
Abstract
Surgical management of truncus arteriosus, or common arterial trunk, has expanded over the past three decades to include earlier surgical intervention, initially during infancy and now chiefly in the neonatal period. Many studies have shown that preoperative truncal valve insufficiency is an independent risk factor for mortality. We herein present the case of a five-month-old boy with severe truncal valve insufficiency who underwent repair of common arterial trunk and prosthetic replacement of the truncal valve with associated annular enlargement after initial stabilization in the newborn period via palliative bilateral pulmonary artery banding. We believe that initial bilateral pulmonary artery banding represents a viable option for some cases of common arterial trunk involving truncal valve insufficiency.
Keywords
Introduction
Truncus arteriosus, or common arterial trunk, is a rare congenital cardiac malformation representing fewer than 3% of all congenital heart malformations. 1 -3 Since the first successful surgical repair of common arterial trunk was performed in 1967, various methods of reconstruction have been developed. Repair of common arterial trunk can now be accomplished with a less than 5% risk of operative mortality. However, surgical management of patients with common arterial trunk is often complicated by the presence of truncal valve (TV) insufficiency. Many studies have shown preoperative truncal valve insufficiency to be an independent risk factor for mortality. 1 -4 We present herein a successful treatment of a case of common arterial trunk with severe truncal valve insufficiency, in which bilateral pulmonary artery banding (BPAB) was used prior to definitive repair that included TV replacement with a mechanical prosthetic valve.
Case
A 2,604 g full-term, male newborn without any chromosomal abnormality or syndrome was delivered to a 38-year-old mother. Fetal echocardiography at 39 weeks of gestation suggested truncus arteriosus (common arterial trunk) of Collett and Edwards type 2, with TV stenosis and regurgitation. At birth, echocardiography confirmed this diagnosis, including a ventricular septal defect (VSD) and an atrial septal defect (ASD). The TV annular diameter was 9.7 mm. The velocity through the TV was 2.77 m/s, and severe TV regurgitation was observed. Nitrogen inhalation was initiated due to pulmonary overcirculation. On postpartum day 3, BPAB was performed using ligation clips (Horizon clip ML; Teleflex Medical Inc, Research Triangle Park, North Carolina) as reported elsewhere
5
(postbanding right pulmonary artery 1.3 mm; left pulmonary artery 1.3 mm). On postpartum day 14, readjustment of the pulmonary artery banding was needed due to arterial desaturation. Two 1.8-mm clips were applied to the bilateral pulmonary arteries to achieve an arterial blood gas with Pa
The postoperative course was uneventful except for an increase in the brain natriuretic peptide (BNP) level from 120 to 452 pg/mL. The severity of truncal valve insufficiency showed no remarkable change. Administration of angiotensin-converting enzyme inhibitor was associated with decrease in the BNP level to 268 pg/mL over time and enabled the patient to be discharged with satisfactory hemodynamic status. Cardiac catheterization three months after banding revealed that pulmonary arterial pressure distal to the bands was 21 mm Hg in the left pulmonary artery and 10 mm Hg in the right pulmonary artery. The left coronary artery orifice was noted to be positioned abnormally toward the right (Figure 1). A preoperative echocardiogram showed the left ventricular (LV) diastolic diameter of 15.9 mm, the systolic diameter of 11.5 mm, and the LV ejection fraction of 62.2%. There were four TV leaflets and a subaortic-type VSD of 12.6 mm in size. The TV leaflets were dysmorphic and showed poor coaptation.
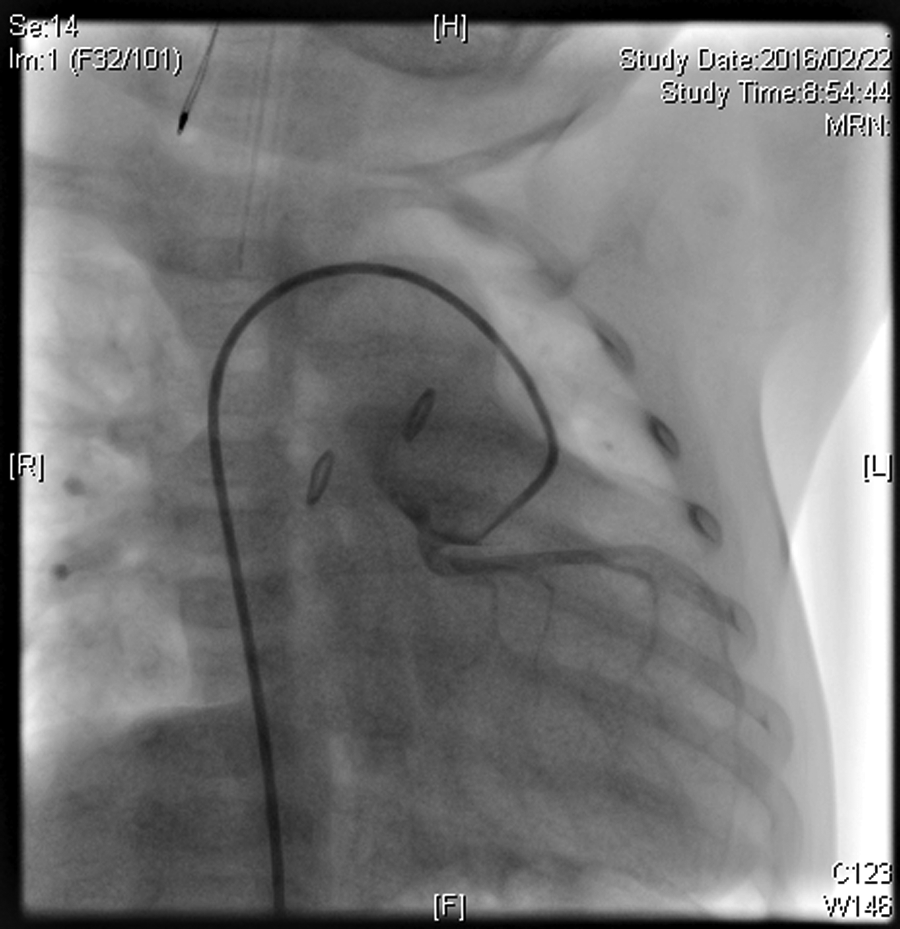
Left coronary angiography revealed abnormal rightward positioning of the left coronary artery orifice.
At 5 months of age and with a body weight of 4.6 kg, the patient underwent reparative surgery. Through a median sternotomy approach, cardiopulmonary bypass was established with ascending aortic perfusion and bicaval drainage. Both antegrade and retrograde cardioplegia were used to obtain cardiac arrest. An aortotomy was performed to divide the pulmonary arteries from the common trunk and to provide access to the TV. The left coronary artery was observed to originate above the dorsal right-sided cusp and ran along the TV annulus across the commissure (Figure 2). A truncal valvuloplasty was considered, but this was ruled out due to the possibility of distorting the course of the left main coronary artery. Instead, a prosthetic valve (SJM Regent Mechanical Valve, St. Jude Medical, Inc., St. Paul, MN, USA) was used to replace the TV. Annular enlargement was unavoidable in order to insert the prosthetic valve. The TV annulus was incised by an aortotomy that extended into the right ventricle using a method similar to that of Konno. 6 Three-quarters of the sewing ring of the prosthesis was sutured to the original truncal annulus and one-quarter was sutured to the top of the VSD patch. After the ASD was closed by direct suture, the right ventricular outflow tract was reconstructed using a 12-mm Polytetrafluoroethylene (PTFE) conduit with trileaflet valve and bulging sinuses. 7 After the patient was safely weaned from cardiopulmonary bypass, an intermittent atrioventricular block was transiently observed but improved spontaneously. After hemostasis was achieved, the skin was closed while the sternum was kept open. Delayed sternal closure was performed on postoperative day 4. Warfarin was administrated as an anticoagulant. Postoperative echocardiography revealed that the diastolic diameter, systolic diameter, and ejection fraction of the left ventricle were 10.8 mm, 18.2 mm, and 79%, respectively. No LV outflow tract stenosis was observed. The patient was discharged without any complication on postoperative day 21.
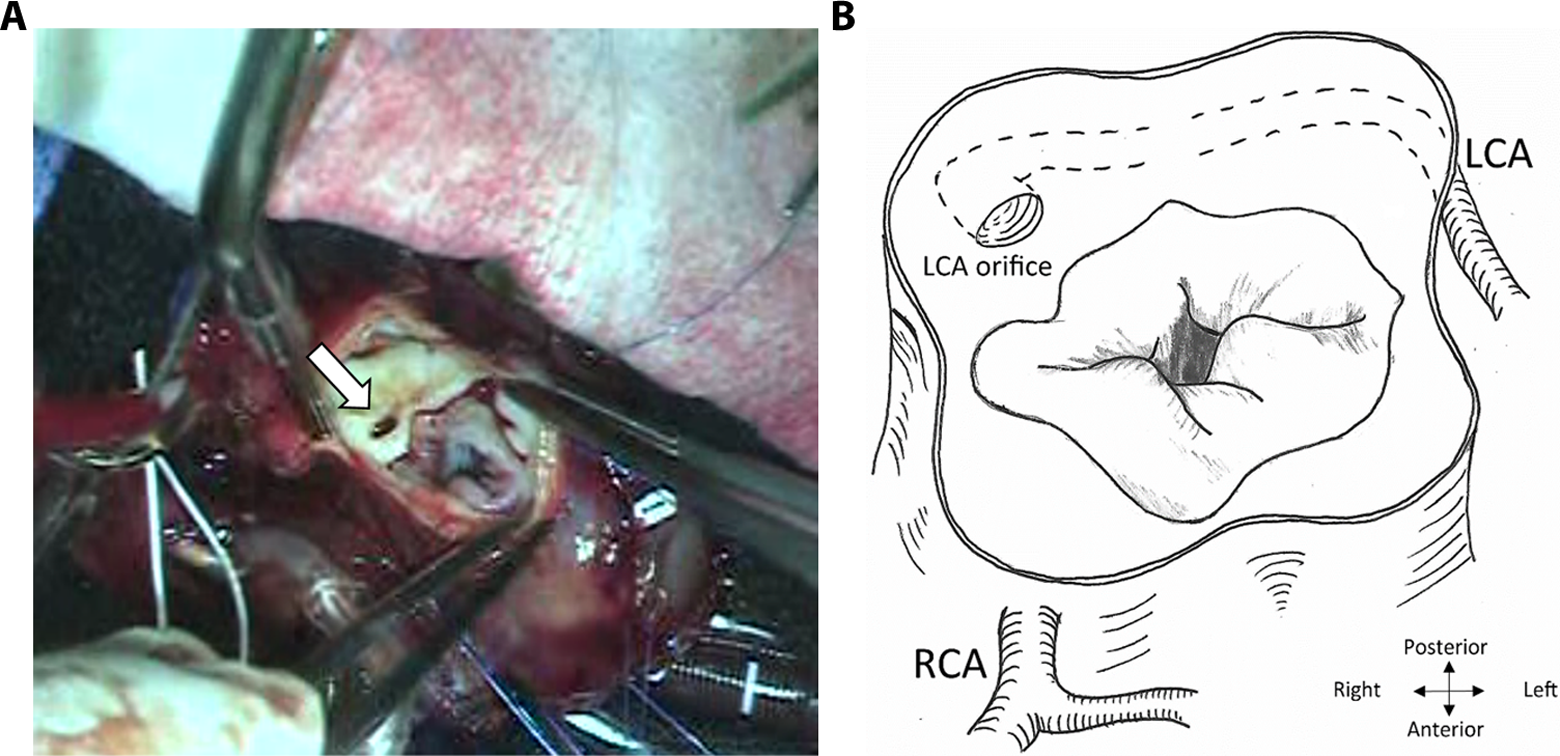
A, The surgeon’s view revealed a dysmorphic truncal valve. The left coronary orifice (arrow) can be seen. B, The schematic anatomy of the truncal valve in this patient showed the presence of a dysmorphic quadricuspid truncal valve with the left coronary artery running along the truncal valve annulus.
Discussion
For the past three decades, most patients with common arterial trunk have been managed by early primary repair, predominantly as neonates. 1 -4 One of the many complicating factors encountered in repair of common arterial trunk is the presence of truncal valve dysfunction, including regurgitation, which reportedly occurs in 14% to 28% of cases. 3 Several single institutional studies have identified preoperative truncal valve insufficiency as a risk factor for mortality. 1 -4 Freedom from reintervention on the truncal valve was 70% at 5 years and 50% at 7 years after initial valve repair. In that study by Henaine et al, initial moderate or severe TV insufficiency was shown to be a risk factor for late truncal valve surgery or late severe truncal valve insufficiency in a multivariate logistic regression analysis, though it was not shown to be associated with early mortality. 4
Performing TV surgery (repair or replacement) at the time of initial repair of common arterial trunk with significant TV insufficiency remains controversial. Mild to moderate regurgitation is usually tolerated well postoperatively after the reduction in the volume overload. 2 Some authors have suggested that truncal valve repair should be the first option in cases of common arterial trunk with severe TV insufficiency because it is effective and durable. 4
Rajasinghe and associates 1 have shown that moderate or greater TV insufficiency in neonates is a significant risk factor for late death and for earlier need for truncal valve replacement, further supporting an aggressive repair policy for initial truncal valve insufficiency of moderate or greater severity. Truncal valve replacement can be achieved with modest risk and should be carried out when severe regurgitation refractory to valvuloplasty is present. 2 Good short-term results using the aortic allograft in TV replacement have been reported, but long-term results of allografts in children have been disappointing. 8
Currently in Japan, staged repair for common arterial trunk tends to be preferred over single-stage neonatal repair. According to a national database, 9 42 cases underwent repair of common arterial trunk in 2013. Of these, 21 repairs were performed during infancy and 14 were performed at 1 to 17 years of age. Only six neonatal patients were considered for initial repair. On the other hand, BPAB was performed in 30 cases (20 as neonates and 10 during infancy). Compared to other countries, homografts are not readily available in Japan. Performing BPAB prior to a complete repair of common arterial trunk is therefore a practical strategy.
Using BPAB as a temporizing measure until the performance of a staged repair including replacement of the TV was successful in this case. The BPAB was advantageous not only for avoidance of neonatal cardiopulmonary bypass but also in order for the patient to gain sufficient body weight to allow the insertion of a prosthetic valve at the time of definitive repair. Furthermore, a patient with palliated common arterial trunk can be discharged from hospital after BPAB without any intravenous drips. This strategy may be considered as one of the initial treatment options for patients with common arterial trunk, even with significant truncal valve insufficiency, although careful follow-up is still required in order to monitor for increased TV insufficiency, ventricular dysfunction, or other hemodynamic compromise.
Footnotes
Authors’ Note
The parents of the patient have consented to the publication of the case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.