
Abstract
Commercial spaceflight is expanding participant profiles while medical evacuation and resupply remain constrained by distance, cadence, and operational risk. For operators and regulators, the practical question is not whether rare, high-consequence events can be managed with “hospital-like” capability, but whether minimum critical functions remain executable when escalation options are limited. Pregnancy is often assumed to be excluded by policy; however, readiness engineering must still address low-probability, high-impact scenarios when unpreparedness could jeopardize crew safety, mission continuity, liability exposure, and public trust. This perspective uses “Midwifery on Mars” as an extreme-constraints analog to introduce the “Aerospace Midwife” concept: a role-based, auditable capability framework for no-evacuation birth care. It does not advocate pregnancy in space. It does not assume that a Mars mission would manifest dedicated obstetric systems, specialist staffing, or policy approval for such care. Instead, it asks a narrower readiness question: if any autonomous birth-care readiness were claimed under severe mass, volume, power, logistics, communication, and policy constraints, what minimum functions would need to remain executable and auditable? Within this concept, the “Aerospace Midwife” is a designated crew role, held by a clinician or trained nonclinician, authorized to lead physiological birth care, detect early deterioration, initiate time-bounded first-response bundles for postpartum hemorrhage and neonatal transition, and enforce gate conditions for operative escalation. A capability-based minimum set is presented as operational functions rather than equipment lists, emphasizing auditable checks, simulation-based maintenance, training records, and after-action review. The framework is intended to support operator implementation and regulatory oversight of autonomous medical readiness under constraint, with secondary relevance to terrestrial austere settings where timely transfer cannot be assumed.
Keywords
WHY THIS MATTERS NOW FOR OPERATORS AND REGULATORS
Commercial spaceflight is expanding the range of participants and mission profiles, while evacuation and resupply remain constrained by distance, cadence, and operational risk. In this context, “medical rescue” is not a single capability; it is an interdependent system that can fail when one prerequisite degrades. For operators, unpreparedness for low-probability, high-impact medical events can create disproportionate consequences, including mission interruption, downstream liability and insurance exposure, and loss of public trust. For regulators and standards bodies, the challenge is to define readiness requirements that are auditable rather than aspirational. Mission-specific policies, flight medical standards, and risk posture would likely restrict or exclude pregnancy for many exploration-class missions. This Perspective does not advocate pregnancy in space, does not presume policy permissibility, and does not assume routine obstetric capability beyond Earth. Instead, “Midwifery on Mars” is used as an extreme-constraints analog to stress-test autonomous medical operations under “no-evacuation” conditions and to define minimum-viable, auditable functions that can be standardized for training and governance.
WHY MARS IS A USEFUL ANALOG (AND WHY MARS IS NOT THE POINT)
Mars is not the point; constraints are. When evacuation, resupply, blood products, and specialist reinforcement cannot be assumed within clinically meaningful timeframes, obstetric “backup” becomes a fragile dependency chain rather than a reliable safety net. Here, “no-evacuation” refers to settings in which timely transfer to higher-level care cannot be assumed. Mars makes constraints operationally explicit, including communication latency, mass and volume limits, and disrupted logistics, forcing clarity about prerequisites that are often implicit in facility-based assumptions about rescue capacity. 1 Although Mars is an extreme analog, the framework is intended to inform readiness design in any setting where timely transfer cannot be assumed. Planetary health scholarship similarly supports designing care systems that remain safe under compound shocks and translate back to terrestrial resilience. 2
Mars also makes engineering scarcity explicit. In exploration-class missions, medical systems must compete for mass, volume, power, crew time, maintenance burden, and logistics robustness within vehicles and habitats already constrained by life support, mission equipment, and long-duration sustainment. Accordingly, this paper does not assume that a Mars transit vehicle or early settlement would have the habitable volume, logistics margin, policy latitude, or specialist support required for a dedicated obstetric package. Rather, Mars is used here to make overclaiming of “capability” harder by asking which functions would remain credible if resupply, reinforcement, or one critical prerequisite failed.3–5
THE “AEROSPACE MIDWIFE” CONCEPT: A ROLE FRAMEWORK, NOT A CREDENTIAL
This Perspective presents the “Aerospace Midwife” as a concept for an autonomy capability: a designated crew role, held by a midwife, nurse, physician, or trained nonclinician crew member, who is trained and authorized to (i) lead physiological birth care, (ii) detect early deterioration, and (iii) initiate time-bounded first-response bundles for postpartum hemorrhage and neonatal transition, while enforcing explicit gate conditions for operative escalation. It is not a new credential and not a claim that a Mars mission would necessarily manifest such a role in practice. Rather, it is a readiness-oriented role framework that can be taught, assessed, bounded, and maintained if an operator elects to claim any autonomous birth-care capability under no-evacuation conditions. Whether any mission would implement this concept, and at what level, would depend on policy decisions, engineering trade-offs, scope-of-practice limits, crew composition, and sustainment burden.
It clarifies scope, decision authority, and documentation standards under constrained options, and it shifts preparation from equipment checklists to competency-based functions that can be validated through simulation. From an operator and regulator perspective, “auditable” means that readiness produces evidence. Examples include competency sign-offs, drill logs with pass criteria, training records with revalidation cadence, checklist use, and documented after-action reviews (AARs) that close gaps. These artifacts allow oversight to focus on whether critical functions remain executable under stress rather than whether a broad list of devices exists on paper. Recent disruptions, including those affecting referral pathways during the COVID-19 pandemic and in conflict-affected settings, illustrate how quickly “rescue capacity” can become unavailable in practice, underscoring the value of designing care around reliability rather than fragile dependencies.6–9
The Aerospace Midwife concept is intentionally scoped to what can be trained, executed, and audited under no-evacuation constraints. It is not a claim of comprehensive obstetric capability, nor a substitute for physician-led specialty care when evacuation and full perioperative support are available. It is also not an assertion that all prerequisites could be manifested within a Mars transit vehicle or early settlement. Rather, the concept is designed to reduce reliance on brittle prerequisites, prioritize time-bounded first response, and make escalation limits explicit when prerequisites cannot be sustained. As a governance artifact, it also supports transparent risk communication: operators can define what care is and is not deliverable on a given mission class, and document the conditions under which “stop rules” and gate conditions apply. This explicit boundary setting is consistent with the ethics of constrained choice in long-duration spaceflight. In such settings, moral burden is concentrated, and the option set is structurally limited.
TWO DESIGN LOGICS: DEPENDENCY-HEAVY SURGICAL RESCUE VS. PHYSIOLOGY-FIRST RELIABILITY
A common instinct under constraint is to expand surgical capacity forward. In a no-evacuation environment, however, surgical capability is a dependency chain. If any link fails, including sterility, anesthesia monitoring and airway rescue, hemostatic capability without blood products, or sustained postoperative observation and infection surveillance, outcomes can worsen even when a procedure is technically feasible. This is not an argument against operative obstetrics in principle; it is an argument that “surgery-capable” is easy to overestimate when prerequisites cannot be guaranteed over time. A physiology-first, midwifery-led model takes a different stance. It aims to reduce the probability that a complex rescue will be needed by optimizing normal labor and early recognition, and it prioritizes robust first response to high-frequency, high-consequence threats that cannot wait for definitive care. In autonomy settings, the design objective is not maximal capability but reliable execution of a small set of decisive functions.
GATE CONDITIONS: MINIMUM STANDARDS FOR OPERATIVE ESCALATION
In a no-evacuation setting, being able to operate is not equivalent to being able to deliver safe operative care. Explicit gate conditions are required before initiating a surgical rescue pathway, such as cesarean birth. At minimum, these include sterility sufficient to reduce preventable contamination, anesthesia monitoring and airway rescue meeting predefined minimums, and postoperative observation and infection surveillance that can be sustained for days rather than hours. If any gate condition cannot be met, the default should remain physiology-first care and stabilization with remote consultation when feasible.
To prevent gate conditions from becoming aspirational, they must be operationalized as auditable checks. Sterility can be defined by clean-birth and clean-procedure capability, hand hygiene resources, and feasible instrument reprocessing. Anesthesia readiness can be defined by minimum monitoring, oxygen delivery capacity, and a rehearsed airway rescue plan. Postoperative sustainment can be defined by observation frequency, infection surveillance triggers, analgesia, and the ability to provide antibiotics and wound care for a defined period. When these conditions cannot be met, avoiding the creation of postoperative dependency may be safer than attempting technically feasible surgery. This framing is consistent with evidence that disruption degrades infection prevention and continuity, compounding risks of preventable harm.7,8
STOP RULES: TURNING AUTONOMY INTO ACCOUNTABLE DECISIONS
Autonomy requires simple, prebriefed rules aligned to recognized guidance, with stop rules that are teachable, drillable, and reviewable after action. The purpose of stop rules is not to replace clinical judgment with rigid algorithms, but to make decision boundaries explicit under constraint: when to continue, when to stabilize, when to consult, and when escalation is unsafe because prerequisites are not met. For labor progress, a locally adopted definition of arrest should be prebriefed, and documentation should capture time, findings, and actions. For hemorrhage, documentation should capture estimated blood loss, shock index trajectory, and response to each first-response element. This matches the prolonged care doctrine that treats trend monitoring and documentation as core clinical functions when evacuation is delayed or intermittent. 10
If progress arrests despite adequate contractions over a predefined interval, transition to damage-control obstetrics and seek remote consultation when possible. Operative escalation should be attempted only if gate conditions are met. If bleeding is clinically concerning or shock index is rising, assume postpartum hemorrhage and initiate first response immediately, including uterine massage, uterotonics, intravenous access and fluids, and tranexamic acid when indicated.11,12 If bleeding persists, add mechanical measures such as uterine balloon tamponade when feasible. 13 If shock progresses without blood products or definitive rescue options, activate contingency plans and predefined ethical limits. 14 If apnea or bradycardia persists after initial newborn steps, begin bag-mask ventilation promptly and reassess at short intervals, consistent with essential newborn care principles. 15
WHY POSTPARTUM HEMORRHAGE AND NEONATAL TRANSITION DOMINATE THE MINIMUM SET
Postpartum hemorrhage remains a leading cause of maternal mortality. Large-scale evidence identifies uterine atony as a dominant cause and highlights risk factors that can be magnified in austere settings. 16 In no-evacuation environments, time to definitive care is effectively unbounded, making early detection and structured first response decisive. Expert consensus supports optimizing early detection and obstetric first response in high-risk workflows. 17 Prevention and treatment are guideline-rich, but the operational problem is execution under constraint. WHO recommendations on uterotonics clarify what should be feasible across settings, while local plans must account for route, staffing, monitoring, and supply robustness. 18 Evidence on oxytocin administration routes reinforces that regimen choice affects feasibility and safety when monitoring capacity is limited. 19 Tranexamic acid effectiveness is time-sensitive and supported by international recommendations and synthesis.11,12 Uterine balloon tamponade is a reasonable adjunct capability, but it depends on sterile technique and follow-up and therefore should be framed as a supplement rather than a substitute for early bundle execution. 13 International guidance on managing complications provides a reference point for what nonspecialist teams can reasonably be expected to deliver and what should trigger escalation planning, even when definitive rescue is not available. 20 Neonatal transition is similarly time-critical. A minimum-viable system requires drying, warming, airway positioning, and effective bag-mask ventilation supported by routine simulation. Structured neonatal resuscitation training programs, including Helping Babies Breathe, improve outcomes in resource-limited settings, supporting the general principle that simple algorithms plus repeated practice can outperform complex plans that cannot be executed reliably. 21
GOVERNANCE, OVERSIGHT, AND DOCUMENTATION AS READINESS INFRASTRUCTURE
No-evacuation obstetrics forces decisions about when escalation no longer benefits the patient and who decides. Long-duration mission ethics supports explicit governance when choice is constrained and moral burden is concentrated. 14 Governance is therefore a minimum capability requiring a named clinical authority (or designated clinical decision-maker), defined scope, and prebriefed escalation limits aligned to context and resources. From a New Space readiness perspective, governance must be inspectable. Operators can define decision rights, documentation requirements, and minimum drill cadence; regulators can require evidence that these controls are active (training records, competency sign-offs, drill results, and AARs) rather than merely declared.
PROPOSED MINIMUM-VIABLE CAPABILITIES
In practice, a minimal audit trail for this role framework can be reduced to four artifacts: (1) role designation and decision rights (who can initiate a bundle, declare a stop rule, and authorize escalation), (2) competency evidence (initial sign-off and periodic revalidation for PPH and neonatal ventilation scenarios), (3) performance evidence from drills (time-to-bundle, ventilation initiation, and checklist adherence recorded under simulation conditions), and (4) learning evidence (AARs with tracked corrective actions and closure). These artifacts shift oversight from inventories and intent statements to verification that critical functions remain executable under stress. This “evidence-first” approach aligns with prolonged care doctrine, emphasizing trend monitoring and documentation when evacuation is delayed. 10
Table 1 summarizes a concept-level, capability-based minimum set. Here, “minimum” is defined as operational functions that must remain reliably executable under constraint rather than a procurement list. The emphasis is on time-bounded first response for postpartum hemorrhage and neonatal transition, infection prevention as a system, training sustainment, and governance. Making these functions auditable through drills, training records, and AAR converts autonomy from aspiration into a readiness standard. The table is therefore intended as a readiness scaffold for evaluating claims of capability, not as an assumption that all listed functions, supplies, or staffing could or would be manifested on an actual Mars transit vehicle or early settlement.
Concept-Level Minimum-Viable Capabilities for Autonomous Birth Care When Evacuation is Impossible (Mars as an Extreme Analog)
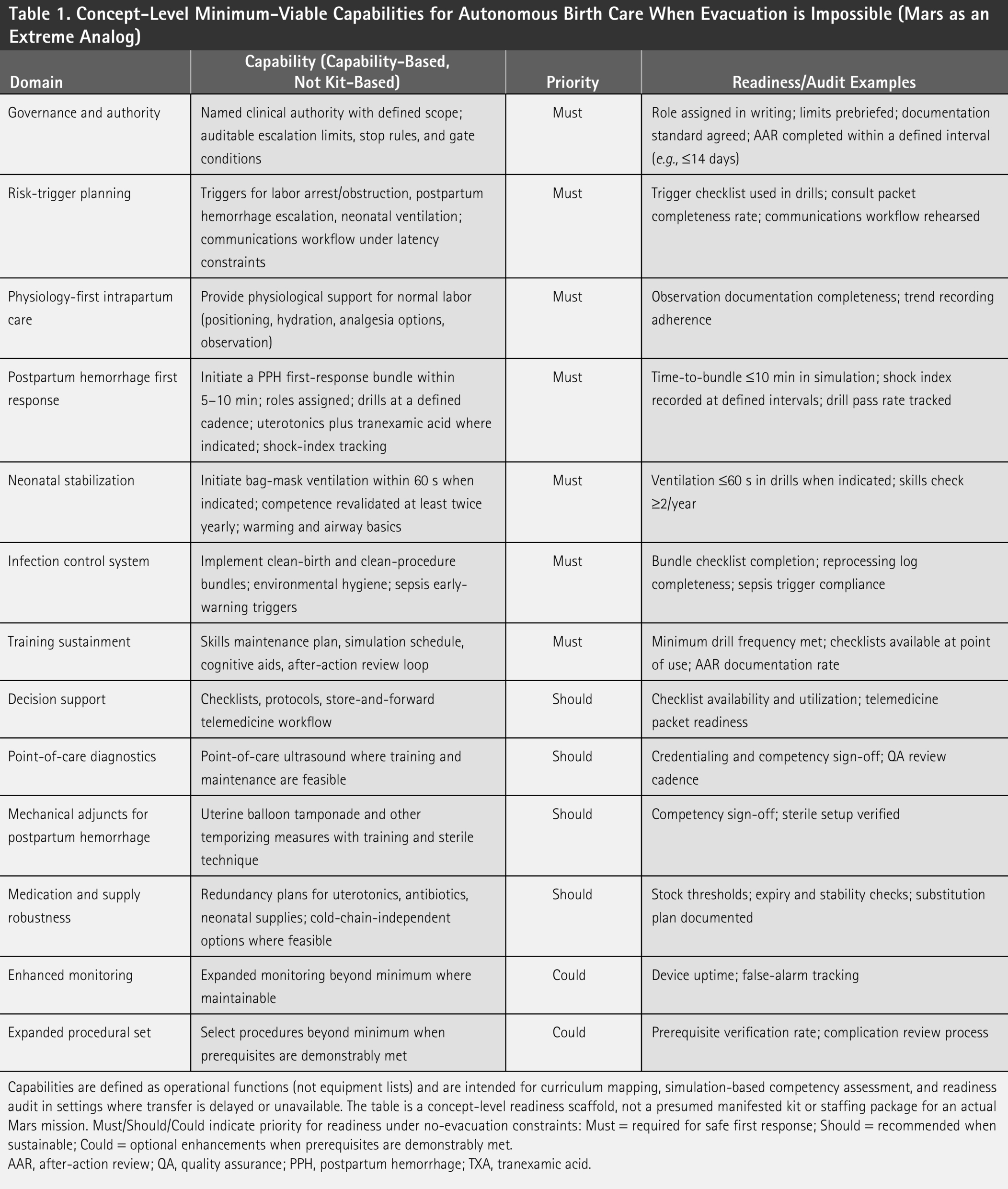
Capabilities are defined as operational functions (not equipment lists) and are intended for curriculum mapping, simulation-based competency assessment, and readiness audit in settings where transfer is delayed or unavailable. The table is a concept-level readiness scaffold, not a presumed manifested kit or staffing package for an actual Mars mission. Must/Should/Could indicate priority for readiness under no-evacuation constraints: Must = required for safe first response; Should = recommended when sustainable; Could = optional enhancements when prerequisites are demonstrably met.
AAR, after-action review; QA, quality assurance; PPH, postpartum hemorrhage; TXA, tranexamic acid.
How to use Table 1 : Operators can treat it as a requirements checklist for training, authority assignment, drills, and documentation evidence. Regulators and standards bodies can use it to specify auditable readiness criteria focused on executable functions rather than broad “capability” claims.
Implementation note (operators and regulators): A practical pathway is to treat the Aerospace Midwife concept as a role-based “minimum medical operations standard” for no-evacuation scenarios. Operators can implement this in three layers: (1) role designation and decision rights (who can declare a stop rule, who can open an escalation pathway), (2) competency package (simulation scenarios for PPH and neonatal ventilation, plus infection-control drills) with pass criteria, and (3) sustainment evidence (drill logs, revalidation cadence, checklist completion, and AAR closure). Regulators and standards bodies can then audit the evidence rather than the narrative: whether gate-condition checklists exist and are used, whether first-response timing targets are met in drills, and whether corrective actions are documented and tracked. This approach reduces the risk of overestimating readiness when prerequisites degrade.
SCOPE AND LIMITATIONS
This perspective addresses low-risk pregnancies and births managed by small teams in environments where time-critical evacuation cannot be assumed; it does not advocate comprehensive operative obstetrics without the ability to sustain perioperative systems. Evidence for human pregnancy, labor, and neonatal transition in partial gravity remains limited; Mars is used here as an extreme constraints analog rather than a direct physiological prediction. 1 Several limitations follow from this framing. First, the proposed minimum-viable capabilities are normative and implementation-oriented: they specify what should be reliably executable under constraint rather than what is currently feasible in any specific organization. They are not a claim that a Mars transit vehicle or early settlement would have sufficient habitable volume, logistics margin, or policy latitude to carry a dedicated obstetric package. Feasibility will vary with workforce composition, scope of practice and licensure, mission rules, manifest trades, supply chains, and local governance, and the table should be interpreted as a readiness target to be adapted and made auditable rather than a universal or immediately deployable standard.3–5 Second, the framework emphasizes reliability and early, time-bounded first response, but it does not resolve clinical scenarios in which definitive care would ordinarily require surgery, transfusion, or intensive monitoring. In no-evacuation settings, ethically defensible limits may be reached earlier than in facility-based care, making prebriefed governance, documentation expectations, and contingency planning essential rather than optional. Finally, external validity depends on the plausibility that “backup” assumptions fail under shock. Disruption to staffing, logistics, and referral pathways during the COVID-19 pandemic and in conflict-affected settings supports this premise and motivates designing care that remains safe when rescue capacity is not reliably available.6–8
CONCLUSION
When evacuation and layered backup are uncertain, autonomous birth care should be treated as a reliability and mission-assurance problem, not a scaled-down version of hospital rescue. The “Aerospace Midwife” concept is proposed as an auditable role-based framework that prioritizes physiology-first care, rapid first response to postpartum hemorrhage and neonatal transition, and enforceable limits on escalation when prerequisites are not sustainable. For Mars-class missions, its primary value is not to assume deployability, but to discipline claims of readiness under severe policy, engineering, and logistics constraints. Three near-term standardization targets follow. First, specify and audit gate conditions for operative escalation (sterility, airway and anesthesia readiness, and postoperative sustainment). Second, train and maintain time-bounded first-response bundles and documentation rules that function under latency, uncertainty, and workload. Third, institutionalize a sustainment loop, including simulation frequency, checklists, training records, and AAR, so that autonomy is a maintained capability rather than an assumption.
AUTHORS’ CONTRIBUTIONS
K.K.: Conceptualization; writing—original draft; and writing—review and editing.
Footnotes
ACKNOWLEDGMENTS
The author is grateful to Mr. Masahiro Ishida, who proposed the idea of space nursing more than two decades ago and inspired the conceptualization of this article.
DECLARATION OF GENERATIVE AI AND AI-ASSISTED TECHNOLOGIES IN THE MANUSCRIPT PREPARATION PROCESS
During the preparation of this article, the author used an AI-assisted language tool to improve readability and organization. The author reviewed and edited the content as needed and takes full responsibility for the content of the published work.
ETHICAL CONSIDERATIONS
Not applicable. This article is a Perspective and does not report new studies involving human participants, human data, human tissue, or animals.
DATA AVAILABILITY
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
AUTHOR DISCLOSURE STATEMENT
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING INFORMATION
The author received no financial support for the research, authorship, and/or publication of this article.