
Abstract
Using a four-wave longitudinal sample of young Canadian adults (18–24), this study identified five latent trajectory classes: low stable, high stable, high decreasing, moderate decreasing, and low increasing. The identification of a class characterized by an increasing trajectory of depression symptoms across the transition to adulthood is a novel finding. Of the risk and protective factors assessed, only initial student status and perceived family support helped prospectively distinguish between trajectory classes—students with higher depression symptomology in late adolescence are at increased risk for depression across the transition to adulthood, while perceived family social support in late adolescence is a protective factor associated with reduced probability of being in more symptomatic depression trajectories. Although limitations related to sample size warrant due caution, the findings still have diagnostic, prevention, and treatment implications related to the prospective differentiation of diverging depression symptom trajectories (i.e., multifinality) in the transition to adulthood.
The transition from late adolescence into young adulthood, or emerging adulthood, is a critical developmental period accompanied by multiple changes in roles, expectations, and responsibilities (Arnett, 2000). How well a person manages such major life transitions can have important consequences for their mental health and well-being (Schulenberg & Maggs, 2002). Mental health can be conceptualized, in part, as a function of how well a person is able to adjust to various transitions and changing contexts and life circumstances (Masten & Coatsworth, 1995). A developmental psychopathological perspective—that focuses on the links between life transitions and health risk—views emerging adulthood as a seminal period for psychosocial adjustment that can affect the subsequent course of mental health and psychopathology across adulthood (Schulenberg, Sameroff, & Cicchetti, 2004; Schulenberg & Zarrett, 2006).
As a major life transition accompanied by more extensive individual and contextual change than any other phase of life, emerging adulthood presents both great opportunity and challenge for young people faced with decreasing institutional constraints and increasing choice and self-direction. This burgeoning autonomy can produce enhanced person-context alignment and mental health for some and overwhelming psychosocial disruption for others (Schulenberg & Zarrett, 2006). Accordingly, at the general population level, emerging adulthood is characterized by increases in both mean mental health and psychopathology, with the incidence of depression rising across ages 15–22 (Kessler & Walters, 1998). Schulenberg and Zarrett (2006) note that such mean-level trends mask the increasing heterogeneity in life courses deriving from mounting contextual and role transitions in emerging adulthood and that the seemingly contradictory rise in both general mental health and the incidence of depression is in part due to such increased heterogeneity. They observe that such transitions can act alternately as agents of both continuity and discontinuity. Accordingly, the rise in depressive disorders over this period may, for some individuals, reflect decreases in structure or support or in person-context alignment that overwhelm coping capacities and exacerbate continuing psychosocial adaptive vulnerabilities, while for others, it may reflect novel developmental disturbances or negative turning points. Entering postsecondary education is an example one of these transitions during which the compounding of multiple developmental and contextual changes can cause disruptive shifts in roles and expectations, heightened distress, and increased vulnerability to disordered mental health (Adlaf, Gliksman, Demers, & Newton-Taylor, 2001; Conley, Kirsch, Dickson, & Bryant, 2014).
Trajectories of Depression
Although the general course of depression is characterized by increases in early adolescence /mid-adolescence and decreases across early adulthood (Galambos, Barker, & Krahn, 2006; Ge, Lorenz, Conger, Elder, & Simons, 1994; Ge, Natsuaki, & Conger, 2006; Hankin et al., 1998; Kim, Capaldi, & Stoolmiller, 2003; Natsuaki, Biehl, & Ge, 2009; Pettit, Lewinsohn, Seeley, Roberts, & Yaroslavsky, 2010), as noted above, courses can vary in terms of continuity and discontinuity, describing various trajectories, with considerable evidence that mental health difficulties (e.g., depression) in this period may continue to have repercussions into adulthood (Hankin, 2017; Rao, Hammen, & Daley, 1999; Rao et al., 1995; Reinherz, Giaconia, Hauf, Wasserman, & Silverman, 1999; Schulenberg & Zarrett, 2006).
A number of recent studies have looked at heterogeneity in depression trajectories in adolescence (Brendgen, Wanner, Morin, & Vitaro, 2005; Brière, Janosz, Fallu, & Morizot, 2015; Repetto, Caldwell, & Zimmerman, 2005; Rodriguez, Moss, & Audrain-McGovern, 2005). Chaiton et al. (2013) identified three trajectories across the Grades 7–11 time period. Dekker et al. (2007) identified six trajectory classes from childhood into late adolescence. Wickrama, Wickrama, and Lott (2009) specified four theoretically derived youth depressive symptom trajectory groups: “chronically high,” “consistently low,” “increasing,” and “decreasing,” which they empirically confirmed with latent class analysis (Wickrama & Wickrama, 2010).
While Wickrama’s two studies (Wickrama & Wickrama, 2010; Wickrama, Wickrama, & Lott, 2009) tracked trajectories across adolescence until the age of 19, few studies have tracked trajectories across late adolescence into emerging adulthood. For example, Yaroslavsky, Pettit, Lewinsohn, Seeley, and Roberts (2013) tracked trajectories of depressive symptoms from mid-adolescence (14–18) to age 30. They found three trajectory classes: “high stable” (32%), “moderate decreasing” (44%), and “low decreasing” (24%). Stoolmiller, Kim, and Capaldi (2005) examined trajectories in young men (age 15–24) and identified four depressive symptom classes: “very low” (6%), “moderate decreasing” (34%), “high decreasing” (36%), and “high persistent” (24%). Ferro, Gorter, and Boyle (2015) traced trajectories over 14 years (age 10–25) and found three distinct classes, which they labeled “minimal” (55%), “subclinical” (39%), and “clinical” (6%).
Risk and Protective Factors
Of additional importance to the identification of multiple distinct depression trajectories is the capacity to predict membership in trajectory classes. There is still a gap in our ability to identify risk and/or protective factors that help prospectively distinguish between worsening, stable, and improving trajectories or between diverging (similar starting points but splitting over time—multifinality) and converging (different starting points that lead to similar end points—equifinality) trajectories (Cicchetti & Rogosch, 1996). Identifying trajectory-specific risk and protective factors may help improve our understanding of the etiology and course of depression and help clinicians more effectively tailor their treatment and prevention efforts (Yaroslavsky, Pettit, Lewinsohn, Seeley, & Roberts, 2013).
There is substantial evidence in the literature underscoring a number of risk and protective factors for depression in youth. The developmental psychopathology framework guiding this study highlights the importance of understanding what factors influence patterns of adjustment and maladjustment over the life course. This perspective views maladaptive outcomes, including psychopathology, as primarily consequences of developmental processes (Sroufe, 1997). Stages of development unfold successively, with competencies and capabilities building upon previous adaptations, such that developmental difficulties or disruptions in previous periods can carry forward and affect how individuals handle developmental tasks and transitions in subsequent periods (McLaughlin, Michl, and Herts, 2013). As noted earlier, the transition from adolescence to adulthood is a key developmental period of potentially taxing psychosocial adjustments characterized variously by continuity, discontinuity, and critical turning points. The emerging adult’s ability to adapt to these new opportunities and demands is influenced by previous development and has developmental consequences further into adulthood. Although developmental patterns of psychosocial adaptation and maladaptation, and consequent psychopathology such as depression, are also influenced by neurobiological and contextual factors, this study will limit its focus to a subset of personality, coping, and sociodemographic factors associated with psychosocial adjustment. 1
In terms of personality and/or psychological factors, neuroticism (Kotov, Gamez, Schmidt, & Watson, 2010; Rhebergen et al., 2011; Rhebergen et al., 2012; Robinson, Shankman, & McFarland, 2009; Wiersma et al., 2011) has been associated with greater risk of depression, while extroversion (Kotov et al., 2010; Rhebergen et al., 2012; Robinson et al., 2009; Wiersma et al., 2011) and self-esteem (Pelkonen, Marttunen, & Aro, 2003; Rawana & Morgan, 2014; Rieger, Gollner, Tautwein, & Roberts, 2016; Wickrama, Noh, & Elder, 2009) have both been negatively associated with risk of depression. How one copes with stress and change has important implications for psychosocial adaptation, given the multiple transitions confronting emerging adults. Negative coping strategies such as escape–avoidance have been associated with greater risk of depression (Evans et al., 2015; Hermann-Stahl, Stemmler, & Petersen, 1995; Ireland, Boustead, & Ireland, 2005; Seiffge-Krenke & Klessinger, 2000; Wadsworth & Compass, 2002), while positive coping strategies such as planful problem-solving have been associated with reduced risk of depression (Evans et al., 2015; Ng & Hurry, 2011; Seiffge-Krenke & Klessinger, 2000; Van Voorhees et al., 2008). Social and demographic factors that have been associated with depression include social support, gender, and being a college student. Females are generally at higher risk than males for depression (Abela & Hankin, 2008; Galambos, Leadbeater, & Barker, 2004; Hyde, Mezulis, & Abramson, 2008; Nolen-Hoeksema, Larson, & Grayson, 1999; Rawana & Morgan, 2014; Zarate, 2010). College, as a time of multiple transitions and adjustments (Conley et al., 2014), is also associated with increased psychosocial vulnerability, including risk of depression (Adlaf et al., 2001; Bayram & Bilgel, 2008). There is also evidence that social support, especially important in such transitional periods, is negatively associated with risk of depression (Barth, Hofmann, & Schori, 2014; Colman et al., 2014; Khatib, Bhui, & Stansfeld, 2013; McDougall et al., 2016; Rueger, Malecki, Pyun, Aycock, & Coyle, 2016). Finally, it is well-documented that substance use disorders such as alcohol dependence—which tend to be more acute in emerging adulthood (Sussman & Arnett, 2014)—are also associated with increased risk of depression (Afifi, Enns, Cox, & Martens, 2005; Swendsen et al., 1998).
The Current Study
Although a growing number of studies have sought to examine heterogeneity in depression trajectories across the youth to adulthood transition, there is still uncertainty regarding the number, shape, and magnitude of trajectories as well as regarding reliable predictors of differing trajectories. Additionally, we are only aware of one previous study that examines heterogeneity in depression trajectories in a Canadian sample of emerging adults. Ferro et al. (2015) found three trajectories of depression symptoms (clinical, subclinical, and minimal)—none of which trended upward or downward over time, suggesting few individuals change risk levels across emerging adulthood. The current study seeks to further understand all three of these points.
This exploratory study undertakes a secondary data analysis of a four-wave longitudinal survey data set. It uses latent class growth analysis to (a) enumerate multiple distinct trajectories of depression symptoms in a Canadian sample of emerging adults and (b) assess the usefulness of a number of documented risk and/or protective factors for depression as predictors of latent class membership. Based on previous studies of multiple trajectories of depression symptoms across the late adolescence to adulthood transition, we expect that three or four trajectories will be evident, reflecting high, moderate, and low levels of depression and persistent or decreasing trajectories. Furthermore, we expect the previously identified depression risk factors (neuroticism, escape–avoidance coping, alcohol dependence, being female, and a college student) to be predictive of membership in more symptomatic trajectories and the protective factors (extroversion, self-esteem, problem-solving coping, and social support) to be predictive of less symptomatic trajectory class membership.
There are two important ways this study differs from Ferro et al. (2015). First, they used control variables when they enumerated trajectory classes, which means the trajectory classes are conditional on the particular set of variables used. The current study will model unconditional trajectory classes, which are unaffected by the particular set of variables used. Second, Ferro et al. used pairwise contrasts to compare the different classes on mean levels of the control variables, whereas the current study will use multinomial logistic regression to identify which predictors affect the probability of membership in the identified classes.
Method
Data and Measures
The study is a secondary data analysis of the Manitoba Longitudinal Study of Young Adults (MLSYA), 2 which was conducted in four cycles from December 2007 through December 2011. All four waves consisted of a survey (self-report questionnaire) that was administered by phone and a second survey done by either paper mail-out or online (chosen by the respondent). Respondents were first recruited either as part of a convenience sample of young gamblers in casinos or via random digit dialing. From the sample of convenience and random subjects, additional respondents were added through a snowball sample where referrals of new respondents were made by existing participants in exchange for US$5 gift cards (maximum US$5 per individual referrer). Retention rates for Cycles 2–4 were 91.90% (624 participants), 85.12% (578 participants), and 78.06% (530 participants), respectively. Key demographic characteristics of the original sample are reported in Table 1. All measures used in the study are from previously validated instruments administered as part of the MLSYA study.
Baseline Demographic Characteristics of the Manitoba Longitudinal Study of Young Adults Sample.
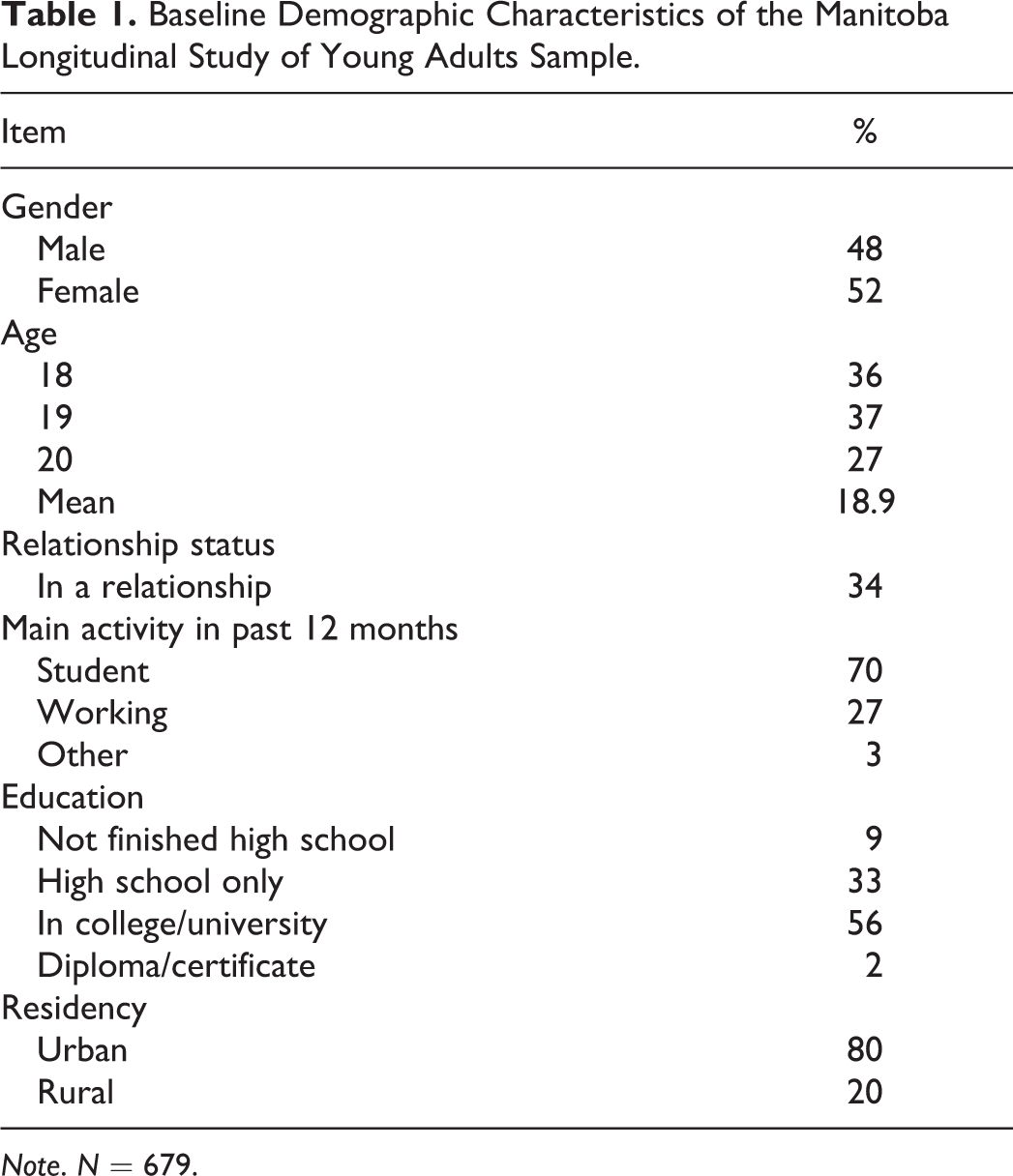
Note. N = 679.
Dependent variable
Section A of the Composite International Diagnostic Interview–Short Form (CIDI-SF; Walters, Kessler, Nelson, & Mroczek, 2002) determines probability of caseness for diagnosis of major depression based on the full CIDI instrument. Scores range from 0 to 7, with higher scores indicating greater probability of caseness for major depression. The CIDI-SF is psychometrically sound, with strong test–retest reliability (kappa = .95) and adequate interrater reliability (kappa = .71; Wittchen, 1994). Additionally, 89.6% of major depressive episodes were correctly identified using the CIDI-SF, compared with its longer version (Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998).
Baseline Predictor Variables
Alcohol dependence
The Alcohol Dependence Scale was adapted with some modification from the Canadian Community Health Survey and the National Comorbidity Survey and is based on the CIDI-SF and DSM-III-R classification (Kessler et al., 1998; Statistics Canada, 2003) and was designed to measure Criteria A and B of the DSM-III-R diagnosis for psychoactive Substance Use Disorder (SUD) (Nelson, Kessler, & Mroczek, 2001). Possible scores range from 0 to 9, where higher scores correspond with a higher likelihood of alcohol dependence. Scores ≥3 indicate a probable diagnosis of alcohol dependence and were coded as 1, those below 3 were coded as 0.
Coping styles
The 8-Item Escape–Avoidance (range of scores = 0–24, α = .80) and the 6-Item Planful Problem-Solving (range of scores = 0–18, α = .75) subscales of the Ways of Coping Questionnaire (Folkman & Lazarus, 1980, 1988) were used. Raw scores for each subscale are calculated by simple summation of responses to four-category Likert-type items.
Neuroticism and extroversion
Neuroticism and extroversion are measured using the neuroticism (α = .91) and extroversion (α = .87) factor scores from the NEO Five Factor Inventory (Costa & McCrae, 1992). Factor scores for each domain are calculated from 12 Likert-type scale questionnaire items scored from 0 = strongly disagree to 4 = strongly agree (or vice versa in the case of reverse-coded questions). Possible factor scores range from 0 to 48 with higher values indicating a more pronounced disposition toward that personality trait.
Family social support
Family social support is measured by the 4-Item Family (α = .85) subscale of the Multidimensional Scale of Perceived Social Support (Zimet, Dahlem, Zimet, & Farley, 1988). Questions are scored on a 7-point Likert-type scale ranging from 1 (very strongly disagree) to 7 (very strongly agree), total scores range from 4 to 28 for each subscale, with higher scores indicating higher perceived support.
Self-esteem
The Rosenberg Self-Esteem Scale (Rosenberg, 1965; α = .89) asks respondents whether they strongly disagree, disagree, agree, or strongly agree with 10 statements that are scored from 0 to 3, respectively. Possible scores range from 0 to 30 with higher scores indicating higher levels of self-esteem. Five negatively framed items (i.e., I feel I do not have much to be proud of) were reverse-coded, so that the sums of all questions could be tallied.
Missing Data
Maximum likelihood estimation assumes that missing data are missing at random (MAR). We cannot test the MAR assumption and so cannot completely rule out that data are missing not at random (MNAR), but there are ways to strengthen the plausibility of the MAR assumption. One way to help address this concern is to use multiple imputation with missing data correlates (or auxiliary variables) added to the multiple imputation model to help better account for missingness, thus making the MAR assumption more plausible and reducing bias in estimates (Collins, Schafer, & Kam, 2001; Enders, 2010; Graham, 2003; Schafer, 2003).
Accordingly, a dichotomous “dropout” variable was created to compare cases that had data for all four waves (code = 0) to those cases that dropped out (code = 1). Student t tests indicated that dropouts reported higher baseline levels of depression, impulsivity (measured by the Barratt Impulsiveness Scale; Patton, Stanford, & Barratt, 1995), and problem gambling (measured by the Problem Gambling Severity Index; Wynne, 2003). 3 Hence, both impulsivity and problem gambling were included, as correlates of missingness in the multiple imputation model (Enders, 2010) used to generate 20 data sets in Mplus Version 7.1.
Analysis
Instead of estimating a single mean trajectory, latent class growth modeling allows the estimation of two or more latent classes, each with a distinct mean trajectory. The first step is to enumerate the optimal number of trajectory classes. For example, does a two-latent-class model fit better than the single-class model? Does a three-class model improve fit over a two-class model? Once the best unconditional multiple trajectory class model was determined, then the R3Step procedure in Mplus was used to regress the unconditional classes on predictors (e.g., gender, family social support, neuroticism), and the contribution of these predictors to the probability of an individual being in one class or another was calculated in the form of log odds.
Model fit was assessed based on the Bayesian information criterion (BIC) statistic, 4 and the entropy value, as well as the interpretability and theoretical plausibility of the latent classes. Lower BIC numbers indicate a better fitting model, while entropy values above .80 indicate that individuals are classified with accuracy and that latent classes are adequately distinct (Greenbaum, Del Boca, Darkes, Wang, & Goldman, 2005; Muthén, 2004).
Results
Determining the Number of Trajectory Classes
It was determined that a five-class linear trajectory model was the most suitable solution (Table 2). 5 The five classes (see Table 3 and Figure 1) are a normative, low-stable, class (78.4%); a high-stable class (4.4%); high-decreasing class (5.8%); moderate-decreasing class (6.5%); and a low-increasing class (4.9%). Although the six- and seven-class models had smaller BIC values (see Table 2), the five-class model was chosen due to considerations related to (a) overextraction of classes (Bauer and Preacher, 2003) and (b) greater alignment with theoretically and empirically derived trajectory classes in previous studies of depression symptoms.
Model Fit and Quality of Classification.
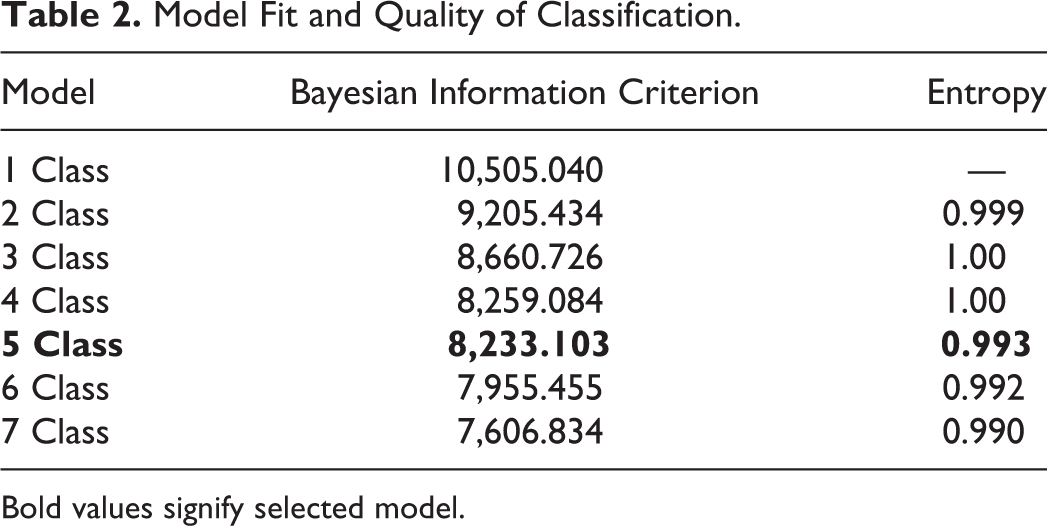
Bold values signify selected model.
Growth Parameter Estimates by Trajectory Class.
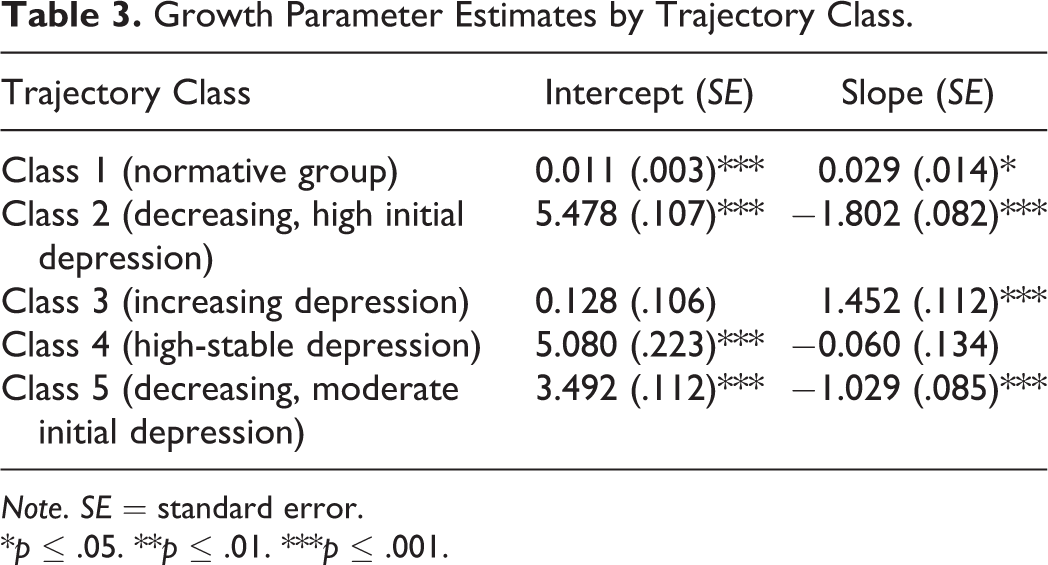
Note. SE = standard error.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
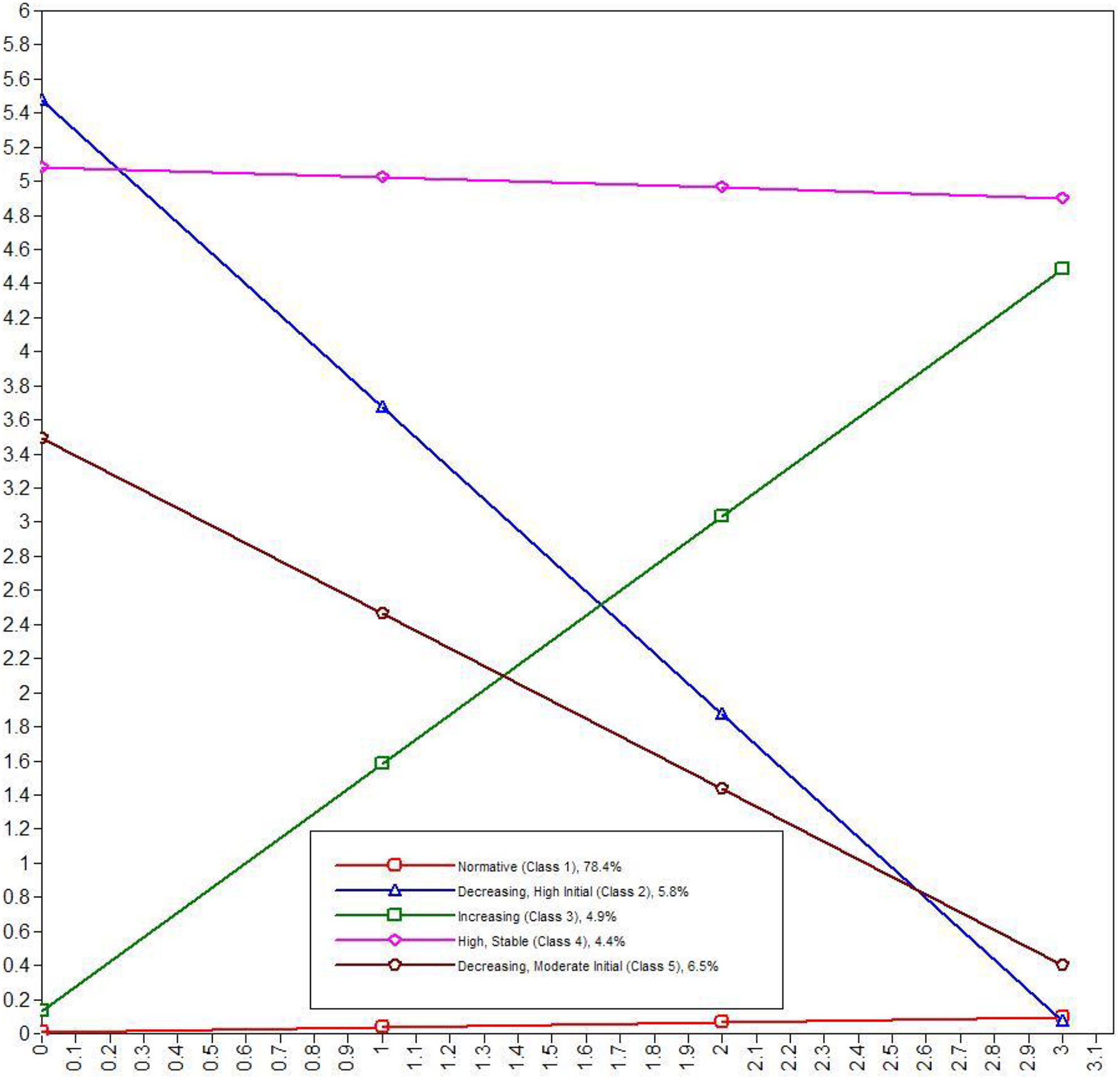
Estimated latent class trajectories for depression symptoms.
The six-class solution had two classes with less than 3% of respondents and the seven-class solution had two trajectory groups with less than 2% of the sample. Generally, classes with less than 5% of the total sample or an n smaller than 25 are not recommended unless the case for “what is gained” from their inclusion can be compellingly made (Wickrama, Lee, O’Neal, & Lorenz, 2016). Furthermore, the normative, low-stable, class remained about the same size across the different class solutions with the six- and seven-class solutions simply partitioning the remaining fifth of the sample into more, ever smaller subgroups. The diminishing size of these subgroups raises doubts about their substantive relevance as well as concerns regarding sufficient statistical power to address the second objective of this study—identifying predictors of latent class membership via multinomial regression.
The five-class model is also stronger in terms of alignment with theory and previous findings. For example, the low-stable, high-stable, and increasing trajectory groups are consistent with the first three of Wickrama’s theoretically and empirically specified trajectory groups (Wickrama et al., 2009; Wickrama & Wickrama, 2010) and the high-decreasing and moderate-decreasing groups are variations of Wickrama’s final decreasing group. Stoolmiller et al. (2005) also found a low-stable, a high-persistent, and moderate-decreasing and low-decreasing classes, but no increasing class. Yaroslavsky et al. (2013) also found a high-stable group and two decreasing groups, but no low-stable group or increasing group. Ferro et al. (2015) found high-persistent (“clinical”) and low-stable (“minimal”) trajectory classes, but no increasing or decreasing classes. Note that the five-class solution was also substantively better than the four-class solution in the current study as the latter deviated markedly from previous studies in not identifying a high-stable class (instead identifying three decreasing classes, distinguished only by different baseline levels).
Predicting Membership in Trajectory Classes
Odds ratios from the multinomial regression for the purported baseline predictors (see Table 4, for descriptive statistics) of latent trajectory class membership are reported in Table 5. Unexpectedly, the only predictors that significantly differentiated between trajectory classes were student status and perceived level of social support from family. Those who were students at baseline were 4 times more likely than nonstudents to be in the high-stable class compared to the high-decreasing class. Higher levels of perceived family social support were associated with decreased probability of being in any of the more symptomatic classes compared to being in the low depression, relatively stable normative class. Put another way, higher perceived level of family social support is associated with greater probability of being in the normative, low depression class and conversely, with decreased probability of being in the more symptomatic classes. Unfortunately, family social support did not distinguish between the more symptomatic classes (e.g., high stable vs. high decreasing).
Means (SE) of Predictors by Class and Total Sample.
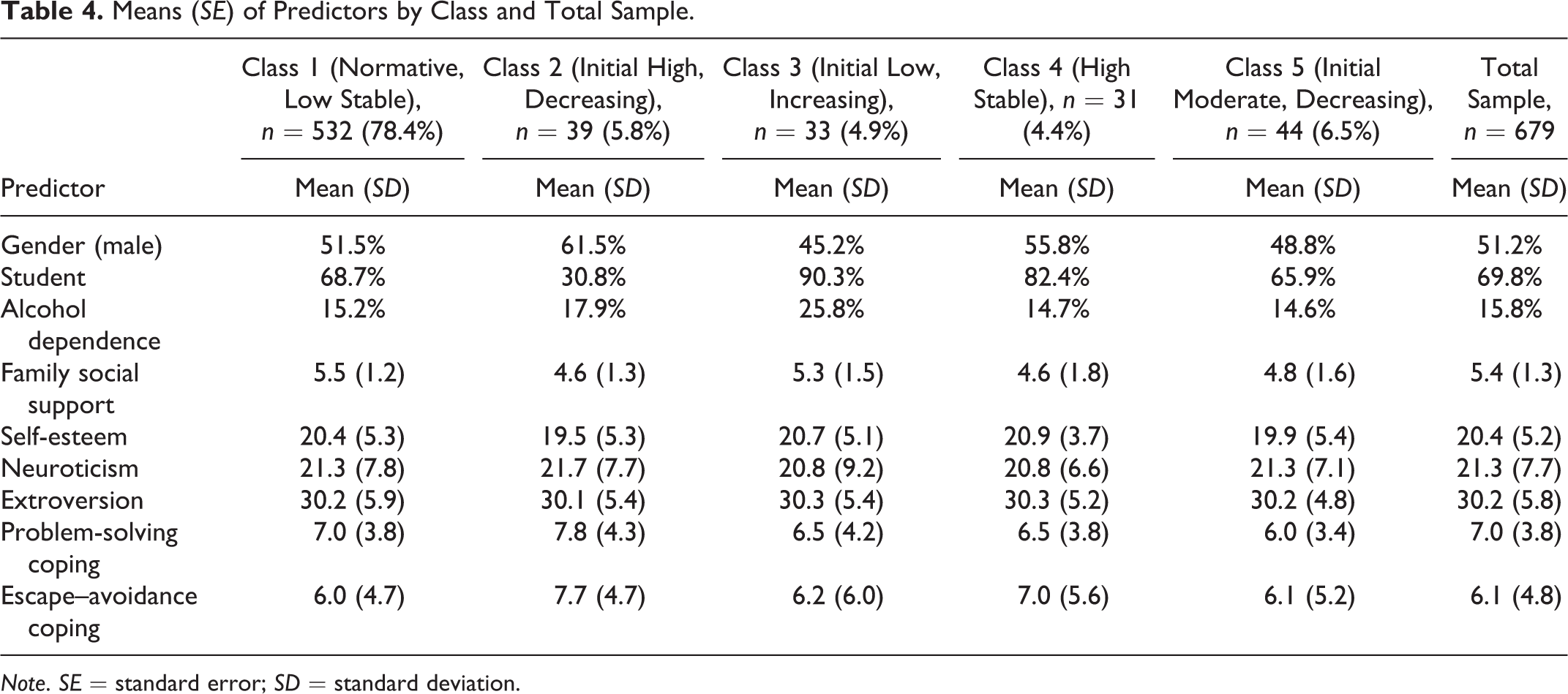
Note. SE = standard error; SD = standard deviation.
Group Comparisons on Latent Class Predictorsa—Odds Ratios (Standard Errors).
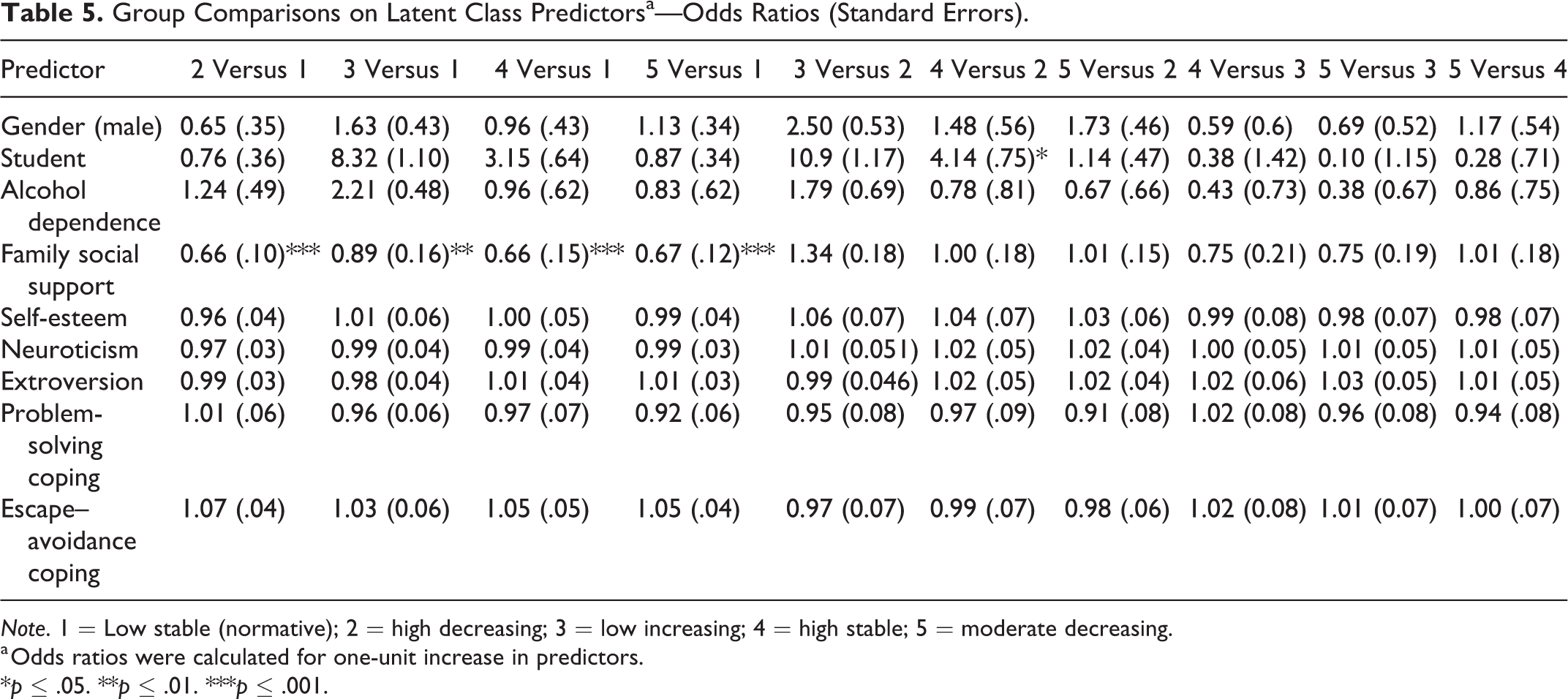
Note. 1 = Low stable (normative); 2 = high decreasing; 3 = low increasing; 4 = high stable; 5 = moderate decreasing.
a Odds ratios were calculated for one-unit increase in predictors.
*p ≤ .05. **p ≤ .01. ***p ≤ .001.
Discussion
This study identified a five-class latent trajectory model, comprised of a normative, low-stable class (78.4%); a high-stable class (4.4%); high-decreasing class (5.8%); moderate-decreasing class (6.5%); and a low-increasing class (4.9%). This solution is largely consistent with theory and previous findings. Wickrama et al. (2009) specified four theoretically derived youth depressive symptom trajectory groups: “chronically high,” “consistently low,” “increasing,” and “decreasing,” which they also subsequently empirically confirmed with Latent Class Analyses (Wickrama & Wickrama, 2010). In the present findings, the low-stable, high-stable, and increasing trajectory groups are consistent with the first three of Wickrama’s trajectory groups, while the high-decreasing and moderate-decreasing groups identified here are variations of Wickrama’s final decreasing group.
Of note, this research is only the second study that we are aware of that assessed the heterogeneity of depression symptom trajectories in a Canadian sample of emerging adults. A previous Canadian study by Ferro et al. (2015) traced trajectories over 14 years (age 10–25) and found three distinct classes, which they labeled minimal (55%), subclinical (39%), and clinical (6%). All three trajectories peaked by age 17 and were basically parallel with no significant cross-diagonal movement (differing primarily in level of symptoms but not rate of change). Present findings also found that depression symptoms peaked in late adolescence for most of the sample, but, in addition, identified one class characterized by increasing depression across the late adolescent to adulthood transition. It should be noted that although no significant nonlinear growth patterns were detected in the present study, Ferro et al. found nonlinear trajectories for all three groups, this difference may be in part due to their modeling of trajectories over seven time points compared to only four in the present study.
The identification of an increasing trajectory of depression symptoms in emerging adulthood is a novel finding. None of the previous studies we are aware of that tracked trajectories across late adolescence into early adulthood identified a group with an increasing trajectory over this period. Wickrama’s studies followed adolescents until age 19, but the present study followed individuals between ages 18 and 24, and so evidence of an increasing trajectory class across this time of emerging adulthood represents a potentially significant result that merits further study. The lack of gender differences stands in contrast to a number of previous studies (e.g., Dekker et al., 2007). While the finding that only student status and perceived level of family social support were significant predictors of latent trajectory class was disappointing and may in part have to do with the modest size of some of the trajectory groups, each with 5–6% of the sample comprised of between 31 and 41 people. It may be that with a larger sample and more statistical power, modest, but meaningful differences undetected here, would become evident. Additionally, depression tends to be episodic in nature with symptoms flaring up and subsiding over short periods of time (e.g., weeks or months), hence tracing trajectories across more time points separated by shorter intervals may provide further clarification, including enhanced ability to detect nonlinear growth curves. Further to this concern, it should be noted that each wave of data collection took place over several months and so there is bound to be some interindividual variation in the length of time in between assessments, unfortunately there is no variable in the data set to allow us to control for variation in the between wave intervals. Finally, the student status variable does not indicate whether students were in high school or postsecondary education at Time 1 (although only 9% of respondents had not finished high school at that time), a potentially important distinction given the importance of the transition college. This transition, which coincides with emerging adulthood, requires adaptation to various changes including new academic, social, and often living arrangements. It can produce, especially in the first few months, a variety of psychosocial adjustment problems including declines in psychological well-being, cognitive–affective functioning, and social well-being as well as increased distress and cognitive–emotional vulnerability (Conley et al., 2014).
Conclusion
Largely consistent with Schulenberg and Zarrett (2006) observations regarding the burgeoning heterogeneity of life courses—marked variously by continuity, discontinuity, developmental disturbances, and turning points—that underlie the seemingly contradictory increase in both mean mental health and psychopathology in emerging adulthood, there was substantial heterogeneity in depression symptom trajectories evident in the sample under study. Five trajectory classes of depression symptoms were identified; these classes were generally consistent with previous findings with the notable exception of a class characterized by an increasing trajectory of depression symptoms across the transition to adulthood. Initial student status helped distinguish between high-stable and high-decreasing trajectories, suggesting students with higher depression symptomology in late adolescence are at increased risk for depression across the transition to adulthood. This finding has implications for the important prognostic issue of multifinality (Cicchetti & Rogosch, 1996) or how to prospectively differentiate between diverging trajectories such as chronic or worsening versus acute or decreasing. The ability to distinguish between trajectories with similar starting points but different ends stands to help increase the effectiveness of diagnostic, prevention, and treatment efforts (Nolen-Hoeksema & Watkins, 2011). Finally, consistent with a number of previous studies (see Rueger et al., 2016), perceived family social support was a protective factor associated with reduced probability of being in the more symptomatic trajectories—also a finding with diagnostic implications for distinguishing initially low but increasing (adult onset) from continuing low-depression symptom trajectories in the transition to adulthood.
Footnotes
Author Contribution
Jason D. Edgerton contributed to conception, design, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Souradet Shaw contributed to conception, design, analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy. Lance W. Roberts contributed to conception and design, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.