
Abstract
Virtual reality (VR)-based mirror exposure therapies (VR-MET) are widely used for the treatment of anorexia nervosa (AN). However, their effectiveness may depend on how much patients perceive a virtual body as their own, a phenomenon known as the full-body illusion (FBI). This study examined FBI levels and their clinical correlates in adolescents with AN, a key developmental period in the disorder. Forty-nine female adolescents with AN were immersed in a VR environment and embodied in avatars reflecting their own body shape and weight through visuomotor and visuo-tactile stimulation. The FBI was assessed using both unidimensional measures and a multidimensional embodiment questionnaire. Correlation analyses and multiple linear regressions were conducted to explore associations between FBI components and AN-related variables, including body mass index, body dissatisfaction, body anxiety, state anxiety, and fear of gaining weight (FGW). Results showed significant negative correlations between body anxiety and FGW and FBI, particularly its unidimensional and ownership components, with FGW explaining 28.1 percent of FBI variance. Consistent with the Allocentric Lock hypothesis, these findings suggest that adolescents with AN may rely more strongly on stored, distorted body representations than on immediate multisensory evidence (sight, touch, and proprioception), creating a cognitive barrier to virtual ownership and potentially limiting VR-MET effectiveness during adolescence. Future research should incorporate more diverse samples—including different ages and genders—to further clarify the clinical role of embodiment processes in VR-based interventions.
Introduction
In recent decades, virtual reality (VR)-based interventions have become an integral part of “Embodied Medicine,” an emerging interdisciplinary field focused on leveraging cutting-edge technologies to enhance overall health and well-being. 1 –4 VR has demonstrated its potential to influence perceptual, motor, and executive functions, as well as social cognition. 5 –7 Notably, VR-based Mirror Exposure Therapy (VR-MET) has been proposed as a valuable tool to specifically improve the treatment of anorexia nervosa (AN), 8,9 a severe eating disorder (ED) characterized by extreme underweight, body image disturbances, and an intense fear of gaining weight (FGW). 10 According to the Williamson et al.’s (2004) 11 model of EDs, these symptoms are maintained by a negative body schema that manifests through specific clinical markers: body dissatisfaction (perceptual-evaluative), body anxiety (affective), and FGW (behavioral-cognitive). Since VR-MET aims to disrupt this schema, evaluating these variables is essential to understanding how internal body representations are modified and updated during therapy.
VR-MET provides a controlled and immersive environment with high ecological validity and personal relevance for AN patients (e.g., locker rooms, shop fitting rooms), 9,12 –16 and enables increased control over exposure parameters, such as the controlled and graded manipulation of the virtual body reflected in the mirror. For instance, Porras-García et al. (2021) 17 developed a VR-MET procedure that gradually increased the virtual avatar’s weight and shape across sessions, allowing participants to confront their bodies, reaching a healthy body mass index (BMI). Their results demonstrated that this VR-based hierarchical exposure effectively reduced FGW and body anxiety in AN patients.
Concurrently, research has attempted to elucidate the underlying mechanisms that explain the effectiveness of VR-MET for ED treatment. Building on the foundational example of the rubber hand illusion (RHI), 18 various authors showed that the synchronous tactile stimulation (i.e., seeing the rubber hand being touched while simultaneously feeling the touch on one’s own hidden hand), used to elicit the illusory experience of owning (“embodying”) the rubber hand, could also be applied to the entire body to effectively elicit an FBI in a VR environment. 19 –23 Moreover, the capacity that the patients perceive and accept their virtual body as their own could also be enhanced by more complete sensory-motor experiences involving interoceptive, proprioceptive, and sensory information. 1,3,5 –7 Consequently, new embodiment techniques (“body swapping”) have been proposed to enhance the FBI, such as visuo-motor stimulation (i.e., avatar moves synchronously with the participant’s real movements) or the combination of various viewing perspectives within the VR environment: ‘first-person’ (i.e., directly observing one’s avatar, primarily influenced by current sensory inputs) and ‘third-person’ (i.e., observing one’s avatar in a virtual mirror, more influenced by cognitive, affective inputs, or stored false memories, e.g., belief of being overweight or thin-ideal internalization). 24,25 Notably, from a neuropsychological perspective, the FBI can be explained by the ability to modify (i.e., structure, augment, or replace) the egocentric and allocentric internal body representations through the induction of multisensory conflicts (e.g., through visuomotor or visuo-tactile stimulation procedures) within the bodily self-consciousness, understood as a coherent supramodal body representation. 1,6,26 –28
Numerous studies have demonstrated that a greater level of FBI, elicited through embodiment stimulation techniques, can enhance VR-MET effectiveness in reducing body dissatisfaction and distortion in patients with AN, thereby improving AN treatment outcomes. 8,15,29 –31 However, Porras-Garcia et al. (2020) 32 reported that female patients with AN experienced weaker FBI (assessed via a single ad-hoc question) compared to healthy young women with varying levels of body dissatisfaction. This occurred despite all participants being immersed in the same VR setting and following identical embodiment stimulation procedures. Such a weaker FBI could then potentially limit VR-MET effectiveness in patients with AN.
Nevertheless, as highlighted in recent reviews, 14,33 interpreting FBI findings in current VR embodiment research remains limited. These limitations largely stem from an unclear FBI construct definition and a lack of standardization across measurement instruments. Specifically, Mottelson et al. (2023) 33 noted that various ad-hoc questionnaires, often lacking adequate psychometric validation, have been used to assess FBI across studies, thus hindering direct comparison and interpretation of findings. Peck and Gonzalez-Franco (2021) 34 employed exploratory factor analysis to develop the Avatar Embodiment Questionnaire (AEQ). This instrument was designed to standardize the assessment of the FBI, directly addressing existing methodological limitations. The factor analysis also provided a clearer definition of the FBI construct by identifying four components: appearance (how much participants perceived the avatar resembled their appearance), ownership (how much they felt ownership over the avatar), response (how well the avatar’s movements matched their own), and multi-sensory (the realism of sensory experiences). A fifth component, agency (participant sense of control over the avatar), was additionally included for backward compatibility with previous studies. Following the development of this questionnaire, the authors explicitly recommended the use of the AEQ whenever participants are provided with a self-avatar. In their view, this recommendation is essential given prior research highlighting significant inter-individual differences even among participants exposed to identical experimental conditions. 34,35 This recommendation is especially relevant, as recent neurobiological models suggest that individuals with AN may prioritize distorted, stored body representations over immediate multisensory inputs (e.g., vision, touch, proprioception), thereby differentially shaping multidimensional FBI components. 27,36,37
To explore potential constraints on VR-MET effectiveness in AN treatment, this study aimed to provide data on FBI levels in female adolescents with AN using both a unidimensional question and the AEQ, which Peck and Gonzalez-Franco (2021) 34 proposed as a multidimensional tool to standardize the FBI construct’s evaluation. Specifically, this study aimed to examine the associations and predictive relationships between FBI components and AN clinical markers (i.e., BMI, body dissatisfaction, body anxiety, and FGW).
Material and Method
Participants
The minimum sample size was initially determined using G*Power software version 3.1.9.7 for regression analyses. Parameters were set to a significance level of α = 0.05, statistical power of 1−β = 0.80, and a large effect size (f2 = 0.35), with a maximum of seven predictors: BMI, body dissatisfaction, body anxiety, body satisfaction, FGW, state anxiety, and age. This analysis indicated a required sample size of N = 49, corresponding to an actual power of 0.81.
The clinical sample initially comprised 54 adolescent girls with AN. Five participants dropped out, resulting in a final sample of 49. Inclusion criteria required participants to be female, aged 12–17 years, and diagnosed with AN according to DSM-5-TR criteria. 10 Exclusion criteria included serious cognitive impairment, visual or auditory deficits, epilepsy, pregnancy, cardiac irregularities, and male gender to ensure a homogeneous sample regarding gender-specific body image disturbances 38 –41 potentially influencing the FBI. Among the initial sample, 53 participants were diagnosed with restrictive-type AN and one with purgative-type AN.
Regarding treatment, 36 patients were enrolled in an inpatient day program (ED-11h), consisting of 11 hours of daily care with overnight stays at home, while 18 participants followed a Home Treatment (HoT) program bridging inpatient and outpatient care. 42 At the time of assessment, the mean duration since disorder onset was 13 months, and the mean duration since initiation of ED-11h treatment was 6 months.
Instruments
The study used hardware and software similar to prior research 17,32,43,44 to create virtual bodies and design the VR environment. Participants wore an HTC VIVE Pro EyeTM Head-Mounted Display (HMD), with five trackers attached to the headset, hand controllers, and feet to enable full-body tracking. This setup allowed their movements to be reproduced in real time on their virtual avatars. The virtual environment was a simple room containing a mirror placed 1.5 meters in front of the participant and two boxes, with no additional furniture (Figure 1a). Generic female avatars dressed in standard clothing (t-shirt, pants, and shoes) were customized to match each participant’s body shape. Participants could view their avatars from both third-person and first-person perspectives—either observing themselves in the mirror or looking down at and moving their virtual bodies (Figure 1b–c). Previous research indicates that combining these perspectives strengthens body ownership, amplifies physiological responses, and facilitates updates to central body representations. 45 Detailed technical specifications for hardware and software are provided in the Supplementary Data.
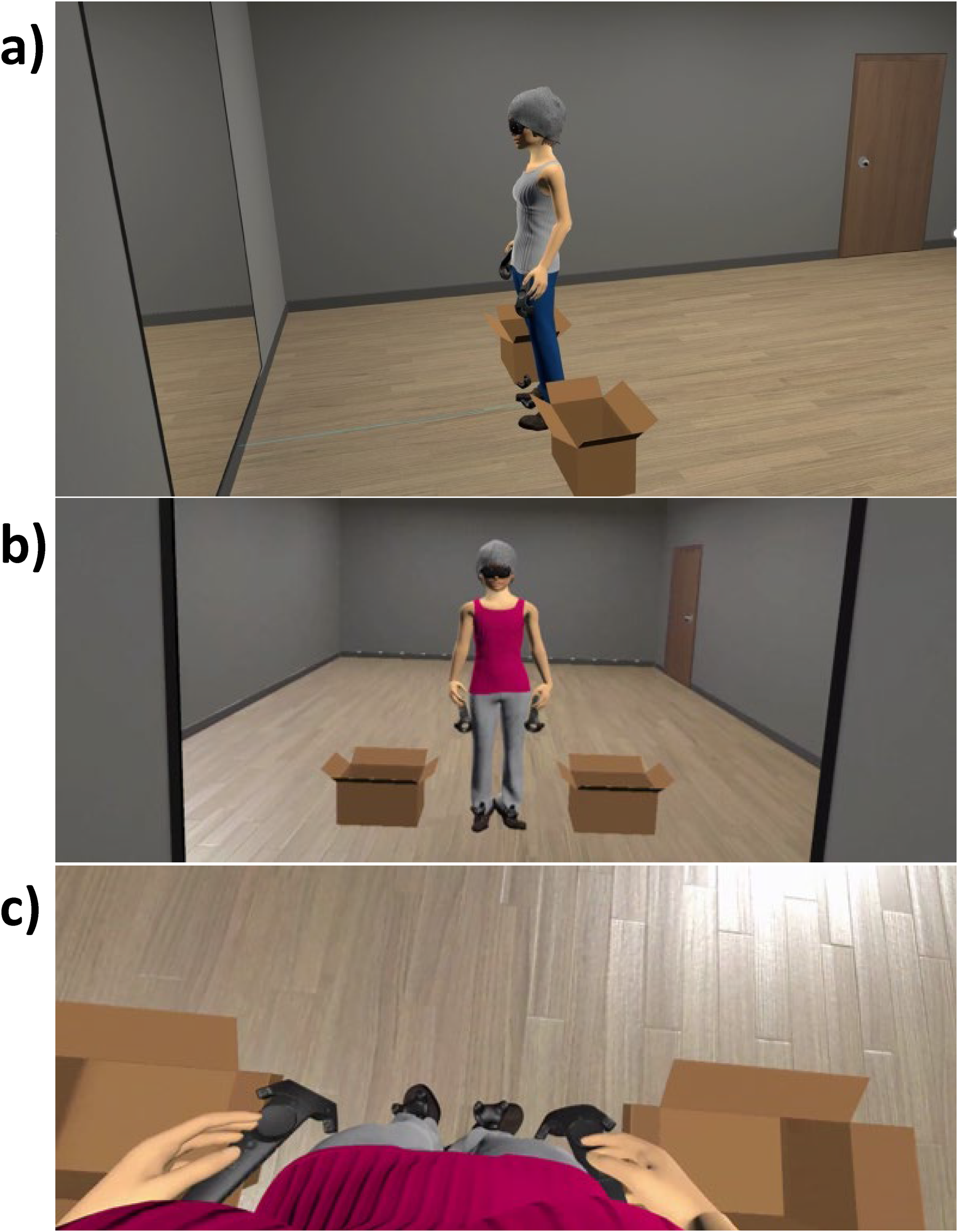
VR setting and virtual body. The handheld controllers and trackers were rendered visible within the virtual environment, to ensure multimodal coherence between the participant’s tactile sensations and visual input.
Measures
BMI was calculated after measuring participants’ weight and height on-site: BMI = weight (kg)/height (m2). 2
State body anxiety was measured using the Physical Appearance State and Trait Anxiety Scale (PASTAS), 46 a self-reported questionnaire based on a five-point Likert scale that assesses tension, negative thoughts, and physiological responses. Only the 8 items from the weight-related scale were used, targeting body areas such as the stomach, hips, waist, thighs, and legs, which reported good internal consistency (Cronbach’s alpha = 0.81).
Body dissatisfaction as a trait was measured using the Spanish version 47 of the EDI-3 inventory, 48 a self-reported 91-item questionnaire based on a six-point Likert scale, which has shown good reliability (Cronbach’s alpha ranging from 0.74 to 0.96). 47,49 Only the total score of the 10-item Body Dissatisfaction Subscale (EDI-BD) was used to provide a global measure of body dissatisfaction with the whole body.
Visual Analog Scales (VAS) for state measures: participants rated their current experience regarding the following items:
Body Satisfaction (VAS_BS): “Indicate how satisfied you are with the appearance of your body right now.” Anxiety (VAS_Anxiety): “Indicate the level of anxiety you are experiencing right now.” Fear of Gaining Weight (VAS_FGW): “Indicate how much you are afraid of gaining weight right now.” Embodiment (VAS_Embodiment, i.e., unidimensional FBI): “Indicate how much you feel that the virtual body is your own body.”
All items were rated on a scale from 0 to 100, where 0 represented “not at all” and 100 represented “completely.”
The multidimensional FBI was measured using the AEQ, 34 a 16-item 7-point Likert self-reported scale. The AEQ provides a general index of FBI along with five subscales: how much participants perceived the avatar resembled their appearance (FBI_Appearance), how much they felt ownership over the avatar (FBI_Ownership), how well the avatar’s movements matched their own (FBI_Response), the realism of sensory experiences (FBI_Multisensory), and their sense of control over the avatar (FBI_Agency). The AEQ subscales demonstrated acceptable internal consistency, with Cronbach’s alpha values—calculated specifically for this study’s adolescent female sample—ranging from 0.71 (FBI_Multisensory and FBI_Agency) to 0.78 (FBI_Ownership).
Procedure
The procedure comprised the following steps:
Preparation and consent: The procedure was explained, questions were addressed, and parental and participant informed consent was obtained, including the right to withdraw anytime. Body image assessment and avatar creation: Body image was evaluated using questionnaires on body anxiety (PASTAS) and body dissatisfaction (EDI-BD), Virtual avatars were created based on established methods from prior studies,
17,32,43,44
through photographic procedure detailed in the Supplementary Data. FBI induction: To elicit the FBI, two 5-minute stimulation techniques were implemented based on prior studies,
17,32,43,44
detailed in the Supplementary Data.
Visuomotor stimulation: Participants performed a series of pre-determined movements, which their avatars mirrored in real-time. Visuotactile stimulation: A VR controller was used to gently touch specific areas of the participants’ bodies, while participants simultaneously saw a virtual controller touching the corresponding areas of their avatars’ bodies. Body satisfaction (VAS_BS), anxiety (VAS_Anxiety), fear of gaining weight (VAS_FGW), embodiment (VAS_Embodiment), and FBI (via the AEQ questionnaire) were assessed within the virtual environment. Questions were displayed on a virtual blackboard positioned next to the virtual mirror (Figure 2), allowing participants to respond without removing the HMD and disrupting FBI. This setup ensured participants could continue viewing their avatars from both first- and third-person perspectives throughout the assessment. After the HMD and body trackers were removed, any questions, concerns, or negative experiences participants might have had during the session were addressed.
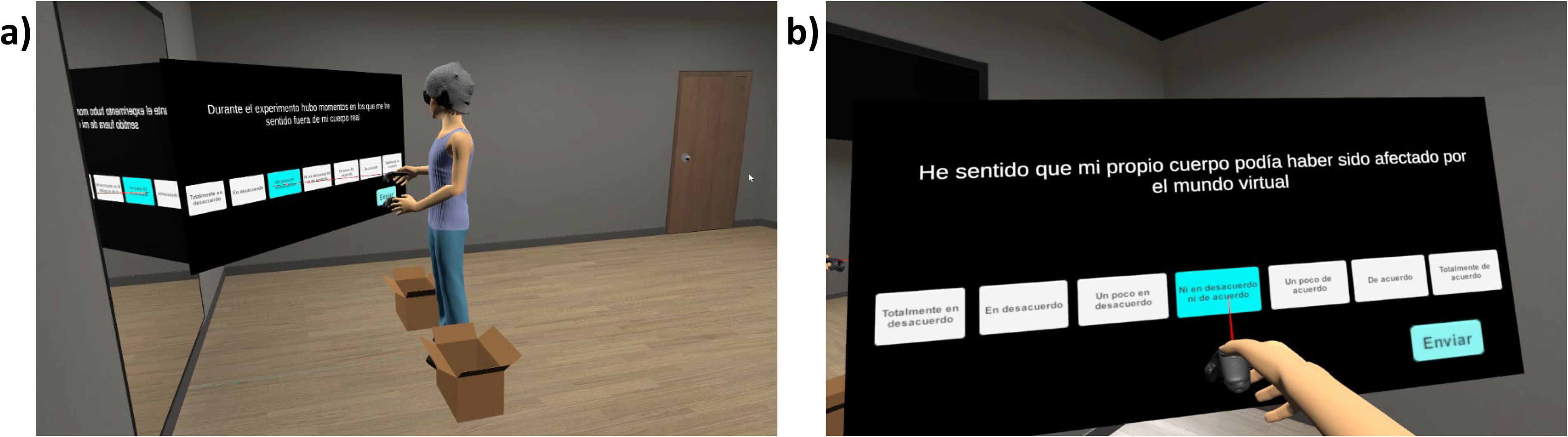
Full-body illusion assessment within the VR environment. The rating scale is presented on a fixed virtual blackboard integrated into the room environment beside the mirror.
Statistical analysis
Statistical analyses were performed using SPSS Statistics v.29 (IBM Company, Armonk, NY, USA). Outlier analysis (using a detection criterion of ± 3 standard deviations) identified one outlier related to the FBI assessment. After removing this outlier, the sample size for subsequent analyses was 48.
First, correlation analyses were carried out between participant characteristics (age, BMI, body anxiety, body dissatisfaction, VAS_BS, VAS_Anxiety, and VAS_FGW) and FBI-related variables (VAS_Embodiment, FBI General Index, and its five components). Multiple linear regression analyses were subsequently conducted with FBI indices and dimensions as dependent variables and other variables as potential predictors. To account for the sample size and limit the number of potential predictors included in the regression models, only variables that showed significant correlations with the dependent variables were included as potential predictors in the analyses. For all models, the assumptions of linear regression were met: linear relationships were confirmed through scatter plots; no multicollinearity was observed (tolerance > 0.1 and VIF < 10 for all variables); homoscedasticity of residuals was verified (nonsignificant Pearson correlation; p > 0.05 for all variables); residuals followed a normal distribution (non-significant bilateral asymptotic significance in the Kolmogorov–Smirnov test; p > 0.05 for all variables); and residuals were independent (Durbin–Watson statistics ranged from 1.5 to 2.5).
Results
Table 1 presents descriptive characteristics of the study sample.
Descriptive Statistics
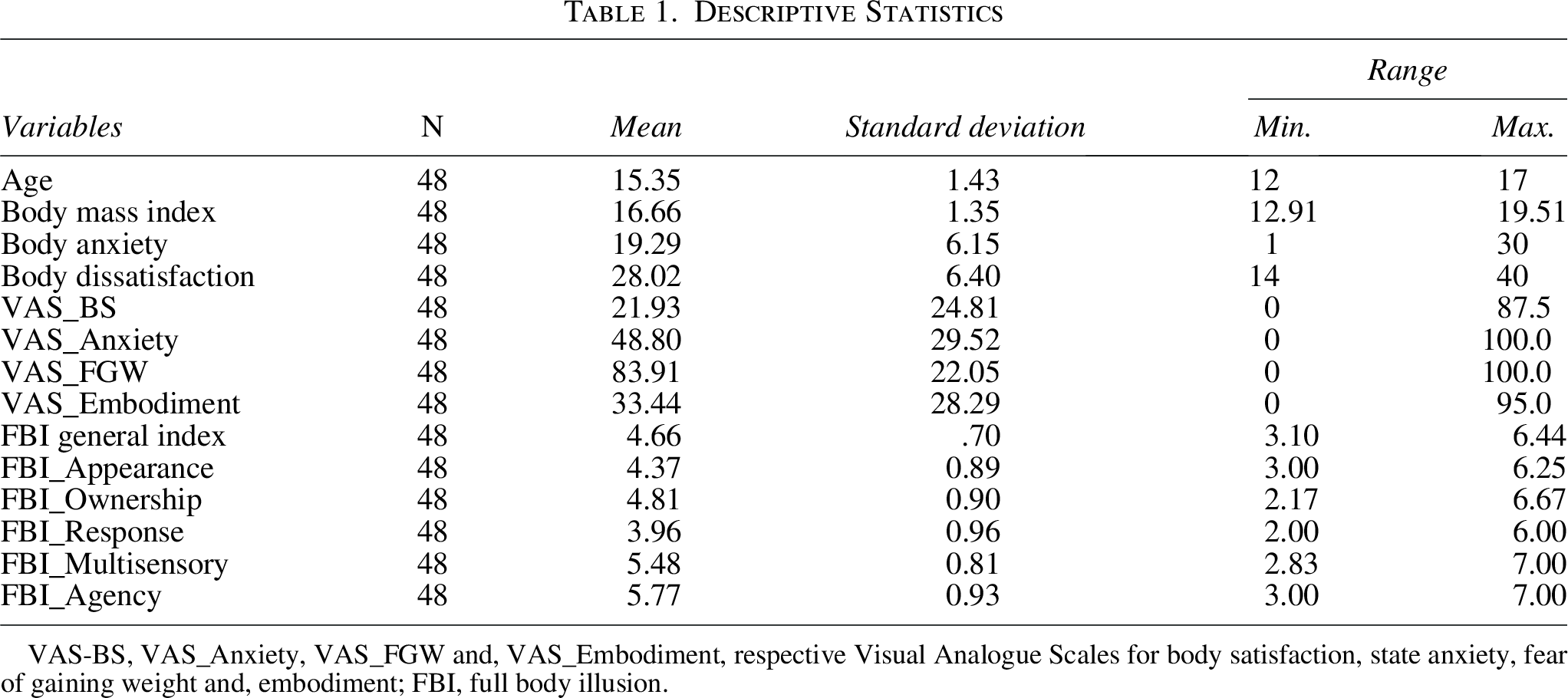
VAS-BS, VAS_Anxiety, VAS_FGW and, VAS_Embodiment, respective Visual Analogue Scales for body satisfaction, state anxiety, fear of gaining weight and, embodiment; FBI, full body illusion.
Table 2 shows the results of the correlation analysis between participant characteristics and the FBI-related variables.
Correlations Between Participant Characteristics and Full Body Illusion
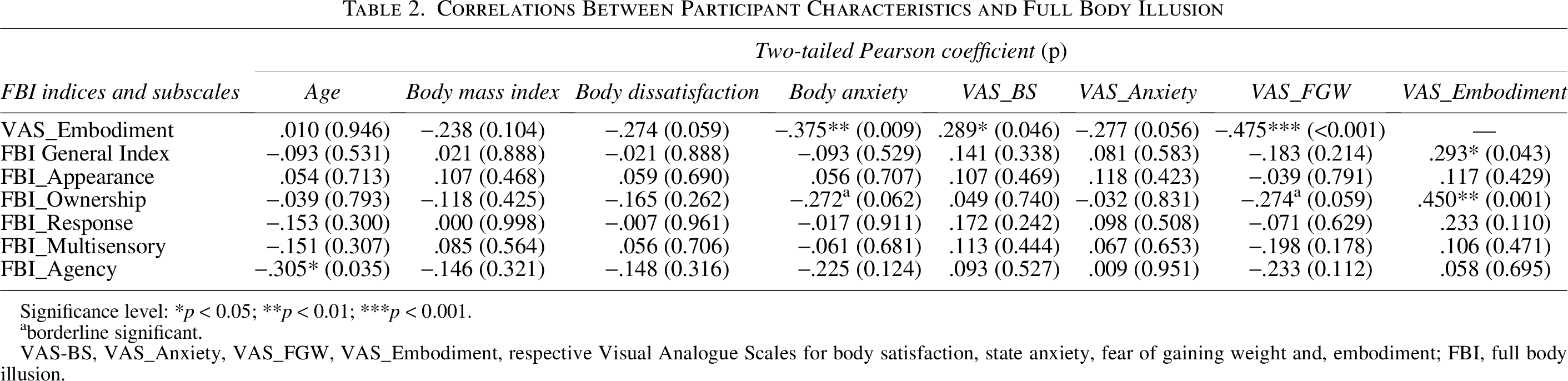
Significance level: *p < 0.05; **p < 0.01; ***p < 0.001.
borderline significant.
VAS-BS, VAS_Anxiety, VAS_FGW, VAS_Embodiment, respective Visual Analogue Scales for body satisfaction, state anxiety, fear of gaining weight and, embodiment; FBI, full body illusion.
Table 3 presents the results of the multiple linear regression analyses with FBI indices and its dimensions as dependent variables.
Multiple Linear Regression Analyses’ Results
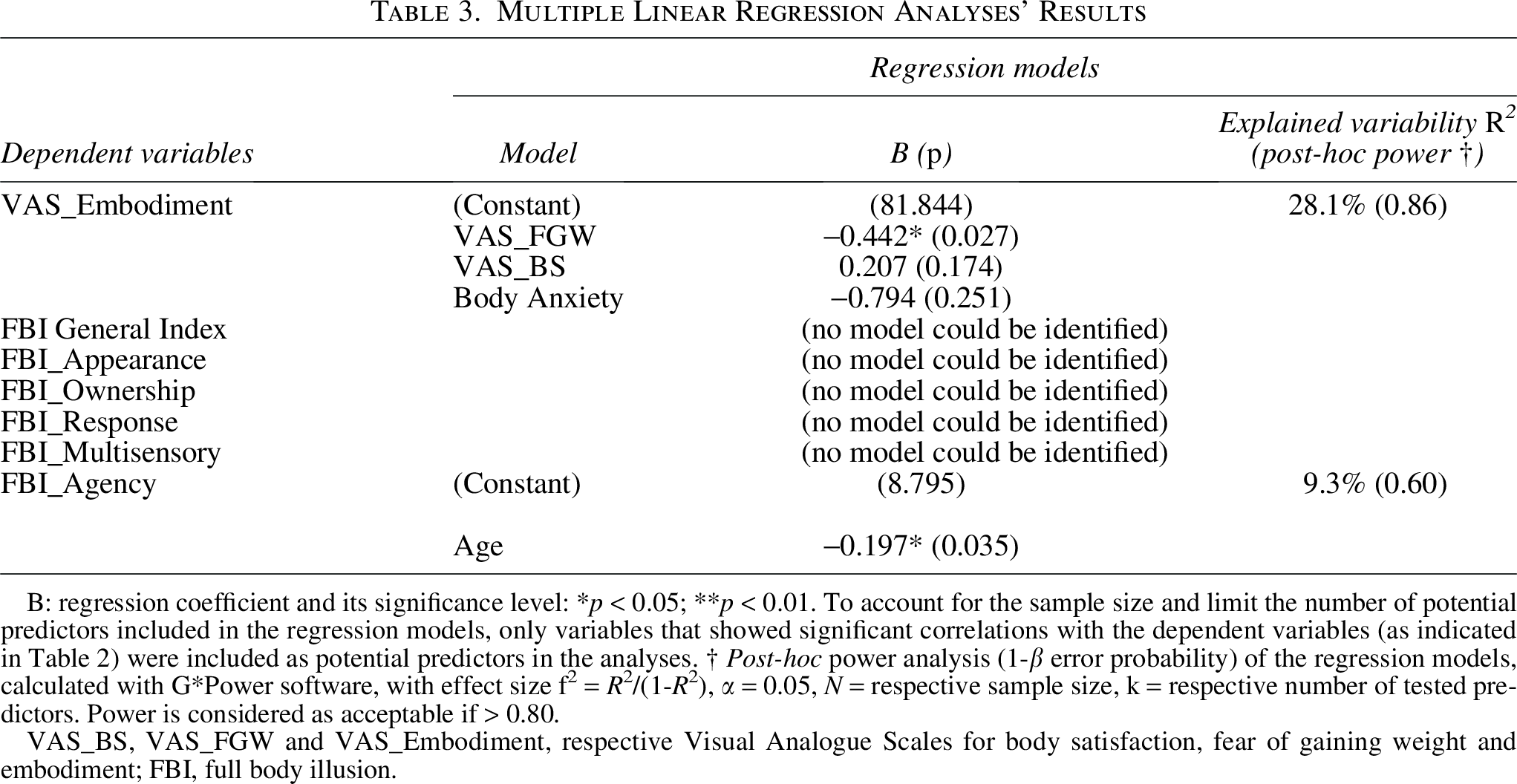
B: regression coefficient and its significance level: *p < 0.05; **p < 0.01. To account for the sample size and limit the number of potential predictors included in the regression models, only variables that showed significant correlations with the dependent variables (as indicated in Table 2) were included as potential predictors in the analyses. † Post-hoc power analysis (1-β error probability) of the regression models, calculated with G*Power software, with effect size f2 = R 2/(1-R 2), α = 0.05, N = respective sample size, k = respective number of tested predictors. Power is considered as acceptable if > 0.80.
VAS_BS, VAS_FGW and VAS_Embodiment, respective Visual Analogue Scales for body satisfaction, fear of gaining weight and embodiment; FBI, full body illusion.
Discussion
This study examined FBI experiences elicited by visuomotor and visuo-tactile stimulation in a VR setting. By incorporating both unidimensional and multidimensional assessments, the study aimed to provide a more comprehensive characterization of embodiment processes within VR-MET research. The significant correlation between VAS_Embodiment and the AEQ’s General Index (Table 2) supports the validity of using single-item VAS for rapid clinical FBI screening. In addition, the strong correlation between VAS_Embodiment and AEQ’s Ownership subscale suggests that, when female adolescents with AN provide a global rating of embodiment, they are predominantly reflecting on their sense of ownership of the virtual body. Furthermore, results revealed significant negative correlations between body anxiety, FGW, and the unidimensional FBI score (Table 2). FGW also accounted for 28.1 percent of the variance in the unidimensional FBI score (R 2 = 0.281, Table 3). A borderline significant negative association was additionally observed between FGW and the AEQ’s ownership subscale (Table 2). Although the multidimensional assessment allowed a more nuanced characterization of embodiment processes, the strongest associations observed for the unidimensional FBI with FGW and body anxiety suggest that global ownership experiences may be particularly sensitive to cognitive and affective components of body image disturbances in female adolescents with AN.
While speculative, these results potentially point toward a role of internal cognitive-affective states in preventing the update of the body schema involved in the FBI induction procedures, a key assumption of the Allocentric Lock hypothesis. 27,36,37 Within this framework, AN onset and maintenance are driven by dysfunctional multisensory integration, characterized by the dominance of distorted, memory-based body representations (allocentric frame) over real-time bodily perception (egocentric frame). These stored representations have been shown to be influenced by cognitive and affective schemas (weight-related beliefs, thin-ideal internalization, false memories, etc.), 24,25 in turn closely associated with FGW and body anxiety. 11 Accordingly, increased FGW and body anxiety in adolescent females with AN may reduce susceptibility to FBI. While this association is evident in the unidimensional FBI index, multidimensional assessments reveal that the ownership component may also be affected (Table 2). Indeed, the significant negative correlations observed may be attributed to the specific formulation of the unidimensional FBI and ownership measures (which were significantly inter-correlated; Table 2), since these scales appear to capture a global (top-down from allocentric frame) identification with the avatar rather than reflecting stimulus-driven (bottom-up) bodily perception. Conversely, other FBI dimensions (appearance, response, multisensory, and agency) may rely more heavily on egocentric bodily signals (vision, touch, and proprioception). This suggests that the Allocentric Lock acts as a cognitive barrier that prevents the temporary virtual illusion from being integrated into the patient’s stable bodily self-consciousness. Consequently, our results suggest a core limitation of current VR-MET for AN treatment: for patients with high FGW and body anxiety, usual visuomotor and visuo-tactile FBI stimulation procedures may be insufficient, requiring more intensive or ‘top-down’ clinical interventions to facilitate embodiment.
However, this study’s findings are still limited by the inclusion of only female adolescents with AN. As recommended by Birckhead et al. (2019), 50 future research on AN should account for a broader range of variables, including age, gender, ethnicity, health conditions, and social position. Regarding age, results showed a general trend of negative correlations between age and the AEQ’s FBI-related variables, reaching significance only for the agency component (Table 2) but explaining only a small proportion of variance (R 2 ≤ 10 percent, Table 3). This limited effect may be due to the narrow age range of the study adolescent sample, reflected in a low standard deviation (1.43 years, Table 1). Previous studies, however, have consistently demonstrated age-related differences in FBI. For instance, Peck and Gonzalez-Franco (2021) 34 reported lower FBI scores in participants over 30 compared to younger individuals, while Serino et al. (2018) 51 suggested that these differences may reflect more stable body representations in older adults, potentially modulating FBI. Although unidimensional FBI scores in the present study were lower than those reported in previous studies involving young adults exposed to similar FBI induction procedures e.g., 32 this difference may be related to the developmental stage of our adolescent sample, as adolescents with AN often exhibit more rigid body schemas and interoceptive deficits that may hinder the multisensory integration processes underlying the FBI. 52,53
To consolidate these findings and ensure cross-group comparability, future studies should include diverse samples of different ages, genders, and health conditions to clarify the associations between AN clinical markers and FBI’s components and ensure that personalized VR-based therapies effectively address the cognitive barriers characteristic of AN. Furthermore, to enhance future protocols, researchers may also consider personalized FBI induction durations, high-fidelity 3D body scans e.g., 54 for avatar design, and the integration of interoceptive stimulations 55 –58 —such as sonoception e.g., 59 —to modulate the synthetic multisensory experience.
In conclusion, this study identified FGW and body anxiety as clinical correlates of reduced virtual embodiment in female adolescents with AN. These findings suggest that cognitive-affective aspects of body image disturbance may influence the multisensory and representational processes involved in the FBI, potentially limiting the effectiveness of standard VR-MET embodiment procedures in some patients. Recognizing these clinical correlates may help optimize the development of more personalized VR interventions.
Authors’ Contributions
F.-A.M.-A.: Conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, and visualization; M.A.: Conceptualization, methodology, software, validation, formal analysis, investigation, and writing—review and editing; M.-T.M.-M.: Conceptualization, methodology, validation, formal analysis, investigation, and writing—review and editing; E.S.-T.: Resources, writing—review and editing, and supervision; M.C.-R.: Investigation, resources, and writing—review and editing; M.F.-G.: Conceptualization, methodology, resources, writing—review and editing, and supervision; J.G.-M.: Conceptualization, methodology, validation, formal analysis, investigation, resources, writing—review and editing, supervision, project administration, and funding acquisition. All authors have read and agreed to the published version of the article.
Footnotes
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Hospital Sant Joan de Déu in Barcelona (approval code: PS-21-20, date: 25-March-2021).
Informed Consent Statement
Informed consent was obtained from all subjects and parents involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Author Disclosure Statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results. None of the authors have a financial arrangement or affiliation with any product or services used or discussed in this article.
Funding Information
This study was funded by the Spanish Ministry of Science and Innovation (Agencia Estatal de Investigación, Ministerio de Ciencia e Innovación, Spain). Grant PID2019-108657RB-I00 funded by MCIN/AEI/ 10.13039/501100011033. This study also has the support of “Fundació La Marató de TV3”, Grant 202217-10. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.