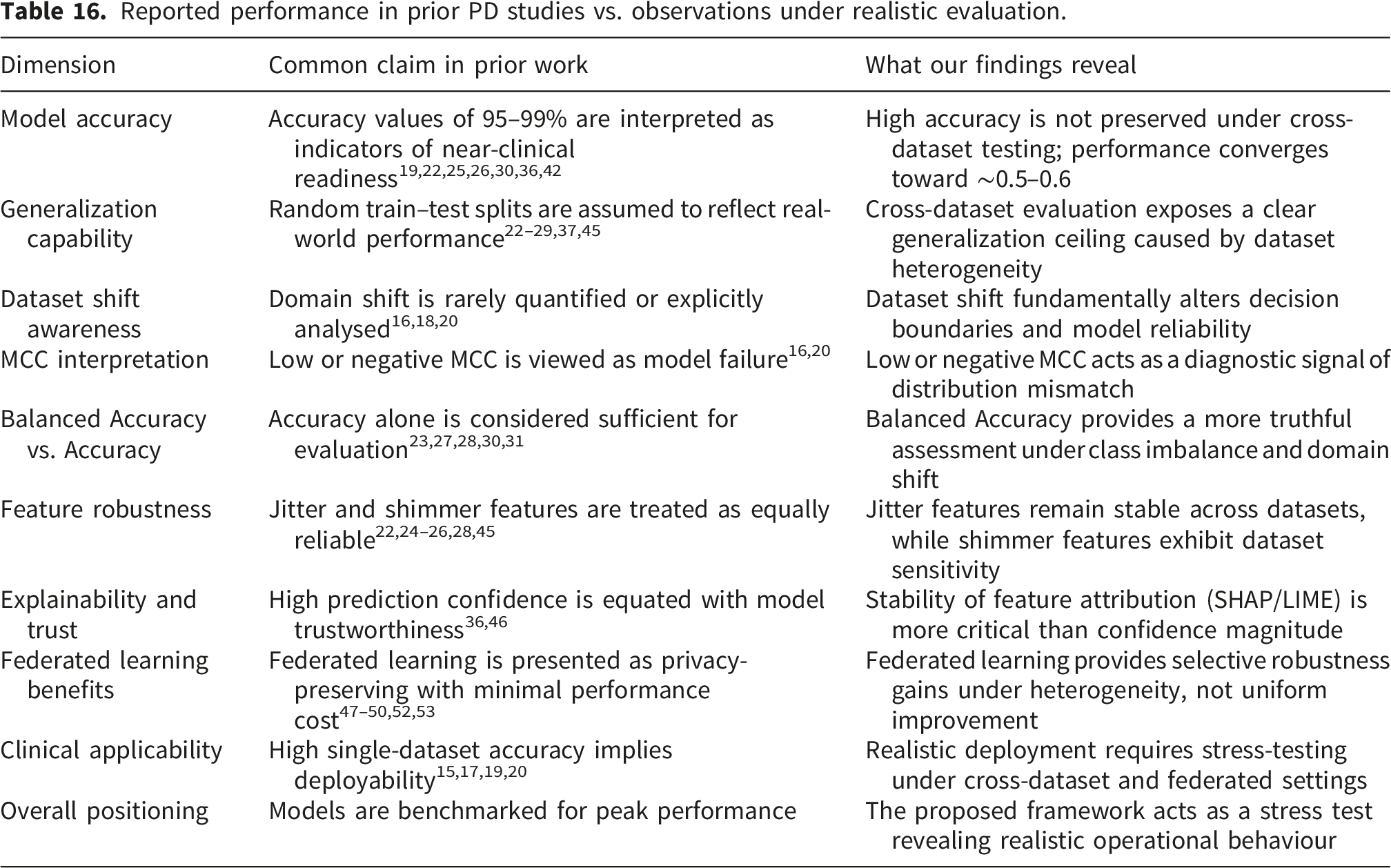
A key limitation underlying many of these high-accuracy claims is the rarity of cross-dataset validation. As reflected in Table 16, most prior studies assume that random splits are sufficient to assess generalization, despite the well-documented heterogeneity in PD data arising from differences in recording devices, speech tasks, patient demographics, disease stages, and preprocessing pipelines. Consequently, performance estimates derived from single-dataset evaluations tend to conflate memorization of dataset-specific characteristics with genuine disease-related learning. The absence of systematic cross-dataset testing has allowed inflated accuracy figures to persist in the literature without adequately addressing real-world deployment constraints. In contrast, the present study deliberately adopts a more stringent evaluation strategy by emphasizing cross-dataset generalization. When models trained on one dataset are evaluated on another, performance consistently converges to a more modest accuracy range of approximately 0.5–0.6, as shown in Table 16. Although these values appear substantially lower than those reported in prior work, they provide a more realistic estimate of expected performance under clinical variability. Rather than masking distributional mismatch, this evaluation exposes the intrinsic difficulty of PD detection across heterogeneous data sources and highlights a generalization ceiling that remains largely unacknowledged in earlier studies.
Importantly, this work reframes lower performance metrics not as indicators of failure, but as informative signals about model robustness. Metrics such as Balanced Accuracy and MCC, which are rarely emphasized in earlier studies, reveal systematic degradation under dataset shift that accuracy alone fails to capture. As summarized in Table 16, negative or near-zero MCC values reflect domain mismatch and class imbalance effects rather than poor model construction. By explicitly reporting and interpreting these metrics, this study provides a more transparent assessment of model behaviour in realistic scenarios. Taken together, these comparisons position the present work as a stress test rather than a benchmark. While prior studies focus on achieving peak performance under controlled conditions, this research prioritizes realism by probing how models respond to distribution shift, heterogeneous datasets, and privacy-preserving learning paradigms. As illustrated in Table 16, the goal is not to outperform existing studies in terms of absolute accuracy, but to interrogate the assumptions underlying commonly reported results and to establish evaluation practices that better align with real-world clinical deployment. This shift in perspective strengthens the novelty of the work by moving the field from optimistic performance reporting toward evidence-based robustness assessment.
5.9. Practical design guidelines for future PD detection systems
Based on the empirical findings and deployment-oriented evaluation conducted in this study, several practical design guidelines can be derived for future PD detection systems using voice data. These guidelines aim to bridge the gap between experimental performance and real-world clinical usability. • First, cross-dataset validation should be treated as a mandatory evaluation component rather than an optional extension. Single-dataset accuracy alone is insufficient to assess deployment readiness, as models frequently exploit dataset-specific artifacts that fail under distribution shift. Evaluating models on unseen datasets provides a more realistic estimate of robustness and should become standard practice in healthcare ML research. • Second, feature selection should prioritize robustness over feature richness. The consistent dominance of jitter-related features across datasets and models indicates that frequency-based perturbation measures are more reliable biomarkers of Parkinson’s disease than amplitude-based shimmer features under heterogeneous recording conditions. Future systems should therefore emphasize jitter-focused or robustness-tested acoustic feature sets rather than relying on large, dataset-specific feature pools. • Third, evaluation metrics must extend beyond overall accuracy. Metrics such as MCC and balanced accuracy provide critical insight into class-wise discrimination and model reliability, particularly under class imbalance and dataset shift. Reporting these metrics alongside accuracy enables more transparent and clinically meaningful model assessment. • Fourth, explainability should be evaluated for stability, not merely presence. XAI techniques should be applied under realistic evaluation settings, including cross-dataset scenarios, to assess whether explanations remain consistent when predictive performance degrades. Stable global and local explanations, as demonstrated in this study, are essential for clinician trust and diagnostic accountability. • Finally, federated learning should be considered when data sharing is constrained. Although federated models may not universally outperform centralized training, selective performance gains under heterogeneous conditions, combined with strong privacy guarantees, make FL a practical and ethically aligned choice for multi-institutional PD screening systems.
Collectively, these guidelines provide actionable principles for designing PD detection systems that prioritize robustness, interpretability, and privacy, extending the utility of this research beyond academic benchmarking toward real-world clinical deployment.
5.10. Limitations and future research scope of the study
While this study provides a realistic and deployment-aware assessment of voice-based PD detection, several limitations should be acknowledged and viewed as directions for future research. • First, the evaluation is conducted using three publicly available voice datasets, which, although heterogeneous, do not fully capture the global diversity of languages, accents, recording devices, and clinical settings encountered in real-world deployment. Expanding cross-dataset evaluation to larger and more diverse cohorts would further strengthen generalization analysis. • Second, the study focuses exclusively on voice-based acoustic features. While voice is a non-invasive and clinically relevant modality, PD manifests across multiple domains, including gait, handwriting, and neuroimaging. Future work should explore multimodal frameworks that integrate complementary signals while preserving generalization-aware evaluation principles. • Third, the current framework does not model longitudinal disease progression. Parkinson’s disease is inherently progressive, and temporal analysis of voice changes could provide valuable insights into disease staging and monitoring. Incorporating longitudinal data remains an important avenue for extending the clinical relevance of the proposed approach. • Fourth, the federated learning experiments are conducted in a simulated environment, where each dataset is treated as a separate client. While this setup reflects realistic institutional heterogeneity, real-world federated deployments involve additional challenges such as communication constraints, partial participation, and system-level variability. Future studies should evaluate the framework under real clinical FL infrastructures.
Importantly, these limitations do not undermine the study’s conclusions. Rather, they highlight the complexity of deploying ML systems in healthcare and reinforce the need for continued research that prioritizes realism, robustness, and ethical considerations over isolated performance gains.
5.11. External validation and real-world clinical applicability
While the proposed framework emphasizes generalization through cross-dataset evaluation and federated learning, the current study is limited to retrospective analysis using publicly available datasets. Although these datasets exhibit substantial heterogeneity in terms of recording conditions, subject populations, and feature distributions, they cannot fully replicate the complexity and variability of real-world clinical environments. Consequently, the reported results should be interpreted as an intermediate step toward deployment rather than definitive evidence of clinical readiness.
To establish external validity, prospective validation on real-world clinical data is essential. Such validation would involve deploying the trained models in hospital or telemedicine settings, where voice recordings are collected from previously unseen patients under routine clinical workflows. Unlike controlled datasets, real-world data introduce additional sources of variability, including differences in recording devices, environmental noise, language, accent, and patient compliance. Evaluating model performance under these conditions would provide a more accurate estimate of robustness and clinical utility. A practical pathway for real-world validation is a multi-center prospective study, where participating institutions independently collect patient voice samples and evaluate the model in a decentralized manner. In this context, the federated learning framework proposed in this study offers a natural foundation for deployment, as it allows multiple hospitals to collaboratively refine models without sharing sensitive patient data. This approach not only preserves privacy but also ensures that the model continuously adapts to diverse patient populations and clinical settings.
In addition to prospective validation, integration into clinical decision-support systems would require careful calibration and usability considerations. Model outputs should be presented as probabilistic risk scores accompanied by interpretable explanations, enabling clinicians to incorporate predictions into their diagnostic reasoning rather than relying on automated decisions. The stability of explainability observed in this study supports this requirement, as consistent feature attribution enhances trust even when predictive performance varies.
Finally, regulatory and ethical considerations must be addressed before deployment. Clinical-grade validation requires compliance with healthcare regulations, reproducibility across independent cohorts, and ongoing post-deployment monitoring to detect performance drift. These requirements highlight that achieving real-world applicability is not solely a technical challenge but also an operational and regulatory one.
In simple terms, while the current study demonstrates that generalization-aware evaluation and privacy-preserving learning are feasible, translating these findings into clinical practice requires systematic prospective validation, multi-institutional collaboration, and careful integration into healthcare workflows. This progression represents a critical next step toward developing reliable and deployable Parkinson’s disease detection systems.
6. Conclusion
This study presents a comprehensive and realistic investigation of voice-based PD detection by shifting the focus from dataset-specific accuracy to generalization, interpretability, and privacy preservation. Through strict feature harmonization and cross-dataset evaluation, we demonstrate that high performance reported in single-dataset studies often fails to generalize under realistic deployment conditions. The results reveal a consistent performance ceiling imposed by dataset heterogeneity rather than model inadequacy, emphasizing the limitations of accuracy-centric evaluation paradigms. Our analysis shows that frequency-based acoustic perturbation features, particularly jitter-related measures, remain more robust across datasets than amplitude-based features. Explainability analysis confirms that clinically meaningful acoustic biomarkers can be consistently identified even when predictive performance degrades, reinforcing the value of XAI for clinical trust. Furthermore, federated learning is shown to improve generalization robustness while preserving data privacy, highlighting its potential for collaborative healthcare AI without centralized data sharing. By combining cross-dataset validation, explainability, federated learning, ablation studies, and statistical testing within a unified framework, this work provides a stress-tested and clinically grounded assessment of PD voice detection systems. The findings underscore the need for evaluation criteria beyond accuracy and offer practical guidance for designing reliable, interpretable, and privacy-aware diagnostic tools.
Footnotes
Acknowledgement
The authors have nothing to acknowledge.
Ethical considerations
All datasets used and experimental protocols used in this study were reviewed and approved by the Noakhali Science and Technology University Ethics Committee (NSTUEC). The study was conducted in accordance with the ethical standards of the institutional committee (i.e., NSTUEC). The Ethics Clearance Approval Number for this study is NSTU/SCI/EC/2026/578.
Consent to participate
All the authors have voluntarily agreed to participate in this research study.
Consent for publication
All the authors have given their consent for the publication of identifiable details, which can include image(s) and/or videos and/or case history and/or details within the text (“Material”) to be published in this Article.
Author contributions
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used in this study is publicly available. The Dataset 1 (D1) is available at: https://www.kaggle.com/datasets/vikasukani/parkinsons-disease-data-set, Dataset 2 (D2) is available at: https://archive.ics.uci.edu/dataset/301/parkinson+speech+dataset+with+multiple+types+of+sound+recordings, Dataset 3 (D3) is available at: ![]() .For reproducibility, the code will be made available upon reasonable request to corresponding author.
.For reproducibility, the code will be made available upon reasonable request to corresponding author.
Generative AI statement
During the preparation of this paper, Generative AI tool (ChatGPT (OpenAI)) is used for smooth writing, correcting grammar, and enhanced readability. However, the authors have read, reviewed, and checked the final output and take full responsibility of the content. Authors confirm that, ChatGPT (OpenAI) was used only for language refinement and manuscript structuring. No scientific content generation or result interpretation was automated.