
Abstract
Objective
African-born immigrants (ABIs) represent a growing demographic in the United States, constituting nearly half of the foreign-born Black population. They face distinct health challenges, with ABI women experiencing disproportionately high rates of HIV incidence. A critical factor contributing to this health disparity is limited sexual and reproductive health (SRH) literacy. The primary objective of the study was to pilot and evaluate an intervention that employed a culturally responsive, community-led approach to sexual and reproductive health (SRH) education for HIV prevention among ABI women.
Methods
The community-based sexual and reproductive health education was implemented using the African Women Making Healthy Choices (AWMHC) curriculum which consists of 10 modules, delivered across 6 sessions. Sessions were facilitated by AB women and combined didactic and interactive learning elements. The primary outcomes measured were HIV-related health literacy and self-efficacy in protective sexual health behaviors. Ten ABI women were recruited through community-based organizations. Demographic and questionnaire data were summarized using frequencies and proportions. Changes in knowledge and perception of risk associated with HIV were assessed using paired t-tests.
Results
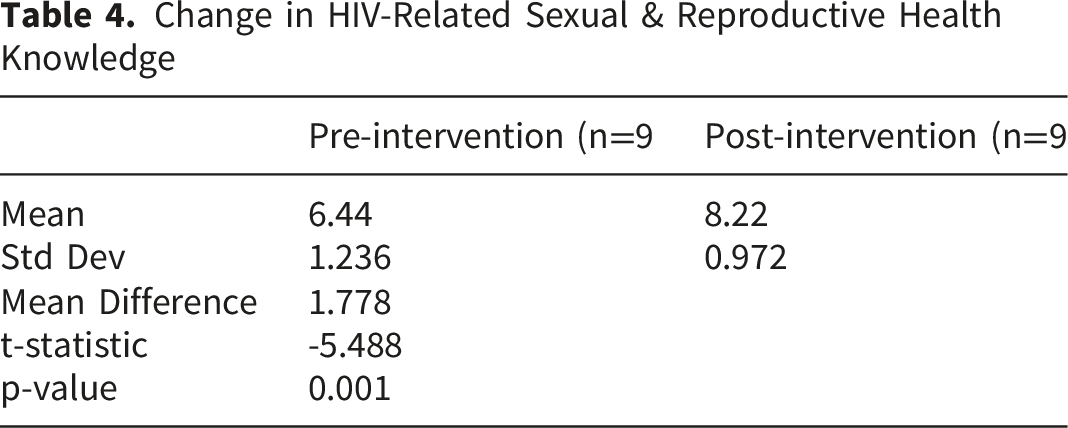
Among the 10 study participants, significant improvements were observed in HIV/SRH knowledge following the intervention, with mean scores increasing from 6.4 to 8.2 out of 10 (p<0.05). Additionally, participants demonstrated enhanced self-efficacy in multiple domains, including condom use negotiation, sexual violence reporting, and healthcare provider engagement. Assertiveness items showing the largest gains related to knowing how to report sexual violence and how to request exams and ask questions of a healthcare provider, each increasing from 6 to 10 affirmative responses.
Conclusion
The findings suggest that culturally tailored SRH education interventions can effectively enhance HIV-related knowledge and self-efficacy among ABI women. Addressing SRH literacy gaps - particularly around fertility, condom use, and sexual rights - appears to be a promising strategy for reducing HIV disparities in this population. The community-led delivery model, grounded in African cultural values, was central to participant engagement and may serve as a replicable framework for scaling up SRH programming with ABI communities. Additional research is warranted to evaluate the intervention’s long-term impact on behavioral outcomes.
Keywords
Background
Historical Trends of Immigration
African-born immigrants (ABIs) in the United States (U.S.) have one of the fastest growth rates compared to other immigrant groups. The U.S. Census Bureau data indicates that the numbers have approximately doubled each decade since 1970. 1 The first two decades of the 21st century saw a dramatic increase of ABIs in the U.S. While there were approximately 600,000 African-born Black residents in 2000, this number more than tripled to reach 2 million by 2019, representing a 246% increase. 1 This significant growth changed the composition of America’s foreign-born Black community - whereas African-born individuals previously made up less than a quarter (23%) of foreign-born Black residents in 2000, they came to represent nearly half (42%) of this population by 2019. 2
Most ABIs in the U.S. originate from sub-Saharan Africa. From 2010 to 2018, the sub-Saharan African population in the U.S. increased by 52 percent, which was significantly higher than the overall foreign-born population growth rate of 12 percent. 3 Minnesota is one of the states with the largest population of ABIs, who are mostly from sub-Saharan Africa. As of 2015 – 2019, Minnesota was the residence for 6% of sub-Saharan ABIs in the U.S. 3 The increasing ABI population in Minnesota has prompted new challenges and unmet needs for this particularly vulnerable group of immigrants. One issue of great concern is that of HIV incidence rates.
HIV in African-Born Immigrants in Minnesota
In 2023, ABIs constituted 3% of the State population, but accounted for 10% of the new cases of HIV diagnosed. 4 In this population. ABI women were even more disparately affected, as they accounted for 23% of newly diagnosed HIV cases among women, by race/ethnicity. 4 This incidence rate represents an improvement in trends as ABI women have accounted for as high as 54% of all new diagnoses among women in MN, in 2015 5 ; which data informed the community-based efforts being reported.
Findings from a preliminary study conducted as a community-based participatory needs assessment, pointed to gender-specific socio-cultural factors as key drivers of HIV transmission and unique barriers to HIV care for ABI women. 6 These included domestic/intimate partner violence; gender-biased stigma; discriminatory cultural beliefs and normative values/expectations based on gender; unprotected sex with husbands who maintain sexual relationships with other men; gender discordance in provider-patient healthcare encounters (preference for female provider); and sexual/reproductive health illiteracy. Of these factors, there was emphasis on limited sexual and reproductive health education as a major issue that had intersection with most of the other factors identified. Poor understanding of sexual and reproductive health was attributed to cultural norms that consider conversations about sex inappropriate, particularly for female members of the community.
HIV and Sexual & Reproductive Health Knowledge
Sexual and reproductive health (SRH) literacy has been associated with more accurate self-assessment of HIV infection risk and shown to influence subsequent sexual behavior.7,8 This relationship aligns with the Health Belief Model’s theoretical framework, which proposes that health-related behaviors are shaped by individuals’ beliefs about health problems, their perceived risk and susceptibility, their assessment of benefits and barriers to recommended actions, and their confidence in their ability to implement these recommendations. 9 Therefore, limited sexual and reproductive health literacy may lead to inaccurate HIV risk perceptions among ABI women, increasing their vulnerability when combined with other risk factors. A community-based sexual and reproductive health educational intervention was strongly recommended as a strategy to address HIV risk in this population.
The primary objective was to pilot and evaluate an intervention that employed a culturally responsive, community-led approach to sexual and reproductive health (SRH) education for HIV prevention among ABI women. The study assessed two key outcomes: HIV-related health literacy (specifically, increased knowledge and understanding); and self-efficacy regarding protective sexual health behaviors.
Methods and Materials - The Pilot
This was a single-cohort, pre-post pilot study examining the feasibility and preliminary efficacy of a culturally responsive, community-based sexual and reproductive health (SRH) educational intervention for HIV prevention among African-born immigrant (ABI) women in Minnesota. The study employed a community-engaged approach, with community members as active partners in both curriculum development, intervention design and program delivery.
Inclusion Criteria
To be a part of the study, participants had to be female, 18 years and older, self-identify as born in Africa (1st generation immigrant) or daughter to parent(s) of African origin, English-speaking, able to read and write in English, and resident in the state of Minnesota. Sexual orientation was not considered in recruitment.
Recruitment and Enrolment
A sample of 10 African-born immigrant (ABI) women who met stated criteria were recruited through community-based organizations and social networks using fliers. At the first session held in the conference facility/community center located in a Church, the purpose of the study was stated and the expectations of participants described. The women were encouraged to ask questions and seek clarification before informed consent was obtained from each participant. Consenting participants then filled out a demographic sheet and a pre-intervention survey.
The Curriculum
The African Women Making Healthy Choices (AWMHC) Curriculum

The curriculum was structured to be culturally responsive and yet flexible to accommodate variances between African cultures. The framework developed was also used in the implementation of the proposed project. This framework leverages the cultural significance of African women as central figures (“the core”) in their families and communities, where they serve as caregivers, educators, leaders, and pillars of support. By recognizing these traditional roles and values around communal well-being, the framework taps into women’s inherent motivation to take action on behalf of their children, families, and communities, even when faced with cultural barriers. The key message for promoting SRH education was then that being empowered with sexual health knowledge, as women, would enable them to, in turn, empower their families, friends, and broader community.
The Intervention
The first module of the African Women Making Healthy Choices curriculum was facilitated at the first session. The ten participants then reached a consensus on what days and times were convenient for subsequent sessions. Participants elected to have the remaining five sessions conducted over a weekend. A more convenient venue - a Mosque - was proposed; to which participants agreed. Each of the sessions lasted for 2-3 hours. After the first session (introductions, ice-breaker activities, getting-to-know “you”, laying down ground rules, and administering informed consent, module 1), the subsequent four sessions each covered two (2) modules from the AWMHC curriculum. Module 10 was covered in the final session, followed by the administration of the post-intervention survey (see Table 1.). Each session was facilitated by two AB women who were also members of the team that put together the AWMHC curriculum used for the intervention. Each session included didactic and interactive learning elements and allowed for questions which stimulated robust discussion. One of the investigators served as a participant observer – taking field notes and weighing in on the discussions. Meals were provided for participants and childcare as needed. Each participant was compensated with a $20 gift card per session.
Data Collection
Demographic information with no personal identifiers was obtained from each participant. A questionnaire (assessing sexual and reproductive health literacy, knowledge and perception of risk associated with HIV/STDs, and assertiveness) was administered pre- and post-intervention. The questionnaire was developed during the curriculum development process.
Data Analysis
The demographic and questionnaire data were summarized using frequencies and proportions. Changes in the outcome measures – knowledge and perception of risk associated with HIV/STDs, and assertiveness – were assessed using paired t-tests. For the knowledge-based questions, a score of one was assigned to each correct response to an item. Similarly, a point was given if a response was in the affirmative for statements regarding self-efficacy regarding sexual encounters. For change in knowledge, only data from the nine participants who completed both the pre- and post-evaluations were included in the data analysis.
Results
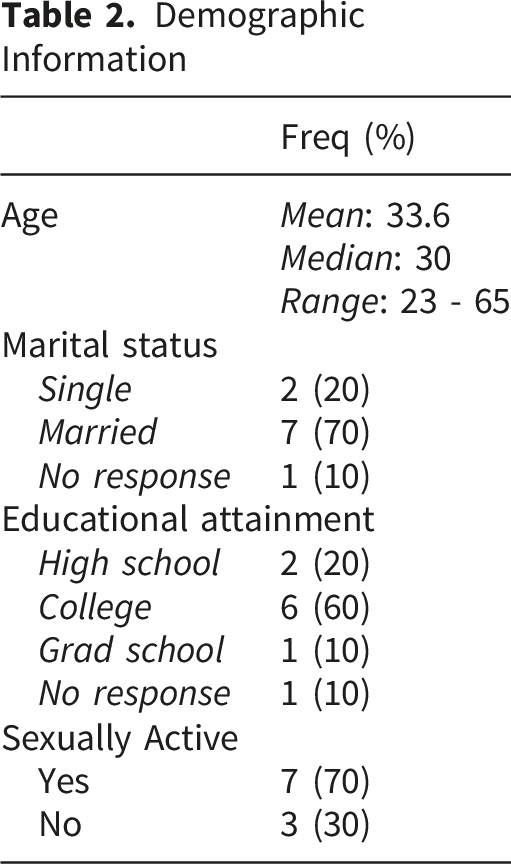
Demographic Information
Demographic Information
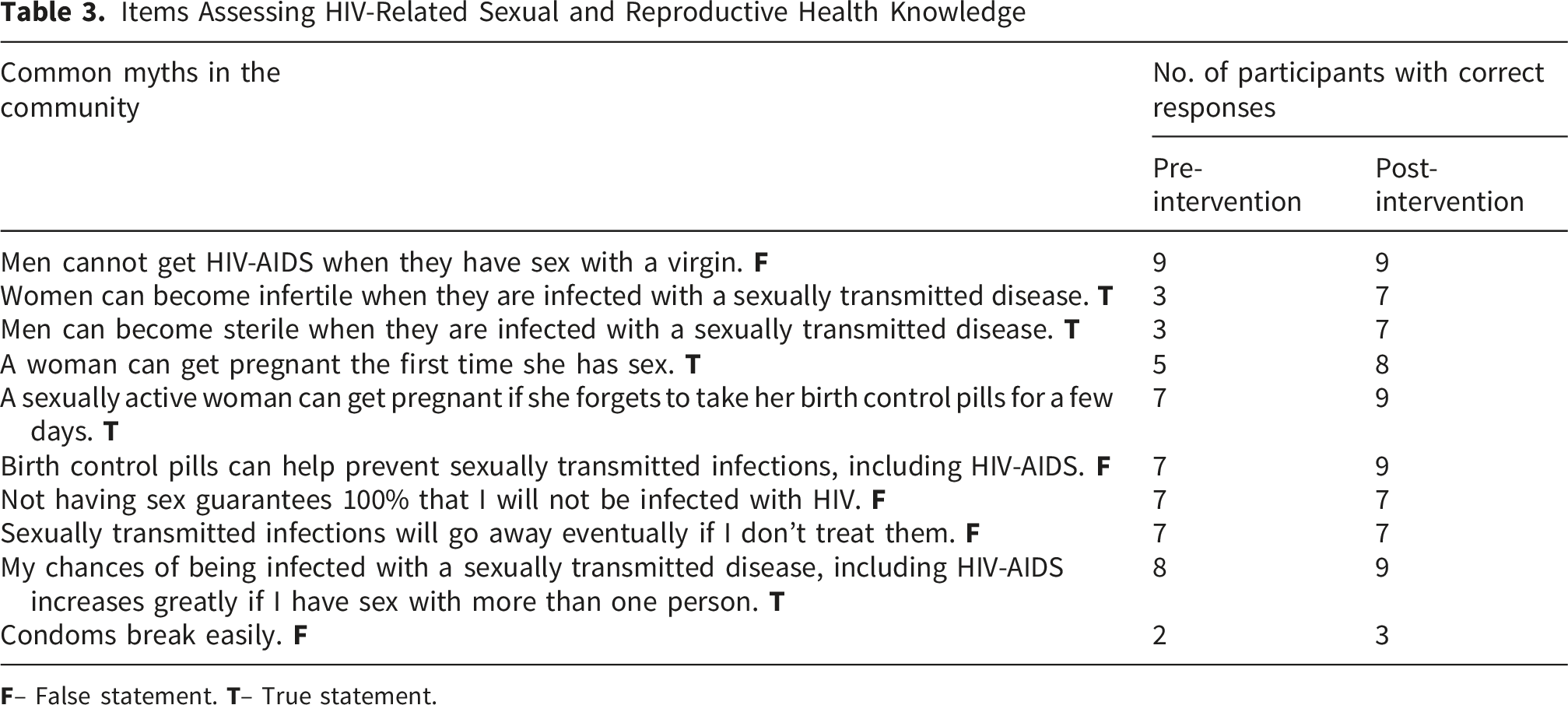
Items Assessing HIV-Related Sexual and Reproductive Health Knowledge
Change in HIV-Related Sexual & Reproductive Health Knowledge
Self-Assessment of HIV Risk Perception and Prevention
Self-Efficacy in Addressing HIV Risk Behaviors [N = 9]

*Limiting factor to self-efficacy in addressing HIV risk.
Assertiveness
Assertiveness - Attitudes and Knowledge Associated With Sexual Health

^One participant’s data excluded due to non-completion of pre-evaluation.
*Negative attitudes associated with sexual health.
Discussion
Demographics
Most of the participants were married. While recruitment efforts did not target married women, it is likely that single women may have felt less comfortable enrolling in the study because being sexually active prior to marriage is frowned upon in African communities. Per cultural values, talking about sex outside marriage is often perceived as being indicative of promiscuity. 12 However, there have been community-based programs targeting adolescent girls and young women to educate them about sexual health and HIV risk, 13 suggesting separate programming for single and married women respectively, when scaling up the current pilot. While the women were from different countries, the cultural backgrounds are sufficiently similar to accommodate single programming with success.
Debunking Myths About HIV and Sexual Health
In assessing knowledge, common myths heard in the community were used. The items that had the least correct response pre-intervention included “Women can become infertile when they are infected with a sexually transmitted disease” (3 correct), “Men can become sterile when they are infected with a sexually transmitted disease” (3 correct), and “A woman can get pregnant the first time she has sex” (5 correct). These items were all related to fertility, suggesting limited sexual and reproductive health literacy even though seven of the 10 participants had a college education. This further supports the premise of this study that HIV risk may be higher among ABI women because of their lack of sexual and reproductive health knowledge. 6
The myth that persisted was that “Condoms break easily”, even following the intervention. While there is possibility of condom breaking, this is often associated with factors extrinsic to the condom including wrong method of use, doubling condoms, “fit”, using an expired condom, and contact with sharp objects. 14 This may be an area for education in this community as there may be a prevalent belief that condoms are susceptible to breaking easily, which would then deter use despite the proven protective benefits, particularly in the prevention of HIV.15,16
Knowledge Gaps
The items showing the largest pre-/post-evaluation improvements (from 6 to 10 participants responding in the affirmative) focused on knowing appropriate actions in specific situations. Two of these questions addressed responses to sexual violence without specifying the perpetrator. Some participants may have interpreted these through the lens of intimate partner violence, as many African cultures often do not acknowledge forced sexual relations within partnerships (e.g. marriage) as rape. 17 Additionally, the significant stigma associated with sexual assault often prevents women from reporting due to shame. The intervention directly addressed these misconceptions by providing women with specific information about reporting options for sexual violence cases.
Other items showing substantial improvement (from 7 to 10 affirmative responses) were related to understanding sexual rights and reproductive anatomy. One of the sessions of the intervention specifically explained the female reproductive system anatomy and educated participants about their sexual rights. These knowledge gaps and the subsequent improvements following the intervention highlight the critical need for comprehensive sexual and reproductive health education in this population.
Strengths and Limitations
A notable strength of this intervention was the intentional concordance of identities, with African-born women serving as facilitators. This approach fostered trust and encouraged open dialogue, as facilitators also leaned into culturally aligned communication modes such as storytelling and use of idioms and proverbs. The informal, community-centered design of the sessions, including the use of familiar community spaces, provision of meals, and availability of childcare, further reduced participation barriers and created an accessible, welcoming environment for a population that may otherwise face significant logistical and cultural obstacles to engagement. Although formal feedback was not systematically collected, informal debriefing revealed that participants found the educational content to be valuable and empowering, and appreciated the safe, communal learning environment as a space for connection and mutual support.
The study had several limitations. First, it utilized a small sample size as this was primarily a pilot study designed to assess feasibility. Second, the research relied on knowledge assessment and risk perception measures as proxies rather than direct behavioral observations. While this approach has limitations, it’s worth noting that perception of risk has been established in previous research as a significant factor that influences health-related behaviors. Finally, the study employed a convenience sampling method - participants were not necessarily individuals at risk of HIV infection, and the majority college-educated - which may limit the generalizability of findings to higher-risk populations and those less educated Additionally, the predominance of married participants may have influenced responses, engagement with the curriculum, and interpretation of HIV/SRH risk, as relationship status and sexual context often shape how ABI women perceive and discuss sexual health. Findings may therefore not also be generalizable to single or unmarried ABI women.
Implications for Practice
The findings from this pilot study have implications for healthcare providers, community health educators, and public health practitioners working with ABI women. The persistence of the belief that condoms “break easily”, even after the intervention, points to the need for targeted, community-engaged, skills-based educational strategies that go beyond didactic instruction. Incorporating hands-on condom demonstration and role play into community-based sessions can address not only knowledge gaps but also self-efficacy for correct and consistent use of condoms. These strategies should be delivered within culturally responsive conceptual frameworks such as the African Queens Health Education Wheel, utilizing community health workers whose cultural backgrounds and values are aligned with this priority population. Approaches should also consider separate programming for those who are single, to provide an environment where they do not feel judged. The improvements in assertiveness, particularly regarding reporting sexual violence and engaging healthcare providers, suggest that community-based interventions that leverage relational trust, trainer-trainee cultural concordance, and safe learning spaces, can increase self-efficacy in limiting risk associated with sexual behavior and advocating for self. Community-engaged approaches should therefore be encouraged.
The significant pre-intervention deficits in fertility-related knowledge, despite most participants having college degrees, demonstrate that formal education alone does not confer SRH literacy, especially in populations that have been historically discouraged from having discussions around sexual health. Clinical encounters therefore represent an underutilized opportunity for SRH education. Healthcare providers serving ABI women should be equipped to integrate culturally sensitive SRH counseling into routine visits, thus normalizing conversations about reproductive anatomy, contraception, and the consequences of sexually transmitted diseases.
Conclusion
The findings suggest that culturally tailored SRH education interventions can effectively enhance HIV-related knowledge and self-efficacy among ABI women. Addressing SRH literacy gaps appears to be a promising strategy for reducing HIV disparities in this population. Subsequent studies should consider enrolling larger samples and accounting for differences in participants’ relationship status and whether or not they are sexually active, through purposive stratification or targeted subgroup programming, to more precisely capture how these contextual factors influence SRH learning and perception of HIV risk. Additional research is also warranted to evaluate the intervention’s long-term impact on behavioral outcomes.
Footnotes
Acknowledgement
We acknowledge the contributions of the women who facilitated the educational sessions and all the participants.
Ethical Considerations
This study was reviewed and approved by the University of Minnesota Institutional Review Board.
Consent to Participate
Written informed consent was obtained from all the study participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the lead author’s startup funds.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this pilot study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.