
Abstract
Introduction:
The incidence of colorectal cancer (CRC) in adolescents and young adults is increasing, and affected individuals often face diagnostic delays, psychological distress, fertility-related concerns, and limited access to social support. Few studies have evaluated these multidimensional factors. This study aimed to clarify the clinical characteristics, psychosocial burden, fertility-related issues, and support needs of young adults with CRC.
Patients and Methods:
Patients aged 15–39 years diagnosed with CRC between 2012 and 2025 were evaluated. Clinical characteristics, psychological distress, fertility-related concerns, and utilization of social support resources were assessed using medical records, nursing documentation, multidisciplinary reports, and institutional assessment tools. Documented psychological and fertility concerns were categorized, and survival outcomes were estimated using the Kaplan–Meier method.
Results:
Symptom-driven diagnosis occurred in 59.2% overall and was significantly more common in patients in their 20 seconds (91.7% vs 52.5%, p = 0.011). Screening-based detection was lower in the 20 seconds (16.7%) than in the 30 seconds (49.2%, p = 0.039). Advanced disease (Stage II–IV) accounted for 56.3% of cases and was associated with poorer survival (p = 0.013). Psychological distress was documented in 77.5% of patients. Fertility-related anxiety occurred in 22.5% and was more frequent in women (35.5% vs 12.5%, p = 0.022). Fertility preservation was performed in 9.9%. Social worker involvement was noted in 66.2%, while use of public support systems remained low.
Conclusion:
Young adults with CRC face delayed diagnosis, substantial psychological distress, sex-specific fertility concerns, and limited engagement with public support programs. Improved symptom recognition, routine distress screening, gender-inclusive fertility counseling, and strengthened multidisciplinary support are needed for this population.
Keywords
Introduction
Young-onset colorectal cancer (YO-CRC) is increasing worldwide and has become a significant public health concern.1–3 Despite advances in cancer care, evidence regarding optimal screening strategies, clinical management, and supportive care for younger populations remains limited.4–8 Adolescents and young adults (AYA; ages 15–39) represent a unique subgroup, as cancer occurs during a life stage characterized by major transitions in education, employment, relationships, and family planning. Consequently, the impact of CRC in this age group extends beyond oncologic outcomes.5,6 AYA patients are more likely to present with advanced-stage disease and often lack access to routine screening programs, with delays in medical evaluation contributing to late diagnosis.1,2,4 In addition to clinical challenges, AYA patients frequently experience substantial psychosocial and socioeconomic burdens, including concerns related to fertility, employment, financial stability, and family responsibilities.5–7 However, few studies have comprehensively evaluated these domains specifically in AYA CRC, and the real-world utilization of fertility preservation and public support systems remains poorly characterized. 8
Given these gaps, this study aimed to assess clinical characteristics, psychological distress, fertility-related concerns, and the use of social support resources among AYA patients with CRC.
Methods
Study design and setting
This retrospective observational study was conducted at a single tertiary care center, Tokyo Medical University Hospital, and included adolescent and young adult (AYA) patients diagnosed with CRC between January 2012 and February 2025. The study protocol was approved by the Ethics Committee of Tokyo Medical University Hospital (Approval No. T2025-0014). Informed consent was obtained using an opt-out procedure in accordance with institutional and national guidelines.
Patients
Eligible patients were defined as individuals aged 15–39 years at diagnosis with pathologically confirmed colon or rectal adenocarcinoma. Patients aged ≥40 years at diagnosis or those whose primary management was performed at another institution were excluded. All eligible patients had sufficient data for the variables analyzed, and no patients were excluded due to missing data. Data were retrospectively extracted from medical records, including standardized intake forms routinely used to assess psychosocial concerns. No patients aged 15–19 years were identified; therefore, all included cases were young adults aged 20–39 years.
Data collection
Data abstraction was performed manually by trained physicians using a standardized data collection form. Clinical, psychosocial, and treatment-related data were retrospectively extracted from electronic medical records, nursing documentation, multidisciplinary support conference records, and standardized institutional support screening and assessment tools. Clinical variables included age, sex, time from symptom onset to diagnosis, presenting symptoms, disease stage based on the 8th edition of the UICC TNM classification, histological subtype, serum tumor marker levels, treatment modalities, follow-up duration, and survival status. Psychological distress was assessed based on documentation in physician and nursing notes, psychiatry consultations, multidisciplinary records, and institutional screening tools and categorized into predefined domains including future-related anxiety, economic concerns, treatment-related anxiety, family burden, and employment or educational difficulties. In addition to routine clinical documentation, standardized institutional screening tools used at admission and discharge—such as structured intake and discharge support assessment forms—were systematically reviewed to capture psychosocial concerns. These tools evaluated domains including anxiety, social concerns, and support needs as part of routine clinical care. Patients were classified as having no psychological concerns only when no concerns were identified across all available data sources, including these structured assessments.
Fertility-related data included documentation of fertility-related anxiety, fertility counseling, and fertility preservation practices when applicable. Social support needs were evaluated based on medical social worker involvement, discharge planning, utilization of public support systems, and documentation of work-related or financial difficulties.
Outcomes
The primary outcomes were the prevalence and types of psychological distress, fertility-related concerns and interventions, and utilization of social support resources. Secondary outcomes included clinical characteristics at diagnosis and overall survival.
Exploratory analyses
Exploratory age-stratified analyses were performed by dividing patients into younger (20–29 years) and older (30–39 years) AYA groups, consistent with prior AYA oncology studies.
Statistical analysis
Continuous variables were reported as medians with interquartile ranges (IQRs) and compared using the Mann–Whitney U test. Categorical variables were analyzed using the χ2 test or Fisher’s exact test as appropriate. Age-associated patterns were explored using supplementary comparisons between patients in their twenties and thirties. Overall survival was estimated using the Kaplan–Meier method, and differences between groups were compared using the log-rank test. All analyses were conducted using SPSS Statistics version 31, with a two-sided p value < 0.05 considered statistically significant.
Ethical considerations
This study was approved by the Ethics Committee of Tokyo Medical University Hospital (Approval No. T2025-0014). In accordance with institutional policy for retrospective studies, informed consent was obtained via an opt-out procedure.
Results
Patient characteristics
Baseline demographic and clinical characteristics are summarized in Table 1. A total of 71 AYA patients with CRC were included. The median age at diagnosis was 35 years (IQR 31–37); 12 patients (16.9%) were in their twenties and 59 (83.1%) were in their thirties. There were 40 men (56.3%) and 31 women (43.7%), and the median BMI was 21.3 (IQR 19.8–24.8). A total of 47 patients (66.2%) were unmarried, and 17 (23.9%) had children. Employment was documented in 56 patients (78.9%). Six patients (8.5%) had a history of non-CRC malignancy. Family history of CRC was present in five patients (7.0%) among first-degree relatives and six patients (8.5%) among second-degree relatives. Four patients (5.6%) had inflammatory bowel disease-associated CRC, and one (1.4%) had hereditary CRC; the remaining 66 patients (93.0%) had sporadic disease. Presenting symptoms included hematochezia (29 patients, 40.8%), positive fecal immunochemical test (FIT) (21 patients, 29.6%), abdominal pain (4 patients, 5.6%), constipation (3 patients, 4.2%), and anemia (6 patients, 8.5%). Symptomatic presentation was documented in 42 patients (59.2%). A prior colonoscopy was recorded in 61 patients (85.9%). Tumor location was the right colon in 17 patients (23.9%), left colon in 20 (28.2%), and rectum in 30 (42.3%). T classification ranged from Tis (29.6%) to T4 (16.9%). N classification ranged from N0 (52.1%) to N3 (8.5%). Metastatic disease (M1) was present in 13 patients (18.3%). Disease stages were Stage 0 (29.6%), I (14.1%), II (8.5%), III (29.6%), and IV (18.3%). Initial treatment included endoscopic resection in 22 patients (31.0%), curative-intent surgery in 35 (49.3%), chemotherapy plus palliative surgery in 5 (7.0%), chemotherapy alone in 6 (8.5%), and additional surgery after endoscopic resection in 3 (4.2%). Chemotherapy was administered to 38 patients (53.5%), and stoma creation was performed in 12 (16.9%). CEA was elevated in 17 of 53 patients (32.1%), and CA19-9 in 47 of 53 (88.7%). The median follow-up was 51 months (IQR 27–72), with 65 patients (91.5%) alive and 6 (8.5%) deceased at last follow-up.
Baseline Characteristics of the Patients
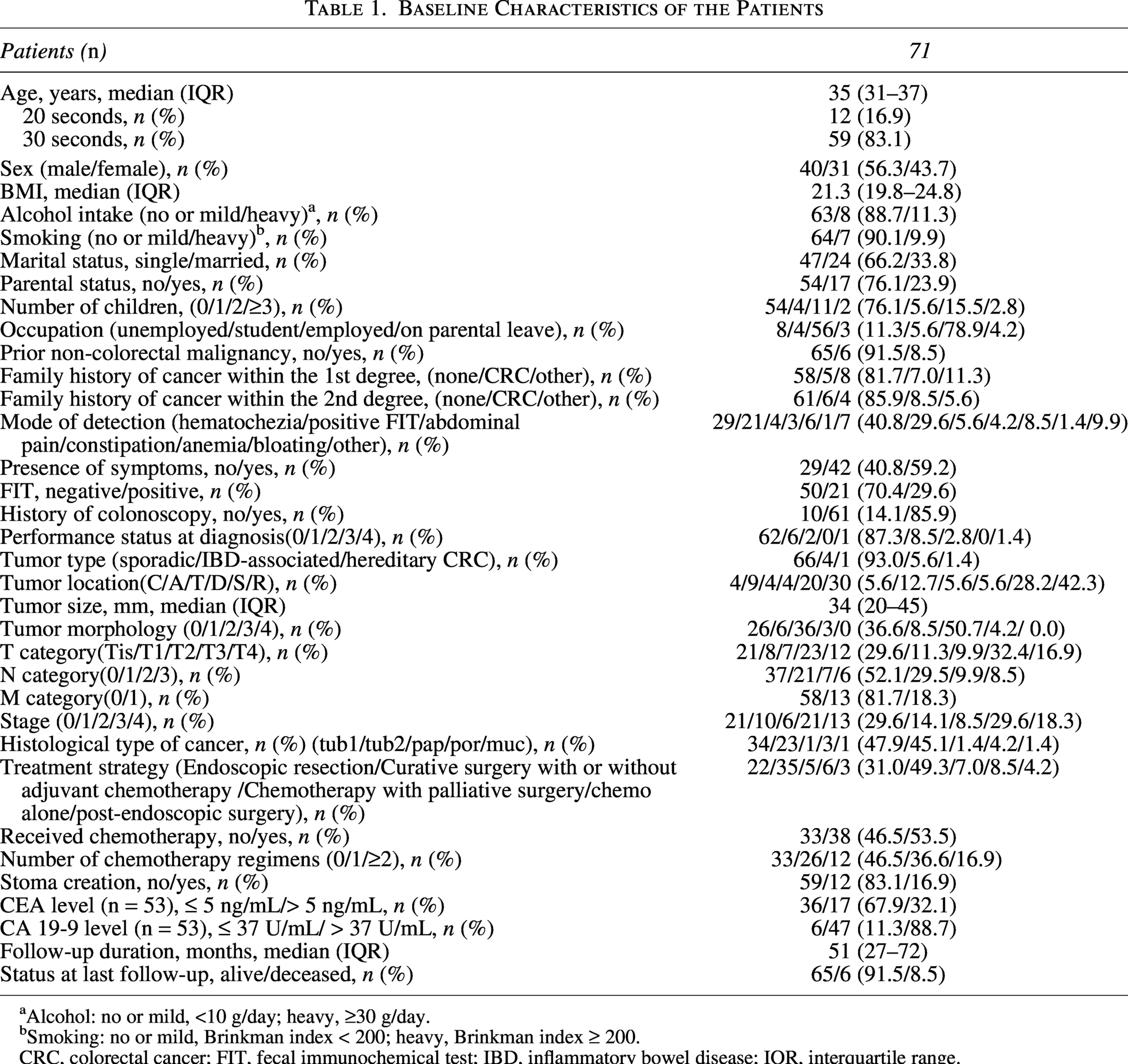
Alcohol: no or mild, <10 g/day; heavy, ≥30 g/day.
Smoking: no or mild, Brinkman index < 200; heavy, Brinkman index ≥ 200.
CRC, colorectal cancer; FIT, fecal immunochemical test; IBD, inflammatory bowel disease; IQR, interquartile range.
Comparison between patients in their 20 seconds and 30 seconds
Age-stratified comparisons are shown in Table 2. No statistically significant differences were observed in sex, BMI, alcohol use, smoking history, family history, history of ulcerative colitis, tumor location, or tumor markers between the age groups. In contrast, diagnostic presentation differed significantly. Symptomatic diagnosis occurred in 11/12 patients (91.7%) in their twenties, compared with 31/59 patients (52.5%) in their thirties (p = 0.011). Screening-based detection (FIT or medical checkup) was significantly lower in the twenties (16.7%) than in the thirties (49.2%, p = 0.039). Stage distribution (0–I vs II–IV), tumor morphology, T classification, and treatment patterns did not differ significantly. Chemotherapy tended to be more common in the twenties (75.0%) compared with the thirties (49.2%), although the difference was not statistically significant (p = 0.102).
Comparison of Baseline Characteristics Between AYA Patients with Colorectal Cancer in Their 20 Seconds and 30 Seconds
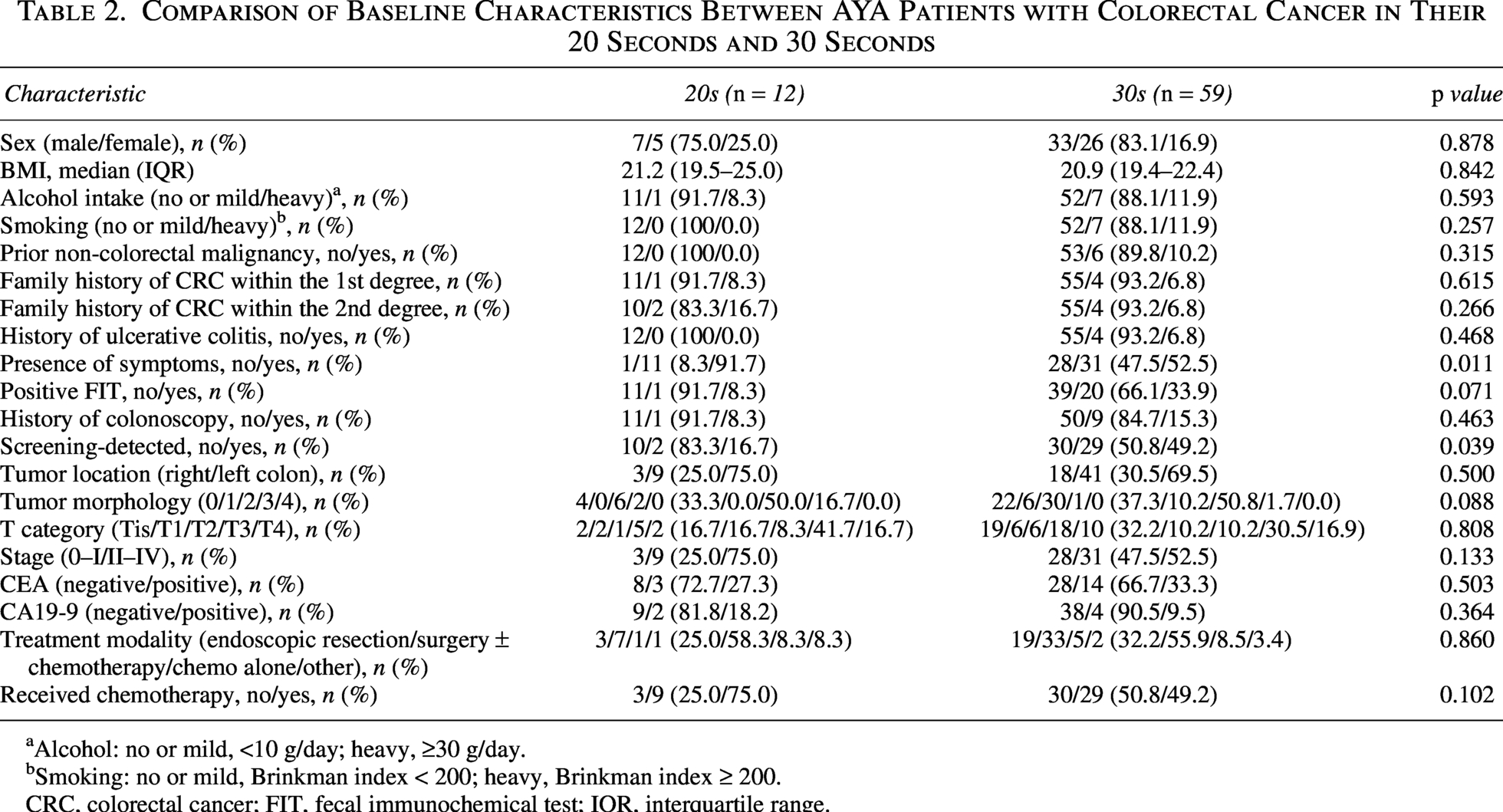
Alcohol: no or mild, <10 g/day; heavy, ≥30 g/day.
Smoking: no or mild, Brinkman index < 200; heavy, Brinkman index ≥ 200.
CRC, colorectal cancer; FIT, fecal immunochemical test; IQR, interquartile range.
Psychological distress
Psychological profiles are presented in Table 3. General anxiety was recorded in 55 patients (77.5%), future anxiety in 46 (64.8%), and treatment-related anxiety in 32 (45.1%). Economic or social concerns were present in 16 patients (22.5%) and family or life-stability concerns in 11 (15.5%). A total of 55 patients (77.5%) had at least one psychological concern, while 16 (22.5%) had no identified or documented psychological concerns. Fertility-related anxiety was present in 16 patients (22.5%).
Distribution of Anxiety Domains among AYA Colorectal Cancer Patients

AYA, adolescent and young adult.
Fertility-related concerns and counseling
Sex-specific fertility outcomes are summarized in Table 4 and depicted in Figure 1. Fertility-related anxiety was significantly more common in women (35.5%) than in men (12.5%, p = 0.022). Fertility counseling was also more frequently documented in women (32.3%) than in men (12.5%, p = 0.042). Discussion of fertility preservation occurred in 13/71 patients (18.3%), without a significant sex difference (p = 0.130). Fertility preservation procedures were performed in 7 patients (9.9%) with comparable rates in men (10.0%) and women (9.7%) (p = 0.964).
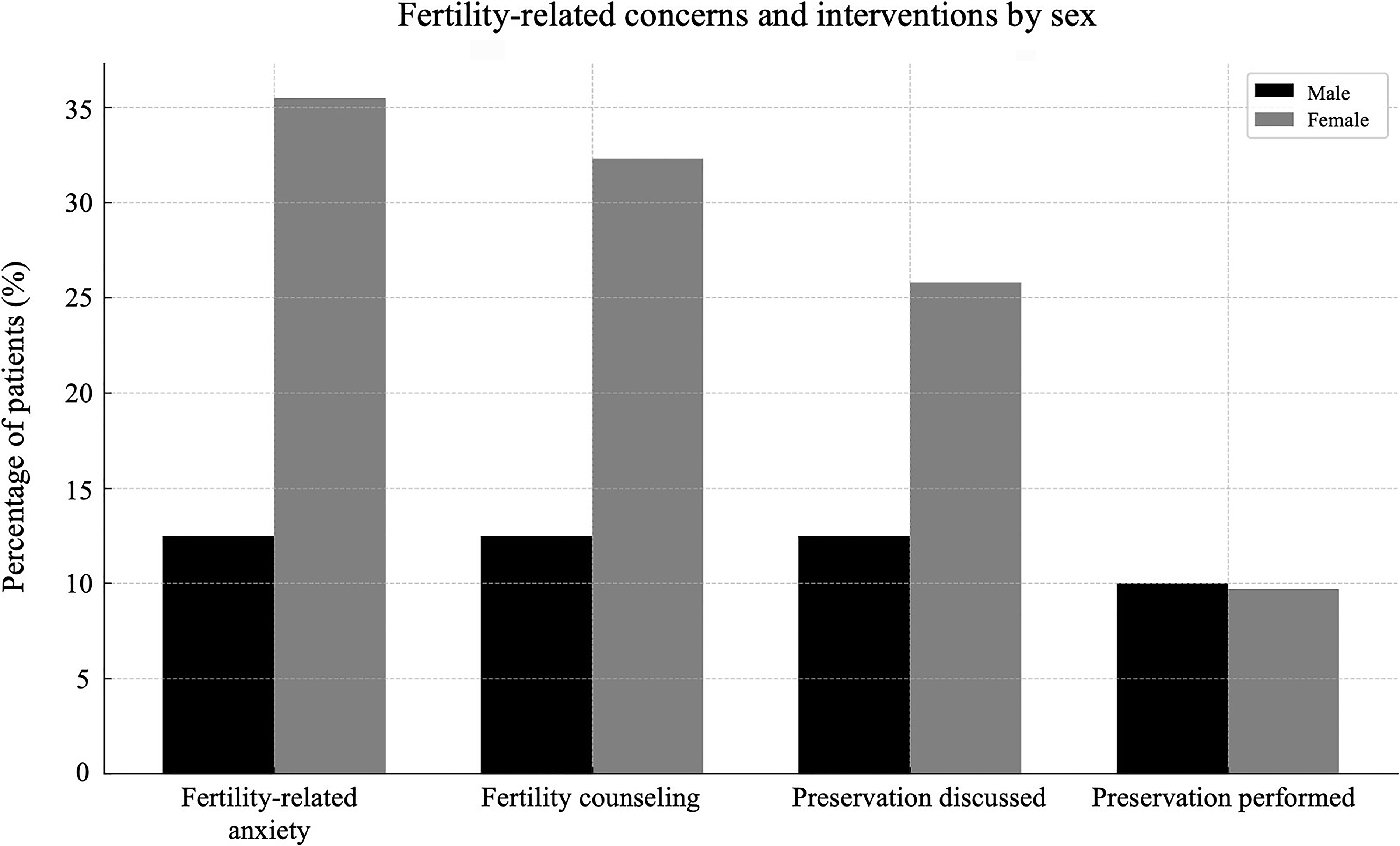
Comparison of fertility-related concerns and reproductive interventions between male and female AYA patients with colorectal cancer. The figure illustrates four domains: fertility-related anxiety, fertility counseling, fertility preservation discussed, and fertility preservation performed. Female patients showed significantly higher rates of anxiety (35.5% vs. 12.5%) and counseling (32.3% vs. 12.5%), whereas the rates of preservation discussed and performed did not differ significantly between sexes. AYA, adolescent and young adult.
Fertility-Related Concerns and Reproductive Counseling among AYA Colorectal Cancer Patients, Stratified by Sex
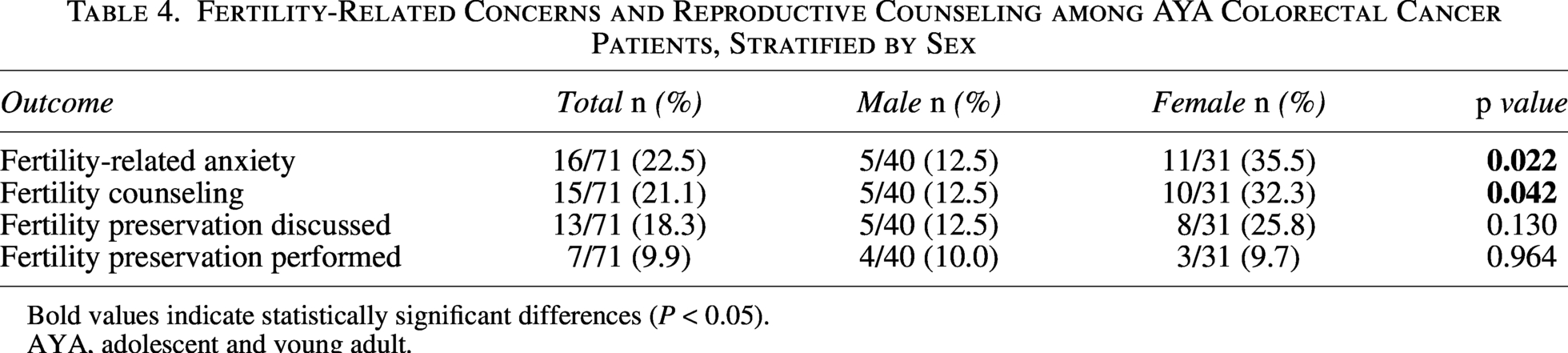
Bold values indicate statistically significant differences (P < 0.05).
AYA, adolescent and young adult.
Social, economic, and in-hospital support
Support utilization is detailed in Table 5. Hospitalization occurred in 56 patients (78.9%), medical social worker involvement in 47 (66.2%), and discharge planning support in 50 (70.4%). Sickness allowance was used by 7 patients (9.9%), whereas 38 patients (53.5%) received private insurance benefits. Use of public support systems was limited: designated intractable disease certification (5.6%), disability certification (12.7%), and welfare assistance (1.4%). Definitions of these social support systems are provided in Supplementary Table S3.
Types of Social, Economic, and in-Hospital Support Utilized by AYA Colorectal Cancer Patients
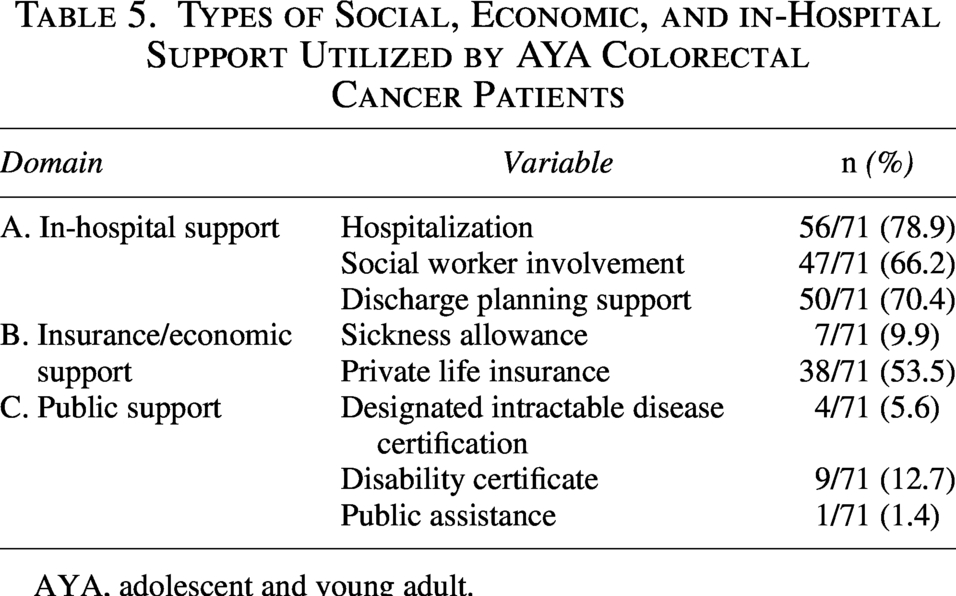
AYA, adolescent and young adult.
Survival analysis
Overall survival curves are shown in Figure 2. During the median follow-up of 51 months, 6 patients (8.5%) died. Patients with Stage II–IV disease had significantly worse overall survival than those with Stage 0–I (log-rank p = 0.013).
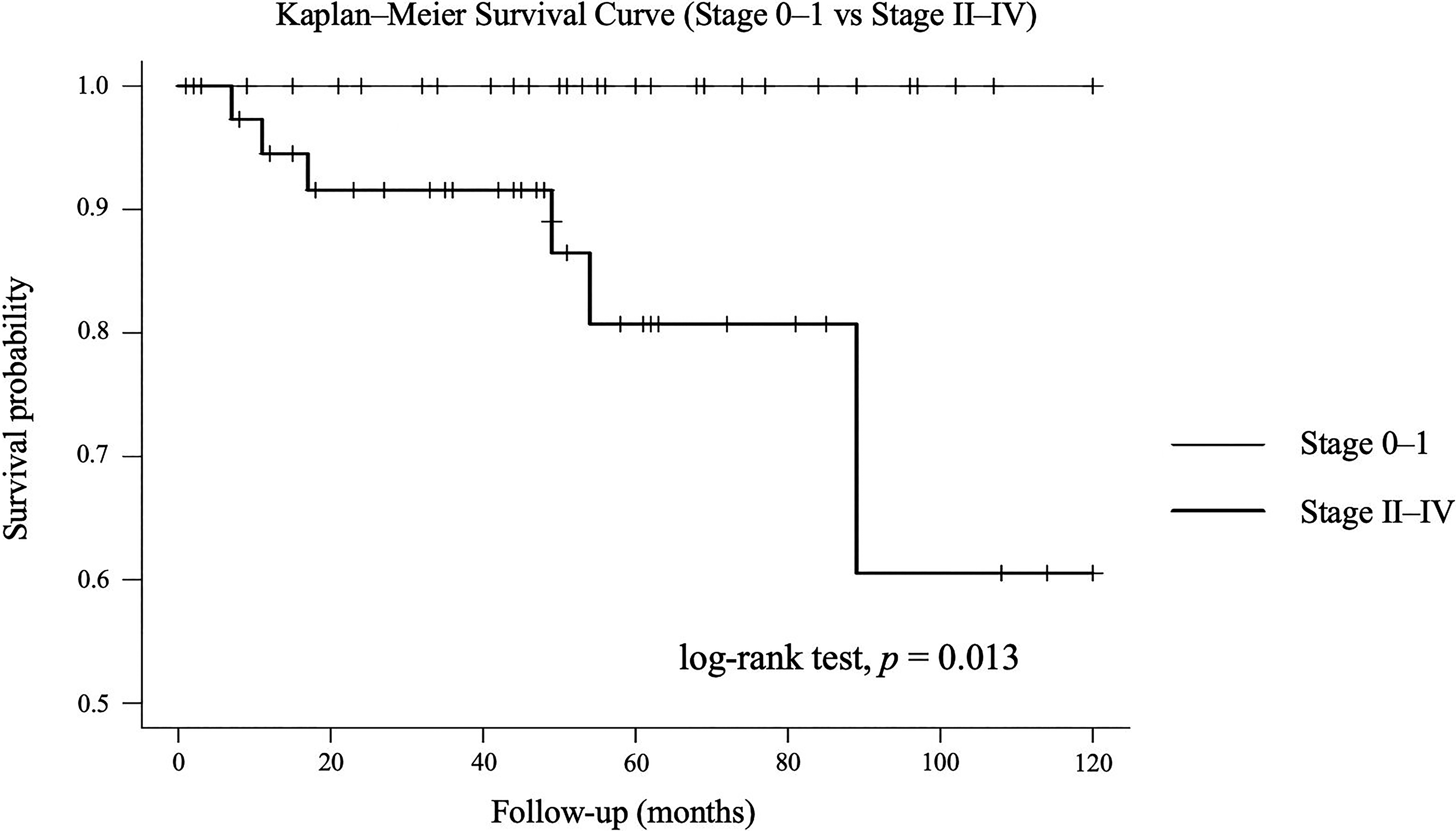
Kaplan–Meier overall survival curves for patients with Stage 0–I versus Stage II–IV colorectal cancer. Survival was significantly worse in patients with Stage II–IV disease (log-rank p = 0.013).
There were no significant differences in overall survival by age group (20 seconds vs 30 seconds) or by sex.
Supplementary analyses
Further comparisons of early- and advanced-stage disease are shown in Supplementary Table S1. Advanced-stage patients exhibited higher rates of CEA positivity (40.0% vs. 7.7%, p = 0.028), significantly more symptomatic presentations (72.5% vs. 41.9%, p = 0.009), and a markedly greater need for systemic chemotherapy (90.0% vs. 6.5%, p < 0.001).
Discussion
This study comprehensively evaluated the clinical characteristics, psychological and social burdens, fertility-related concerns, and utilization of support services among young adults aged 15–39 years diagnosed with CRC. The median age at diagnosis in this population was 35 years, with the majority in their thirties and a smaller—but clinically meaningful—proportion in their twenties. Our findings revealed that 59.2% of patients were diagnosed following symptomatic presentation, with this proportion rising to 91.7% among those in their twenties. In contrast, screening-based detection was significantly less frequent in this younger subgroup (16.7%) compared with those in their thirties (49.2%). These results are consistent with the expected pattern that diagnosis in younger adults is largely symptom-driven. However, our data further demonstrate that even within the AYA population, there is a substantial age-related difference, with patients in their twenties being almost exclusively diagnosed based on symptoms, whereas those in their thirties more frequently undergo screening or opportunistic detection. Given that population-based CRC screening in Japan generally begins at age 40, screening-detected cases in younger individuals likely reflect opportunistic screening, employer-based health checkups, or evaluations prompted by mild symptoms rather than organized screening programs.
This pattern is in agreement with international evidence showing that AYA are rarely included in routine CRC screening programs and often underestimate their own cancer risk, resulting in delayed medical evaluation.2,4,9 Singh and colleagues reported that diagnostic delays are common in AYA CRC, in part because symptoms are frequently misinterpreted as benign conditions due to the patient’s young age.2,9 The particularly low screening detection rate among individuals in their twenties in our study underscores the need for improved awareness, earlier recognition of warning signs, and proactive diagnostic strategies for younger adults.
Regarding tumor characteristics, a substantial proportion of patients presented with advanced disease, including Stage II–IV cases and nearly half with lymph node involvement. These findings are concordant with prior studies indicating that young adults tend to present at more advanced stages.9,10 Although young age itself does not necessarily predict poorer prognosis, delayed diagnosis contributes significantly to advanced disease at presentation. In keeping with established prognostic trends in CRC, patients with Stage II–IV disease demonstrated significantly worse overall survival compared with those with Stage 0–I disease. Meanwhile, survival outcomes did not differ between patients in their twenties and thirties, nor between men and women, suggesting that within the AYA population, tumor burden and treatment factors play a more decisive role than age.
Representative previous studies addressing psychosocial distress, fertility-related concerns, and supportive care in adolescents and young adults with cancer and young-onset colorectal cancer are summarized in Supplementary Table S2. Psychological distress was notably prevalent. A total of 77.5% of patients experienced at least one psychological concern, with future-related anxiety (64.8%), treatment-related anxiety (45.1%), and economic or daily-life worries (22.5%) being particularly common. These rates exceed the distress prevalence of 30%–50% reported in prior AYA cancer studies, such as those by Wong et al., 11 indicating that young adults with CRC may be uniquely vulnerable to psychological stress. Zebrack and colleagues have emphasized that AYA patients often experience emotional isolation and uncertainty due to disruptions in career development, education, social relationships, and independence. 5 In our cohort, nearly 80% of patients were employed at diagnosis, yet almost one-quarter reported financial concerns, reflecting the precarious socioeconomic position characteristic of early adulthood.
Fertility-related concerns also played a substantial role in the psychosocial impact of cancer within this population. Fertility anxiety was present in 22.5% of patients, with a significantly higher prevalence among women (35.5%) than men (12.5%). Fertility counseling likewise occurred more frequently among women (32.3%) compared with men (12.5%). These findings parallel previous research by Peate et al., who reported significant decisional conflict among AYA patients regarding fertility, and by Loren et al., who documented globally low rates of fertility preservation despite widespread concern.12–14 Only 9.9% of patients in our cohort underwent fertility preservation, consistent with international reports of low uptake.14,15 Barriers may include the short interval between diagnosis and treatment initiation, insufficient counseling, cost, and lack of structured referral pathways. The observed sex disparity in counseling reflects prior findings suggesting that women are more commonly engaged in fertility discussions, whereas men may be less likely to receive or seek such information.12,14 These results highlight the need for standardized, gender-inclusive fertility counseling for all reproductive-age patients with CRC.
With regard to social support, the majority of patients required hospitalization, and medical social workers were involved in two-thirds of cases. Discharge planning support was provided to more than 70% of patients, indicating that in-hospital support was relatively well established. However, public support programs were markedly underutilized: only small proportions of patients received designated intractable disease certification, disability certification, or welfare assistance. Although more than half of the patients benefited from private insurance, only 9.9% used sickness allowance. This mismatch between documented economic concerns and limited use of public resources mirrors findings from United States studies, such as those by Guy et al., highlighting the substantial financial toxicity experienced by AYA cancer survivors. 16 Barriers to public support may include lack of awareness among patients and providers, burdensome administrative requirements, and the cultural perception that young adults are not typical beneficiaries of such programs. Early involvement of social workers and targeted guidance regarding public assistance are therefore essential.17,18
These findings are consistent with prior AYA oncology literature demonstrating high levels of psychological distress and barriers to social support.5,11–20 Importantly, our study extends this evidence by providing CRC-specific data from a Japanese cohort, highlighting marked sex differences in fertility-related concerns and low utilization of public support systems.
These findings have several important implications for clinical practice in AYA CRC. First, the extremely high rate of symptomatic diagnosis among individuals in their twenties highlights the need for earlier recognition of warning signs and structured referral pathways for young adults presenting with hematochezia, persistent abdominal symptoms, or unexplained anemia. Educational outreach targeting both the public and primary care physicians may help reduce diagnostic delays. Second, given that nearly 80% of patients experienced psychological distress, routine distress screening should be integrated into standard CRC care for AYA patients, ideally at diagnosis and at major treatment decision points. Third, the marked sex disparities and overall low rates of fertility counseling and preservation underscore the necessity of implementing universal, gender-inclusive fertility discussions within the initial oncology consultation. Finally, the low uptake of public support systems suggests that early, proactive involvement of medical social workers may facilitate timely access to financial and social resources. A structured multidisciplinary care model—incorporating oncology, psychology, reproductive specialists, and social work—would be particularly beneficial for addressing the multidimensional needs of this population.
A relatively large proportion of patients in this cohort had Stage 0 disease and were treated with endoscopic resection. Although these patients generally undergo less intensive treatment, AYA individuals may still experience substantial psychosocial and fertility-related concerns regardless of disease stage. Nevertheless, the inclusion of early-stage cases may have influenced the overall burden estimates, as their clinical trajectories differ from those with advanced disease. Future studies focusing on stage-specific psychosocial needs are warranted. This study has limitations inherent to its retrospective, single-center design and reliance on medical record documentation, which may have led to underestimation of psychosocial and fertility-related concerns. Although structured screening tools were routinely used to assess psychosocial domains, some degree of underestimation remains possible, as psychological distress may not always be fully captured in retrospective records. In addition, patients classified as having no psychological concerns may have had undocumented distress, which could have led to misclassification bias. Nevertheless, a key strength of this study lies in its comprehensive, real-world evaluation of multidimensional unmet needs among Japanese young adults with CRC. The relatively small sample size, particularly in the younger subgroup, may have limited the statistical power to detect differences in several clinical variables; therefore, negative findings should be interpreted with caution.
Conclusion
In conclusion, young adults with CRC face multidimensional challenges that extend beyond tumor biology, including delayed diagnosis, substantial psychological distress, fertility-related concerns, and inadequate utilization of social support systems. Our findings highlight the need for improved early recognition of symptoms in younger individuals, routine assessment of psychological distress, and equitable, gender-inclusive fertility counseling. Furthermore, the low uptake of public support resources underscores the importance of strengthening multidisciplinary support systems that proactively connect AYA patients with available financial and social services. By addressing these unmet needs through a comprehensive, age-appropriate care model, outcomes and quality of life for this vulnerable population can be meaningfully improved.
Authors’ Contributions
H.Y. conceived and designed the study. H.Y. and M.F. collected and analyzed the data. H.Y. supervised the project and critically revised the article. H.Y., M.F., M.M., T.I., F.Y., T.Ic., D.N., T.M., Y.K., K.U., A.M., T.M., Y.Y., S.K., S.N., T.K., and T.It. contributed to patient care and clinical data acquisition. All authors interpreted the results, drafted or revised the article, and approved the final version of the article.
Supplemental Material
sj-docx-1-jay-10.1177_21565333261464965 — Supplemental material for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer
Supplemental material, sj-docx-1-jay-10.1177_21565333261464965 for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer by Hayato Yamaguchi, Masakatsu Fukuzawa, Takashi Kawai, Midori Muzumachi, Tomohiro Ida, Fumito Yamanishi, Tadashi Ichimiya, Daiki Nemoto, Takahiro Muramatsu, Yasuyuki Kagawa, Kumiko Uchida, Akira Madarame, Takashi Morise, Yoshiya Yamauchi, Shin Kono, Sakiko Naito, and Takao Itoi
Supplemental Material
sj-docx-2-jay-10.1177_21565333261464965 — Supplemental material for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer
Supplemental material, sj-docx-2-jay-10.1177_21565333261464965 for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer by Hayato Yamaguchi, Masakatsu Fukuzawa, Takashi Kawai, Midori Muzumachi, Tomohiro Ida, Fumito Yamanishi, Tadashi Ichimiya, Daiki Nemoto, Takahiro Muramatsu, Yasuyuki Kagawa, Kumiko Uchida, Akira Madarame, Takashi Morise, Yoshiya Yamauchi, Shin Kono, Sakiko Naito, and Takao Itoi
Supplemental Material
sj-docx-3-jay-10.1177_21565333261464965 — Supplemental material for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer
Supplemental material, sj-docx-3-jay-10.1177_21565333261464965 for Clinical Characteristics, Psychosocial Concerns, and Supportive Care Needs in Young Adults with Colorectal Cancer by Hayato Yamaguchi, Masakatsu Fukuzawa, Takashi Kawai, Midori Muzumachi, Tomohiro Ida, Fumito Yamanishi, Tadashi Ichimiya, Daiki Nemoto, Takahiro Muramatsu, Yasuyuki Kagawa, Kumiko Uchida, Akira Madarame, Takashi Morise, Yoshiya Yamauchi, Shin Kono, Sakiko Naito, and Takao Itoi
Footnotes
Acknowledgment
The authors would like to thank the staff and colleagues from the Department of Gastroenterology for their valuable assistance and support in conducting this study.
Author Disclosure Statement
None of the authors have any conflicts of interest to declare.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.