
Abstract
Language barriers remain a critical challenge in health care delivery, particularly for migrant and multicultural populations. This study presents the design, implementation, and evaluation of an artificial intelligence (AI)–driven multilingual medical health education chatbot to enhance health care communication and accessibility. The proposed system introduces a user-state–driven multi-layer logical architecture, which enables efficient multilingual interaction by dynamically routing user queries to language-specific processing modules. In addition, a hybrid retrieval–generative framework is developed to combine expert-curated health education content with conversational AI (ChatGPT), ensuring both information reliability and interaction flexibility. The system is deployed on the LINE platform and evaluated using the System Usability Scale, Net Promoter Score, and Customer Satisfaction Score with 85 participants from diverse linguistic and cultural backgrounds. The results demonstrate satisfactory usability and user acceptance, with consistent performance observed across nationality groups, supporting the system’s cross-cultural applicability. Overall, the findings indicate that the proposed architecture provides a scalable, efficient, and practical solution for multilingual health care communication, reducing language barriers and improving patient understanding in real-world clinical environments.
Keywords
Introduction
Health education represents a critical and indispensable component of the health care continuum, significantly influencing patients’ recovery processes, self-care behaviors, and long-term health outcomes. Effective health education enables patients to understand treatment procedures, adhere to prescribed medication regimens, and engage in preventive health practices. However, in contemporary clinical settings—characterized by increasing patient volumes and limited consultation time—health care professionals often face challenges in delivering comprehensive post-treatment education.
Recent advances in artificial intelligence (AI) and natural language processing have facilitated the integration of conversational agents into health care environments, enabling scalable and on-demand delivery of health education and patient support. Prior research has demonstrated the effectiveness of chatbot-based interventions in mental health support,1,2 wound care education, 3 chronic disease management,4,5 and behavioral interventions. 6 Despite these advancements, the real-world deployment of multilingual, domain-specific medical chatbots remains limited.
In parallel, Taiwan’s rapid economic development and industrial transformation have led to a substantial increase in the number of foreign migrant workers, primarily from Southeast Asia. These populations often encounter significant linguistic and cultural barriers in health care settings, which may hinder effective communication, reduce access to health information, and increase the burden on health care providers.
Unlike existing health care chatbot systems in Taiwan (e.g., Dalin Tzu Chi Hospital, 7 Taichung Veterans General Hospital, 8 Changhua Christian Hospital, 9 and Show Chwan Memorial Hospital 10 ) which are typically limited to single-language interfaces or rely on static translation mechanisms, the proposed system offers an integrated multilingual framework supporting five languages, enhanced by dynamic user-state management. By combining domain-specific, expert-curated medical knowledge with a hybrid interaction model, the system enables users—particularly migrant populations—to access reliable health education content in their preferred language and engage in interactive information retrieval. This approach effectively addresses language barriers in health care communication and provides a scalable solution for multilingual health care environments.
To further address these challenges, this study proposes a novel AI-driven multilingual medical health education chatbot architecture tailored for real-world deployment. The system introduces a user-state–driven multi-layer logical structure, which dynamically routes user queries to language-specific processing modules, thereby improving computational efficiency and scalability. In addition, a hybrid retrieval–generative framework is employed to integrate expert-curated medical knowledge with conversational AI, ensuring both information reliability and interaction flexibility.
Accordingly, this study makes key contributions from both social impact and system design perspectives. From a social impact perspective, the proposed system addresses health care communication barriers faced by migrant workers in Taiwan, an underserved population in existing digital health solutions. From a system design perspective, the study introduces a user-state–driven multi-layer architecture and a hybrid retrieval–generative framework that together enable efficient, scalable, and reliable multilingual health education delivery in real-world health care settings.
Literature Review
Evolution of chatbot technologies
Since the introduction of ELIZA in 1966, chatbot technologies have undergone rapid development alongside advances in natural language processing and machine learning. Contemporary chatbots are generally classified into retrieval-based and generative-based models. Retrieval-based systems generate responses by selecting from predefined knowledge bases, offering high reliability and grammatical correctness. In contrast, generative models dynamically construct responses but typically require extensive training data and may introduce uncertainty.
Adamopoulou and Moussiades (2020) proposed a generalized chatbot architecture, emphasizing the coordinated integration of language understanding, dialogue management, and response generation. 11 Subsequent innovations include context-aware dialogue management, ontology-driven conversational agents, 12 and end-to-end intent detection frameworks, 13 which collectively establish the technological foundation for modern conversational systems.
Chatbots in health care and health education
Recent empirical evidence has consistently demonstrated the effectiveness of conversational agents and chatbot-based interventions across multiple health care domains. In the field of mental health support, systematic reviews and meta-analyses indicate that conversational agents significantly improve psychological outcomes across diverse populations, 1 while recent comparative studies reveal that AI chatbots achieve outcomes comparable to traditional nurse hotlines in alleviating short-term anxiety and depressive symptoms. 2 Regarding wound care education, ChatGPT-generated postoperative wound care instructions have been shown to exhibit high levels of comprehensibility, usability, and informational quality, supporting the feasibility of chatbot-assisted health education delivery. 3 In the context of chronic disease management, systematic evidence suggests that chatbot-based systems effectively support patient education, self-management behaviors, and treatment adherence.4,5 Finally, within behavioral interventions, rigorous meta-analytic evidence demonstrates that chatbot interventions yield statistically significant improvements in key health behaviors, including physical activity, diet, and sleep patterns, reinforcing the role of conversational agents as scalable tools for population-level health behavior change. 6
Human-centered design and user acceptance
Beyond technical performance, the effectiveness of health care chatbots is strongly shaped by human-centered design principles. Empirical research has demonstrated that users’ perceptions of warmth, empathy, and personalization significantly influence trust formation, engagement, and overall satisfaction with chatbot systems. In particular, anthropomorphic conversational styles and emotionally expressive dialogue have been shown to enhance users’ psychological comfort and willingness to continue interaction. 14 Moreover, recent evidence indicates that social interaction cues and humanlike characteristics contribute substantially to sustaining long-term trust in AI-driven conversational agents. 15 Collectively, these findings suggest that effective health care chatbots must achieve an appropriate balance between technical competence and emotionally intelligent interaction to maximize user acceptance and service impact.
System Architecture and Algorithm Design
Overall system architecture
The proposed system implements a multilingual medical health education chatbot deployed on the LINE messaging platform (see Fig. 1). The architecture integrates cloud computing infrastructure, conversational AI, and domain-specific knowledge management to provide scalable and accessible health education services.
The architecture of the multilingual medical health education chatbot.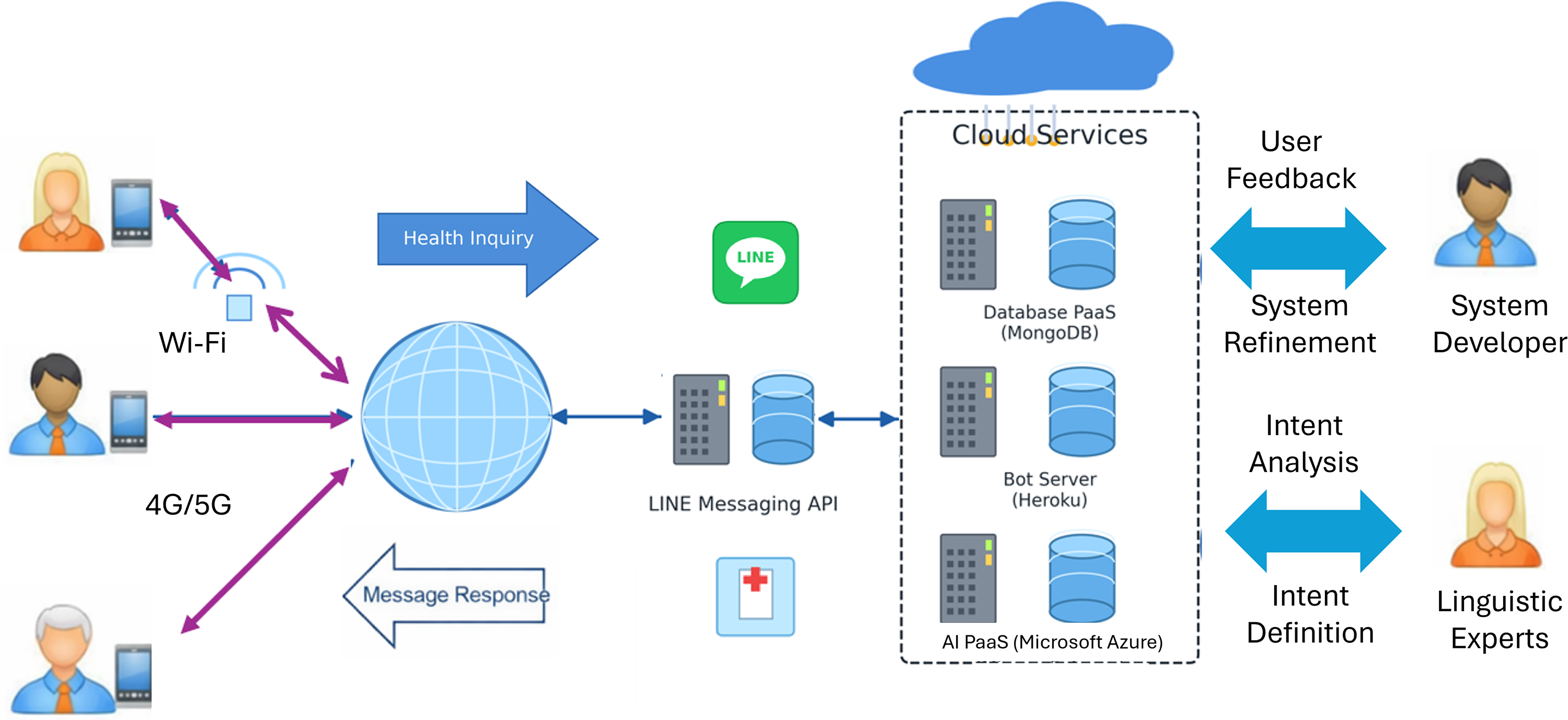
User interactions are conducted via the LINE application on mobile devices. Incoming messages are transmitted through the LINE Messaging API to the backend server, which is implemented using a Flask-based web framework. The backend system coordinates communication among the conversational engine, cloud-based natural language understanding services, and the medical knowledge base. All system components are hosted on cloud platforms to ensure reliability, scalability, and real-time responsiveness. The architecture consists of four primary layers:
User Interface Layer (LINE platform), Application Processing Layer (Flask backend and bot server), Intelligence Layer (Azure’s Conversational Language Understanding [CLU] and learning modules), and Data Layer (user database and multilingual health education knowledge base).
This layered architecture supports modular development and facilitates continuous system extension. All system modules are deployed on cloud-based platforms, enabling horizontal scalability and fault tolerance. The modular architecture supports rapid system updates, integration of new languages, and expansion of medical knowledge domains without disrupting existing services. This design ensures that the proposed chatbot system remains robust, adaptable, and suitable for large-scale deployment in real-world health care environments.
Multi-layer logical structure by user-state
The LINE chatbot follows a question–answer interaction paradigm. User inputs are processed using conditional logic structures, if–elif–else, 16 to determine appropriate responses. For multilingual operation, the system must maintain each user’s language preference to ensure delivery of language-specific health education content. Direct implementation of extensive conditional structures results in high computational complexity and increased response latency as semantic variation grows. To mitigate this limitation, the proposed system introduces an optimized conversational framework that integrates user-state management with conditional logic.
To improve efficiency and scalability, this study proposes the “User-State Multi-Layer Logical Structure (see Fig. 2),” which dynamically controls conversation flow based on each user’s functional and linguistic state. Upon initialization, the system records the user’s selected language (Chinese, English, Indonesian, Vietnamese, or Thai) and interaction context within the user database. Subsequent message processing is restricted to the logic layer associated with the current user state. This design significantly reduces unnecessary logical evaluations and improves response time. Without language-state control, each query would require evaluating the logic of all supported languages (approximately 5 × N conditional rules for five languages), which increases computational overhead. By routing requests based on the user’s language state, the system executes only a single state check and the corresponding language-specific logic branch, thereby reducing redundant evaluations and improving response efficiency. By executing only the relevant language-specific response routines, the system achieves substantial reductions in computational overhead while maintaining high response accuracy and consistency.
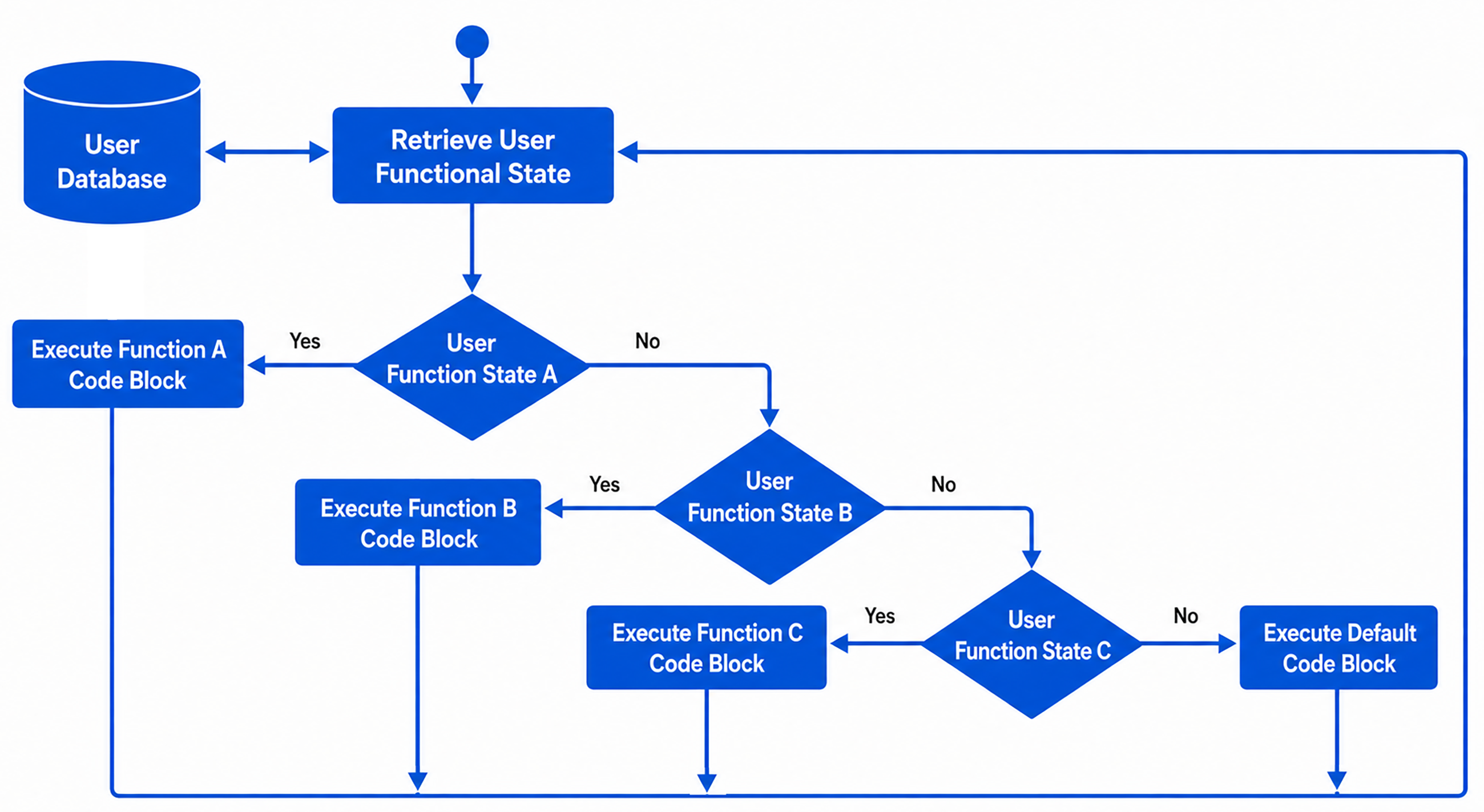
The User-State Multi-Layer Logical Structure.
In addition to the above workflow description, we provide the corresponding algorithmic process illustrating the user-state routing algorithm (shown in Fig. 3). The algorithm first retrieves the user’s current functional state from the user database. A state-driven routing process is then performed using a structured if–elif–else decision framework to determine the appropriate processing path. To further quantify the computational advantage of the proposed approach, the time complexity of the conversational routing process can be analyzed. In conventional rule-based chatbot systems, where all possible language and function conditions are evaluated, the time complexity is approximately O(L × N), where L denotes the number of supported languages, and N represents the number of logical rules. This results in redundant condition checking across all language branches for each user query. In contrast, the proposed Multi-Layer Logical Structure by User-State reduces the time complexity to approximately O(N) by restricting execution to the logic associated with the user’s current state. Specifically, the system performs a single O(N) state retrieval and routes the query to a single language-specific processing module, thereby eliminating unnecessary evaluations across other language branches. This reduction in computational complexity significantly improves system efficiency and scalability, particularly in multilingual environments with an increasing number of supported languages.
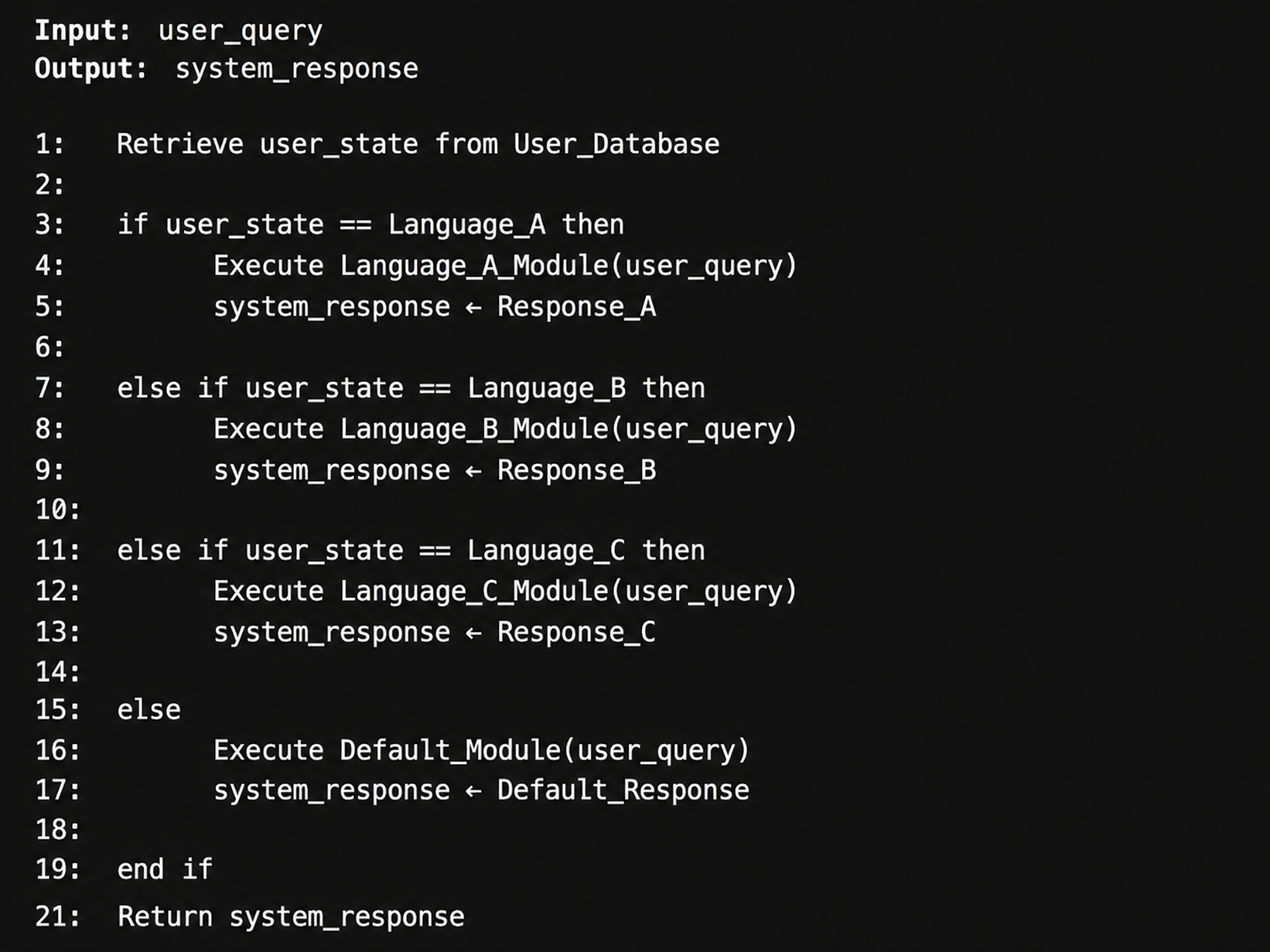
User-State–Driven Query Routing and Response Generation.
Data and learning infrastructure
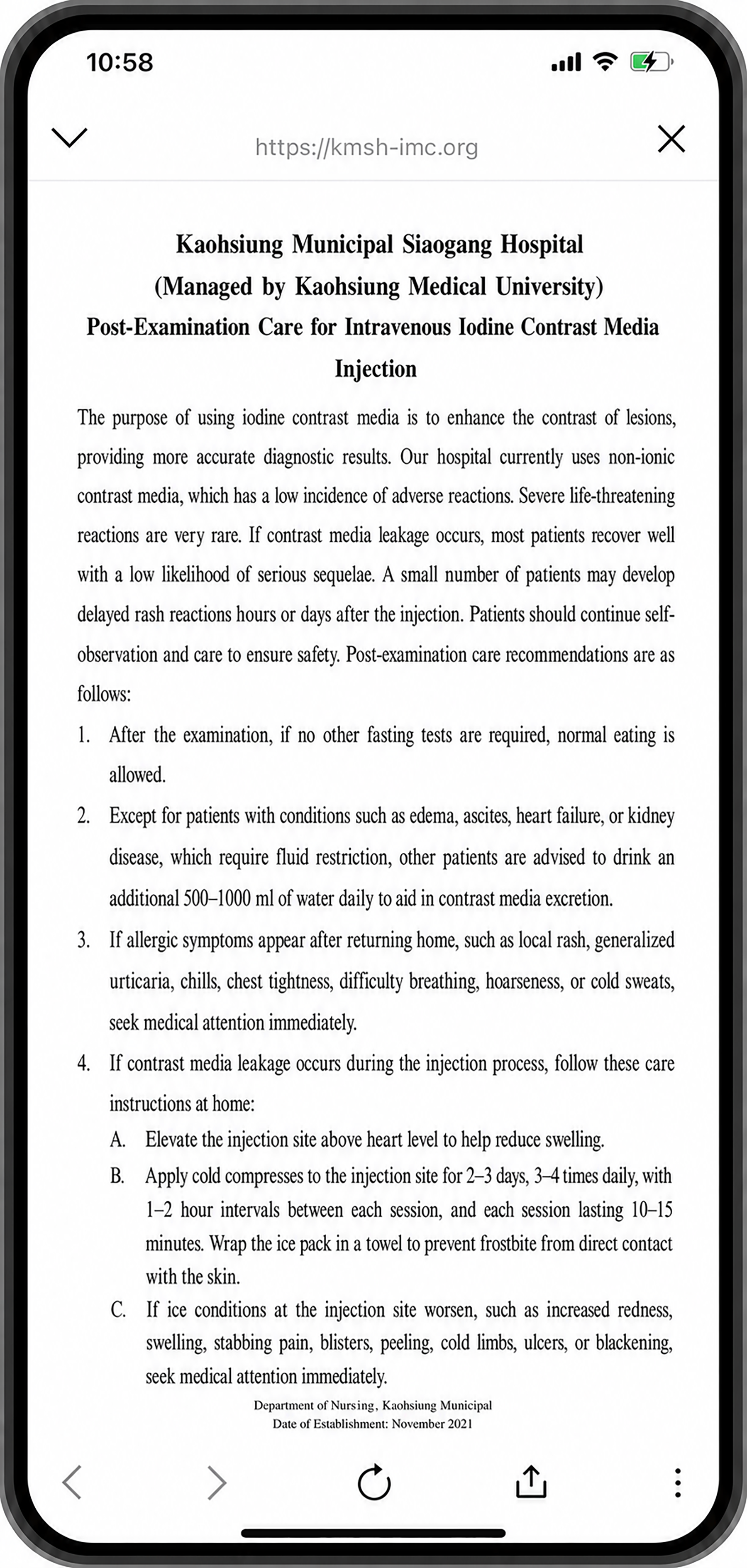
The data layer comprises two primary components: (1) a user database that stores anonymized user states and interaction histories; and (2) a multilingual medical health education knowledge base, derived from the official website of Kaohsiung Municipal Siaogang Hospital (KMSH) 17 and translated by native-speaking linguistic graduate students (including Indonesian, Vietnamese, and Thai) from Wenzao University and AI tools. 18
The intelligence layer leverages Microsoft Azure’s CLU service as a natural language understanding (NLU) framework. 19 The development of the Microsoft Azure’s CLU service follows a seven-stage pipeline: (1) schema definition, (2) multilingual data labeling by domain experts, (3) model training, (4) performance evaluation, (5) iterative model refinement using misclassified queries stored in a cloud database, (6) model deployment via runtime APIs, and (7) real-time intent and entity prediction for response generation. 20 Continuous supervised learning is conducted through expert annotation of unresolved user queries, enabling ongoing improvement of the conversational model’s accuracy and domain coverage.
To enhance the technical clarity of the NLU component, the system adopts Azure Conversational Language Understanding (CLU) to perform intent classification and entity extraction from user inputs. Specifically, user utterances are first preprocessed and sent to the CLU service via API calls, where a trained language model predicts the intent category (e.g., inquiry type) and extracts relevant entities (e.g., medical topics or health education units). The CLU model is developed through a supervised learning pipeline that includes intent definition, entity schema design, and annotation of multilingual training utterances. Annotated data are used to train and validate the model, and performance is iteratively improved through evaluation and refinement of training samples.
During runtime, the predicted intent and extracted entities are integrated with the user-state–driven routing mechanism described in the “Multi-Layer Logical Structure by User-State” section, enabling the system to map user queries to the appropriate language-specific processing module and corresponding health education content. This pipeline allows the chatbot to handle semantically diverse user inputs while maintaining structured and accurate response generation in a multilingual environment.
System Results and Evaluation
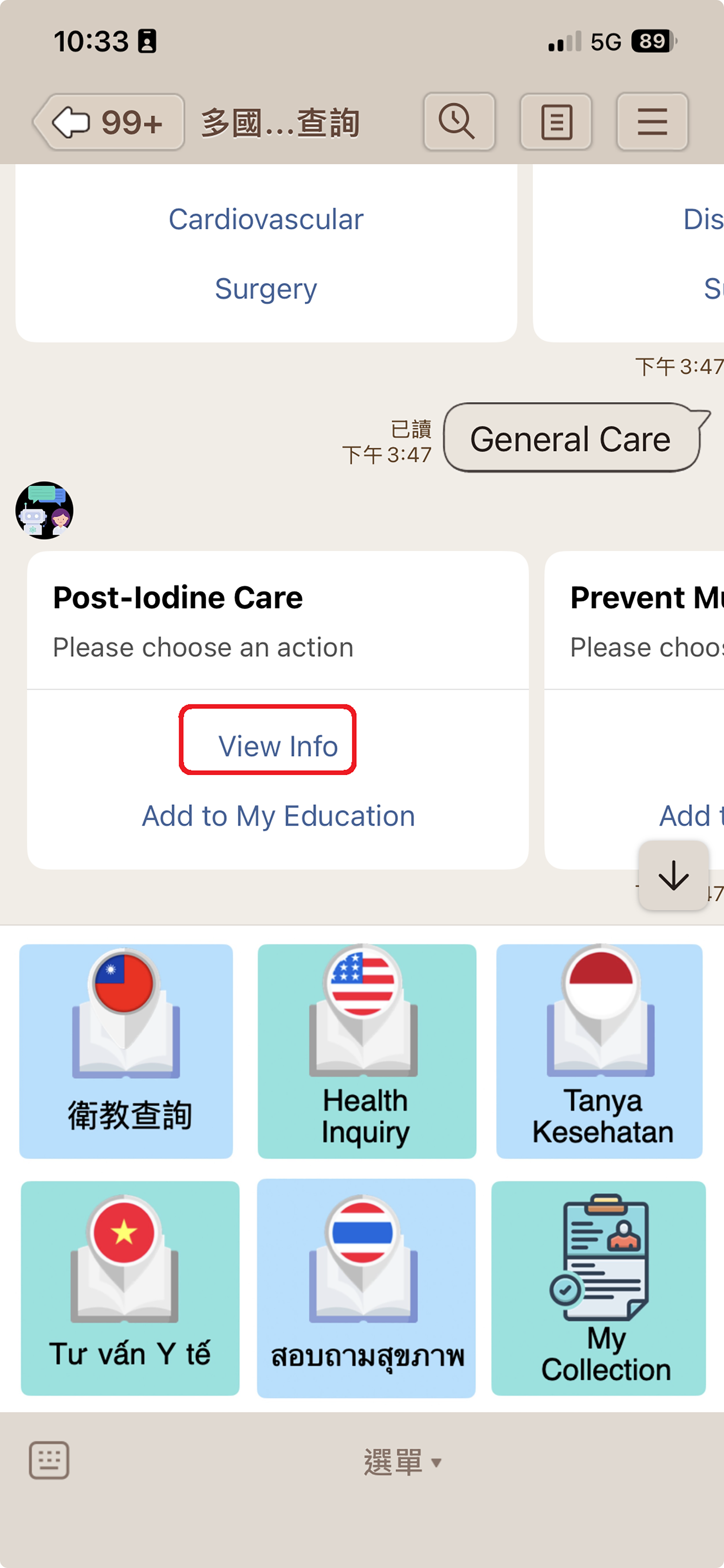
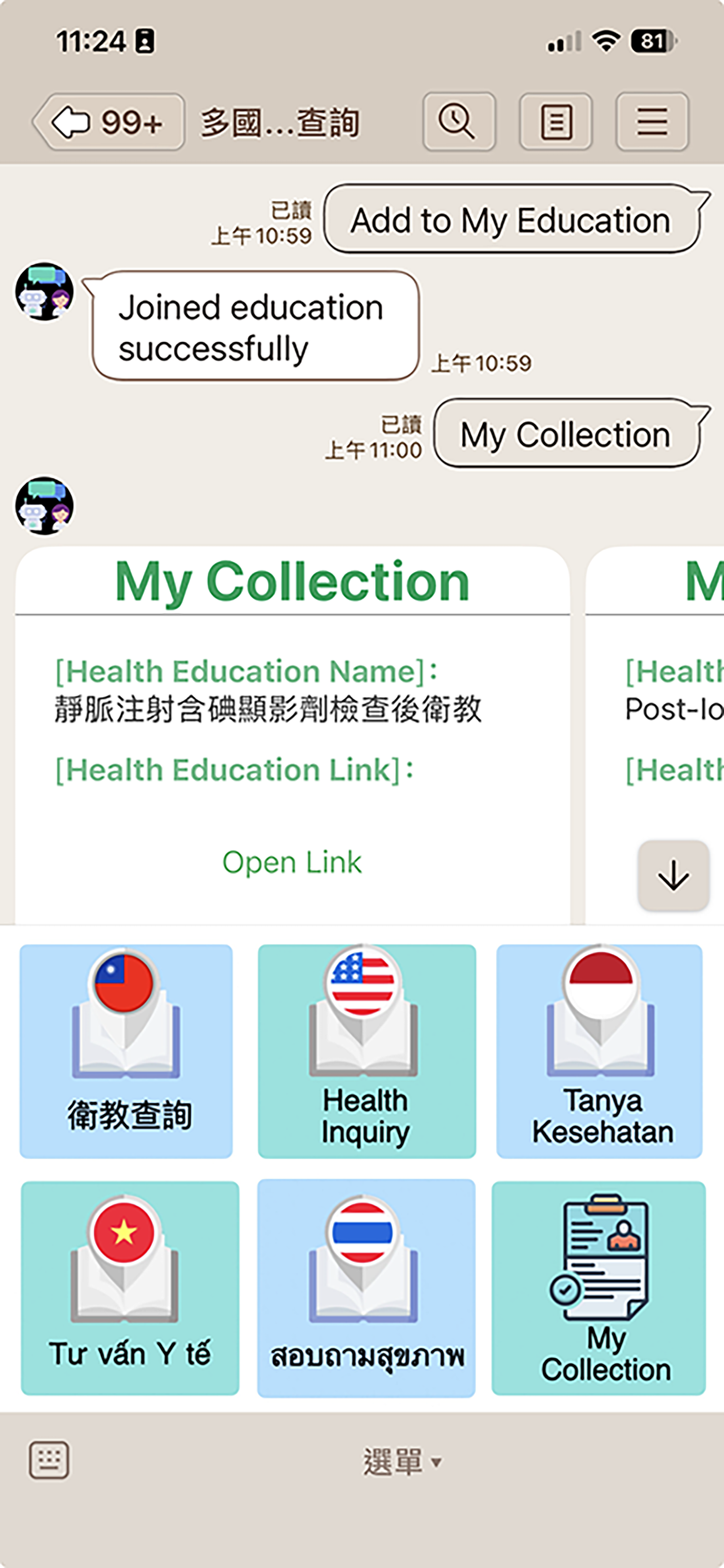
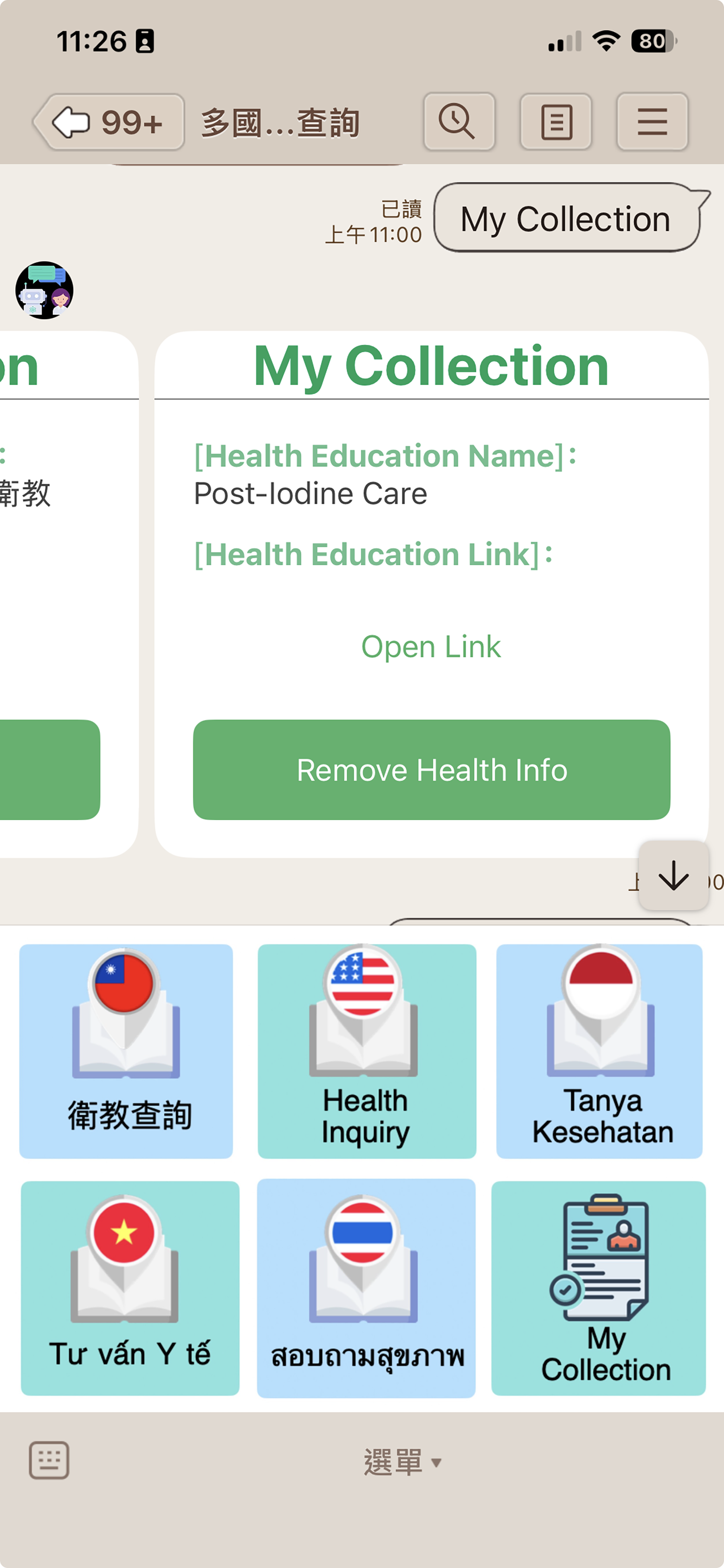
The multilingual system features are illustrated in Figure A1, and the English interface is used to demonstrate the system in Figures 4–8. The interface provides a language selection menu (Chinese, English, Indonesian, Vietnamese, and Thai) at the bottom of the screen, allowing users to choose their preferred language, as well as a “My Collection” function for storing selected health education units. As illustrated in Figure 4, users can select the English health education query option, which generates an English health education menu covering 30 medical departments. In Figure 5, users may choose a specific medical department to access the corresponding English health education unit and save it to their personal collection. When users select “View Info,” the selected health education content is displayed in PDF format with zoom-in and zoom-out functionality to enhance readability (see Fig. 6). Figure 7 demonstrates the storage of selected health education units in users’ personal collections, while Figure 8 presents a complete list of all health education units saved in the personal collection.
Select English health education information query and generate the English health education menu for 30 medical departments. Select the medical department to generate the English health education unit and store the unit in the personal collection. View the English health education unit in PDF format with zoom-in and zoom-out functionality. Store selected health education units in personal collections. List all education units of personal collections.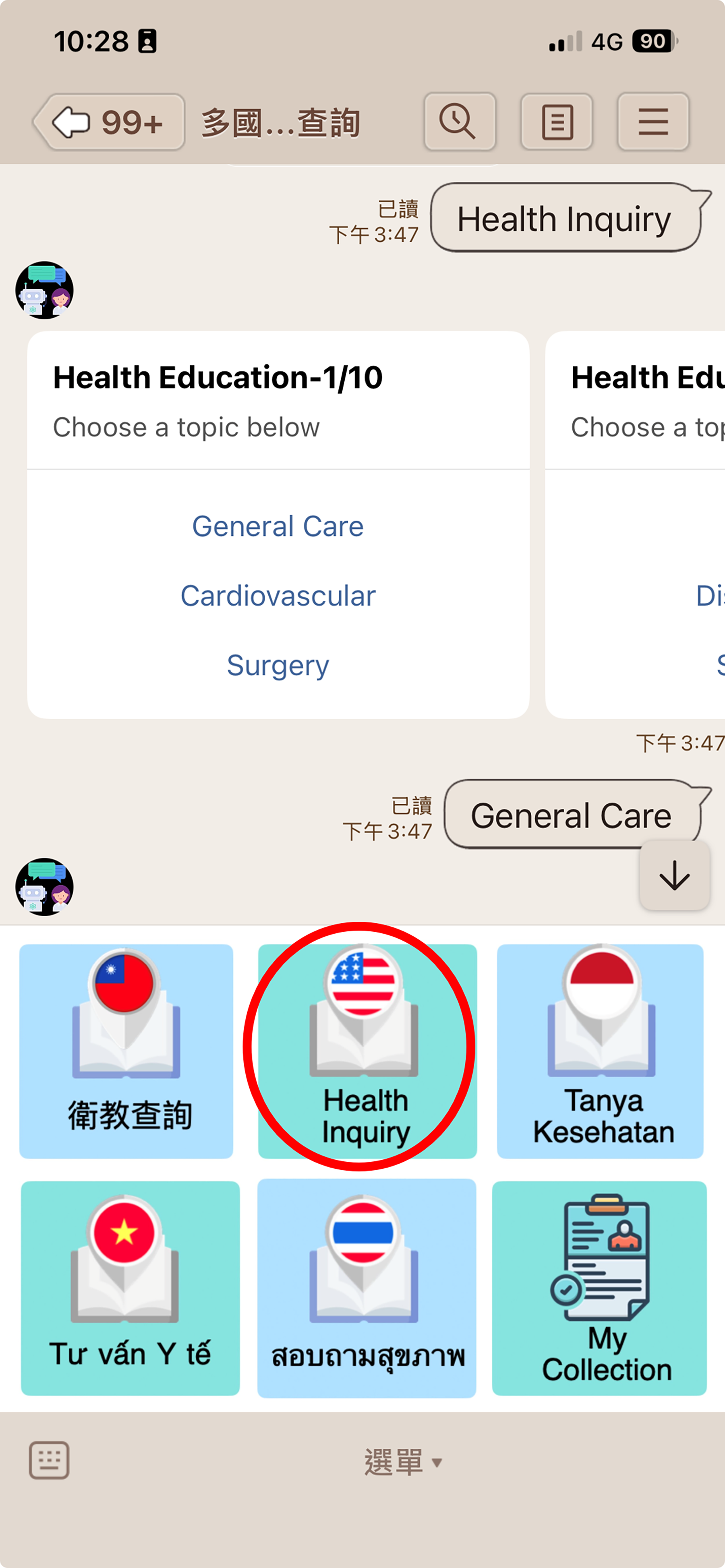
To effectively evaluate the usability and user acceptance of the proposed LINE chatbot system, this study employed three widely adopted evaluation instruments: (1) the System Usability Scale (SUS),
21
(2) the Net Promoter Score (NPS),
22
and (3) Customer Satisfaction Score (CSAT) questions.
23
Brooke (1995) introduced the SUS,
21
a standardized questionnaire (see Fig. A2) used to assess information system usability.24–26 The complete SUS questionnaire used in this study is provided in Appendix 2. Among the 10 items, 5 are positively worded, while the remaining 5 are negatively worded. The overall SUS score ranges from 0 to 100 and is calculated by aggregating the adjusted scores of all questionnaire items. The calculation formula is presented as follows:

The NPS question in this study was designed to assess users’ overall perception of the system and was phrased as follows: “How likely are you to recommend this application (APP) to your friends or colleagues?” Responses were recorded on a 10-point scale, ranging from 0 (not at all likely) to 10 (extremely likely). Based on their ratings, respondents were classified into three standard NPS categories:
Promoters (scores 9 and 10): highly satisfied and loyal users who are likely to continue using the system and actively recommend it to others. Passives (scores 7 and 8): generally satisfied users who, however, lack strong loyalty and enthusiasm. Detractors (scores 0–6): dissatisfied users who are unlikely to reuse the system and may discourage others from adopting it.
These classifications were subsequently used to compute the overall NPS value for evaluating user acceptance and recommendation intention.
The CSAT question in this study was formulated as: “Overall, how satisfied are you with this application (APP)?” Responses were recorded using a 5-point Likert scale, as follows: Very dissatisfied, Dissatisfied, Neutral, Satisfied, and Very satisfied. The CSAT metric was subsequently used to evaluate users’ overall satisfaction with the proposed system.
System evaluation was conducted between November and December 2024. During this period, the research team visited Indonesian migrant community associations and Southeast Asian migrant associations in Taiwan. With the assistance of these organizations, participants were invited to interact with the proposed system and complete the SUS questionnaire. In addition, international students enrolled at Wenzao Ursuline University of Languages were recruited to participate in the evaluation in order to further enhance the diversity of the study sample.
A total of 85 valid questionnaires were collected. The nationality distribution of respondents was as follows: 20 Indonesian, 25 Vietnamese, 7 Thai, 22 Taiwanese, and 11 participants from other nationalities. This heterogeneous sample enabled a comprehensive assessment of system usability across users with different linguistic and cultural backgrounds. The system achieved an overall SUS score of 69.53, which falls within the “Good” usability range according to the standard SUS classification (see Table 1), 27 indicating that users were generally able to interact with the system effectively with minimal usability barriers. The average NPS score was 7.18, indicating that users were generally satisfied with the system, although their level of loyalty and enthusiasm remained moderate. In addition, the CSAT score reached 3.61, demonstrating a good level of satisfaction among the 85 initial system users in terms of usability, language clarity, and functional reliability.
Rating table with System Usability Scale score
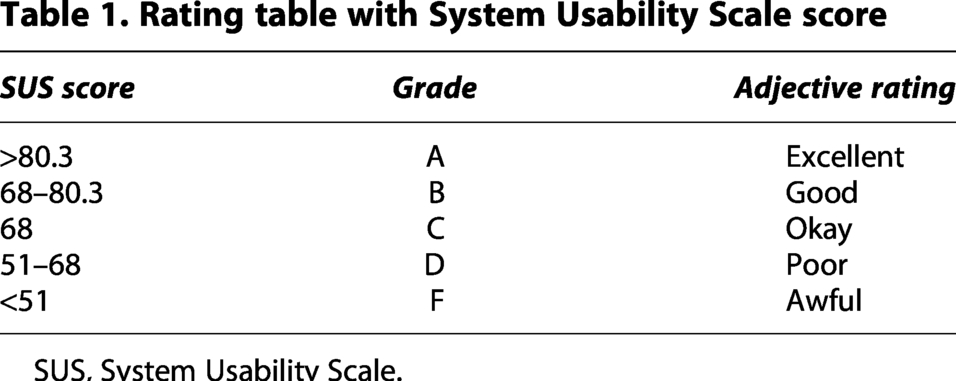
SUS, System Usability Scale.
Although the evaluation included participants from diverse linguistic and cultural backgrounds, several methodological considerations should be acknowledged. Participants were primarily recruited through migrant community associations and university student groups, which may introduce potential sampling bias and may not fully represent the broader population of health care users. In addition, the sample size of 85 participants, while sufficient for an initial usability assessment, may limit the generalizability of the findings. Future studies involving larger and more diverse clinical populations across multiple health care institutions would further strengthen the external validity of the evaluation results.
Discussion
Cross-cultural usability of multilingual health chatbots
The evaluation results indicate that the proposed multilingual chatbot demonstrates satisfactory usability and user acceptance across culturally and linguistically diverse user groups. The overall SUS score of 69.53, categorized as “Good,” suggests that users from different national and language backgrounds were able to interact with the system effectively without requiring extensive learning effort. The heterogeneous composition of the participant sample—including Indonesian, Vietnamese, Thai, Taiwanese, and other nationalities—provides empirical support for the system’s cross-cultural applicability. Notably, migrant users, who often face language and communication barriers in health care environments, reported improved comprehension of health education content and increased confidence in independently accessing medical information. These findings are consistent with prior research, emphasizing the importance of culturally adaptive interfaces in enhancing health care accessibility for minority populations.
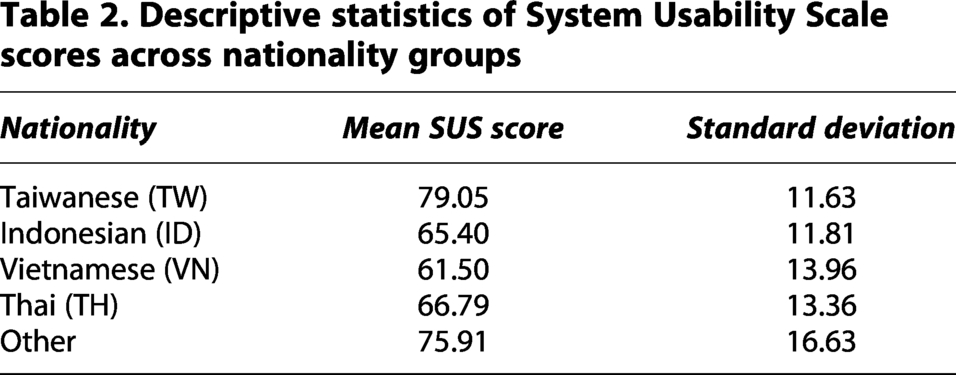
A descriptive comparison across nationality groups (see Table 2) further reveals generally consistent usability outcomes, with mean SUS scores (±standard deviation) of Taiwanese 79.05 ± 11.63, Indonesian 65.40 ± 11.81, Vietnamese 61.50 ± 13.96, Thai 66.79 ± 13.36, and other nationalities 75.91 ± 16.63. While minor variations were observed, these differences are likely attributable to variations in digital literacy and prior experience with chatbot technologies rather than language-related barriers. No substantial differences in usability trends were identified across groups, suggesting that the proposed multilingual design effectively supports cross-cultural interaction. However, future studies with larger subgroup sample sizes are warranted to enable more rigorous statistical comparisons and to further validate these findings.
Descriptive statistics of System Usability Scale scores across nationality groups
Implications and practices for multilingual system design
The findings of this study offer several important implications for the design of multilingual health care chatbots. First, effective multilingual support requires not only accurate translation but also robust language state management to ensure consistent and context-appropriate responses. The proposed multilayered logical structure by user-state successfully reduced logical complexity and response latency, demonstrating a practical solution for scalable multilingual deployment. Second, the integration of supervised learning with expert-curated multilingual health education content proved essential for maintaining clinical accuracy and linguistic reliability. Unlike fully generative approaches, this design balances system safety with conversational flexibility, which is particularly critical in health care applications. Third, user feedback revealed that features such as personal collections of health education units and PDF-based content visualization enhanced usability and information retention. These design elements support self-directed learning and align with the needs of users with varying levels of digital literacy. Overall, this study underscores the importance of combining technical optimization, linguistic expertise, and human-centered design principles when developing multilingual health care information systems. Such systems have significant potential to reduce health information disparities and improve equitable access to health care services for migrant and multicultural populations.
In addition to improving multilingual access to health education information, the proposed chatbot is designed to complement existing clinical workflows. The system primarily supports post-consultation health education, allowing patients to review treatment instructions and health education materials in their preferred language after interacting with health care providers. In this role, the chatbot functions as a digital extension of clinical communication, reinforcing information provided during consultations and helping patients better understand medical instructions. The system may also support pre-consultation information access, enabling patients to explore basic health education topics and prepare questions prior to clinical visits. By providing on-demand multilingual health education resources, the chatbot helps reduce repetitive explanations by health care providers while improving patients’ comprehension and self-management capabilities.
To further illustrate the practical use of the proposed system, several representative user interaction scenarios can be identified. In a typical post-consultation scenario, a patient who has received medical instructions from a health care provider can use the chatbot to review health education materials in their preferred language, thereby reinforcing understanding and supporting self-care. In a pre-consultation scenario, users may access general health education information to better understand symptoms or prepare relevant questions prior to visiting a clinician. Additionally, when predefined menu options do not fully address user needs, the system enables free-text interaction through the conversational AI module, allowing users to obtain supplementary information in a more flexible manner. These cases demonstrate how the chatbot facilitates accessible, multilingual health education and supports patient engagement in everyday clinical contexts.
Broader applicability of the proposed architecture
Although the proposed system was developed and evaluated within the Taiwanese health care context, its architecture is inherently scalable and transferable to other health care environments. The modular design allows adaptation to different institutions by replacing or extending the domain-specific knowledge base with locally curated medical content and guidelines. In addition, the multilingual framework can be extended to support additional languages through targeted linguistic annotation and collaboration with domain experts. Cultural adaptability can also be achieved by incorporating localized health education materials and culturally appropriate communication styles. These characteristics suggest that the proposed system has strong potential for international deployment in diverse health care settings, particularly in regions with multilingual populations and similar communication challenges.
Conclusion
The findings of this study provide clear and robust evidence that multilingual chatbot systems can play a critical role in improving health care communication and the effectiveness of health education delivery, particularly in linguistically and culturally diverse clinical settings. By automating routine health education inquiries and delivering timely, language-appropriate responses, the proposed system contributes to a measurable reduction in clinicians’ workload while enhancing patients’ understanding of medical information and post-treatment care. The evaluation results further demonstrate satisfactory system usability and user acceptance across heterogeneous user groups, including migrant populations and international users.
From a system design perspective, this study identifies and addresses key technical challenges inherent in multilingual health care chatbots, notably the substantial effort required for multilingual linguistic data preparation and constraints imposed by messaging platforms. The adoption of modular knowledge deployment combined with web-based content delivery mechanisms provides a practical, scalable, and effective solution to these challenges, enabling the system to maintain both responsiveness and informational richness without compromising usability.
Beyond its immediate technical contributions, this research highlights the broader potential of multilingual conversational agents to advance digital health equity and promote inclusive access to health care information, particularly for migrant and minority populations who face persistent language barriers. The proposed architecture offers a transferable and sustainable model for health care institutions seeking to deploy human-centered, multilingual digital health solutions in real-world clinical environments.
Future work will focus on expanding language coverage, integrating hybrid learning approaches to enhance conversational adaptability, and conducting longitudinal studies to evaluate long-term impacts on patient adherence, health outcomes, and health care resource utilization.
Limitations
Despite the promising results of this study, several limitations should be acknowledged.
First, although the system supports five major languages frequently used by migrant workers in Taiwan, the linguistic coverage remains limited. Users speaking less common languages or dialects may still experience barriers when accessing the system. Expanding language support requires additional domain experts and substantial linguistic annotation efforts.
Second, the chatbot currently relies primarily on supervised learning with expert-labeled data. While this approach ensures high accuracy and clinical reliability, it also entails considerable manual labor and maintenance costs. The continuous refinement of the knowledge base is therefore dependent on the sustained involvement of medical professionals and linguistic specialists.
Third, the evaluation was conducted within selected hospital environments and among specific user populations. Although the sample size of 85 participants produced stable results, broader deployment across diverse health care institutions and regions would further strengthen the generalizability of the findings.
Last, platform constraints imposed by the LINE messaging interface—particularly message length limitations—necessitated the use of external web-based health education resources. While this workaround improved content readability, it introduced additional interaction steps that may affect user experience.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Professor Chao-Hung Kuo of Kaohsiung Medical University and Dr. Chun-Hung Chen for their administrative support within the KMSH. They also extend their appreciation to Professor Wen-Bin Lin of the Department of Southeast Asian Studies at Wenzao Ursuline University of Languages for providing linguistic resources for Southeast Asian language translation and to Professor Shiueng-Bien Yang of the Department of Digital Content Application and Management for his valuable academic writing guidance. This research was made possible through the support and contributions of these four distinguished experts.
System Enhancement and Future Work
To enhance both reliability and conversational flexibility, the proposed system adopts a hybrid architecture that integrates menu-based knowledge delivery with generative AI assistance. The menu-based modules provide structured access to curated health education content derived from official hospital resources, ensuring the accuracy and consistency of medical information. When users are unable to locate appropriate information through predefined menu options, the system activates a generative AI module (ChatGPT) to support natural language queries. This hybrid design enables the system to maintain the reliability of expert-validated health education materials while offering flexible conversational interaction for diverse user needs in multilingual environments.
Based on feedback collected from the questionnaire survey, a considerable number of respondents suggested that the system incorporate state-of-the-art conversational AI technologies (e.g., ChatGPT and Gemini) to further enhance interaction quality and system responsiveness. While the original menu-based design effectively supported structured health education queries, users expressed a clear need for more flexible and natural conversational interactions when predefined options were insufficient.
In response to these recommendations, OpenAI’s ChatGPT 5.2 was integrated into the system as an auxiliary conversational module. When users are unable to locate appropriate health education information within the existing menu-based units, the system automatically redirects them to a ChatGPT-powered conversational interface, enabling free-text health inquiries and context-aware responses. This AI-driven conversational mechanism complements the supervised, menu-based health education framework and significantly enhances the system’s conversational capability and user experience.
At present, ChatGPT 5.2 has been successfully incorporated into the system’s service functions, supporting conversational-style health education queries. An example of the conversational interaction interface and system operation is illustrated in ![]() . This hybrid architecture represents an important direction for future system development, offering a scalable pathway for integrating generative AI technologies into multilingual health care chatbots while maintaining clinical reliability and usability.
. This hybrid architecture represents an important direction for future system development, offering a scalable pathway for integrating generative AI technologies into multilingual health care chatbots while maintaining clinical reliability and usability.
Future research will focus on extending the system in several directions. First, additional language support will be incorporated to serve a broader range of migrant communities and international patients. Semiautomated annotation techniques and transfer learning approaches will be explored to reduce the cost of multilingual data expansion. Second, hybrid learning strategies that integrate supervised learning with reinforcement learning and large language models will be investigated to enhance conversational adaptability while preserving clinical accuracy. Third, tighter integration with hospital information systems and electronic medical records will be developed to enable personalized, context-aware health education tailored to individual treatment plans and patient histories. Last, large-scale longitudinal studies will be conducted to evaluate the long-term impact of the chatbot on patient adherence, health outcomes, and health care resource utilization.
Ethical Considerations
Given the sensitive nature of health care information, ethical and safety considerations were integrated into the system design. The generative AI component is implemented as a supportive health information assistant, with responses limited to general health education and not intended to replace professional medical advice. A hybrid architecture ensures that expert-curated, menu-based content remains the primary information source, while generative AI is activated only when necessary. All health education materials were derived from the official website of KMSH, 17 and user data are anonymized in compliance with data protection principles. This layered approach balances conversational flexibility with clinical safety in real-world health care applications.
Authors’ Contributions
Tai-Liang Chen contributed to the study conception and design, system architecture development, chatbot implementation, data collection, usability evaluation, data analysis, and manuscript drafting. Yi-Hui Liu contributed to the research design, healthcare application framework, interpretation of findings, manuscript review, and academic revision. Both authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this article, the authors used ChatGPT 5.2 to assist with English language editing and grammar refinement. All generated content was carefully reviewed and revised by the authors, who take full responsibility for the accuracy and integrity of the final published work.
Author Disclosure Statement
The authors declare that they have no financial or non-financial conflicts of interest related to this study. The development, evaluation, and reporting of the multilingual medical health education chatbot were conducted independently, and no commercial entity influenced the study design, data analysis, or manuscript preparation.
Funding Information
This research is partially sponsored by the
Abbreviations Used
Appendix
Appendix I Multilingual system interface and functions
Appendix II SUS questionnaire