
Abstract
Background:
Extracorporeal cardiopulmonary resuscitation (ECPR) is increasingly used to rescue patients with cardiac arrest refractory to conventional therapy, necessitating evaluation of factors that may affect outcomes.
Methods:
A single-center retrospective review of pediatric patients (<21 years old) who underwent ECPR from January 2010 to November 2017. Comparisons between nonsurvivors and survivors, to decannulation and discharge, were made. Factors associated with survival and rate of complications were examined.
Results:
Seventy patients were supported with ECPR. Forty-nine (70%) patients survived to decannulation and 38 (54%) patients to discharge. There was no statistical difference between baseline characteristics of survivors and nonsurvivors, including age at cannulation, weight (kg), time to cannulation (minutes), and total time on extracorporeal membrane oxygenation (hours). Survivors to discharge had significantly higher pH prior to cannulation compared to nonsurvivors (7.11 ± 0.24 vs 6.97 ± 0.21, P = .01). Of all, 23.2% of patients received renal replacement therapy (RRT), 39.4% had significant bleeding, 22.5% had thrombotic complications, and 68.8% had neurologic injury on imaging studies. A greater number of nonsurvivors received RRT compared to survivors to discharge (35.5% vs 10.8%, P = .02). There were no differences in bleeding or thrombotic complications or radiographically established neurologic injury.
Conclusions:
Although ECPR effectively increases overall survival, a better characterization of long-term outcomes is needed.
Keywords
Introduction
Institution of extracorporeal life support (ECLS) during cardiopulmonary resuscitation (CPR), known as extracorporeal cardiopulmonary resuscitation (ECPR), has become an accepted therapeutic modality to rescue patients following refractory witnessed in-hospital cardiac arrest. 1 Cardiac arrest occurs in up to 2% of patients admitted to a pediatric intensive care unit (PICU) 2 and 3% to 6% of patients admitted to a pediatric cardiac ICU. 3 Return of spontaneous circulation (ROSC) is achieved in 78% of these patients, but only 45% will survive to hospital discharge. 4 Furthermore, longer duration of CPR has been associated with decreased survival to discharge, 5 66% in patients with 1 to 3 minutes of CPR and 28% in those with >30 minutes. 4 Furthermore, recent studies demonstrate good neurologic and cognitive outcomes in patients who underwent ECPR. 6 Hence, ECLS has become increasingly utilized during CPR.
The 2016 Extracorporeal Life Support Organization (ELSO) registry reports a 35% and 67% increase in neonatal and pediatric ECPR use, respectively, between 2009 and 2015. 7 Multiple studies in adults have demonstrated improved survival with ECPR compared to conventional CPR (CCPR) with respect to survival to discharge and neurologic impairment. 8,9 These findings have also been demonstrated in the pediatric population with children receiving ECPR having more favorable neurological outcomes compared to children receiving CCPR. 10 The American Heart Association (AHA) has recommended consideration of ECPR in pediatric patients with heart disease when the etiology of the arrest is thought to be “amenable to recovery or transplantation.” 11 Despite the increased utilization of ECPR, there are few established criteria for patient selection, effective deployment, or prognostic factors to govern its use.
The reported survival to discharge for ECPR has ranged from 14% to 56% 5,12 -16 for pediatric patients. Several factors have been associated with nonsurvival from ECPR including renal dysfunction, neurologic complications, high lactate, and longer extracorporeal membrane oxygenation (ECMO) duration. 17 However, identification of these and other potentially modifiable predictors remains an area requiring further study. As the utilization of ECPR becomes more widespread, it is imperative to examine indications, patient selection, and most importantly outcomes to help guide appropriate deployment of this invasive and resource-intensive therapy. To that end, we review our institutional experience with ECPR and evaluate factors that affect survival.
Methods
A single-center, retrospective study was performed after institutional review board approval (IRB# AAAR0525), which included all patients younger than 21 years who underwent ECPR between January 2010 and November 2017. Extracorporeal cardiopulmonary resuscitation was defined as the use of ECMO during CPR for witnessed in-hospital cardiac arrest.
The deployment of ECPR was standardized. The ECMO circuit consisted of 1/4 × 1/16 SMART coated polyvinyl chloride (PVC) tubing pack with a CARDIOHELP System (Maquet Medical Systems USA, Wayne, New Jersey) and a Quadrox-ID Adult PMP Oxygenator (Maquet Medical Systems USA). Circuits were primed with Plasma-Lyte 148. Wet primed circuits and ECMO carts consisting of surgical trays and all sterile equipment necessary for emergent neck, chest, and peripheral cannulations were present in the neonatal ICU (NICU), PICU, and cardiac catheterization laboratory. Two units of packed red blood cells were stored in the ICUs for neonatal cannulations. Patients were heparinized with 100 U/kg prior to cannulation if no strict contraindication to anticoagulation was present. All ECMO cannulation consults were received by a dedicated pediatric ECMO fellow and cannulations performed by the attending pediatric or cardiac surgeon, pediatric surgery and ECMO fellows, and a pediatric perfusionist.
Cannulation location was characterized as operating room, NICU, PICU, or cardiac catheterization laboratory. Any period of ROSC during arrest was noted. Time to cannulation (TTC) was determined from start of compressions to time of ECMO flow initiation. Extracorporeal membrane oxygenation duration was determined from time of flow initiation to decannulation. Daytime cannulation was defined as 7
Underlying cardiac anatomy was defined as normal cardiac anatomy, biventricular congenital heart disease, or single ventricle physiology. It was also noted if patients had undergone cardiac surgery within 72 hours of ECPR cannulation. Presence of underlying diseases included cardiomyopathy and pulmonary hypertension (PHTN). Analyzed laboratory markers collected within 24 hours of cannulation included creatinine (Cr), white blood cell (WBC) count, hemoglobin, hematocrit, platelets, aspartate transaminase (AST), alanine transaminase (ALT), total bilirubin, partial thromboplastin time (PTT), prothrombin time, and international normalized ratio (INR). The worst pH and lactate prior to initiation of ECMO flows was also collected. Vasoactive inotropic score was calculated as described by Gaies et al. 18
Complications on ECMO were categorized as follows: (1) Bleeding complications defined as any bleeding event requiring return to operating room, chest washout, or deviance from the institutional anticoagulation protocol. (2) Thrombotic complications as need for circuit exchange, visible thrombi in oxygenator, or tubing affecting circuit pressures or causing hemolysis. (3) Positive cultures on ECMO included respiratory, urine, blood, wound, or sternal cultures. (4) Renal replacement therapy (RRT): The criteria for RRT initiation included oliguric renal failure, uremia, severe electrolyte disturbances, and metabolic derangements. (5) Stroke defined by the presence of imaging changes on head ultrasound (HUS) or computed tomography (CT) scan while on ECMO or magnetic resonance imaging (MRI) following ECMO decannulation but prior to discharge.
Primary outcome was survival to discharge and secondary outcome was survival to decannulation. We evaluated factors affecting survival and complications of ECMO, specifically receiving RRT, bleeding and thrombotic complications, and rate of neurologic injury as determined by imaging findings.
Statistical Analysis
To understand differences in pre-ECPR patient characteristics and post-ECPR patient outcomes, comparisons between survivors and nonsurvivors to decannulation and discharge were made. Categorical variables were compared using χ2 tests, and continuous covariates were compared using Fisher exact test and Wilcoxon rank sum test where appropriate.
All potential factors that may be associated with receiving RRT were evaluated using univariate logistic regression and reported as crude odds ratios (ORs). Then a multivariable logistic regression model was fit using all clinically relevant and statistically significant factors that were potentially associated with receiving RRT and reported as adjusted ORs. For all logistic regression modeling, model quality and fit were assessed using Akaike Information Criterion and logistic receiver–operative characteristics, respectively.
A univariate cox proportional hazards model was used to assess all potential factors associated with survival to discharge after ECPR and reported as crude hazard ratios (HRs). A multivariable cox proportional hazards model was then fit using all clinically relevant and statistically significant factors that were associated with survival to discharge and reported as adjusted HRs. The proportional hazards assumption was evaluated using Schoenfeld residuals. All statistical analyses were performed using STATA version 14.1 (StataCorp, College Station, Texas, 2016) and a P value of .05 was considered significant for all analyses.
Results
Patients Characteristics
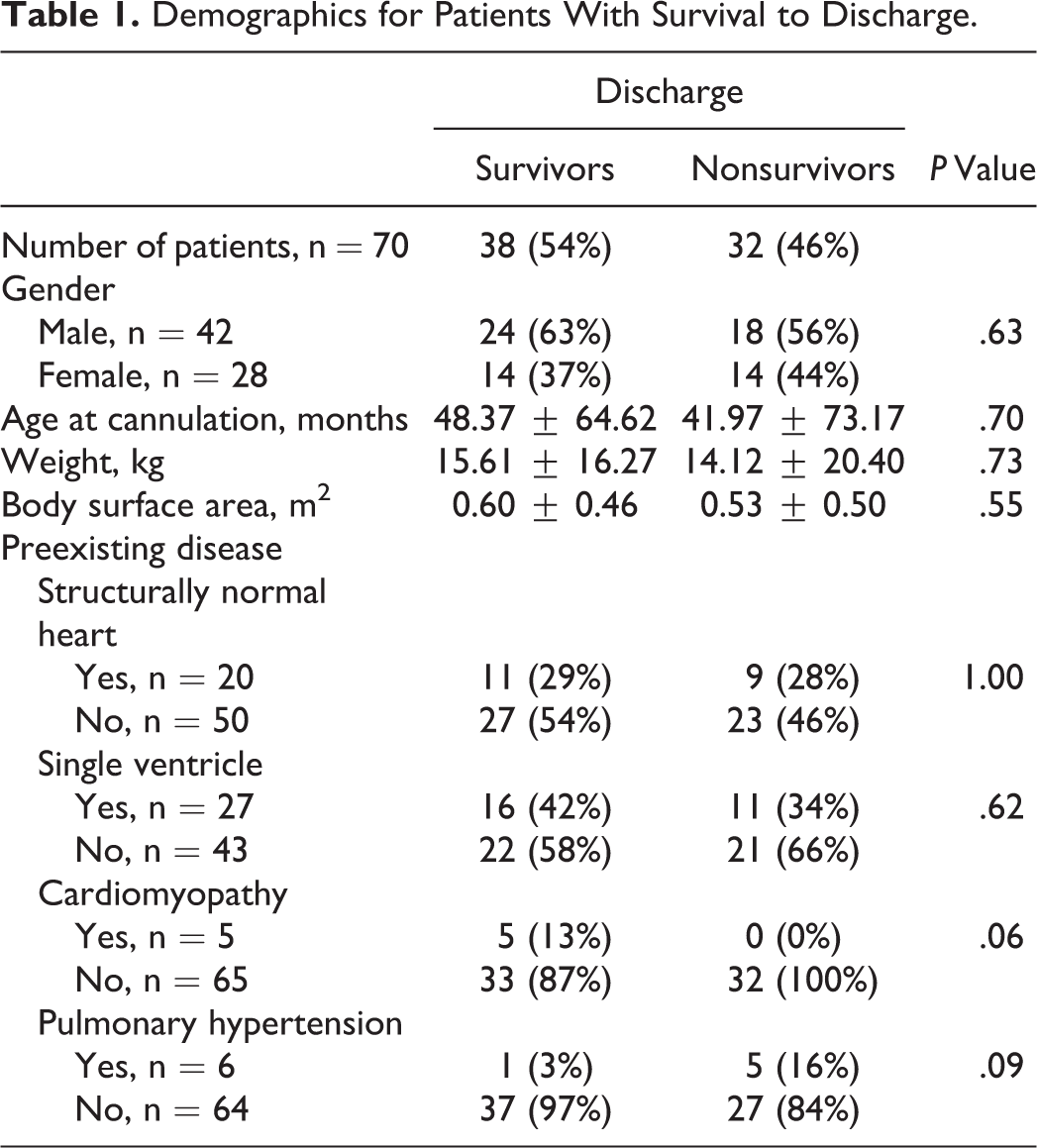
Seventy-one patients were supported with ECPR between January 2010 and November 2017. Fourteen neonates (≤28 days), 28 infants (28-day to 1-year-old), and 29 pediatric patients (1-21 years old) were enrolled in the study. One patient was transferred on ECMO to another institution and was excluded from analysis. Forty-nine (70%) patients survived to decannulation and 38 (54%) survived to discharge. There was no statistical difference between survivors and nonsurvivors with respect to baseline characteristics, including gender, age, weight, and body surface area at the time of cannulation (Table 1, Supplementary Table 1).
Demographics for Patients With Survival to Discharge.
Patient and ECPR Characteristics
Survivors and nonsurvivors to discharge were observed to have similar rates of congenital heart disease and single ventricle physiology (Table 1). Five patients had the diagnosis of cardiomyopathy, all of whom survived to discharge (P = .06). Six patients had PHTN, five were in the nonsurvivors group (P = .09).
The characteristics of ECPR are described in Table 2 and Supplementary Table 2. All patients cannulated in the operating room (n = 2) and cardiac catheterization laboratory (n = 2) survived to discharge. Only 19% (7/27) of patients cannulated in the NICU survived to discharge, compared to 71% (27/39) in the PICU (P < .01). All six patients who experienced any period of ROSC prior to cannulation survived to discharge (P = .02). There was no difference in the mean TTC between survivors and nonsurvivors (62 vs 59 minutes, P = .70) or hours on ECMO (121 vs 167 hours, P = .18). There was no statistically significant difference in cannulation strategy between survivors and nonsurvivors.
Extracorporeal Cardiopulmonary Resuscitation Characteristics for Patients With Survival to Discharge.
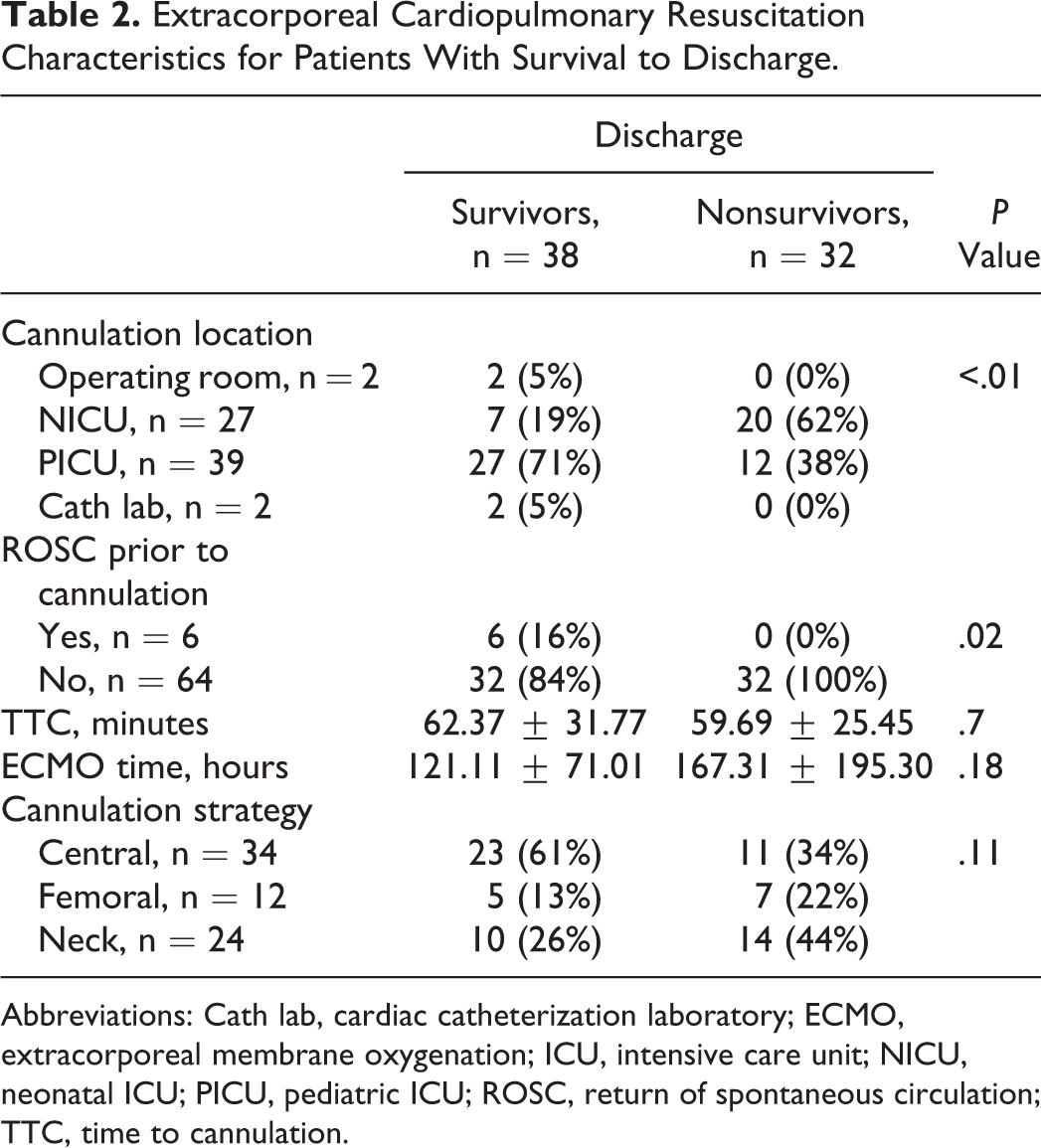
Abbreviations: Cath lab, cardiac catheterization laboratory; ECMO, extracorporeal membrane oxygenation; ICU, intensive care unit; NICU, neonatal ICU; PICU, pediatric ICU; ROSC, return of spontaneous circulation; TTC, time to cannulation.
Laboratory markers prior to cardiac arrest are described in Table 3 and Supplementary Table 3. There was no difference in prearrest Cr, WBC, AST/ALT, coagulopathy (INR, activated PTT), or platelet count between survivors and nonsurvivors to discharge. Of the analyzed laboratory markers, ECPR survivors had a significantly higher pre-ECMO pH of 7.11 compared to nonsurvivors with a pH of 6.97 (P = .02).
Worst Pre-ECMO Parameter for Patients With Survival to Discharge.
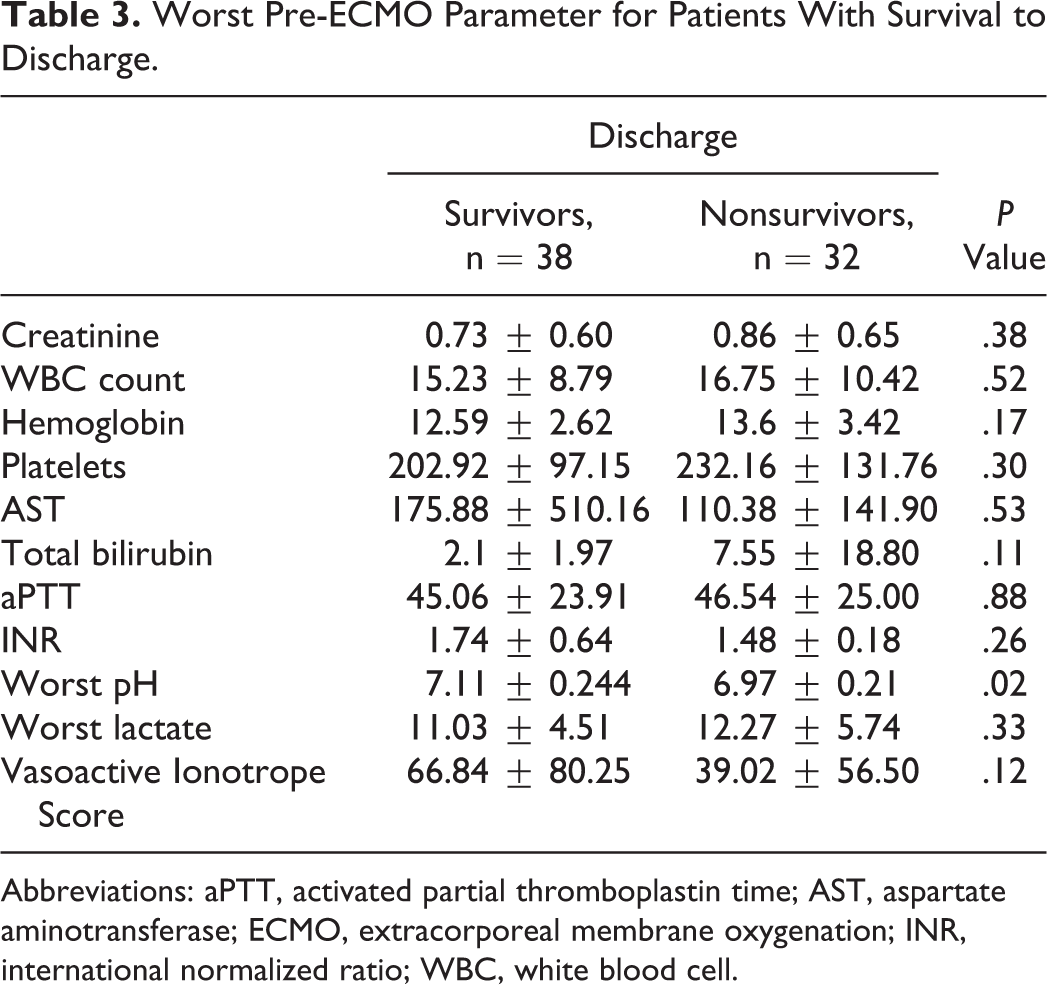
Abbreviations: aPTT, activated partial thromboplastin time; AST, aspartate aminotransferase; ECMO, extracorporeal membrane oxygenation; INR, international normalized ratio; WBC, white blood cell.
Complications on ECMO
Complications while on ECMO, including bleeding, thrombotic, infectious, renal, and neurologic complications, are demonstrated in Figure 1. There was no significant difference in bleeding or thrombotic complications. Twenty-eight (40%) patients had positive cultures on ECMO, of whom 17 were nonsurvivors (P = .05) to discharge. Furthermore, 15 (21%) patients received RRT, of whom 11 were in the nonsurvivors group (P = .02). Median time to initiation of RRT after ECMO cannulation was 53.6 hours (0-218 hours). Only one patient was started on RRT within an hour of cannulation, and this was for the treatment of severe hyperkalemia in the setting of renal failure. Forty-three (61%) patients had imaging findings of stroke while on ECMO, split evenly between survivors (n = 22) and nonsurvivors (n = 21; P = .101).
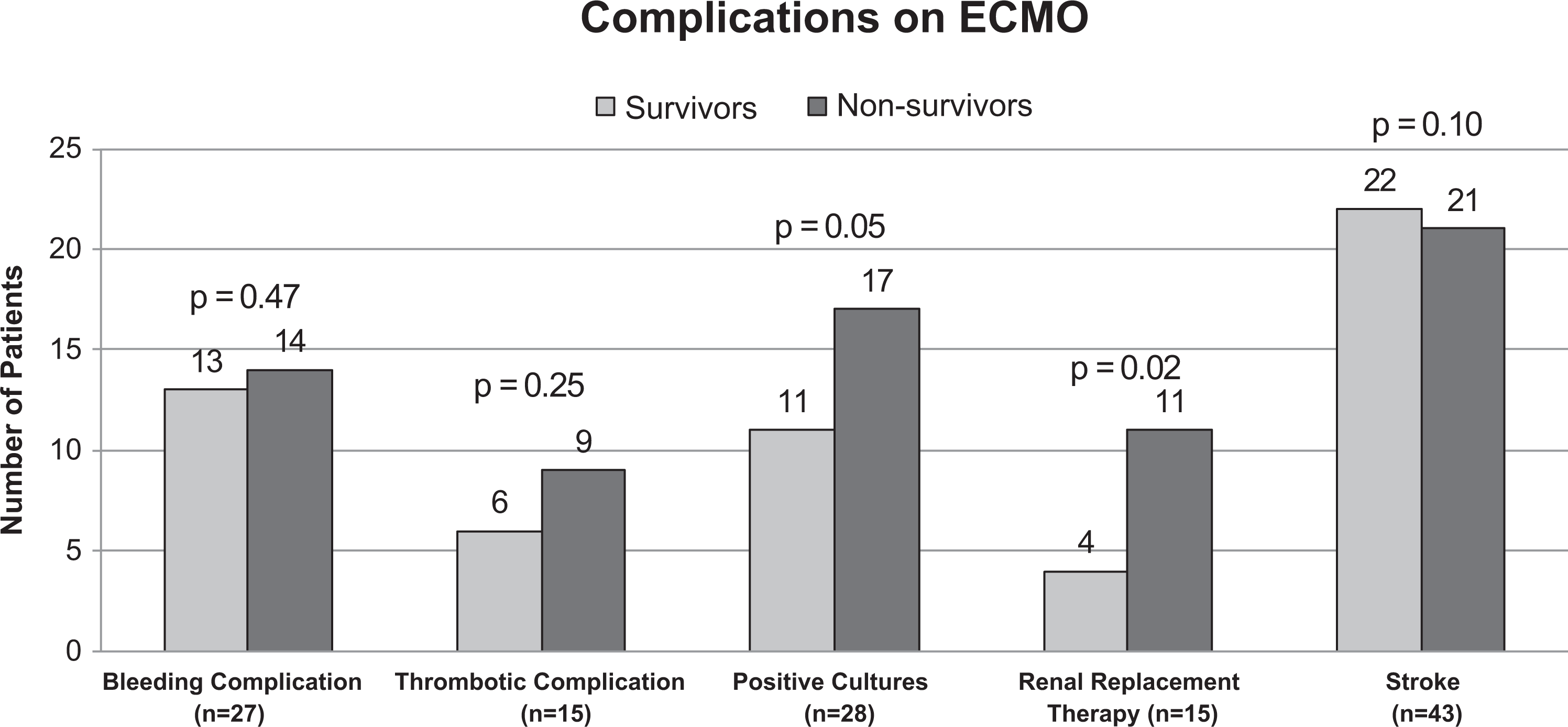
Complications on ECMO. ECMO indicates extracorporeal membrane oxygenation.
A total of 60 patients had 63 imaging studies performed during ECMO support or post-ECMO decannulation: 28 HUS, 16 CT scans, and 19 MRIs. Fifty-two percent (31/60) of patients had imaging findings of ischemic changes/stroke, 3% (2/60) had findings of bleeding, and 8% (5/60) had both ischemic and hemorrhagic findings on imaging. One patient did not have electroencephalographic (EEG) or any imaging but had a clinical examination consistent with a neurologically devastating stroke. Three patients had normal head imaging but flat EEG and clinical examination consistent with significant neurologic injury, concerning for diffuse ischemic injury during arrest. All four of these patients had withdrawal of ECMO. Fifty-five patients had EEG monitoring during their ECMO course. Of these patients, 16 (29%) had EEG evidence of seizures. There was no difference in stroke rate among patients who were cannulated via the neck, femoral vessels, or centrally.
Evaluation of Prognostic Factors Associated With Receiving RRT
A logistic regression analysis was performed for factors associated with requiring RRT (Table 4). Age at cannulation, weight, and duration of ECMO support were all associated with need for RRT. More specifically, we found that for every month increase in age at cannulation, there was a 1% increase in the odds of receiving RRT while on ECMO (OR: 1.01, 95% confidence interval [CI]: 1.00-1.02, P = .01). Similarly, for every additional 12-hour interval on ECMO, there was a 12% increase in the odds of receiving RRT (OR: 1.12, 95% CI: 1.05-1.20, P < .01). Our final multivariable logistic regression model was inclusive of weight (kg), peri-arrest pH, hours on ECMO, and Cr (Table 4). We found that for every additional 12 hours on ECMO, there was an 11% increase in the odds of receiving RRT (OR: 1.11, 95% CI: 0.91-1.14, P < .01), when adjusting for the other three variables in the model. Pre-ECMO Cr value was not found to be significantly associated with receiving RRT after adjusting for the other variables in the model.
Logistic Regression Factors Associated With Receiving RRT.
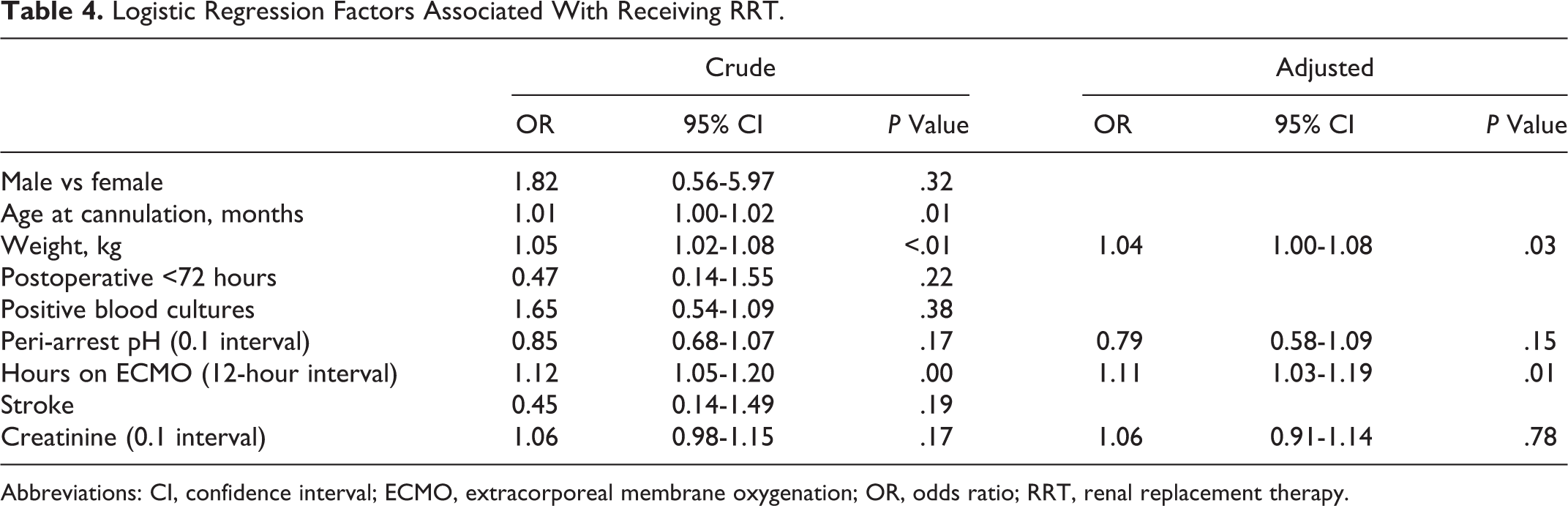
Abbreviations: CI, confidence interval; ECMO, extracorporeal membrane oxygenation; OR, odds ratio; RRT, renal replacement therapy.
Evaluation of Prognostic Factors Associated With Survival to Discharge
A Cox proportional hazard model for factors that may be associated with survival to discharge was performed (Table 5). On univariate analysis, factors associated with discharge included positive cultures on ECMO (HR: 2.06, 95% CI: 1.03-4.14, P = .04) and imaging findings of stroke (HR: 2.74, 95% CI: 1.01-7.43, P = .05). Our final model adjusted for age ≥ 12 months, hours on ECMO, receiving RRT, and imaging findings of stroke (Table 5). Age ≥12 months was found to be protective with a 66% reduction in the hazards of death (HR: 0.34, 95% CI: 0.14-0.87, P = .02) when adjusted for the other three variables in the model. However, receiving RRT (HR: 4.81, 95% CI 1.84-12.58, P < .01) and having evidence of stroke (HR: 3.13, 95% CI: 1.01-8.94, P = .03) were both associated with an increased hazard of death, when adjusted for the other variables in the model.
Cox Proportional Hazards Model for Factors Associated With Survival to Discharge.
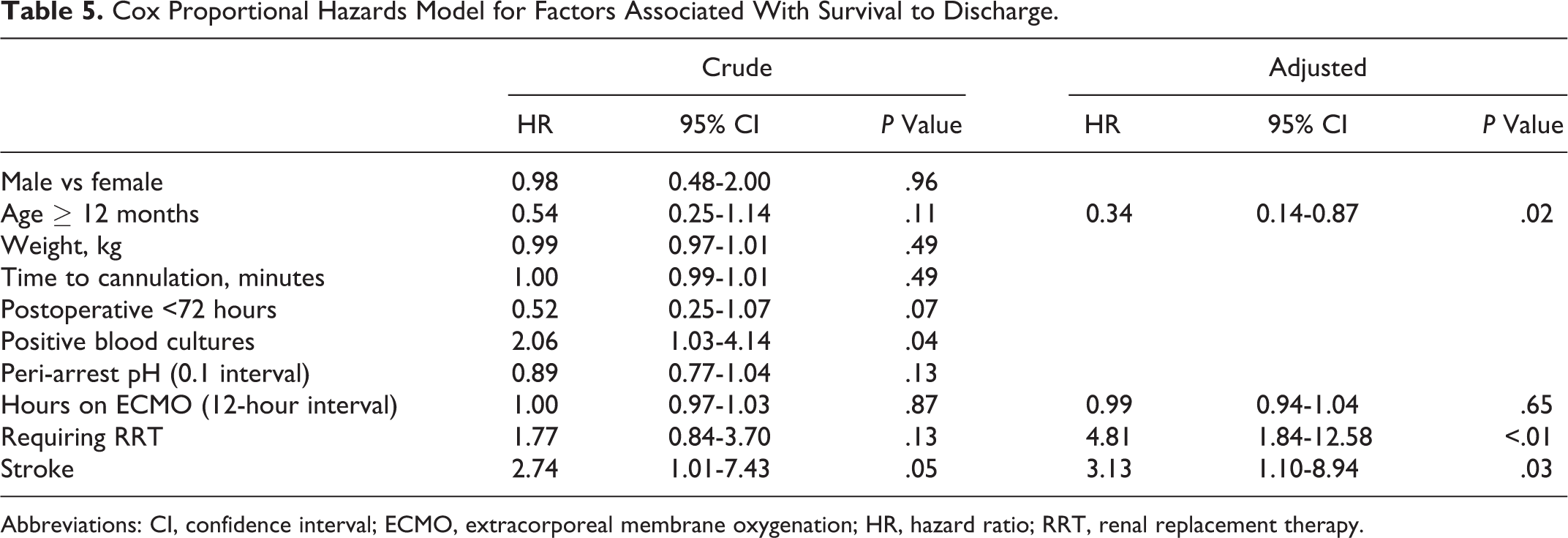
Abbreviations: CI, confidence interval; ECMO, extracorporeal membrane oxygenation; HR, hazard ratio; RRT, renal replacement therapy.
Discussion
While ECPR may be a lifesaving intervention for patients refractory to CCPR, it carries significant risks and use of resources. To our knowledge, this retrospective study is one of the largest single-center studies evaluating pediatric ECPR. The successful use of ECLS in refractory cardiac arrest in adults and children was first demonstrated in the 1990s. 19,20 From 1992 to 2017, 3,879 neonatal and pediatric patients were supported with ECPR in the ELSO registry. 21 This number continues to increase annually. This trend is reflected in our own institutional experience of ECPR, where in 2010, ECPR accounted for only 4% of ECMO cannulations at our institution, whereas in 2017, it accounted for 49% of cannulations.
Cardiac arrest is reported in 1% to 2.2% of neonates and infants admitted to the NICU 22,23 and 2% to 6% of all children admitted to the PICU. 3,24 Reported survival to discharge has varied ranging from 20% to 61% among infants 22,23 and 10% to 44% in the pediatric population. 25 In this retrospective single-institution review, we report 54% survival among ECPR in a heterogenous group of patients. By age groups, we demonstrate 50% (4/8) survival to discharge among neonates aged <28 days, 44% (15/34) in infants, and 66% (19/29) in pediatric patients. The survival reported here is on par with or superior to the numbers reported in the international summary of the 2018 ELSO Registry report of a 40% survival to discharge or transfer in neonates and 42% in pediatric patients receiving ECPR. 21
The benefit of ECPR on survival over CCPR has been well defined in the adult population. 26 -28 However, the literature is sparse in children. A 2016 evaluation of the AHA’s Get With The Guidelines–Resuscitation registry revealed that, for children with in-hospital CPR ≥10 minutes duration, ECPR has been associated with improved survival to hospital discharge and survival with favorable neurologic outcomes. 10 Between 2000 and 2011, they identified 3,765 patients; of whom, 591 (16%) received ECPR and 3,165 (84%) received CCPR. Survival to hospital discharge was higher with ECPR (40% [237/591]) compared to CCPR (27% [862/3,165]). They reported that patient selection, effective implementation of ECPR, adequate prearrest, and arrest resuscitation were ongoing determinants of survival. The identification of modifiable factors in this chain is an essential component to improving outcomes of this highly invasive therapy.
Fluid overload and acute kidney injury (AKI) are frequent complications of ECMO. A survey conducted among 65 international ECMO centers reported that the predominant indication for RRT on ECMO was treatment (43%) or prevention (16%) of fluid overload, AKI (35%), and electrolyte imbalance (4%). 29 A retrospective cohort study of the ELSO registry demonstrated that among 9,903 infants and children who did and did not require RRT, both neonatal and pediatric nonsurvivors experienced more AKI (19% vs 3.9%, P < .0001 and 32.3% vs 12%, P < .0001) and RRT requirement (39.7% vs 16%, P < .0001 and 8.9% vs 30.8%, P < .0001) than survivors, respectively. After adjusting for known predictors of mortality, both AKI and RRT independently predicted mortality in neonates and children on ECMO. While these findings are supported by multiple single institution studies, 30 -33 RRT has been shown to allow for better fluid management and possible reduction of capillary leakage syndrome, ultimately resulting in reduced time on ECMO, improved mechanical ventilation 34 and better fluid balance over non-survivors of RRT. 35
It is important to note that while RRT was negatively associated with survival, it is likely the AKI (for which RRT may be a surrogate marker) and not the RRT itself that contributed to increased risk of death. Prearrest Cr was not statistically different between survivors and nonsurvivors, indicating that the renal injury was either acquired due to a low perfusion state during the arrest or as a complication of ECMO. This finding was also observed by a study conducted by Huang et al, whereby nonsurvivors of ECPR had a higher serum lactate (13.4 ± 6.4 vs 8.8 ± 5.1 mmol/L) prior to ECPR and more renal failure after ECPR (66% vs 20%, P < .01). 36 These patients, similar to our cohort, did not have intrinsic kidney disease before CPR. The authors similarly concluded that the acute renal failure resulted from a hypoperfused state that preceded the arrest and during CPR. Avoidance of secondary organ damage for these patients is essential to improve survival rates.
After the initial ischemic insult to the kidneys during CPR, the duration of ECMO could contribute to secondary injury in the form of emboli, hypermyoglobinemia, toxic byproducts of hemolysis, and systemic inflammation from exposure to a non-self-membrane blood/air interface. 37 In support of this, multivariable logistic regression analysis shows that for every additional 12 hours on ECMO, there was an 11% increase in the odds of receiving RRT, when adjusting for the other three variables in the model (Cr, pH, weight). A third hit to the organ in this situation would be a delay in the initiation of RRT in patients who require it. Han et al conducted a meta-analysis of the current literature and found that the risk ratio of mortality for RRT tended to be greater the longer the initiation of RRT was delayed. 38 A single-center, randomized, clinical trial in critically ill patients with AKI (not on ECMO) showed that early initiation (defined as within eight hours of diagnosis of stage 2 AKI) of continuous veno-venous hemofiltration (CVVH) compared to delayed initiation (within 12 hours of stage 3 AKI or no initiation) was associated with a statistically significant reduction in 90-day mortality (39.3% vs 54.7%, P < .03). 39 Possible areas for improvement based on these findings include minimization of secondary organ injury from ECMO through early initiation of CVVH in patients for whom risk of AKI is high.
There is a paucity of literature reporting long-term outcomes of children after ECPR. Known neurologic morbidities associated with ECMO include hemorrhage, infarction, seizures, brain death, and disrupted cerebral circulation. 40,41 Determining the incidence of these morbidities is an essential first step in addressing these complications. Our cohort demonstrated a 51% incidence of neurologic complications consistent with stroke. The Pediatric Cerebral Performance Score (PCPC) and the Pediatric Overall Performance Score (POPC) are validated models used to evaluate gross neurological outcomes among survivors after ECMO. Prodhan et al utilized these models to ascertain neurological status of patients after ECPR. The authors noted that 18 (75%) of 24 patients had no change in PCPC and POPC scores from a baseline at discharge to outpatient follow-up at a median of 31.5 months. 42 Lasa et al compared survival with favorable neurologic outcomes between children receiving ECPR versus CCPR, also using the PCPC score. The authors observed that the OR for survival with favorable neurologic outcome with ECPR (OR: 2.64, 95% CI: 1.91-3.64, P < .001) was higher than that for patients who received CCPR. 10 More recently, good neurobehavioral outcomes based on the second edition of Vineland Adaptive Behavior Scale have been demonstrated after ECPR at one-year follow-up in a multicenter trial in 37 PICUs in the United States, Canada, and the United Kingdom. 6 While long-term outcome of ECPR survivors (especially those with EEG changes, seizures, or neurologic findings of stroke) remains an understudied area, the neurologic outcomes reported by these series are encouraging.
Conclusions
As the utilization of ECPR increases, a methodical approach to its implementation and monitoring of outcomes becomes essential. Reviewing the institutional experience of high-volume pediatric ECMO centers takes an initial step toward process improvement and more favorable outcomes. While our data add to the growing literature supporting the use of pediatric ECPR, larger, multicenter studies are required to meaningfully describe neurologic outcome and functional status of this patient population; survival is an essential but insufficient measure.
Supplemental Material
Supplementary_Tables - Extracorporeal Cardiopulmonary Resuscitation (ECPR) in Infants and Children: A Single-Center Retrospective Study
Supplementary_Tables for Extracorporeal Cardiopulmonary Resuscitation (ECPR) in Infants and Children: A Single-Center Retrospective Study by Aqsa Shakoor, Felipe E. Pedroso, Shimon E. Jacobs, Shunpei Okochi, Ariela Zenilman, Eva W. Cheung and William Middlesworth in World Journal for Pediatric and Congenital Heart Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations and Acronyms
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.