
Abstract
We report a two-year-old patient with isomerism of the right atrial appendages, a functionally univentricular heart, and associated totally anomalous pulmonary venous connection. The unusual finding was an intrapulmonary course of the vertical vein. We discuss the anatomical findings, management, and outcome.
Introduction
Patients with isomerism of the right atrial appendages and functionally univentricular hearts (UVHs) of necessity have associated totally anomalous pulmonary venous connections (TAPVCs), even when the veins return directly to the heart. This feature increases the risks of univentricular palliation. 1 If unobstructed, and the venous return is to the heart, then the protocol for management need not be changed. Presence of supracardiac, infracardiac, or mixed types of connection, however, requires surgical attention. The supracardiac and infracardiac variants usually unite into a common pulmonary venous confluence, which then drains via a vertical vein. Such a vertical vein can, rarely, course within the pulmonary parenchyma. 2,3 We recently encountered such a patient and discuss here the anatomical findings, management, and outcome.
Case Report
A 2-year-old male patient, weighing 10 kg, presented with cyanosis on crying, which had been present since the age of 3 months. The parents also reported poor weight gain and had noted delayed developmental milestones. Physical examination revealed central cyanosis and minimal clubbing. Examination of the cardiovascular system showed the apex beat to be in the right fifth intercostal space, while a pansystolic murmur, graded at four of six, was heard all over the precordium. Preoperative saturation of oxygen in room air was 70%. Chest radiography revealed a right-sided heart, which was mildly enlarged. Transthoracic echocardiography confirmed the right-sided position of the heart, raised suspicion of interruption of the inferior caval vein, and revealed a common atrium, a common atrioventricular valve which connected both sides of the common atrium to a dominant left ventricle, and a hypoplastic right-sided ventricle, which gave rise to both arterial trunks. The pulmonary veins were seen to drain via a confluence, seemingly to the common atrium. The right and left pulmonary arteries were confluent and of good size. There was evidence of severe valvar and infundibular stenosis. Cardiac catheterization revealed saturation of 90% in the superior caval vein and 74% in the left ventricle. The right ventricular systolic pressure was 110 mm Hg. The catheter could not be negotiated into the pulmonary arteries, so we were unable to measure the pulmonary arterial pressures nor calculate the pulmonary vascular resistance. Left ventricular injection was seen to fill both the aorta and the pulmonary trunk. The pulmonary arteries were confluent and of good size. There was evidence of severe valvar and infundibular stenosis. Computed tomographic angiography (Figures 1 –3) was performed for further delineation of the pulmonary venous anatomy. This revealed right bronchial isomerism (Figure 3), a centrally located liver, a right-sided gastric fundus, bilateral atrial appendages of right morphology with absence of the interatrial septum, and bilateral superior caval veins (Figure 1). The left-sided caval vein, which was larger than the right, drained to the left-sided half of the common atrium. The inferior caval vein was shown to drain centrally, ruling out the possibility of interruption and azygous continuation. The pulmonary veins drained into a common retrocardiac vein, which continued as a tortuous intrapulmonary vertical vein that terminated in the medial aspect of the right-sided superior caval vein (Figure 2). The right ventricle was hypoplastic and gave origin to both arterial trunks. The left ventricle was the dominant ventricle and was connected to the common atrium by a common atrioventricular valve. The atrioventricular connection, therefore, was double inlet left ventricle via a common atrioventricular valve. The aorta, anterior to the pulmonary trunk, continued in right-sided location to become a right-sided aortic arch with mirror-imaged branching, and then a right-sided descending aorta. The pulmonary trunk itself was of 11 mm diameter, while the right and left pulmonary arteries measured 12 and 9 mm in diameter, respectively. The patient was referred for construction of a bilateral bidirectional superior cavopulmonary anastomosis (BDG) and repair of the supracardiac TAPVC. We explained in detail the complex cardiac anatomy to the family, emphasizing the possibility of poor outcomes in both the immediate and long term. We offered then the choice of not opting for surgery, but having considered the situation, they asked us to proceed with surgical treatment.
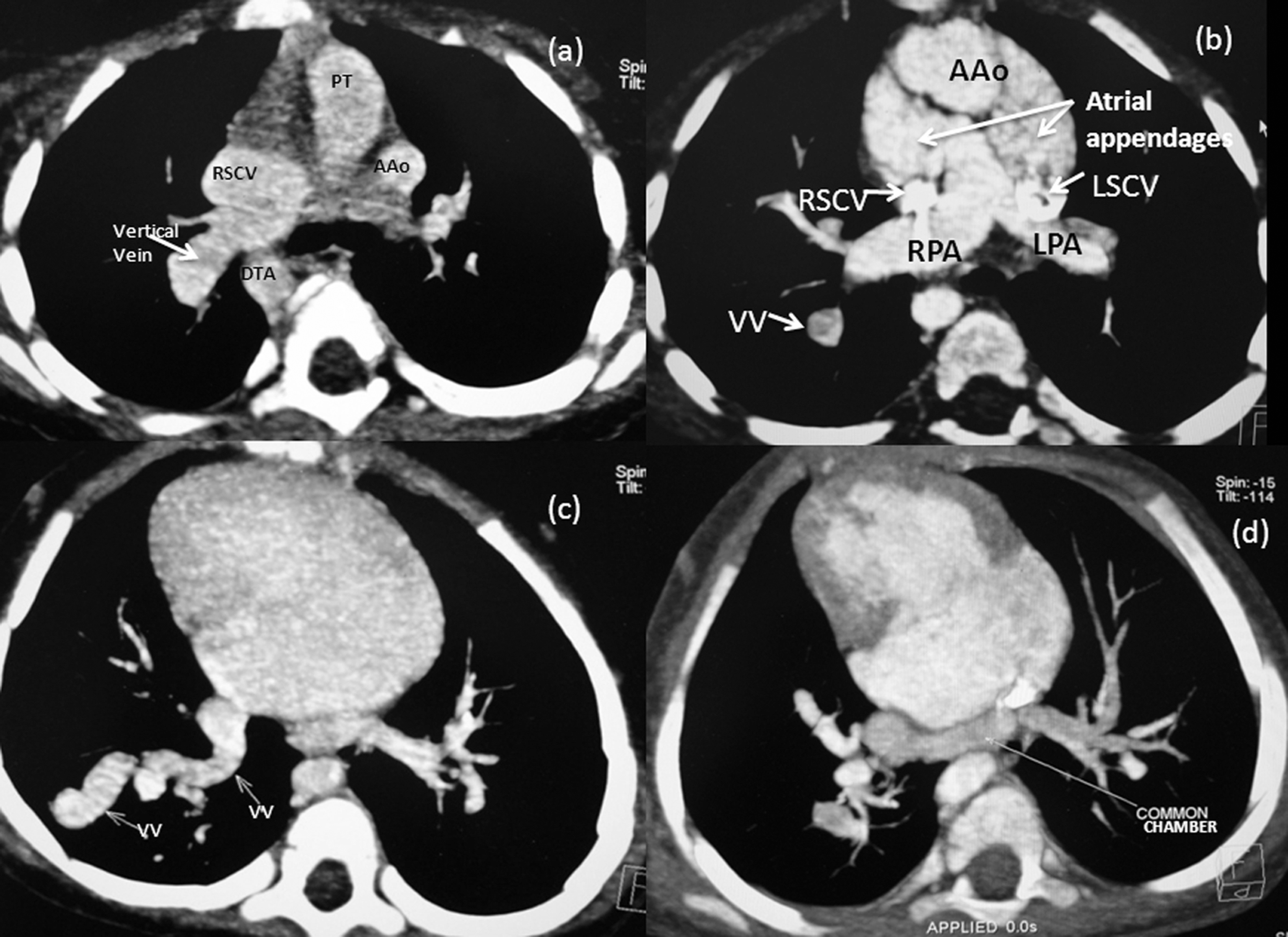
Computed tomography (CT) angiography—oblique axial images showing all pulmonary veins draining into a confluence behind the common atrium (D). This confluence continues on the right as a vertical vein (VV) with a tortuous intrapulmonary course (B, C), finally draining into right superior caval vein (SCV) superiorly (A).

The oblique coronal volume rendered computed tomography (CT) angiographic image shows the tortuous intrapulmonary vertical vein (VV) on right side, draining into the right superior caval vein (SCV). RBr indicates right bronchus; RPA, right pulmonary artery.
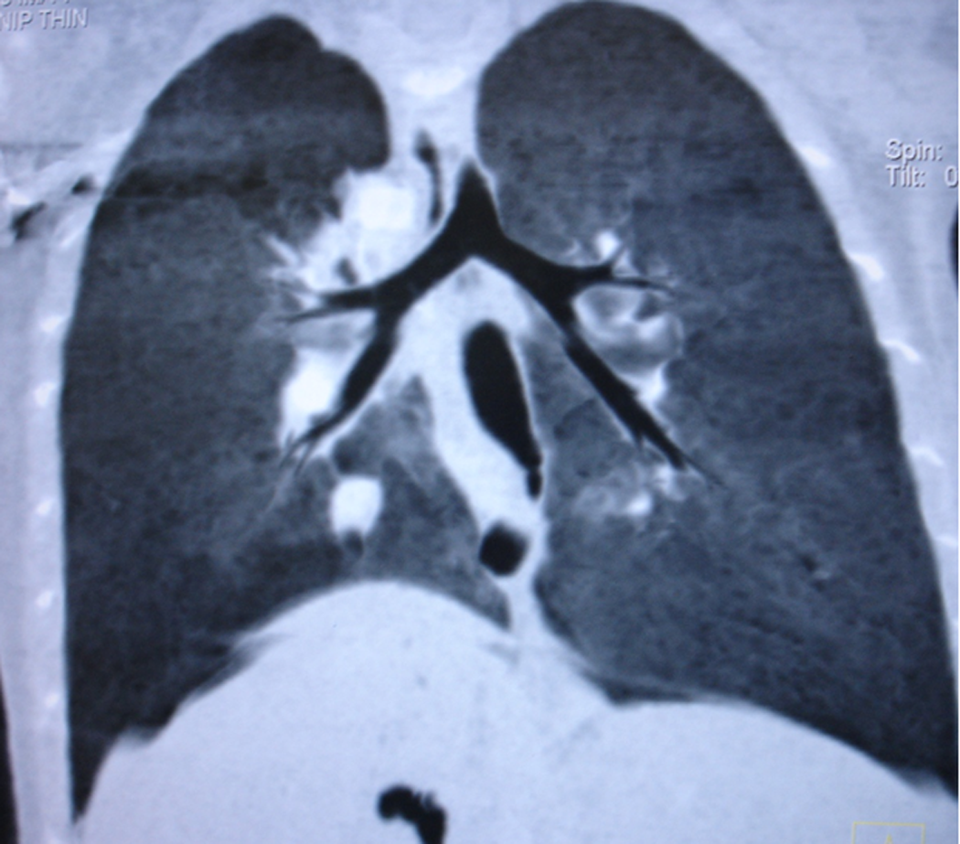
The coronal minimal intensity projection computed tomography (CT) image shows bilateral right bronchial morphology.
Surgical Technique and Course
Following a standard midline sternotomy, the caval veins and pulmonary arteries were dissected, and the drainage of the pulmonary veins through a tortuous vertical vein to the right-sided superior caval vein close to its atrial termination was confirmed. The atrial appendages were seen on both sides of the arterial pedical, but the left-sided appendage was bifid, giving a spurious impression of juxtaposition. Both appendages were broad and triangular, having wide junctions with the common atrial chamber, thus confirming the presence of isomerism of the right atrial appendages. After systemic heparinization, cardiopulmonary bypass (CBP) was established by cannulating the aorta and the right-sided portion of the common atrium. The azygous and hemiazygous veins were ligated and divided. The common pulmonary vein was small in size and was not in close proximity to the common atrial chamber. Noting this anatomy, we opted for an alternative form of repair. The right superior caval vein (RSCV) was divided between two clamps approximately 3 mm above the drainage of the vertical vein. The cardiac end was then closed with a continuous 7-0 polypropylene suture, thus channelling the vertical vein into the heart and providing unobstructed pulmonary venous return. Despite adequate mobilization of the RSCV and the RPA, a considerable gap remained to be bridged between these two structures. This was achieved by inserting a cryopreserved brachiocephalic arterial homograft 3 cm in length and 10 mm in diameter, chosen from our own tissue valve bank, and thus completing the right-sided Glenn anastomosis. Following this, the left superior caval vein (LSCV) was divided between clamps, its cardiac end was oversewn, and the cranial end was anastomosed to the LPA in an end-to-side fashion to complete the left-sided Glenn anastomosis. The patient was uneventfully weaned off CPB on an inotropic support of 5 mcg/kg per min of dopamine, and 0.5 mcg/kg per min of sodium nitroprusside. A cannula placed in the right internal jugular vein showed the venous pressure to be 16 mm Hg, with a nonpulsatile trace. The systemic pressure was 100 mm Hg, and the systemic saturation on 60% fraction of inspired oxygen (F
Discussion
The association of totally anomalous pulmonary venous connection and a functionally univentricular heart, typically seen in patients with isomeric right atrial appendages, is known to increase the risks of univentricular palliation. Patients with this combination often have a difficult postoperative course because of alterations in pulmonary vascular resistance, which may take a considerable time to return to the normal range so as to permit an adequate function of the univentricular pathway. 1 Although there are numerous studies detailing the features of this combination, the association of an intrapulmonary course of the vertical vein draining the lungs is most unusual. 2,3 In one study, which collected four patients with right isomerism and TAPVC, all had an intrapulmonary vertical vein, and in none was the intraparenchymal course demonstrated by transthoracic echocardiography. 2 All these four patients died. We have previously seen and reported this combination in a 20-year-old adult patient who underwent a successful bidirectional Glenn shunt without CPB. In contrast to the other reported patients, who have been shown to have either a hypoplastic pulmonary venous connection, or else an obstructed intraparenchymal pathway, the intrapulmonary part of the vertical vein, and its subsequent drainage into the LSCV, was large and unobstructed in our adult patient, thus facilitating successful palliation. 3 Our current patient was clearly a candidate for univentricular repair, and the best surgical option would have been construction of a superior cavopulmonary anastomosis (bidirectional Glenn shunt), combined with an anastomosis between the common pulmonary vein and the common atrium. If the latter could be successfully achieved, it would have the advantage of providing unobstructed pulmonary venous return to the heart by minimizing the resistance in the circuit. The small size of the pulmonary vein, coupled with the distance between the venous confluence and the common atrium, precluded this approach. Instead, we opted for palliation by constructing the Glenn anastomosis by means of an interposed homograft. Subsequent to this procedure, the supracardiac TAPVC was converted into an unobstructed type of cardiac return, with no physiological effect on the univentricular physiology. One theoretical disadvantage of this form of repair is that it adds resistance to the pulmonary venous circuit since the pulmonary venous return still needs to pass through a long and circuitous vertical vein into the cardiac stump of the RSCV. Serial postoperative echocardiograms, nonetheless, showed unobstructed drainage of the pulmonary venous return into the common atrium.
As has been reported in the previously described cases, however, the postoperative outcome was punctuated by numerous problems. These were addressed to in a timely fashion, but the patient eventually died due to sepsis. The finding of an intrapulmonary vertical vein is seen only, as far as we are aware, in patients with right isomerism. It should, therefore, be anticipated in this setting, albeit that computed tomography (CT) angiography may be needed accurately to delineate the anatomy, thus preparing the way for potential successful surgical palliation. Because of the potentially poor immediate and long-term outcome in such patients, however, it is always important to counsel the families in detail and offer them the option of not choosing to proceed with surgery in these circumstances.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.