
Abstract
Background:
Research on emotional exhaustion (EE) among Lebanese registered nurses (RNs) during the COVID-19 pandemic is lacking, despite the extensive literature addressing EE within the healthcare workforce. This study explores the relationships between EE, self-confidence in learning (SCL), coping strategies, and perceived organizational support (POS).
Methods:
A cross-sectional study analyzed a convenience sample of 82 RNs in medium-to-large acute care settings providing direct COVID-19 patient care. Data were gathered through an online survey that measured sociodemographic, SCL, POS, coping strategies, and EE. Statistical analyses involved descriptive statistics, bivariate analysis, and multiple linear regression to identify EE predictors.
Findings:
Most participants were female (79.0%), married (56.1%), employed in the private sector (85.4%), and located in Beirut (63.4%). Bivariate analysis indicated that problem-focused coping (β = .32; p = .017) and dysfunctional coping (β = .38; p = .019) were positively associated with EE, while POS (β = −.21; p = .002) and marriage (β = .36; p = .040) were negatively related to EE. The final regression model explained 32% of variance in EE (p < .001), showing that POS (β = −.18; p = .007) and emotion-focused coping (β = −.74; p = .001) were associated with lower EE levels, while problem-focused coping (β = .60; p = .003) correlated with higher EE levels.
Conclusions:
POS and emotion-focused coping were protective factors against EE, while problem focus strategies increased EE levels. This highlights the need for enhanced organizational support and tailored coping interventions to mitigate burnout among nurses.
Application to Practice:
Healthcare organizations should prioritize psychological support and resilience training to address EE among nurses. Policies should promote emotion-focused coping and reduce problem-focused coping strategies to enhance workforce well-being and retention.
Background
Emotional exhaustion (EE), a key component of burnout, is characterized by experiencing emotional drain and lack of motivation due to constant exposure to stressors (Khammissa et al., 2022; Maslach & Leiter, 2016; Nabizadeh-Gharghozar et al., 2020). According to the World Health Organization (WHO, 2019), EE is recognized as an occupational phenomenon that impacts the global workforce. In fact, EE is particularly relevant in the healthcare sector, where professionals face extreme personal and professional demands. Research shows that EE in healthcare has far-reaching implications that extend beyond individual well-being to affect job performance, organizational efficacy, and patient safety (Carthon et al., 2021; Schlak et al., 2021).
Healthcare systems often face overwhelming challenges and extraordinary demands during crises, such as natural disasters, economic collapses, and pandemics. As a result, EE, and stress levels among frontline workers, particularly nurses, significantly increase (Al Maqbali et al., 2021; Ding et al., 2022; Tselebis et al., 2020). A 2022 survey underlined the universality and urgency of the situation, revealing that over 60% of nurses reported significant levels of EE during the COVID-19 pandemic (Khan et al., 2022). In consequence, studies indicate that high levels of EE among nurses correlate with an increase in hospital-acquired infections, medical errors, and patient mortality rates, along with reduced patient satisfaction and high turnover (Cimiotti et al., 2012; Kelly et al., 2021; Melnyk et al., 2018).
In fact, addressing EE among nurses in crisis settings also necessitates a comprehensive understanding of coping mechanisms and the role of organizational support in reducing stress. Coping strategies are behavioral, cognitive, and emotional mechanisms used to manage extremely disturbing crises (Carr & Pudrovska, 2007). According to Lazarus (1984), coping strategies are categorized into problem-focused approaches to resolve external challenges and emotion-focused approaches to help regulate internal emotional responses. However, the effectiveness of these strategies depends on contextual situations, stress levels, and the individual’s perceived sense of control over their circumstances (Marcolongo et al., 2021). Evidence from regional studies also suggests that there exists a variation in coping mechanisms across different cultures, highlighting the importance of contextual awareness in developing effective coping interventions (Mohammadzadeh et al., 2021; Rony et al., 2022; Saeedi et al., 2023). The level of organizational support is another critical determinant of well-being and EE, where research indicates that nursing staff offered psychological support programs, resilience training, and stress management resources often experience lower levels of EE (Carthon et al., 2021; Kelly et al., 2021). However, this form of support is deficient in resource-limited settings, which imposes an increased threat of the implications of EE on nurses.
Overlapping crises in resource-limited settings, like Lebanon, place additional pressure on the pre-existing vulnerabilities of health systems and the workforce. The Lebanese healthcare system has been seriously strained by the combined effects of long-term military conflict, economic hardship, the COVID-19 pandemic, and the Beirut port explosion in 2020 (World Bank, 2021). The Beirut explosion particularly damaged and overloaded the healthcare facilities, as it occurred alongside a financial collapse that drastically reduced hospital budgets, staff-to-patient ratios, and nurse compensation (Bou Sanayeh & El Chamieh, 2023; Devi, 2020; Hajjar et al., 2021). As a result, nurses in Lebanon faced unprecedented demands of prolonged working hours, increased exposure to illness, and unpaid overtime, making them especially vulnerable to sustained EE (J. Chen et al., 2021; R. Chen et al., 2021; Kawa et al., 2022; Ness et al., 2021; Shigemura et al., 2020).
However, research on EE among frontline nurses in Lebanon during the COVID-19 pandemic is lacking, despite the extensive body of global literature addressing EE within the healthcare workforce. Accordingly, this study aims to bridge this gap by investigating the factors contributing to EE among Lebanese nurses during COVID-19. Specifically, it explores the relationships between EE, self-confidence in learning, coping strategies, and organizational support, to identify barriers and facilitators of resilience among first-line nurses in Lebanon. The dynamics explored in this study will help develop research-informed and occupational health interventions to optimize nurse training, support systems, and organizational policy, thus contributing to the improved preparation of health systems in resource-limited settings for future crises.
Methods
This study assessed the determinants of EE in Lebanese nurse COVID-19 front liners. We measured self-confidence in learning (SCL) as a factor that helps participants to adopt and consistently adhere to the new practices needed to take care of patients suffering from COVID-19. We evaluated the level of organizational support (OS) perceived by the participants since it plays an important role in supporting, facilitating, and implementing changes. This was especially important to monitor since nurses in COVID-19 wards required extensive training before a change could take place. The coping mechanisms of participants were assessed as part of the evaluation process, which helps individuals adapt or improve their practice based on experience.
Design
This study adopted a cross-sectional design.
Population and Sample
The study consisted of a convenience sample (n = 82) of Lebanese Registered Nurses (RNs) working in medium to large acute care health organizations (HCOs) in Lebanon, and who provided direct nursing care to COVID-19 confirmed or highly suspected cases.
Ethical Considerations
Consent was obtained by the research team before any data collection. Participants received an electronic informed consent form that explained the study purpose, procedures, risks, benefits, voluntary participation, and confidentiality protections. Only participants who provided consent were able to access and complete the survey. Participant privacy and confidentiality were strictly maintained in accordance with the Institutional Review Board (IRB) at the University of Balamand protocol 004-2021t. The survey was administered anonymously through secure online links distributed to participants’ email addresses or phone numbers using the Order of Nurses in Lebanon database. The research team ensured that no identifying information were collected, as stated in the consent document. All data were stored in password-protected files on secured, locked devices located in the primary investigator’s office.
Sampling and Recruitment
Respondents were accessed by direct online survey using the Order of Nurses of Lebanon database. Also, the call for study participation to all registered nurses in the Order of Nurses, including the direct link to the online study survey, was shared publicly on social media platforms for better access to the population of interest. During the COVID-19 pandemic, the use of online surveys for data collection proved to be advantageous, given the education level of the participating nurses (Registered Nurses) and their familiarity with technology. This approach facilitated the advancement of the research activities while ensuring that safety and accessibility for the respondents were preserved.
Sample Size and Power
A priori sample size (n = 70) was estimated using G* power 3.1 software with a study power of 95%, a statistical significance level of .05, an estimated effect size (f2 = 0.35), and seven predictors (including three coping subscales each representing a separate variable). These values were estimated a priori based on reported effect sizes in similar contexts as follows: (a) perceived stress was negatively associated with both self-efficacy (r = −.473, p < .01) and life satisfaction (r = −.470, p < .01; Lee et al., 2016). Also, self-efficacy was positively correlated with life satisfaction (r = .450, p < .01) (Lee et al., 2016). Perceived organizational support was negatively related to emotional exhaustion (r = −.47) and burnout (r = −.46; Kurtessis et al., 2017). In addition, meta-analytical findings showed that the weighted mean correlation between emotional exhaustion and emotion-focused coping (r = .33, p ≤ .001) was significant. The weighted mean correlations between emotional exhaustion and problem-focused coping (r = .05, p ≤ .01), reappraisal (r = .15, p ≤ .05), and acceptance (r = .14, p ≤ .01) were small to medium and were statistically significant (Shin et al., 2014).
Data Sources/Collection
Four waves of COVID-19 infections struck Lebanon, extending between February 2020 and December 2022. Data collection took place after the second wave of COVID-19 between June 2021 and January 2022.
Data Tools
Four instruments producing continuous data were used to collect data, with 30 to 40 minutes total estimated subject burden time. Instruments were provided in English since it was widely and professionally used and was well understood by our target population. The scales used for data collection were:
Predictor Variables
(1) Socio-demographic variables: Gender, marital status, work sector, location, nursing degree categories, and monthly income.
(2) Self-Confidence in Learning (SCL), an 8-item scale that measured respondents’ satisfaction and self-confidence in learning to obtain the instruction they needed. Reported Cronbach’s alpha values for the entire scale (satisfaction and self-confidence) were found to range from .77 to .85 (Unver et al., 2017).
(3) Perceived Organizational Support (POS), the short version of POS (eight items) was used to measure the employee’s perception and belief as to how supportive occupational environments were and to what extent the organization valued the employee’s contribution and well-being. Cronbach alpha ranged between .89 and .94 (Rhoades & Eisenberger, 2002).
(4) Responder’s Coping Mechanism COPE Brief was used to assess the coping mechanism adopted by the participants in this study. The COPE-Brief was composed of 28 items testing 14 coping strategies in three subscales (emotionally focused, problem-focused, and dysfunctional). Psychometric properties of the COPE-Brief showed an overall average alpha reliability for all coping strategies exceeding .60 (Carver, 1997; Trockel et al., 2018) with good reported internal consistencies for emotion-focused, problem-focused, and dysfunctional subscales (α = .72, .84, .75 respectively; Cooper et al., 2008).
Outcome Variables
The Perception of Emotional Exhaustion (EE) was measured using the Professional Fulfillment Index (PFI). A work exhaustion subscale of 10 items measured the respondents’ frequency of feeling emotionally overextended and exhausted by work. This instrument included items that explicitly specify interpersonal disengagement pertaining to patient care resulting from work exhaustion. Test-retest reliability estimate was (α = .86; Trockel et al., 2018).
Data Analysis
The SPSS software package version 28 (IBM Corp.) was used to analyze the acquired data. The overall totals for the main outcome and the covariates were calculated by summing up the items. Then, descriptive statistics for the sample characteristics were conducted and presented as frequencies, percentages, means, and standard deviations (SD). The means and SDs for the outcome and predictors were calculated, and the mean differences between the sample’s characteristics and the outcome were investigated using the independent sample t-test and ANOVA.
The bivariate and multivariate regression analyses were performed. Variable with a p-value of less than .2 as well as main predictors were eligible to be included in the multivariate linear model. The relative contribution of each independent variable was evaluated and the overall goodness of fitness (R2) of the model was explored. Though Simpson’s paradox due to multi-collinearity was experienced after fitting the adjusted linear regression model, both correlated variables were included due to higher R2 and moderate variance inflation factor (VIF; Kim, 2019).
Results
The number of participants in the study was 82 nurses. The characteristics of the sample are reported in Table 1. The mean age of the study sample was 34.5 years old. The majority of participants were female (79.0%). Around half of the participants were married (56.1%). Most of our participants worked in the private sector (85.4%), were located in Beirut (63.4%), and were holders of a bachelor’s degree or below (61%). The majority of our sample reported being from a middle-income family (64.6%). 70.4% of our study sample didn’t report any medical history, where 95% didn’t report any previous mental health history. Slightly more than half of the sample (56.1%) had at least one of the household members testing positive for COVID-19 during the pandemic.
Distribution of Nurses by Demographics and Job Characteristics (N = 82)
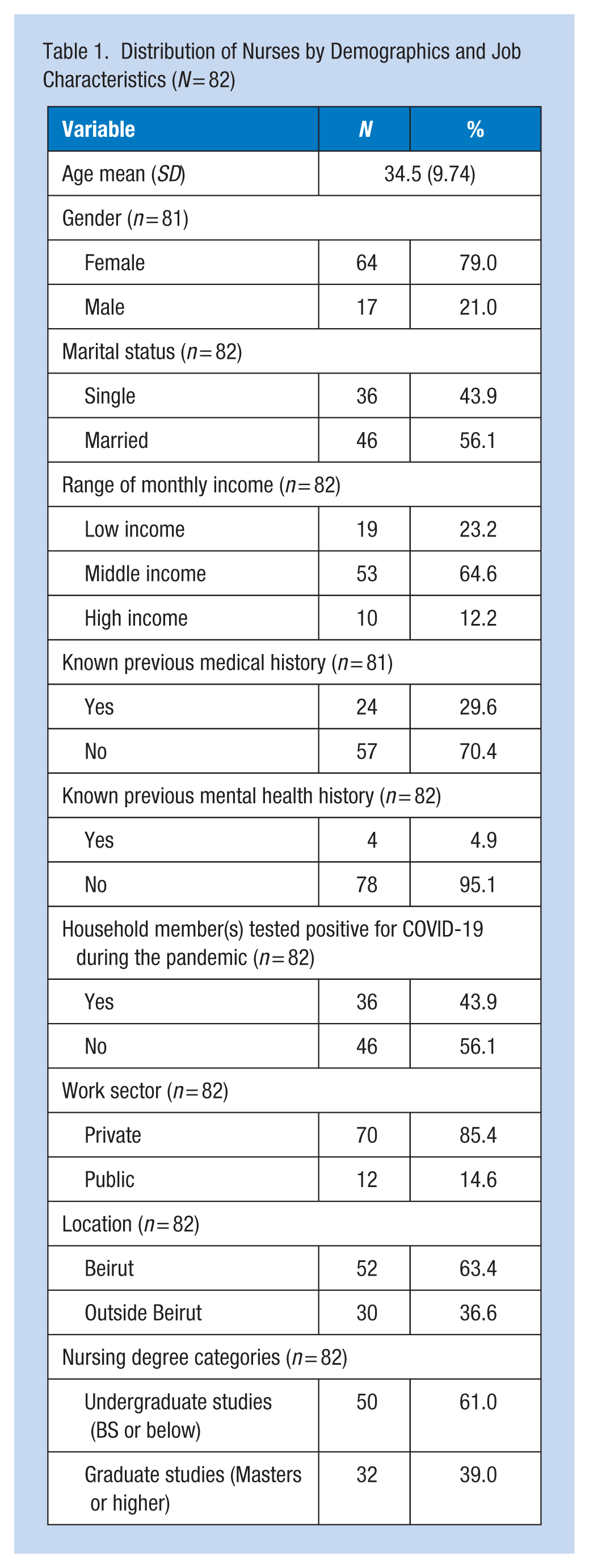
Figure 1 presents the mean and standard deviation for each measured variable. The mean for the outcome, that is, emotional exhaustion, was 2.53 ± 0.79 while that of the predictors ranged from 2.10 to 3.76.
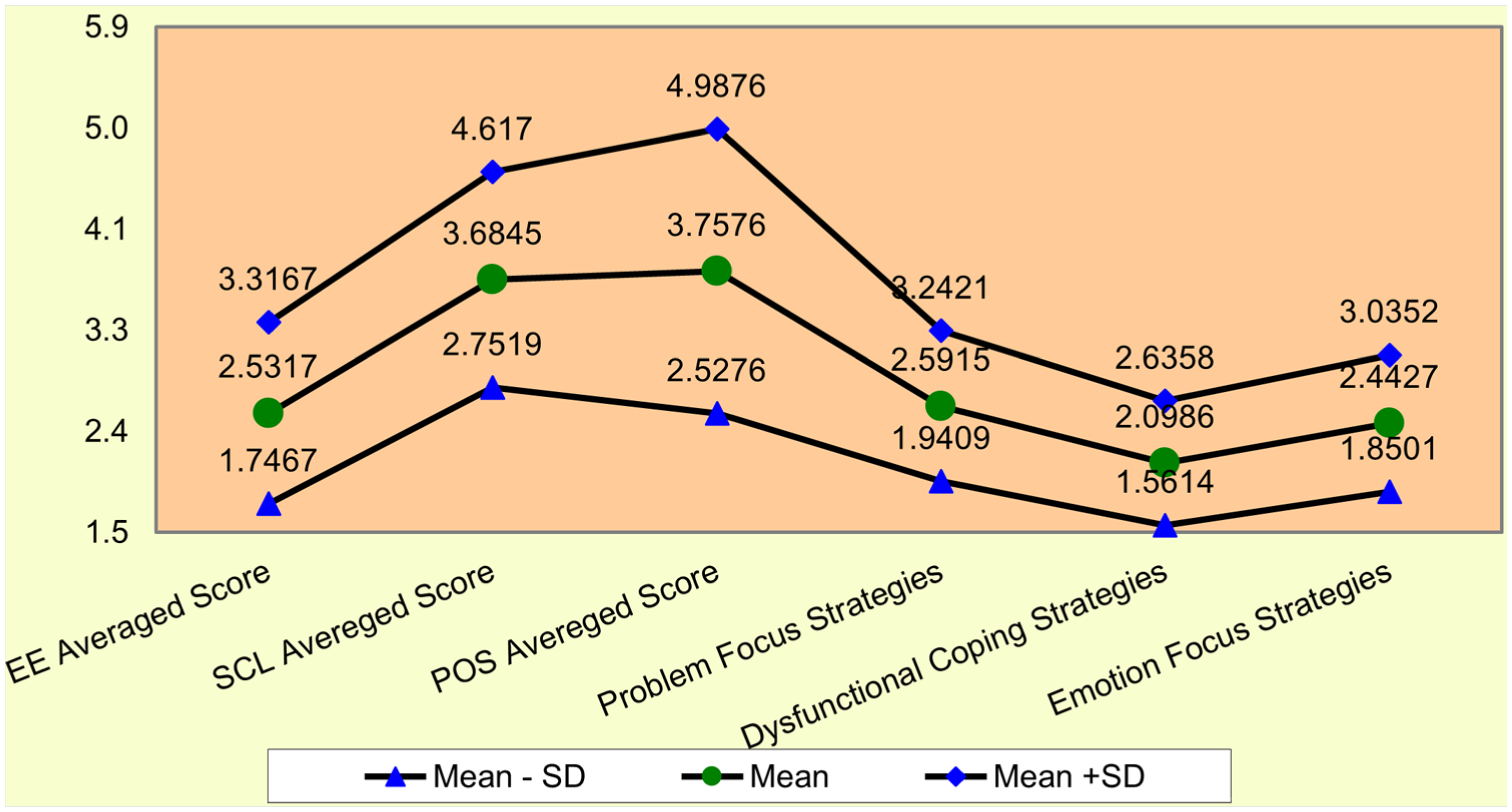
Description of measured variables (mean ± standard deviation)
Table 2 summarizes the mean emotional exhaustion scores across various demographic and professional characteristics of respondents. While marital status was the only factor with a statistically significant difference, with unmarried individuals reporting higher exhaustion (p = .040), gender, work sector, location, nursing degree, and income levels showed minor variations in mean scores that were not statistically significant.
Mean of Emotional Exhaustion by Demographic and Professional Characteristics of Respondents
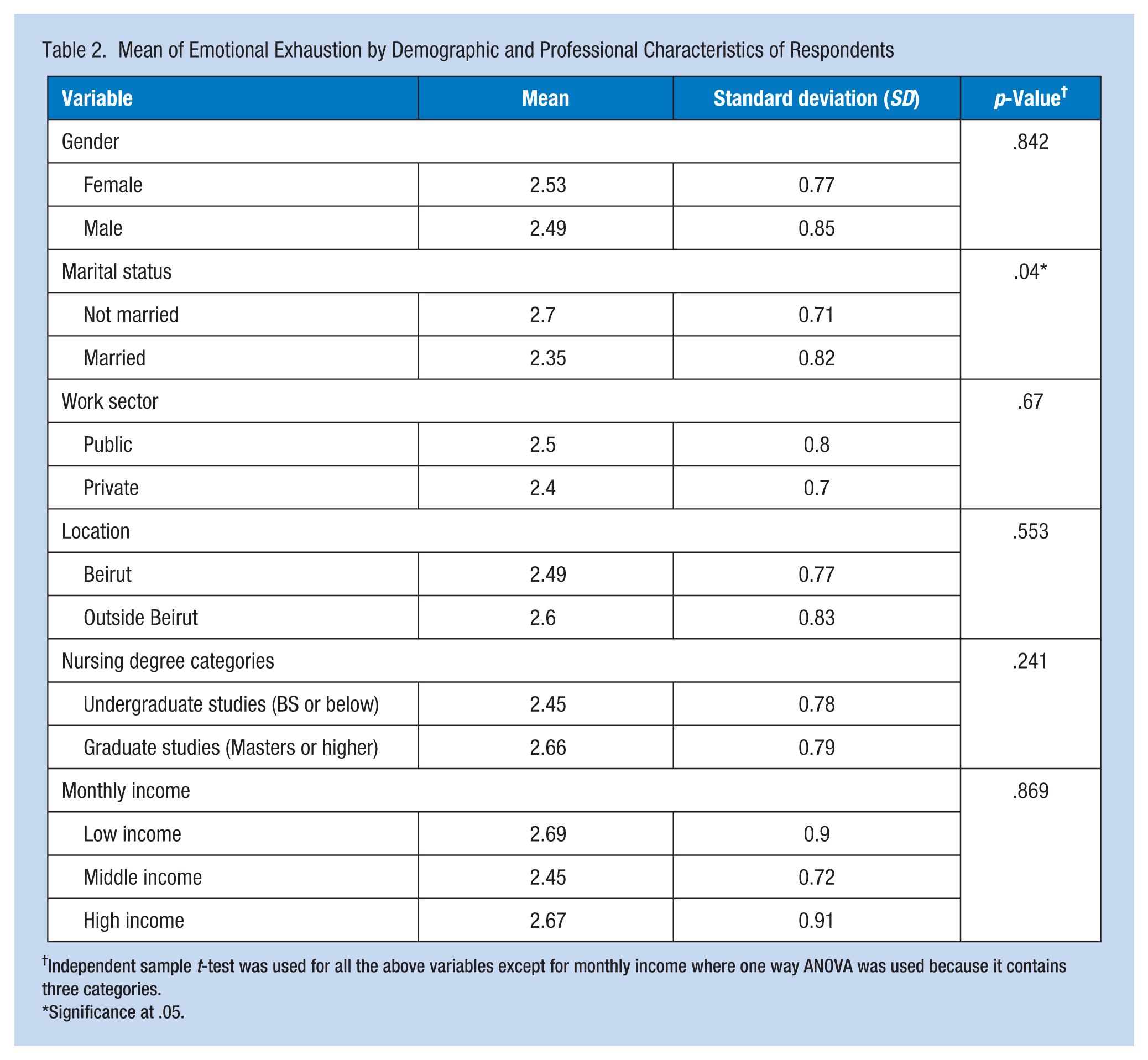
Independent sample t-test was used for all the above variables except for monthly income where one way ANOVA was used because it contains three categories.
Significance at .05.
The unadjusted and adjusted linear regressions are presented in Table 3. The bivariate analysis showed that problem focus strategies (β = .32; p = .017) and dysfunctional coping strategies (β = .38, p = .019) were significantly positively associated with EE, while POS average score (β = −.21, p = .002) and marriage (β = −.36, p = .040) were negatively associated with EE. The final multiple linear regression model explained 32% of the variance in the EE score (p < .001). Findings showed that POS (β = −.18, p = .007) and the cluster of emotion-focused coping strategies (β = −.74, p = .001) were significantly associated with lower levels of EE. Conversely, problem focus strategies (β = .60, p = .003) were significantly associated with higher levels of EE. After adjusting for other covariates, dysfunctional coping strategies (β = .31, p = .080) were not statistically significantly associated with higher levels of EE as well as SCL, marital status, and gender.
Unadjusted and Adjusted Linear Regressions Showing the Variables Predicting Emotional Exhaustion
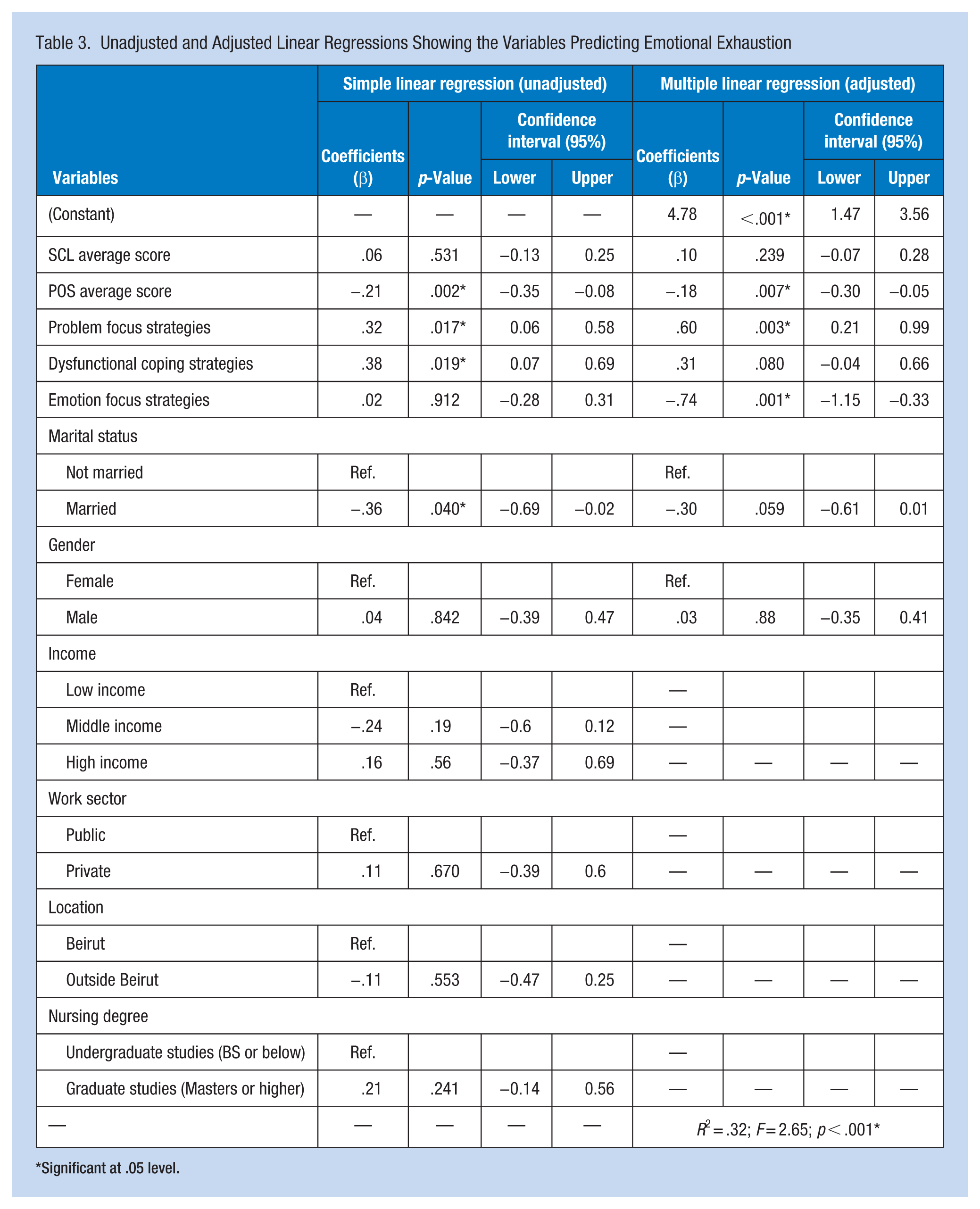
Significant at .05 level.
Discussion
The primary goal of this study was to determine whether self-confidence in learning, perceived organizational support, and responders’ coping mechanisms predict EE among nurses caring for COVID-19 patients. The goal was to investigate the connection between nurses’ EE and socio-demographic factors and the coping strategies. The linear regression model explained 32% variance in the EE. The emotion-focused strategies cluster and POS were associated with lower EE, whereas problem focus strategies were associated with a higher level of EE, and SCL, dysfunctional coping strategies or sociodemographic factors, were not found to account for variation in EE.
The relationship between SCL and EE was not fully explained in this study. This finding may be attributed to the fact that data were collected 5 to 6 months after the peak of the health crisis in Lebanon, at a period when nurses had already built their learning confidence dealing with COVID-19 cases. The effect of the process of normalization could also be at interplay, whereby work pressure, burden, and stressors related to nurses’ lack of self-confidence in learning in relation to COVID-19 had been weakened by the time data collection took place, after already experiencing the first wave of the pandemic.
Researchers have emphasized the importance of recognizing EE among health workers (HCWs). In a large sample of 107,122 HCWs by Sexton et al. (2022), with an average overall response rate of 78.6%, EE was tested over a period of 3 years coinciding with the COVID-19 pandemic. From September 2019 to September 2021, through January 2022, nurses reported a rise in EE from 40.6% to 46.5% in the first year and another rise to 49.2% in 2021 (Sexton et al., 2022). Similar findings were found in a study by Rus et al. (2020) that compared employees’ coping mechanisms and levels of emotional distress. One hundred female medical professionals from both the public and private sectors participated in this study, with a median tenure of 20 years (47%) (Rus et al., 2020). According to this study, when medical staff experience negative emotions (emotional distress), they use a variety of coping (defense) strategies to deal with the difficult situation. Stress coping strategies were found to be especially important for health care workers, who are required to think autonomously, act independently and creatively, find effective solutions to difficult situations, and overcome unconventional obstacles. However, the small sample size of this study posed a limitation to making strong conclusions (Rus et al., 2020). A study done by Wan et al. (2022) demonstrated that 77.40% of nurses during the COVID-19 pandemic reported mild levels of EE. Authors concluded that additional characteristics, which were not addressed in our study, such as more night shifts and higher years of experience, could boost EE further (Wan et al., 2022). Future research should consider these dimensions and determine whether they enhance the prediction capabilities of EE. The findings of this study underscore the critical role of POS strategies in mitigating EE among nurses during the COVID-19 pandemic. POS and coping mechanisms accounted for 32% of the variance of EE in our study sample. Similarly, in a study conducted by Poku et al. (2020), 91.1% of 232 recruited nurses reported moderate to high levels of EE, with POS accounting for 39.6% of the variation in EE.
In alignment with the findings of our study, Poku et al. (2020) also found that registered nurses used problem- and emotion-focused coping strategies to manage EE. The Poku study, however, did not provide any statistical information about the impact of emotion-focused strategies or problem-focused strategies on EE. Our findings, however, clearly showed that problem-focused strategies increase EE while emotion-focused strategies decrease EE. Both studies, Poku, and our current work, used a cross-sectional design, which was determined to be the best model for investigating predictors of EE among nurses. In a recent study done by Yanbei et al. (2023), including a convenience sample of 479 nurses from three tertiary hospitals, showed that POS could moderate the relationship between work frustration and burnout (p = .007) instead of EE. In alignment with our study, Alaseeri et al. (2023) reported a significant inverse relationship between POS and EE, showing that nurses who reported higher organizational support had significantly lower levels of emotional exhaustion, identifying POS as a protective factor against burnout-related exhaustion (Alaseeri et al., 2023). Also, a large national study by Zakaria et al. (2022) in Malaysia, including 2,428 nurses, evaluated the prevalence and risk of burnout including the domains of EE, depersonalization, and low personal accomplishment as well as the coping strategies among nurses. Like our approach, the Zakaria et al.’s (2022) paper used the emotion-focused, problem-focused, and dysfunctional coping strategies to predict EE among this large group of nurses working in hospitals and primary care settings. In their study, one in every four nurses suffered from burnout syndrome with a high score in EE and emotion-focused strategies contributed to lower scores of EE (namely use of emotional support and humor; Zakaria et al., 2022). Emotional exhaustion was significantly associated with work stressors such as night shifts, sleep deprivation, traumatic events, and dysfunctional coping, while receiving psychological support or debriefing after traumatic events was protective against EE, which reflects organizational support practices but not a measured POS construct (Zakaria et al., 2022).
Meta-analysis findings comprising 16,810 nurses concluded that nurses during the COVID-19 pandemic were highly to moderately emotionally exhausted, with several organizational factors contributing to this emotional exhaustion (Alaseeri et al., 2023). The most important organizational and job-factors related to emotional exhaustion that were discussed are linked to high-intensity work conditions, including employment in critical care or isolation units, assignment to COVID-19 quarantine areas, long working hours, frequent night shifts, and exposure to infected or suspected co-workers (Alaseeri et al., 2023). The most important organizational and job-factors related to emotional exhaustion that were discussed are linked to high-intensity work conditions, including employment in critical care or isolation units, assignment to COVID-19 quarantine areas, long working hours, frequent night shifts, and exposure to infected or suspected co-workers (Alaseeri et al., 2023). These meta-analytical findings support our study conclusions.
Study Strengths and Limitations
This study has several strengths, including its focus on registered nurses providing direct COVID-19 patient care in medium-to-large acute care settings, capturing EE in a high-risk clinical environment. By examining POS alongside emotion-focused and problem-focused coping strategies, the study clarifies how organizational and individual factors jointly influence EE. The identification of both protective and risk factors offers clear, actionable targets for practice and policy, and the findings translate directly into organizational strategies such as psychological support and resilience training, strengthening the study’s relevance for workforce well-being and nurse retention within Lebanese hospital settings. While this study successfully examined the predictors of emotional exhaustion of Lebanese nurses front liners during the pandemic, there were some limitations. Though the sample size was bigger than targeted, however, an even larger sample would have added to the effect size of the model and power of the findings. In addition, the study design does not allow cause and effect conclusions. Finally, the timing of data collection (after the second wave) might have neutralized the relationship of some predictors with EE.
Recommendations for Future Research and Nursing Practice
Targeted research is needed, focused on examining the cause-and-effect relationships between the identified predictor factors in the study model and EE of frontline nurses. In addition, testing this model in other population and cultural locations during crisis would enhance the generalization of the findings. Qualitative studies that focus on understanding the experiences of coping with EE and normalization processes employed by nurses when exposed to prolong job stressors (such as a long-haul pandemic) are also key in establishing a deeper understanding and shaping better informed interventions in the professional practice of acute care.
When appropriate and effective interventions are employed, at both the organizational and personal levels, EE will be reduced, decreasing the risk of burnout and improving quality-of-care delivery to patients, especially in uncertain times such as a pandemic. Addressing modifiable factors that can alleviate EE at individual and institutional levels will be beneficial in preventing and reducing burnout and its undesirable effects among nurses. Interventions that promote positive coping strategies should be implemented including psychological resilience training and how to reinforce the use of problem focused coping strategies to alleviate EE. Organization-driven efforts must focus on the enhancement of organizational support capabilities in healthcare facilities, which may include the promotion of healthy and safe work environments, balanced work schedules for nurses, the establishment of structured debriefing services, and counseling following traumatic events. Frequently appraising EE levels among nurses in crises, as a measure of early detection for initiating early intervention, would also be a positive factor. Establishing these interventions will better support the preparation of frontline health care workers, especially nurses, in facing future pandemics or prolonged work-related stressors. These interventions are essential in paving the way toward more resilient healthcare systems and informing policymakers about nurses’ protective mental health strategies in times of crisis.
Implications for Occupational Health Nursing Practice
This study offers actionable recommendations for occupational health nurses and healthcare administrators aiming to reduce EE among frontline nurses. Given that POS and emotion-focused coping strategies were linked with lower EE, occupational health practitioners must advocate for structured institutional support systems, such as ongoing training on resilience-building techniques, peer support networks, and stress management programs.
Occupational health nurses play a key role in detecting early signs of EE and implementing intervention strategies at both individual and organizational levels. This includes providing stress management workshops and mental health resources and integrating burnout prevention strategies into workplace policies. Moreover, as dysfunctional coping strategies were linked to higher EE, occupational health practitioners need to prioritize nurses’ education on adaptive coping, mainly in high-stress environments such as pandemic response units. Additionally, to improve nurse retention and workplace well-being, healthcare organizations should ensure flexible scheduling, proactive workload management, and mental health screenings.
Conclusion
The uniqueness of this study lies in being the only one in Lebanon to capture predictors of emotional exhaustion of frontline Lebanese nurses caring for COVID-19 patients amidst the pandemic. Even before the pandemic, health care workers including nurses were predisposed to high levels of burnout. Examining these predictors and their relationship with EE levels of nurses during the pandemic will hopefully aid in the early development of organizational and national strategies. It is vital to prevent reaching the tipping point of healthcare worker burnout experienced globally in 2022 and to ensure it doesn’t recur in the future.
Respondents were found to be moderately emotionally exhausted. Findings could be mostly attributed to the normalization process effect and timing of data collection following the second wave, which neutralized the relationship between confidence in learning and emotional exhaustion. Understanding the socio-demographic and organizational factors as well as the coping strategies associated with emotional exhaustion of nurses and factors facilitating normalization of care processes following this pandemic are important for implementing better prevention and response mechanisms to disaster and avoiding EE of core clinical frontliners like nurses during a long-haul pandemic.
Applying Research to Occupational Health Practice
Emotional exhaustion (EE) is shown to be a serious occupational health problem affecting frontline nurses, mainly in crisis contexts like the COVID-19 pandemic. This study showed that perceived organizational support (POS) and emotion-focused coping were linked to lower EE levels, highlighting their protective role. In contrast, problem focus strategies increased EE. Accordingly, occupational health nurses must apply these findings to design structured workplace interventions, such as employee assistance programs, psychological resilience training, and coping strategy workshops.
It is important for occupational health practitioners to recognize early signs of EE, thus integrating targeted wellness programs into organizational policy, including mental health counseling services, regular stress assessments, and peer support groups. Moreover, positive coping mechanisms and supportive work environments can help decrease burnout risk and improve nurse well-being. These evidence-based interventions can thus enhance nurse retention, job satisfaction, and patient care outcomes, eventually strengthening the resilience of healthcare systems during future crises.
Footnotes
Acknowledgements
The authors would like to thank the nurses who participated in this study, the Order of Nurses in Lebanon, and the University Research Grant (URG) office at the University of Balamand.
Author Contributions
Bahia Abdallah (BA) was responsible for the study. BA and Rana Abdel Malak (RAM) designed the research study. BA, RAM, Abir Abdel Rahman (AA), and Abed Wahab Al Firikh (AWF) analyzed the data. BA, RAM, AA, and AWF were responsible for drafting and reviewing multiple parts of this manuscript. All authors read and approved the final version of the paper.
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the University of Balamand research grant in 2021. Funding: RGA/FHS/20-21/003 UOB research grant.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of the University of Balamand IRB-REC/O/027-21/0421. The participants were provided with necessary information about the study’s objectives, and they were assured that participation was voluntary and that they could withdraw at any time. Informed consent was obtained from all the participants. The participants were also assured that their information would remain confidential.
Data Availability Statement
Data is available upon request.*