
Abstract
Research has demonstrated the important impact of identity on psychosocial functioning in both community and clinical populations. The present article aims to identify different mechanisms through which identity may be related to psychopathology. Emphasis is placed on neo-Eriksonian identity models targeting identity mechanisms both at the structural and process levels. With respect to psychopathology, the present article focuses mainly on disturbed eating behaviors and nonsuicidal self-injury, with both behaviors sharing a focus on the body. Emerging research lines are identified, and recent research is discussed as a sample case of how developmental theorizing on identity can yield insights in the emergence and development of psychopathological behaviors. In integrating these research lines, the present article discusses emerging themes originating from the field and provides important avenues for future research and intervention efforts.
Keywords
Identity formation is commonly framed as the central developmental task of adolescence and the transition into adulthood, extending from the early teens well into the 20s (Arnett, 2000; Erikson, 1968). This process of identity formation essentially addresses the question “Who am I and where am I heading in life?” (Schwartz, Luyckx, & Vignoles, 2011). Coming up with an answer to this life-defining question not only becomes important throughout the second and third decades of life but remains so throughout the entire life span (Erikson, 1950; Kroger, 2000). A vast amount of research has demonstrated that how one addresses these identity issues is not only related to adaptation and adjustment but also to suboptimal functioning, distress, and even psychopathology (e.g., Crocetti, Luyckx, Scrignaro, & Sica, 2011; Luyckx et al., 2008; Schwartz, Beyers, et al., 2011; Wiley & Berman, 2013). These latter findings should not come as a surprise as identity research and theorizing partially emerged from clinical observations, as can be derived from Erikson’s (1950, 1968) writings. However, for identity research to reach its full potential in terms of informing clinical practice and (preventive) interventions, we still have a long way to go. A main reason for this rather unfortunate state of the field is the considerable gap between developmental and clinical literatures (Kaufman, Montgomery, & Crowell, 2014; Pasupathi, 2014). In the present article, and inspired by a developmental psychopathology framework (Kaufman et al., 2014), we try to bridge these two bodies of literature by demonstrating the added value of neo-Eriksonian identity models for our understanding of pathological behaviors in community and clinical samples.
Assessing Identity Structure and Processes
Our main inspirations for conceptualizing and measuring identity were Erikson’s (1968) identity theorizing and Marcia’s (1966) identity status paradigm. Partially inspired by Marcia’s (2006) seminal article on the link between identity and personality disorders, we commonly assess identity at different levels—covering identity structure as well as behavioral identity processes. As conceptualized by Erikson (1950, 1968), one’s identity structure is characterized by a certain degree of synthesis and confusion, and successful identity development is commonly portrayed as the extent to which synthesis predominates over confusion. Individuals scoring high on identity synthesis experience self-continuity over time and across situations and have developed a stable set of goals, plans, and beliefs (Erikson, 1968; Kaufman et al., 2014). Individuals high on identity confusion experience a fragmented sense of self and limited self-directed decision-making (Schwartz, Zamboanga, Luyckx, Meca, & Ritchie, 2013) . They struggle to find purpose and direction in their life (Schwartz, Zamboanga, Wang, & Olthuis, 2009).
Marcia (1966) developed the status paradigm and defined two key identity processes as behavioral indicators of this identity structure: exploration, or experimenting with identity alternatives and commitment, or adhering to a set of identity-defining goals and values. Based on these two processes, Marcia derived four statuses: achievement (individuals with strong commitments following a period of exploration), foreclosure (individuals having enacted commitments without previous exploration), moratorium (individuals who are still exploring and have not enacted strong commitments yet), and diffusion (individuals who are not proactively exploring and do not have strong guiding commitments).
Several researchers have proposed refined models in which exploration and commitment have been unpacked into a larger set of processes. In one such model, Luyckx, Goossens, and Soenens (2006) distinguished four processes subsumed under two complementary cycles. The first cycle (identity formation) builds on Marcia’s (1966) work and captures the processes through which individuals explore alternatives and make commitments: exploration in breadth, or the proactive exploration of alternatives, and commitment making, or the adherence to a set of choices. The second identity cycle (identity evaluation) captures the processes through which individuals (re-)evaluate their identity choices. This second cycle is also described in terms of two processes: exploration in depth, or the evaluation of current commitments, and identification with commitment, or the degree to which these commitments become integrated to the individual’s sense of self.
To illustrate these two identity cycles, we refer to the higher education context, in which adolescents and young adults consider pursuing a college degree. First, they may gather information about different college majors such as physical therapy, psychology, and biology (exploration in breadth), followed by making a clear choice by enrolling in a psychology program (commitment making). Subsequently, once the academic year has started, they may evaluate the degree to which the courses correspond with their internal standards (exploration in depth) and, as a consequence, identify with or feel certain (or not) about becoming a psychologist (identification with commitment). However, due to a variety of contextual and/or intrapersonal factors, individuals may become stuck in their identity search and experience difficulties enacting commitments (Schwartz, Côté, & Arnett, 2005). The indecisive student may keep on hesitating about the psychology program, without actively looking into other options, which would result in feelings of uncertainty and incompetence. Consequently, ruminative exploration was added as a fifth process that hinders identity development. As individuals scoring high on ruminative exploration are partially troubled by what they perceive as inadequate progress toward personally important goals, they experience difficulty settling on satisfying choices and keep asking themselves the same questions (Luyckx et al., 2008).
The model proposed by Luyckx et al. (2008) also allows for a fine-grained analysis of identity statuses. Through the use of cluster analysis on identity process scores, several identity clusters emerged, of which some were similar to Marcia’s original statuses (e.g., Crocetti et al., 2011; Luyckx et al., 2008; Schwartz, Beyers, et al., 2011). Both achievement and foreclosure were characterized by high scores on commitment processes and low scores on ruminative exploration. In addition, achievement was characterized by substantially higher scores on exploration in breadth and exploration in depth. Hence, individuals who explore when making commitments may be most likely to experience identity synthesis and to ascribe meaning to their lives. Individuals in foreclosure, however, may be less likely to experience such a sense of personal meaning (Schwartz, Beyers, et al., 2011; Waterman, 2007).
As moratorium is associated with distress and low self-worth, several authors have questioned whether this status is truly an adaptive step toward identity synthesis. To the extent that young people are engaged in a “perpetual moratorium,” they may experience aggravated identity confusion as well (Côté & Schwartz, 2002; Marcia, 2002). Luyckx et al. (2008) indeed found that individuals in moratorium scored high on ruminative exploration in addition to proactive exploration. An extended moratorium phase may denote a type of arrested development, blocking individuals from forming commitments and progressing to achievement (Côté & Levine, 2002). Further, previous research has identified individuals in “searching moratorium,” who score high on all exploration processes but still maintain a set of commitments (Mannerström, Hautamäki, & Leikas, 2017; Schwartz, Beyers, et al., 2011). These individuals could thus be willing to change existing commitments, while exploring new alternatives. With respect to diffusion, Luyckx et al. (2008) distinguished troubled from carefree diffusion (Archer & Waterman, 1990; Marcia, 1989). Both clusters were characterized by low scores on commitment processes and limited exploration in breadth and in depth. However, more so than carefree-diffused individuals, troubled-diffused individuals attempted to explore identity issues. However, they did so in a predominantly ruminative manner. Thus, whereas troubled-diffused individuals might be unable to take proactive steps in identity development, carefree-diffused individuals seem to be uninterested or unmotivated to do so (Luyckx, Klimstra, Schwartz, & Duriez, 2013; Schwartz, Beyers, et al., 2011). Finally, an undifferentiated cluster emerged (Luyckx et al., 2008; Schwartz, Beyers, et al., 2011), consisting of individuals who scored close to the sample means on all identity processes.
The Promise of Identity Research for Understanding Psychopathology
Both identity structure and processes have repeatedly been related to indicators of adjustment and distress in community research (e.g., Crocetti et al., 2011; Luyckx et al., 2008; Schwartz, Beyers, et al., 2011; Wiley & Berman, 2013). Recently, there has been increasing research and theorizing focusing on the link between identity and psychopathology: Do certain identity processes and mechanisms render individuals vulnerable for displaying psychopathology? Or, conversely, can one’s identity also protect against experiencing pathological symptoms and behaviors? Both a view on one’s degree of identity synthesis/confusion and a fine-grained perspective on identity commitment and exploration processes (and how they combine into certain identity clusters or statuses) have great potential to improve our understanding of how normative identity development may contribute to, and may become intertwined with, psychopathology. Further, inspired by developmental psychopathology (Kaufman et al., 2014), an explicit focus on normative-developmental constructs can inform us as to how, and under which circumstances, identity development may go awry and give rise to clinical identity problems or disorders. Hence, such a continuum perspective on identity may provide important insights for our understanding of the identity–psychopathology link.
Such an integrative perspective on identity in which both normative and dysfunctional mechanisms are mutually informative for understanding psychopathology emerges prominently in an alternative model for personality disorders as forwarded in DSM-5 Section III (American Psychiatric Association [APA], 2013). In this alternative model, identity is recognized as a potential factor in all personality disorders (and not just borderline personality disorder as was the case in DSM-IV-R, APA, 2000, and earlier editions). More specifically, this alternative model describes personality pathology in terms of impairment in personality functioning (Criterion A) and having one or more pathological personality traits (Criterion B). Moderate or greater impairment in personality functioning is manifested by characteristic difficulties in two or more of the following four domains: identity, self-direction, empathy, and intimacy. When looking at how these domains of identity and self-direction are defined, some references to (neo-)Eriksonian notions of identity structure and decision-making in terms of exploring and committing to life goals can be found. However, the many nuances of key identity constructs forwarded in developmental psychology are not included (Pasupathi, 2014), necessitating integrating more developmental research into the identity–psychopathology linkages.
Such a call for a more fine-grained developmental study of identity in understanding psychopathology has been advanced by several authors. Recently, Klimstra and Denissen (2017) have proposed an integrative framework in which aspects of psychological functioning and identity notions of structure and process are incorporated in a multidimensional space. More specifically, identity components would be positioned in the center of this multidimensional space, and aspects of psychological functioning could be closer or further away from the center. The distance between both would then represent the degree of relevance of these aspects to one’s identity. Furthermore, Klimstra and Denissen argue that one’s identity and psychopathological symptoms may become increasingly interwoven over time. In 2014, Kaufman, Montgomery, and Crowell explicitly advocated for a more integrative study of clinical and developmental perspectives in order to advance our understanding of identity problems and dysfunction. The need for such an integrative study has been emphasized again in their more recent paper in which they have advanced an explanatory framework of identity pathology drawing from complementary evidence from social, developmental, behavioral, clinical, and neuroscience literatures (Kaufman & Crowell, 2018). Further, Kaufman, Montgomery, and Crowell (2014) advocate for a clear definition of different identity terms as both developmental and clinical literatures would greatly benefit from a shared lexicon in which key constructs are defined unambiguously. To build bridges between both literatures, the core building blocks need to be clearly delineated and agreed upon such that definitional confusion can be limited. For instance, although terms such as identity disturbance and diffusion are often used interchangeably, it remains to be determined when and how a normative sense of identity diffusion as defined in neo-Eriksonian traditions sets the stage for or transforms into clinical identity disturbance (Kaufman et al., 2014; Kernberg, 1984; Schmeck, Schlüter-Müller, Foelsch, & Doering, 2013) and, consequently, may render individuals especially vulnerable for experiencing psychopathology (Westen, Betan, & DeFife, 2011).
In the present article, we do not claim (or even aim at) resolving these difficult issues. However, we aim at initiating some first steps in this direction by demonstrating how developmental notions of identity structure and process can inform our understanding of certain psychopathological behaviors. In doing so, we mainly seek to describe research examining behaviors such as eating disorder (ED) symptomatology and nonsuicidal self-injury (NSSI), as both share a common ground in that they are seen as behaviors that “target the body.” The body has long been described as crucial for identity development, although integrative developmental research focusing on body–identity linkages is somewhat lagging behind (Erikson, 1968; Kling, Wängqvist, & Frisén, 2018; Orbach & Mikulincer, 1998; Wängqvist & Frisén, 2013). The feeling of being at home in one’s body is indeed a key component of the self (Erikson, 1968), with the bodily self-developing in close interaction with one’s general sense of self (Cash & Deagle, 1997; Orbach & Mikulincer, 1998). Along these lines, and as further detailed below, body image problems may not only affect how individuals think about themselves (Wängqvist & Frisén, 2013), but these body image issues may become closely intertwined with a sense of identity diffusion or even clinical identity disturbance. Such a suboptimal self-trajectory, in turn, may make individuals especially vulnerable for body dissatisfaction, and partially as a consequence, pathological self-harm behaviors such as disordered eating and NSSI (Muehlenkamp & Brausch, 2012; Orbach, 1996; Vartanian, Hayward, Smyth, Paxton, & Touyz, 2018). Below we describe recent research efforts examining how identity issues may become intertwined with such self-harm behaviors.
Identity and ED Symptoms and Pathology
EDs are prevalent in adolescents and emerging adults and have a devastating impact on both physical and mental health. The DSM-5 (APA, 2013) describes anorexia nervosa (AN), bulimia nervosa (BN), and binge-eating disorder (BED) as the three main EDs. AN is characterized by a restriction of energy intake relative to energy requirements, which leads to a significantly low body weight. Additionally, an intense fear of gaining weight and disturbed body and weight experiences is emphasized. BN is characterized by recurrent binge-eating episodes combined with inappropriate compensatory behavior to prevent weight gain (purging, laxative misuse, fasting, etc.). Individuals with BN also emphasize their body shape and weight disproportionately in their self-evaluation. Finally, BED is characterized by recurrent binge-eating episodes without recurrent inappropriate compensatory behavior to prevent weight gain.
Overall, EDs have a peak onset between the ages of 15 and 19 years (Micali, Hagberg, Petersen, & Treasure, 2013). However, across development, patients may experience diagnostic shifts, with a typical shift from more restrictive ED diagnoses to more binge-eating/purging types over time (Fairburn, Cooper, & Shafran, 2003; Vandereycken & Noordenbos, 2008). In general, BN and BED seem to be more prevalent than AN in both adolescents and adults (Steering Group on Eating Disorders in the Netherlands, 1998; Swanson, Crow, Le Grange, Swendsen, & Merikangas, 2011). Along with these formal diagnoses, disturbed eating behaviors, referring to unhealthy weight control behaviors that do not fulfill diagnostic criteria of an ED (e.g., fasting, taking diet pills or laxatives, vomiting, binge-eating), are highly prevalent in adolescents (approximately 57% for girls and 30% for boys; Croll, Neumark-Sztainer, Story, & Ireland, 2002) and emerging adults (approximately 25% for women and men; Quick & Byrd-Bredbenner, 2013). Generally, females report more disturbed eating behaviors and ED cognitions than males (Lewinsohn, Seeley, Moerk, & Striegel-Moore, 2002; Micali, Ploubidis, De Stavola, Simonoff, & Treasure, 2014).
As the age of onset indicates, adolescence and emerging adulthood represent crucial life periods in which individuals may become vulnerable to display eating symptoms or even an ED. These life periods are characterized by various bodily changes and a great concern with social acceptance (Elkind & Bowen, 1979; Harter, 1999), which may make adolescents especially vulnerable to internalizing certain beauty standards that idealize slim and fit bodies (Suisman et al., 2014). Moreover, research increasingly indicates that the process of identity formation is closely related to the development of such disturbed eating symptoms. Verstuyf, Van Petegem, Vansteenkiste, Soenens, and Boone (2014) found that individuals’ identity styles (Berzonsky, 2004) are differentially related to the internalization of the body perfect ideal and unhealthy dietary restrictions. More specifically, individuals who maintain active and critical attitudes toward identity-relevant information (i.e., information-oriented style) have been found to distance themselves from the body perfect ideal, whereas individuals who are vulnerable to socially expected goals and values (i.e., normative style) tend to internalize the body perfect ideal and adopt appearance-focused and unhealthy dietary restrictions. Finally, individuals who tend to avoid making identity-related decisions (i.e., diffuse-avoidant style) seem to be vulnerable for adopting unhealthy eating patterns.
The identity–ED link also seems to be important in clinical samples, as patients with an ED have been found to experience more identity confusion than individuals without this diagnosis (Auslander & Dunham, 1996; Schupak-Neuberg & Nemeroff, 1993; Sparks, 1993). Focusing on identity processes and statuses, we (Verschueren et al., 2017) compared a clinical ED sample to an age-matched community sample and found that patients with an ED experienced far greater difficulties in forming a personal identity than community individuals did. More specifically, ED patients scored significantly lower on most adaptive identity processes (i.e., commitment making, identification with commitment, and exploration in breadth) and significantly higher on ruminative exploration as compared to community controls. The differences in the commitment processes and ruminative exploration were accompanied by especially large effect sizes. Hence, it seems particularly difficult for patients with an ED to make self-endorsed identity commitments, possibly due to a ruminative identity process. Interestingly, when examining the identity statuses that emerged in the combined sample of patients with an ED and community controls, an identity disorder status was identified, which consisted solely of patients with an ED. This identity status captured individuals scoring very low on all adaptive identity processes combined with a very high score on ruminative exploration (resembling a more pathological form of troubled diffusion) and, hence, indicated serious identity problems or even identity disturbance. Altogether, the results of this study suggested that patients with an ED experience more trouble in making identity-related choices and proactively exploring identity issues and that some patients seem to experience an identity disorder that is associated with maladaptive functioning.
Although an increasing body of research has examined the relation between identity and eating symptomatology, no consensus exists on how the directionality of these associations can be understood. In this respect, most theorists agree that identity difficulties are already present before the onset of ED symptomatology. Bruch (1981, 1982) described AN as developing due to impairments in overall identity development. A disrupted identity may motivate adolescents to search for a (maladaptive) source of self-definition, which is often found in the controllable and culturally valued aspect of body weight (Bruch, 1981; Polivy & Herman, 2007; Schupak-Neuberg & Nemeroff, 1993). Vartanian et al. (2018) indeed found that individuals with lower self-concept clarity (somewhat resembling Erikson’s identity synthesis; Campbell et al., 1996) seem to be especially at risk for internalizing Western beauty ideals and for comparing their appearance more frequently to that of others. In turn, internalization of beauty ideals and appearance comparison may be associated with body image concerns and disordered eating. Hence, restrictive eating may represent a (subconscious) quest for a stronger sense of self and individuation (Bruch, 1981; Casper, 1983).
Building further on these ideas, an increasing number of theorists state that eating symptomatology may not only arise from identity problems, but that it could also play into one’s identity development and even derail normal identity development. Corning and Heibel (2016) note that most individuals with disturbed eating behaviors are preoccupied with their body weight and shape, with body weight representing a disproportionate share of their identity. Fairburn, Cooper, and Shafran (2003) describe a dysfunctional system for self-evaluation as one of the core deficits of patients with an ED. This system would lead patients with an ED to evaluate themselves almost entirely in terms of their eating habits and body shape, while alternative sources of self-worth are lacking. Hence, when these self-aspects are under attack (e.g., by weight teasing or social comparison), they may be experienced as direct threats to the self (Corning & Heibel, 2016; Polivy & Herman, 2007) that in turn motivate patients to adhere even more to strict dieting rules. Indeed, Schupak-Neuberg and Nemeroff (1993) described how controlling food intake could represent a regulation of one’s identity in patients with an ED. This food-self metaphor would not only explain why restrictive eating brings inner calmness to the patient but could also offer insights into binge-purging behavior. Polivy, Herman, and McFarlane (1994) discussed that, when ED patients are confronted with a threat to their self-image, anxious and nervous feelings emerge, which in turn drive them toward binge eating as well. During a binge, the collapse of bodily regulation may represent a collapse of one’s self-definition as well (Schupak-Neuberg & Nemeroff, 1993). The cognitive narrowing that occurs during the binge blocks self-awareness for a short period of time (Heatherton & Baumeister, 1991). After the binge, when self-awareness returns, the remaining negative feelings are then often expelled by purging (Schupak-Neuberg & Nemeroff, 1993). Several authors have described similar ideas regarding the functional mechanisms of binge-purging behavior, in which this type of behavior may help individuals to avoid dealing with identity issues or escape from thoughts about the self (Heatherton & Baumeister, 1991; Herman & Polivy, 1988; Wheeler, Adams, & Keating, 2001).
Altogether, identity functioning and eating symptomatology seem to be closely and reciprocally related to one another, as visually represented in Figure 1. Briefly summarized, individuals experiencing more identity diffusion may also be more susceptible to internalize the body perfect ideal—promoting a slender or muscular body for women and men, respectively. Consequently, this internalization may fuel individuals to consider this perfect body ideal as a source of self-definition. This can, in turn, stimulate the wish to be thinner and trigger disturbed eating behavior, especially in women. Once individuals have engaged in these types of behavior, it may install a harmful cycle in which the body and eating regulation become an increasingly central part of one’s identity and self-esteem. Hence, gaining weight may be regarded as a threat to one’s identity, which contributes to the development of a vulnerable sense of self and, consequently, identity diffusion.
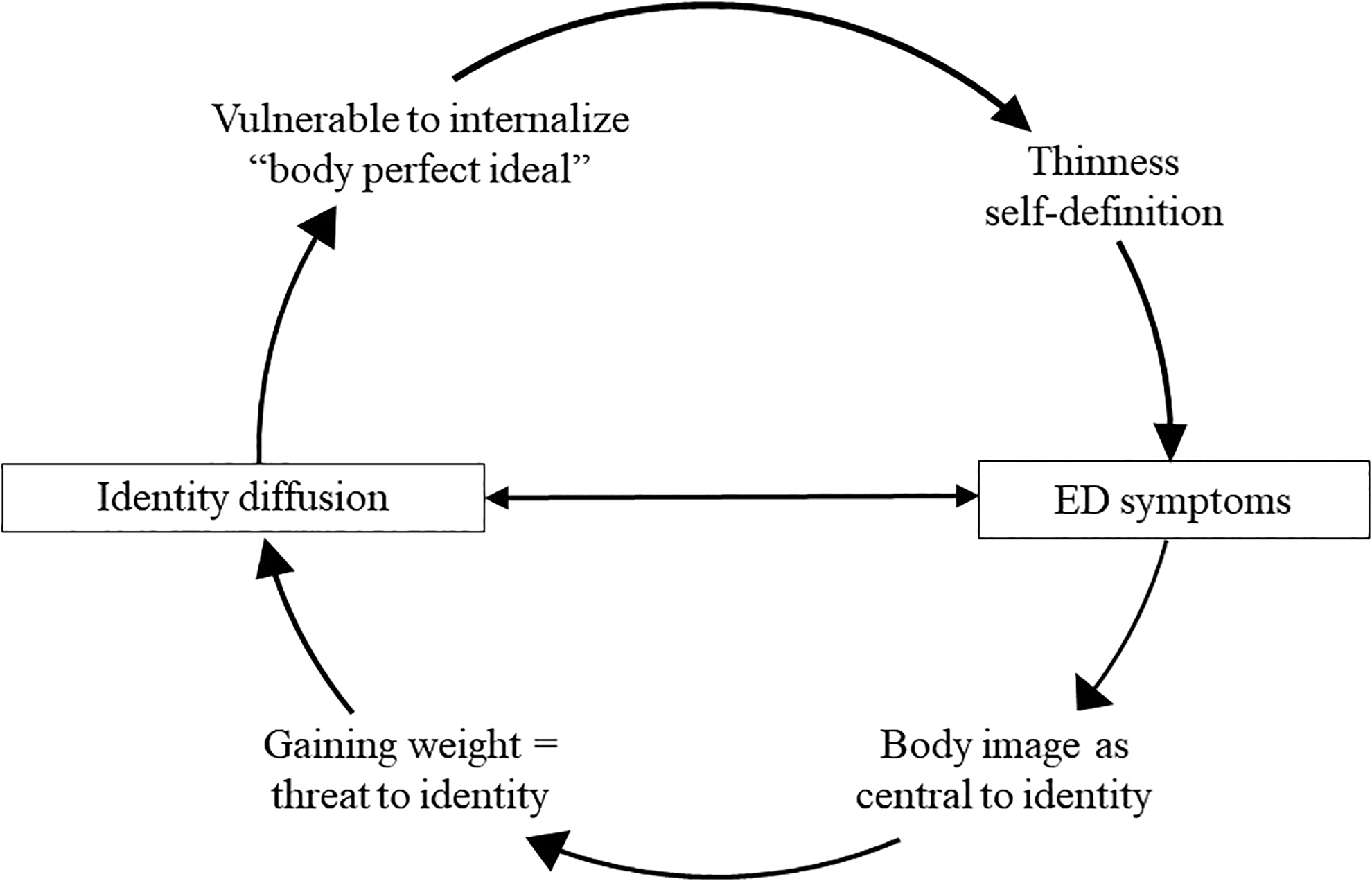
The identity–ED interplay.
To examine such a bidirectional relationship, we conducted a 2-year, three-wave longitudinal study with a community sample of adolescents and emerging adults (Verschueren et al., 2018). Cross-lagged analyses indicated that identity confusion appeared to increase one’s vulnerability to experience body dissatisfaction and display bulimia symptoms over time relative to the rest of the sample, whereas identity synthesis seemed to protect against the emergence of both. Additionally, identity synthesis seemed to protect against the development of drive for thinness as well. Hence, these findings seem to be in line with the idea that adolescents with certain doubts about their identity may be more vulnerable to adopting the body perfect ideal of Western society and experience more eating symptomatology (Berzonsky, 2004; Verstuyf, Van Petegem, Vansteenkiste, Soenens, & Boone, 2014). At the same time, our findings indicated that body dissatisfaction and bulimia symptoms positively predicted identity confusion and negatively predicted identity synthesis over time as well. Eating symptomatology thus seems to hamper normative identity development over time, as individuals with disturbed eating behavior may experience a narrowly defined identity characterized by an overvaluation of body size and weight (Corning & Heibel, 2016; Fairburn et al., 2003).
In line with these results, Corning and Heibel (2016) have advocated for the promotion of a healthy identity development in ED prevention programs, in which adolescents learn to bolster other self-aspects besides their body image and appearance. Such an approach may result in individuals being able to develop a more well-rounded identity and self-esteem in which other self-aspects are valued and may allow them to experience more optimal self-development over time. Similarly, in ED intervention programs, it seems crucial for therapists to pay special attention to identity formation by offering patients tools in which they can learn to break the vicious cycle linking identity problems with eating symptomatology.
Identity and NSSI
NSSI is defined as the repetitive, direct, and deliberate destruction of one’s body tissue without an intention to die, and for purposes not socially sanctioned (Nock & Favazza, 2009). NSSI represents a distinct category of behavior that falls under the umbrella of self-directed violent behaviors and has been increasingly identified as an important public health concern, especially among adolescents. In the past, NSSI has been described using various terms such as self-mutilation, partial or parasuicide, automutilation, delicate cutting, deliberate self-harm, and self-injurious behaviors. Common examples of NSSI include self-cutting, self-scratching, head banging, self-hitting, and self-burning. As NSSI involves direct destruction of the body tissue, indirect self-harming behaviors such as alcoholism, self-poisoning, substance abuse, and EDs are not considered as NSSI.
NSSI is related to both distal and proximal intrapersonal (e.g., personality) and interpersonal (e.g., attachment) vulnerability factors (Nock, 2009) and negative mental health outcomes (e.g., depressive and anxiety symptoms; Kerr, Muehlenkamp, & Turner, 2010). Additionally, approximately 50–75% of individuals with a history of NSSI attempt suicide at some point in their life (Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006). These substantial negative mental health outcomes of NSSI underscore the need for a better understanding of NSSI (Mullins-Sweatt, Lengel, & Grant, 2013). NSSI has been added to the “Conditions for Further Study” section in the DSM-5 (APA, 2013) to stimulate further research on this set of destructive behaviors. Currently, the criteria for NSSI disorder include (A) engaging in NSSI on 5 or more days in the last year, (B) engaging in NSSI to relieve negative feelings, interpersonal difficulty or to induce positive feelings, (C) NSSI being associated with interpersonal difficulties, preoccupation, and thinking about NSSI even when not acted upon, (D) the behavior is not socially sanctioned, (E) causes distress or interference in functioning, and (F) does not occur exclusively during psychotic episodes, delirium, and substance intoxication or withdrawal (APA, 2013, p. 803).
In community samples, lifetime prevalence rates of NSSI are estimated to be around 17.2% among adolescents, 13.4% among young adults, and 5.5% among adults (Muehlenkamp, Claes, Havertape, & Plener, 2012; Swannell, Martin, Page, Hasking, & St John, 2014). In clinical samples, NSSI rates are even higher (Briere & Gil, 1998) and have been found to range from 23.8% to 31.0% in patients with an ED (Cucchi et al., 2016; Muehlenkamp, Claes, Smits, Peat, & Vandereycken, 2011) and rise up to 70–75% in patients with borderline personality disorder (Claes, Van den Eynde, Guillaume, Vogels, & Audenaert, 2012; Kerr et al., 2010). A recent meta-analysis by Bresin and Schoenleber (2015) has demonstrated that NSSI is slightly more common in women than in men. This gender difference is more pronounced in clinical samples than in community samples. Gender differences also exist in the type of methods endorsed by individuals to engage in NSSI—Women tend to engage more often in cutting behaviors, whereas men are more likely to engage in self-battery (e.g., self-hitting, head banging; Bresin & Schoenleber, 2015). Irrespective of the type of sample (community or clinical sample), the age of onset of NSSI peaks around the age of 14–15 years. A second peak is observed around the ages of 20 and 24 years in community and clinical samples, respectively (Gandhi, Luyckx, Baetens, et al., 2018; Plener, Schumacher, Munz, & Groschwitz, 2015). As in the case of EDs, the higher prevalence and greater likelihood of NSSI onset in adolescence and emerging adulthood again raise the possibility of the role of identity development in increasing one’s vulnerability to engage in NSSI.
The association between NSSI and identity formation has long been suggested in extant literature. For example, Podvoll (1969) observed that patients engaging in self-cutting or related self-harm behaviors transformed their symptoms into an identity (slashers, cutters, scratchers, etc.). Based on the observation of patients admitted to a psychiatric hospital, Podvoll reported that patients with NSSI have an enduring feeling of emptiness and a disbelief in their own growth potential. They often believe that the NSSI is all they possess and that nothing else can substantially define their core sense of self (Podvoll, 1969). Consequently, stopping such self-harm behaviors may be experienced to lead to inner emptiness and severe identity diffusion.
Podvoll’s initial observations have been echoed by a number of researchers. Asch (1971), for instance, stated that NSSI may serve as a way of counteracting a sense of emptiness and identity confusion. Interestingly, more recent qualitative studies have drawn similar conclusions. Using thematic analysis of online autobiographical accounts of NSSI on blog posts, Breen, Lewis, and Sutherland (2013) concluded that NSSI may serve as a means of developing a sense of identity (“I am a self-injurer”), through connecting with others who engage in similar behaviors. Hence, despite the problematic and self-destructive nature of NSSI, it may provide individuals with a subjectively experienced coherent sense of self as it may serve as a springboard to connect with a social group (i.e., the group of self-injurers). Subsequently, individuals may draw from such a collective identity to derive a personal sense of self that can persist across time (cf. Klimstra & Denissen, 2017).
A recent study by Claes, Luyckx, and Bijttebier (2014) found that NSSI was negatively associated with identity synthesis and positively associated with identity confusion in a sample of high school students. Further, even when controlling for depressive symptoms, age, and gender, they found that identity confusion explained additional variance in NSSI. These findings have been replicated in multiple cross-sectional studies in both community and clinical samples (Claes et al., 2015; Gandhi, Luyckx, Goossens, Maitra, & Claes, 2016; Luyckx, Gandhi, Bijttebier, & Claes, 2015a, 2015b). Relatedly, the link between experienced identity distress in specific life domains (long-term goals; career choice; friendships; sexual orientation and behavior; religion, values, and beliefs; and group loyalties; Berman, Montgomery, & Kurtines, 2004) and NSSI has been explored as well. Gandhi, Luyckx, Maitra, and Claes (2015) demonstrated that the subjective impairment accompanying such identity distress predicted the lifetime prevalence of NSSI even when controlling for age, gender, anxiety, and depression.
Although such cross-sectional studies appear to suggest that disturbances in identity formation can increase vulnerability to NSSI, a longitudinal study in high school students by Gandhi et al. (2017) provides a more nuanced picture of the identity–NSSI link. Cross-lagged analyses suggested the presence of a bidirectional association between NSSI and identity synthesis/confusion, in much the same way as identity and ED symptoms were related (Verschueren et al., 2018). That is, individuals experiencing less identity synthesis and increased identity confusion were more likely to engage in NSSI 1 year later relative to the rest of the sample. Furthermore, engagement in NSSI at Time 1 was also found to be associated with further relative decreases in identity synthesis and increases in identity confusion. The potential existence of such reciprocal associations was also found in a cross-sectional study linking identity statuses to both past and current NSSI (Luyckx et al., 2015b). Luyckx and colleagues reported that individuals in the moratorium status were most likely, and individuals in the achievement status were least likely, to report NSSI in the past. This finding indicates that engaging in NSSI earlier on in the life span may delay identity formation. On the other hand, troubled-diffused individuals were most likely to report current (but not past) NSSI, suggesting that identity diffusion might play into NSSI as well. That is, NSSI could constitute a problematic coping strategy for dealing with identity issues. In line with Gandhi et al. (2017), these results do indicate that the association between identity and NSSI may be reciprocal.
Based on the existing theoretical understanding of NSSI and identity formation and the findings of the aforementioned cross-sectional and longitudinal research, we propose the following model (Gandhi et al., 2017; see also Figure 2) to explain the observed bidirectional relation between identity formation and NSSI. As detailed below, common pathways linking Figures 1 and 2 can be identified. Engaging in NSSI may help individuals who experience identity confusion in at least two ways. First, it can help them in managing negative affect. An increase in identity confusion has been shown to be associated with a corresponding increase in distress and internalizing symptoms (Luyckx, Klimstra, Duriez, Van Petegem, & Beyers, 2013). To regulate this negative affect, adolescents experiencing identity diffusion may engage in NSSI. Second, engaging in NSSI may offer them an alternate sense of self. NSSI may represent a disproportionate aspect of one’s identity and may even prompt some individuals to form the negative identity of a self-injurer. Negative identities, according to Erikson (1968), are those that go against the values and attitudes prevalent in society. Indeed, apart from the group that encourages NSSI, the negative identity of the self-injurer is less likely to receive validation from one’s immediate interpersonal context. As identities require “inner assuredness of anticipated recognition from those who count” (Erikson, 1968, p. 165) for their stability, the identity of a self-injurer may remain short-lived (Côté & Levine, 1987). Destabilization of the self-injurer identity may lead individuals back to an increased sense of identity diffusion.
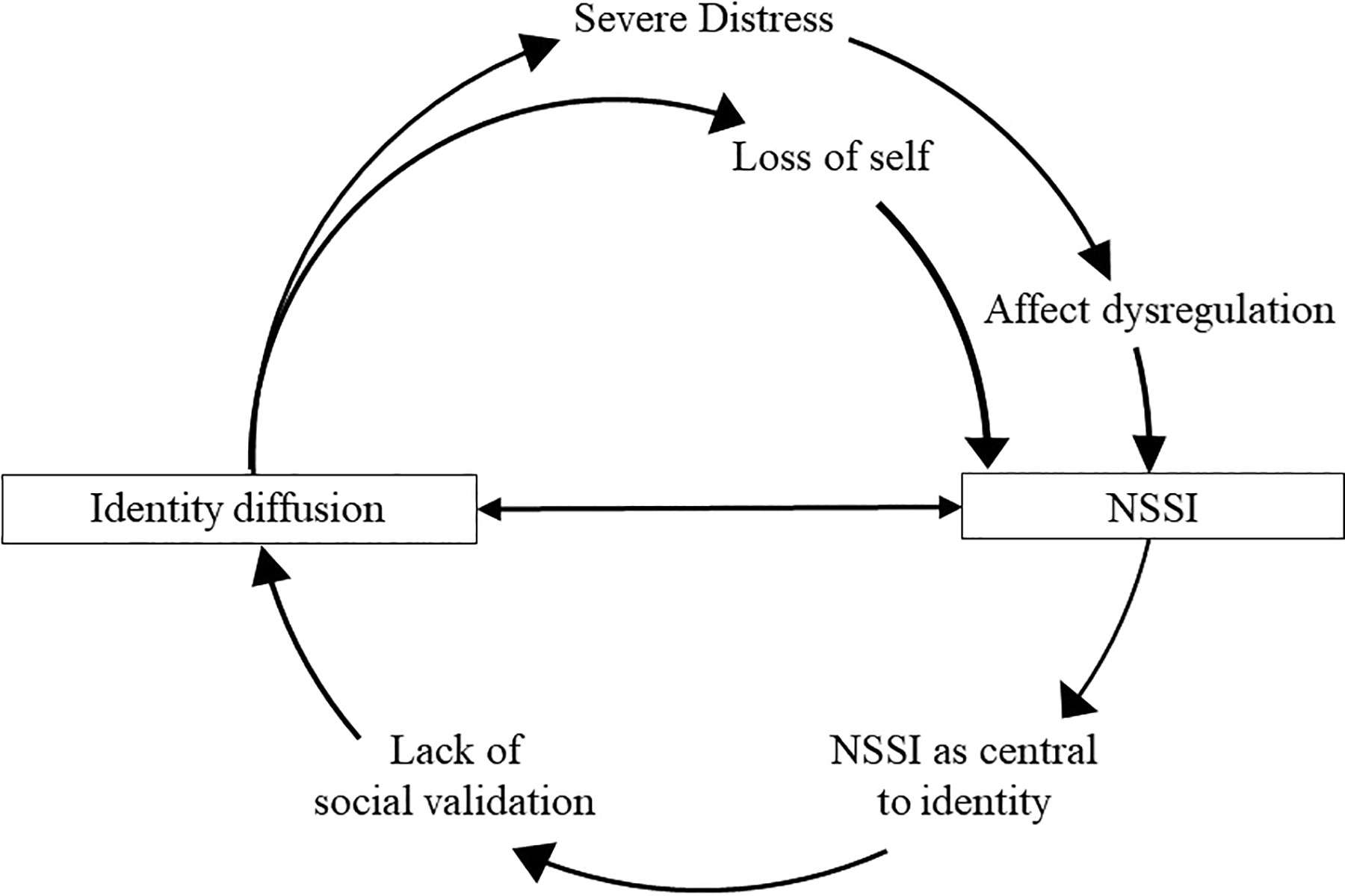
The identity–NSSI interplay.
Common Pathways: The Potential Trans-Diagnostic Value of Identity
Based on the research lines described above, common pathways linking identity to certain body-related psychopathological behaviors may be identified. Not surprisingly, ED and NSSI behaviors are highly comorbid (Claes, Klonsky, Muehlenkamp, Kuppens, & Vandereycken, 2010; Svirko & Hawton, 2007) and share various risk factors (such as emotion dysregulation, dissociation, low body regard, and self-objectification; Claes & Muehlenkamp, 2014). Importantly, both behaviors are described as disturbances in the way the individual experiences one’s own body (Orbach, 1996; Stanghellini, Castellini, Brogna, Faravelli, & Ricca, 2012). Individuals engaging in ED/NSSI behavior have been found to generally experience their body as a physical object that can be looked at by others, in which a first-person perspective is lacking. This self-objectification and materialization of the body results in “a lived body for others” that can be judged or criticized (Stanghellini et al., 2012). Hence, being disconnected from internal bodily experiences, the individual is especially vulnerable to engage in self-harm and/or disturbed eating (Muehlenkamp & Saris–Baglama, 2002; Muehlenkamp, Swanson, & Brausch, 2005). This common risk factor does not only add to the high comorbidity of ED and NSSI but may also relate to their interplay with identity. Research has indicated that, when experiencing this “lived body for others,” the gaze of others on the body becomes highly salient to one’s identity as well (Stanghellini et al., 2012). In these individuals, one’s identity will be almost entirely reduced to the external appearance of the body and individuals will define themselves through evaluations of the other (Stanghellini et al., 2012), similar to the aforementioned theories of Corning and Heibel (2016) and Fairburn et al. (2003) in individuals with an ED. The common mechanisms with identity described above are believed to be present in community samples presenting with subclinical pathological behaviors as well as in clinical samples, where the pathways between identity and body-related pathology would be stronger and could possibly represent a pathological dynamic.
To summarize, identity confusion can bring great distress and feelings of emptiness, which may stimulate individuals to search for a new source of self-definition, be it adaptive or maladaptive (Bruch, 1981; Campbell, 1990). As discussed above, the body represents an important component of the self and is highly valued in Western societies. When confronted with identity confusion and in an attempt to restore their identity, the body may offer some individuals a (maladaptive) source of self-definition. Hence, both disturbed eating and NSSI may be symptomatic of a rather maladaptive quest to experience a coherent sense of self, with the body being perceived as an object that can be controlled. As both behaviors may represent a primary source of self-esteem and identity for these individuals lacking a core sense of self, such an overemphasis and objectification of the body, can be interpreted as a pseudo-identity that can only offer temporary security. As alternative sources of self-esteem and identity are lacking, when confronted with an identity threat, these individuals will lack sources of self-worth (such as occupational or friendship domains) on which to rely. Moreover, as this “ED/NSSI identity” is not socially validated and only provides temporary security, it is highly vulnerable and often yields feelings of identity diffusion. Finally, to cope with feelings of insecurity and self-doubt, both NSSI and ED symptomatology have emotion regulatory capacities that are often used when faced with a challenge. As identity-diffused individuals often experience distress and are prone to internalizing symptoms, self-harming or disturbed eating may help them narrow their cognitive attention on the body. In this way, they avoid dealing with identity issues, which keeps the pathological cycle going.
Based on these common hypothesized pathways of identity with ED and NSSI, future research should address whether similar mechanisms would be at work in other pathologies as well, as identity problems have been described as a trans-diagnostic marker for psychopathology (Kaufman et al., 2014). Somewhat similar to the earlier discussed alternative model for personality disorders in DSM-5, the National Institute for Mental Health has recently described “Perception and Understanding of Self” as a dimensional construct in their Research Domain Criteria (RDoC). The RDoC represents a research framework for investigating and classifying mental disorders, based on dimensions of observable behavior and neurobiological measures. It aims to understand the nature of mental health but does not provide a diagnostic guide. The “Perception and Understanding of Self” comprises processes involved in agency and self-knowledge and promotes self-awareness, self-monitoring, and self-knowledge. Agency is described as recognizing oneself as the agent of one’s actions and thoughts, whereas self-knowledge comprises the ability to make judgments about internal states and traits. Both constructs share a common ground with the identity processes of exploration and commitment focusing on proactively engaging in the identity quest (Luyckx et al., 2008), and the identity synthesis construct of Erikson (1968), in which one experiences oneself as internally consistent. The RDoC framework describes this “Perception and Understanding of Self”-dimension as an important element in trying to understand the development of mental health problems, as it comprises important abilities that can protect or harm an individual vis-à-vis various mental issues.
In line with these recent developments, an increasing number of studies describe identity formation as playing an important role in non-body-related disorders as well (such as hoarding and compulsive buying; Claes, Luyckx, Vogel, Verschueren, & Müller, 2018; Claes, Müller, & Luyckx, 2016; Dittmar, Long, & Bond, 2007; Reeves, Baker, & Truluck, 2012). Hence, similar pathways identified for the ED/NSSI–identity interplay may apply to these disorders as well. With regard to compulsive buying, Reeves, Baker, and Truluck (2012) have described how the acquisition of nonessential goods may offer fulfillment for individuals with an “empty self” (Cushman, 1990). Doing so, buying material goods would offer a way to restore the “empty self” and would complete one’s identity. Similarly, Dittmar, Long, and Bond (2007) underscored how material goods may serve as potential identity substitutes, in which they become an expression of “who one is” (Wicklund & Gollwitzer, 1982). These theoretical ideas offer an understanding of compulsive hoarding as well, as it explains why it is difficult for these individuals to get rid of their possessions—which would feel like losing a part of one’s identity (Frost, Kyrios, McCarthy, & Matthews, 2007).
Future Directions and Concluding Remarks
The present article has integrated various clinically relevant research lines and discussed developmental notions of identity structure and processes to increase our understanding of how certain psychopathological behaviors may emerge and develop. In doing so, we focused mainly on research investigating behaviors that “target the body”—ED symptomatology and NSSI. Hence, although these initial research efforts certainly have their merit as they explicitly direct our attention to how these behaviors may be linked to identity, more systematic and in-depth research is urgently needed to place these findings into a broader perspective. Partially inspired by authors such as Klimstra and Denissen (2017) and Kaufman et al. (2014), we briefly discuss some of these challenges for future research programs.
First, as previously discussed, we reiterate the need to investigate whether similar pathways as outlined in the present article are at work when relating non-body-related pathological behaviors to identity problems. Only when such research has been conducted systematically across different pathological behaviors can the trans-diagnostic value of identity be corroborated and/or can the exact role of identity mechanisms can be pinpointed in specific pathologies. An important challenge in this respect is to assess the incremental predictive validity of identity over and above other, well-established predictors. In doing so, both broad trans-diagnostic vulnerabilities for psychopathology (e.g., impulsivity, negative affectivity, neurobiological markers) and specific risky behavioral processes (e.g., dysregulated behaviors, negative self-evaluations) should be incorporated in future studies to explore how identity may play into psychopathology (Kaufman & Crowell, 2018). In the ideal scenario, such research would adopt a life span perspective, as identity may function as a more proximal intervening mechanism (e.g., mediator) linking psychopathology to well-established factors such as childhood trauma (Kaufman et al., 2014; Klimstra & Denissen, 2017).
Second, the present article focused primarily on research assessing individuals’ identity structure and the behavioral processes of exploration and commitment and does not attend to the content of the identity being developed. However, as highlighted above, if we want to understand the identity functions of pathological behavior, we should consider both identity process/structure and identity content (McLean, Syed, & Shucard, 2016). The importance of identity content for the understanding of psychopathology led Klimstra and Denissen (2017) to propose a multidimensional theoretical framework in which, as noted above, one’s identity content (e.g., the internalization of the body perfect ideal; Vartanian, 2009; Wängqvist & Frisén, 2013) and psychopathological symptoms may become increasingly interwoven over time. A narrative identity approach may be especially suitable for examining how in a subjective process of meaning-making identity content and psychopathology may become increasingly intermixed throughout personal development (Adler, Lodi-Smith, Philippe, & Houle, 2016; McAdams & McLean, 2013). With regard to body image, a recent qualitative study in young adults (Kling et al., 2018) investigated both positive and negative ways in which the body is salient in identity. Thematic analysis identified four main themes (identification with the body, body functionality in performing identity-relevant tasks, appearance and identity in social interactions, and identity-relevant bodily engagement) and provides information on the interindividual differences with respect to this body–identity integration. Further, Dings (2019) has elaborated on the dynamic interplay between narrative identity and embodiment, focusing on the underlying mechanisms that could be at work. In his paper, he describes the debate on this matter that points to a potential bidirectional relation linking both constructs. More specifically, embodiment can be regarded a prerequisite for narrative self-understanding, while changes in the narrative also seem to affect one’s experience of the body.
Third, closely aligned with this notion of identity content, we briefly discussed that behaviors such as NSSI may also have important social identity functions in that they may play into a sense of group belonging, as individuals may affiliate with others displaying similar behaviors (“we are self-injurers”). This phenomenon can be observed, for instance, in school or other peer contexts (Breen, Lewis, & Sutherland, 2013; Giletta, Burk, Scholte, Engels, & Prinstein, 2013; Muehlenkamp, Brausch, Quigley, & Whitlock, 2013) as well as in online communities, such as the so-called pro-ana and pro-mia websites. However, the recent research lines discussed in the present article mainly focused on ego-identity and personal identity, somewhat at the expense of social identity mechanisms. Further, personal and social identity mechanisms intersect in that certain group memberships may predominantly shape one’s personal sense of identity as they become their main defining identity asset, somewhat at the expense of other identity domains (Albarello, Crocetti, & Rubini, 2018; Erikson, 1968). In other words, one’s identity may become engulfed with these specific contents related to pathological behavior (see Klimstra & Denissen, 2017 for a more extended discussion). In sum, to fully understand how identity and psychopathology are related, research targeting identity at the personal, relational, and social levels is urgently needed (cf. Schwartz, Luyckx, et al., 2011).
Fourth, most identity research originating from the West is based on the notion that a consistent sense of self (i.e., identity synthesis from an Eriksonian perspective) plays into general well-being and positive mental health (Erikson, 1950, 1968). However, cultural psychologists highlight that the need for such a consistent self is more likely a feature of Western cultures than of Eastern cultures (Church et al., 2008; Markus & Kitayama, 1991; Suh, 2002). Given the collectivistic nature of most of the Eastern cultures, a flexible sense of self—which changes and molds itself in accordance to the needs of different interpersonal relations—can aid in maintaining social harmony. Consequently, self-consistency may not be as an important goal in Eastern cultures as it is in Western cultures (Heine, 2001; Heine & Lehman, 1999; Suh, 2002). Empirical research has indeed shown that a lack of a consistent sense of self in Eastern samples often has a weaker link with poor psychological outcomes as compared to Western samples (Church et al., 2008; Kanagawa, Cross, & Markus, 2001; Markus & Kitayama, 1991; Suh, 2002). Some preliminary NSSI research does seem to support this observation. Gandhi, Luyckx, Adhikari, et al. (2018) found disturbances in identity formation (low identity synthesis and high identity confusion) to be stronger predictors of NSSI in Belgian youth as compared to Indian youth. In summary, existing research and theory suggest that cross-cultural replication is necessary to determine whether similar mechanisms linking identity and (body-related) pathological behaviors can be found in different cultures.
Finally, the existing body of research has investigated identity formation primarily from a between-person perspective, comparing individuals’ scores relative to the scores of other individuals in the sample. Although this approach provides valuable information, it fails to examine how certain (identity) processes and mechanisms fluctuate over time within the individual. As identity formation is regarded a highly idiosyncratic developmental process, a within-person modeling approach provides important information as well (Becht et al., 2017; Lichtwarck-Aschoff, van Geert, Bosma, & Kunnen, 2008). To illustrate, a recent study by Bogaerts et al. (2018) examined the directionality of effects linking identity structure and processes in adolescence by focusing on both between- and within-person associations. Combining these two perspectives, the study was able to identify (1) which individuals experienced substantial identity difficulties compared to their peers (i.e., at the between-person level) and (2) which mechanisms were at work in the intrapersonal development of such identity issues (i.e., at the within-person level). Hence, applying both between-person and within-person analyses is important in identity research, as both perspectives can uncover important parts of the puzzle.
In sum, in line with recent work (e.g., Klimstra & Denissen, 2017), it is our hope that the present article may help in bringing neo-Eriksonian identity research closer again to where it originated from, that is, the clinic, such that the clinical and practical potential and utility of the identity construct may reach its full potential in the years to come.
Footnotes
Authors’ Note
The present article is based on the keynote speech by K. Luyckx held at the SSEA 2018 Self and Identity thematic conference: “Moving the identity field forward: Bridging developmental and clinical research.”
Author Contributions
Margaux Verschueren, Laurence Claes, Amarendra Gandhi, and Koen Luyckx contributed to conception, design, acquisition, analysis, and interpretation; drafted the article; critically revised the article; gave final approval; and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Open Practices
Data and materials for this study have not been made publicly available. The design and analysis plans were not preregistered.