
Abstract
The palatability of oral drugs influences patient adherence to prescribed regimens, especially for children. Various factors influence palatability, including smell, taste, texture, and dose volume. Evaluation of these factors plays an important role in pediatric drug development and is a target for regulatory scrutiny. The Global Alliance for Pediatric Therapeutics, a public–private consortium under the guidance of the Institute for Pediatric Innovation, convened the Alliance Palatability Working Group to discuss the issues related to the assessment of palatability in the development of pediatric oral dosage forms. An extensive scientific literature search was conducted, in addition to a multicompany industry survey and a series of workshops with the Alliance Palatability Working Group. Based on the results, 3 best practice recommendations emerged regarding the assessment of palatability for oral dosage forms in pediatric drug development. These best practice recommendations offer researchers guidance for the preclinical and clinical assessment of palatability of oral dosage forms and serve to operationalize the assessment process within the overall drug development program.
Keywords
Palatability has been identified as 1 of the most crucial factors influencing adherence to therapeutic regimens, with the efficacy of oral drugs in pediatric patients viewed as highly dependent on overall adherence to the prescribed treatment regimen. 1,2 Defined as the overall acceptance of a medication toward its smell, taste, texture, dose volume, and aftertaste, 3 palatability in pediatric patients is directly dependent on a child’s willingness and ability to ingest the product. 4 Although taste masking of medicines for oral use is often used to improve the overall taste of an oral dosage form, a wide variety of factors influence palatability and thus therapeutic acceptance. Evaluation of the factors influencing adherence and palatability in pediatric patients now plays an increasingly important role in the development cycle of new drugs and has become a target for greater regulatory scrutiny. 5
Palatability in Pediatric Drug Development
The goal for pharmaceutical research is the development of a safe, effective, and well-tolerated product that enables compliance throughout the treatment course. There are, however, a number of clinical and practical issues that must be considered in designing the overall drug delivery system. Previous research has highlighted that young children (aged <10 years) often have difficulty swallowing capsules and tablets larger than 10 mm in diameter and may require alternative formulations for drug delivery. 4,6 –8 Although children younger than 7 years have been shown to be able to manage tablets smaller than 10 mm, most are often prescribed oral solutions, chewable tablets, rapidly dispersing tablets, or mini-tablets. 9,10 Drugs that require dosing based on body weight may require formulation as liquid doses, solid doses that are scored, or solid dose development in multiple strengths. However, although liquid formulations facilitate dose titration and offer ease of administration, there are various development constraints related to taste, viscosity, texture, appearance, smell, and dosing accuracy. Stability of the liquid in multiple-dose bottles also must be maintained, often by using stabilizers and preservatives. Taste-masking agents, preservatives, and solubilizing excipients must have an acceptable safety profile in pediatric patients, as well as the ability to improve overall dosage form acceptability.
Similar considerations must be taken into account when the drug development goal is to reformulate a drug currently approved for use in adults for use in pediatric patients. Although many of the formulation steps are similar for development of pediatric and adult drugs, the physical and chemical properties, such as solubility, salt form, stability, and the taste of the active pharmaceutical ingredient (API), must be known or established in pediatric patients. The traditional sources for acceptable excipients, the Generally Regarded as Safe (GRAS) list (ie, 21 CFR Parts 182, 184, and 186) and the Inactive Ingredients Guide from the US Food and Drug Administration (FDA), have all been developed based on data obtained primarily in adults. Investigation into the safety data in the pediatric population available for the potential excipients—although recommended—is not currently required. And although industry best practices suggest that formulation excipients should be chosen based on the physiochemical properties of API and the overall palatability profile of the final proposed formulation, no formal guidance is available.
Palatability is now acknowledged as a critical factor in achieving therapeutic and commercial success for oral dosage forms, especially when the formulation is being developed for use in pediatric patients. Regulatory legislation, including the FDA Safety and Innovation Act (FDASIA), Pediatric Research Equity Act (PREA), and the Best Pharmaceuticals for Children Act (BPCA), have all highlighted the importance of palatability in the compliance among pediatric patients and now require clinical testing to be performed in pediatric patients if specific regulatory labeling is sought. Although electronic taste-sensing systems provide formulation scientists with the ability to rapidly qualify the acceptability of a formulation’s taste and flavor, direct human sensory and palatability assessment—particularly in pediatric populations—is often lacking. The palatability of the API should contribute to the choice of the selected oral dosage form(s) and—unless otherwise justified—the palatability of the pediatric oral dosage form should be seen as satisfactory without requiring crushing or mixing with food or beverages.
Palatability has been traditionally assessed in pharmaceutical drug development by determining the organoleptic properties of the API and other excipients targeted for use in the final finished dosage form. 6 Information regarding the palatability of the API is often acquired at a very early stage in the development process using a combination of quantitative and qualitative assessment measures, including dedicated adult taste-test (sensory) panels, regulatory databases, electronic taste sensing, and available scientific literature. Palatability assessment of the final oral dosage form is rarely assessed during clinical development, 11 with input on palatability and swallowability often limited to patient-reported safety and tolerability outcomes such as gagging and choking. The timing of palatability testing within the overall drug development process of any oral dosage form is, however, variable.
Regulatory and Legislative Considerations
Regulatory and legislative authorities, as well as the World Health Organization, have called for greater understanding of, and research into, the issue of treatment adherence and dosing compliance in pediatric drug development. The US Congress has enacted various legislation to ensure appropriate determination of pediatric applicability and adequate labeling instructions for children, including the FDA Modernization Act of 1997 (FDAMA), BPCA in January 2002 (which provided the innovator a 6-month extension of exclusivity if adequate pediatric studies were performed and allowed FDA to formally request such studies be performed), and the PREA in 2003 (which enabled the FDA to use bridging data from adult studies when approving pediatric medicines). The BPCA and the PREA were further extended and amended by the FDA Amendments Act (FDAAA) of 2007. These 3 acts, in combination with legislation through the Prescription Drug User Fee Act (PDUFA) renewals, encouraged the development of pediatric drugs, making the development of age-appropriate formulations a legal requirement if the drug under development is appropriate for children.
In follow-up to FDAMA, BPCA, and PREA, the FDA announced FDASIA in July 2012, which was designed to assist drug developers by expediting the development and review of new drugs with preliminary clinical evidence that “indicates the drug may offer a substantial improvement over available therapies for patients with serious or life-threatening diseases.” 12 In addition, FDASIA issued a specific industry guidance regarding the development and submission of a dedicated Pediatric Study Plan for compounds targeted for development in pediatric patients. 13 This legislation was in line with the Paediatric Regulation announced in Europe in January 2007, which was designed to aid drug development in children without subjecting them to unnecessary clinical trials or delaying market authorization for use in adults. Comprising 2 separate regulations—Regulation (EC) No 1901/2006 from the European Parliament and Council regarding medicinal products for pediatric use and the amendment Regulation (EC) No 1902/2006 by the European Commission—the objective of the Paediatric Regulation was to improve the health of children in Europe by facilitating the development and availability of medicines for children aged 0 to 17 years by ensuring medicines targeted for use in children are of high quality, ethically researched, and reviewed and authorized appropriately.
Global Alliance for Pediatric Therapeutics
The Global Alliance for Pediatric Therapeutics (the Alliance), a public–private consortium of industry, clinical, and pediatric advocacy groups, was convened in January 2013 by the Institute for Pediatric Innovation to discuss specific issues related to the assessment of palatability in the development of oral dosage forms targeted for pediatric patients. Through a series of workshops with representatives from academic and hospital research, pharmaceutical industry, and industry experts (Alliance Palatability Working Group), 3 primary action steps were agreed on by the Alliance to investigate and address the issue of palatability in pediatric drug development. Step 1. Understand the tools and methodologies used to assess palatability of oral dosage forms in pediatric populations through a comprehensive literature search
14
Step 2. Investigate the current industry practices related to the assessment of palatability and swallowability in pediatric drug development through an Internet-based survey
11
Step 3. Provide recommendations to the pharmaceutical industry on the appropriate assessment of palatability in the development process of oral dosage forms for pediatric patients
Scientific Literature Search
The relationship between acceptance and compliance of oral dosage forms in pediatric populations, and the need for greater research on organoleptic properties, including palatability and swallowability, is well documented in the literature. In the systematic literature review of palatability testing of medicines in children, Davies and Tuleu 15 revealed that from 2002 to 2008 half of the identified studies used a facial hedonic scale (FHS) ranging from 2 to 10 points, with a 5-point scale being the most common. For the remainder of the studies identified, a variety of assessments were used, including rank order assessment, visual analog scale (VAS), Likert-type scale, and verbal descriptive response. Assessment of palatability was conducted in children as young as 3 years and as old as 19, with the parent/caregiver often assisting in studies with younger patients. A follow-up systematic literature review was conducted by Squires and colleagues 14 in 2013. The PubMed, Embase, and CINAHL databases were searched for relevant studies published between January 2008 and March 2013 and restricted to English language. All medical subject heading searches were explored using a Boolean-based keyword search criteria and included the following terms: palatability, taste, swallowability, dosage transit, dosage form transit, dysphagia, organoleptic properties, adherence, treatment adherence, medication adherence, compliance, treatment compliance, medication compliance, concordance, treatment concordance, and medication concordance. The focus of the systematic literature review was to address 2 key issues: (1) what the most recent scientific evidence was regarding the assessment of palatability or swallowability in pediatric drug development and (2) if there was a potential relationship between the assessment of palatability and improved treatment adherence and overall compliance. A total of 137 citations were identified and reviewed as part of the systematic review, with a total of 27 articles highlighting multiple approaches to the evaluation of palatability in pediatric populations. The results of the literature review from 2008 to 2013 identified limited scientific evidence related to the assessment of oral dosage forms in pediatric drug development, despite the reported importance of palatability to therapeutic adherence and compliance. The FHS and 100-mm VAS were the most commonly used tools to assess palatability in pediatric populations as well as in adult taste panels. There was, however, no standardized assessment process or statistical analysis plan. Furthermore, there was limited evidence regarding a potential correlation between treatment adherence and the palatability of oral dosage forms in pediatric patients.
Industry Survey
An in-depth, Internet-based survey of representatives from clinical research and development at major pharmaceutical companies was conducted in March 2013 to research current industry practices for the assessment of palatability and swallowability of pediatric solid dosage forms. 11 The survey was sent to representatives from 21 pharmaceutical companies and was distributed to members of the American Academy of Pediatrics’ Provisional Section on Advances in Therapeutics and Technology 16 through a web-based survey management system. The industry survey was divided into 7 sections: company resource allocation, product development methodology, evaluation of palatability and swallowability, validation and utility of palatability and swallowability scales, target audiences, regulatory environment, and potential for development of a palatability assessment tool. The survey contained 36 multiple-choice questions and allowed for additional open-text input. A total of 10 fully completed survey responses were received from mid- to large-sized pharmaceutical companies, 9 of which were from divisions in the United States. Most participants responded on behalf of a working team, and the majority had been in their current position for at least 5 years. There was no consistent approach among respondents to the assessment of organoleptic properties of solid dosage forms, including excipients. The use of adult taste test panels was divided among respondents, with no utility of pediatric “taste testers.” All respondents agreed that no testing was conducted using placebo formulations, with limited testing for swallowability in any population. The majority of respondents indicated their company had received regulatory requests for a development plan to determine the palatability of an oral dose formulation targeted for pediatric patients. The majority had also received regulatory agreement for a plan to assess pediatric formulation palatability in the last 5 years as part of a Paediatric Investigation Plan (European Medicines Agency [EMA]) or a Pediatric Study Plan (FDA).
In the direct assessment of palatability in pediatric populations, a variety of methods were used across the companies responding to the Internet survey, including simple and complex hedonic scales, numerical and nonnumerical Likert-type scales, VASs, and visual intensity scales. No assessment method identified by any participant was acknowledged as validated or with any statistical correlates, with many stating that scales used in the pharmaceutical industry are adapted from the significant work conducted in the food service industry. Most respondents indicated that they work directly with pediatric subjects, with some also including the parent or caregiver. 11
Key Considerations
Based on the results of the scientific literature review and industry survey, the Alliance Palatability Working Group concluded its preliminary findings by determining that (1) the testing of organoleptic properties of API and excipients are often evaluated by pharmaceutical companies through the use of electronic taste-sensing systems; (2) palatability testing of oral dosage forms does not appear to be consistently performed in pediatric subjects as part of the pediatric drug development process; (3) when palatability is assessed, it is most commonly determined through the use of 1 of 2 unvalidated but widely accepted visual scales; and (4) there is no standard statistical methodology for analyzing results of palatability assessment when using these common scales, or the cross-comparison of results across studies or formulations.
There is a strong clinical rationale for sharing industry-based best practice regarding the assessment of palatability of oral dosage forms targeted for use in pediatric populations, as part of the overall drug development process. Based on the cumulative experience of the members of the Alliance Palatability Working Group, a series of workshops with working group members, and the key findings from the scientific literature search and industry survey, this best practice is designed to address: Recommendations regarding the evaluation process for the assessment of organoleptic properties of active drugs and excipients used in the development of oral dosage forms. Development of a standardized assessment scale for use in the clinical evaluation of palatability in solid dosage forms targeted for pediatric patients. Definition of a standardized statistical methodology for evaluating palatability using the standardized assessment scale in the clinical development of pediatric oral dosage forms.
To ensure consensus in the development of these best practices, additional clinical and drug development input was sought from other key stakeholders outside the Alliance Palatability Working Group, including clinicians, pediatric advocacy organizations, regulatory science experts, and consumer product testing companies. Through a series of focused workgroups, recommendations to address the key findings were identified.
Best Practice Recommendation 1
The use of adult taste test panels, electronic taste-sensing devices, or other assessment methods is recommended for all oral dosage forms targeted for use in pediatric populations during early-stage drug formulation development prior to clinical use in children to assess and evaluate the organoleptic properties of the API and proposed formulation excipients.
Rationale
The early-stage evaluation of organoleptic properties has been internationally recognized by regulatory authorities, academicians, and the pharmaceutical industry as an essential part of drug development in pediatric subjects. Traditional evaluation has used either adult sensory panels (with the extrapolation of test results into pediatric populations) or electronic taste-sensing technology (e-tongues). Laboratory testing is occasionally employed by pharmaceutical stakeholders to determine the chemical parameters known to influence taste/palatability of drug formulations.
Sensory panels are primarily employed when the standard of palatability needs to be established, controlled, or assured. Executed through the use of “expert adult taste testers,” sensory panels have particular advantages and disadvantages that may impact the overall study conclusions. Sensory panel testing can be quicker than most nonsensory methods, with panelists using more than 1 sense, making them more flexible instruments. In addition, sensory panelists can be very sensitive and adroit at detecting minute differences in product characteristics and are able to provide objective and subjective feedback. Sensory panelists can, however, become fatigued with the testing process and the need for descriptive data, and may be subject to biases (eg, from loss of interest or from distractions). Panelists may also not be adept at quantifying perceptions, with the interpretation of results potentially open to conjecture.
Electronic taste-sensing technology provides a technically suitable and cost-effective alternative method for screening APIs and potentially informing candidate selection and identifying a need for further formulation enhancement such as taste masking. The simplicity, speed of analysis, and low sample requirement of electronic taste-sensing devices are 3 items that enable the assessment of organoleptic properties of sweeteners and flavor excipients for taste masking, the quality control of raw materials (including identification level of residual solvents), as well as the stability and consistency of oral formulations. 4 Electronic taste-sensing technology can safely reduce the reliance on human taste panels as well as the potential for subjective bias. Electronic taste-sensing devices do not fatigue like the human tongue (particularly for bitterness). 17 Although “e-tongues” provide advantages of speed, relatively low cost, and lack of risk, several constraints exist that may limit overall clinical utility in determining the ultimate acceptability of a particular pharmaceutical formulation. Electronic taste-sensing devices do not contain biological receptors and so may not adequately report bitterness. 18 Similarly, sensory devices utilize normative values to identify sensory extremes and may not truly identify perceptions and preferences associated with human senses. Finally, electronic sensing devices are unable to provide qualitative feedback on physical characteristics related to palatability and swallowability, such as dry mouth, aftertaste, indigestion, or nausea.
Independent of specific testing procedure, the Alliance Palatability Working Group recommends the evaluation of organoleptic properties prior to clinical testing in children to understand any potential issues related to palatability for APIs.
Project Management Approach
No operational standards have been established related to the timing for the use of adult taste test panels or electronic taste-sensing devices in pharmaceutical drug development. Lorenz et al, 7 in their evaluation of the utility of taste-sensing devices in formulation development, outlined a decision tree for the potential utility of electronic taste-sensing devices into the overall drug development program (Figure 1). The Alliance Palatability Working Group recommends the use of a similar decision tree in the early-stage development of an API to guide the development of an appropriate oral dosage form prior to clinical testing in pediatric subjects.
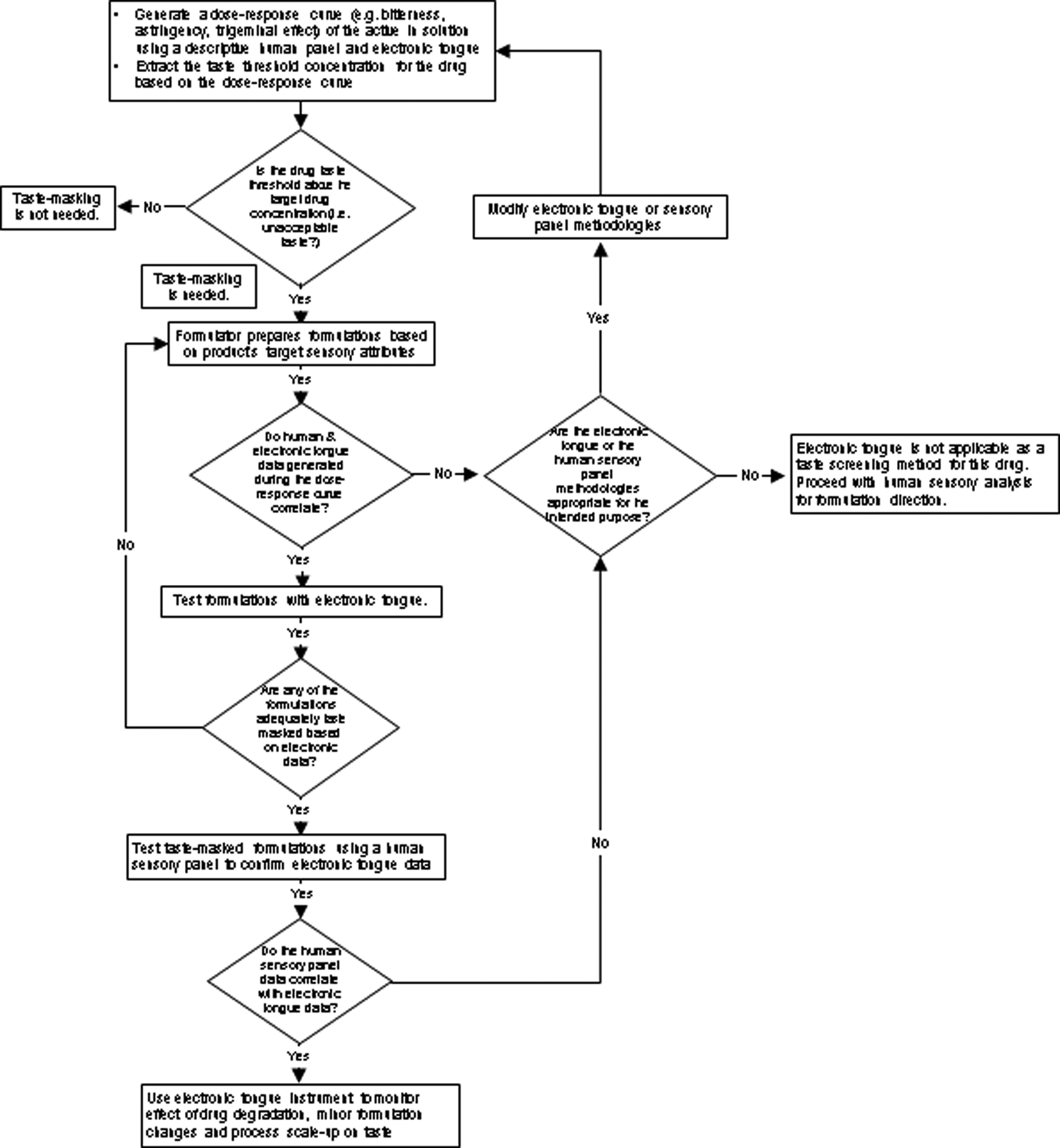
The project management approach to the assessment of the organoleptic properties of active pharmaceutical ingredients in pediatric oral dosage forms. Image reprinted with permission from Lorenz et al. 7
Best Practice Recommendation 2
The use of a visual assessment scale that utilizes hedonic and analog characteristics is recommended to comparatively assess the palatability of oral dosage forms targeted for use in pediatric populations. Specifically, recommendations are given for the use of a horizontal visual assessment scale, the FHS/VAS-5 (Figure 2), which directly incorporates a facial hedonic scale and a 100-point visual analog scale. In addition, the hedonic scale utilizes 5 faces for all ages.
Five-point facial hedonic scale with a correlated 100-point visual analog scale (FHS/VAS-5) for use in children aged 4 to 18 years.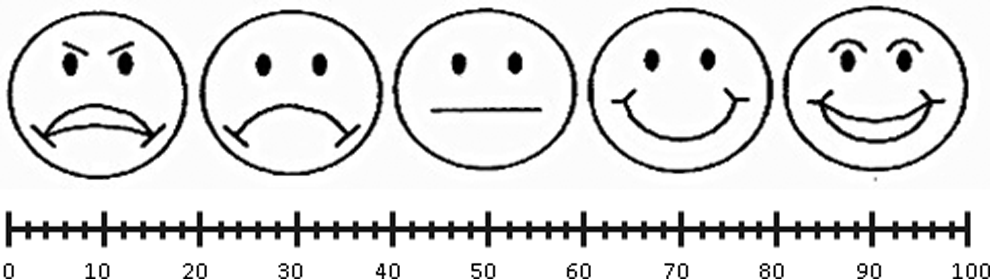
Rationale
The hedonic scale, also known as degree-of-liking scale, is the most common scale for measuring product liking in the food technology industry. Extensive research in the 1950s 19 –21 revealed that scales with up to 9 intervals were more discriminating than shorter, “yes/no” scales. The hedonic scale is based on equal interval assessment, which is important in the assignment of numerical values to the response choices and to the use of parametric statistics in analysis of the data. To assist in evaluation, hedonic scales may also be labeled (“like extremely,” “like very much,” “like slightly,” “neutral,” etc), use visual cues (simple faces, complex faces, figures, etc), or use a combination of both visual and labeled cues.
Although 7-, 9-, and 11-point hedonic assessment scales have proven successful in evaluating preference and acceptability in adult subjects, these longer hedonic scales may be time-consuming—especially when used in comparative assessment. Children should be treated as a special population, however, and the appropriate testing environment and protocol must be used because children show a wide range of cognitive abilities and attention spans. Recent investigation into the age-appropriateness of hedonic scales suggests that the scales that use a smaller number of visual cues are more clinically relevant in pediatric patients, 22 confirming that children as young as 4 years are able to use a 5-point hedonic scale. 15
The Alliance Palatability Working Group recommends the use of a 5-face FHS to assess general palatability in all children aged 4 to 18 years. If required, the Alliance suggests the use of specific verbal cues (such as “very bad,” “bad,” “not okay,” “neither good or bad,” “okay,” “good,” and “very good”) to assist in the determination of overall palatability and to assist in clarification. Furthermore, the Alliance recommends that these specific verbal cues be used only when the test subject is unable to make an immediate correlation to 1 of the visual indicators of overall palatability.
The use of a VAS is common in psychometric evaluation of subjective characteristics or attitudes that cannot be directly measured. When responding to a question through a VAS, the respondent specifies their level of agreement to a statement by marking a position along a continuous line. The analog (or continuous) nature of the scale differentiates it from discrete scales (such as the Likert-type scale) where “in-between” answers are not permitted. There is evidence showing that VASs have superior metrical characteristics than do discrete scales, allowing a wider range of statistical methods to be applied. 23 Furthermore, the use of numeric quantifier obviates the need for subsequent measurement. Although limitations have been noted regarding the ability of pediatric patients to accurately and consistently identify change on a VAS over a specified time course, its utility at a single time point assessment has been well documented. 24,25
When used in combination, the facial hedonic and visual analog aspects are expected to provide a complementary response regarding the assessment of palatability. Laslett et al 26 directly compared the clinical utility of a visual pain scale with a 100-mm VAS in the measurement of pain intensity in adult patients. The investigators concluded that the 2 methods are not interchangeable and are best used in combination when subject to direct and comparative assessment. 26
In providing its recommendation, the Alliance Palatability Working Group recommends modifying the design of the traditional 100-mm VAS, which was most commonly used to assess palatability, by utilizing a 100-point linear VAS, with point 0 aligning with the extreme left of the facial prompt used in the FHS and point 100 aligning with the extreme right of the FHS. This change is expected to alleviate many of the limitations identified when using the FHS or VAS independently.
Proposed Assessment Methodology for the FHS/VAS-5
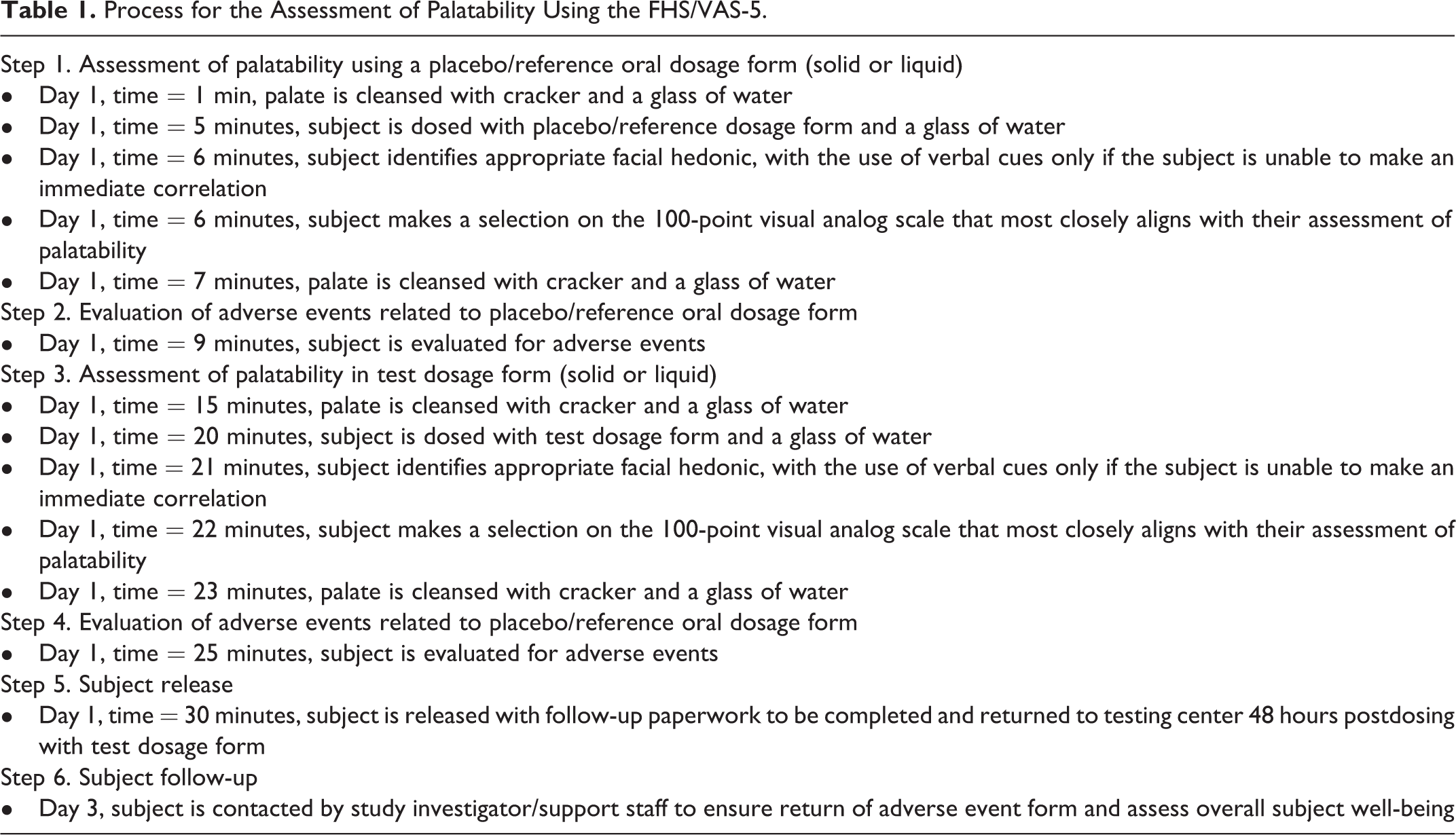
Based on the currently available scientific literature and feedback from the industry survey, the Alliance proposes that the palatability assessment of oral formulations be conducted in a single visit over a 30-minute test period, with follow-up on day 3 to assess any potential adverse event or issues related to palatability (Table 1). Any adverse events reported that are not directly related to palatability should be reported to the study sponsor as directed by their adverse event reporting instructions.
Process for the Assessment of Palatability Using the FHS/VAS-5.
Project Management Approach to the Assessment of Palatability
No formal regulatory timelines or operational standards have been established by the FDA or EMA regarding the specific assessment of palatability of oral dosage forms in pediatric drug development. Based on the findings of the literature search, industry survey, and cumulative professional experience of members of the Alliance Palatability Working Group, the Global Alliance for Pediatric Therapeutics recommends consideration of palatability assessment during phase 2 drug development or at an appropriate time to ensure a palatable oral dosage form is developed and available prior to large-scale, phase 3 testing in children, which is likely to take place after phase 3 testing in adults. Specifically, the Alliance recommends that palatability assessment use an assessment scale such as the FHS/VAS-5.
The Alliance recommends that in addition to early palatability clinical assessment in children, compliance and adherence be evaluated during phase 3 clinical development in the targeted pediatric population. This assessment should provide greater insight into potential issues related to convenience, adherence, and compliance—addressing the overall goal of palatability testing. Specifically, the Alliance suggests an ongoing mechanism to monitor compliance and adherence during phase 3 clinical testing, the point at which the pediatric patient is most susceptible to issues related to dosage form palatability and swallowability. 27 Evaluating and tracking compliance and adherence will provide investigators with salient clinical information useful in drug development, including the role of swallowability and palatability in dosage form acceptance.
No recommendations or guidance are provided regarding the target population for involvement in the assessment of the palatability of oral dosage forms. Although the Alliance strongly supports the assessment of palatability in pediatric patients, we acknowledge the clinical utility of adult taste panels and the potential appropriateness of using such panels in lieu of pediatric subjects.
Best Practice Recommendation 3
The use of a standardized statistical assessment protocol is recommended to directly and comparatively assess the palatability of oral dosage forms in pediatric clinical trials.
Proposed Statistical Methodology
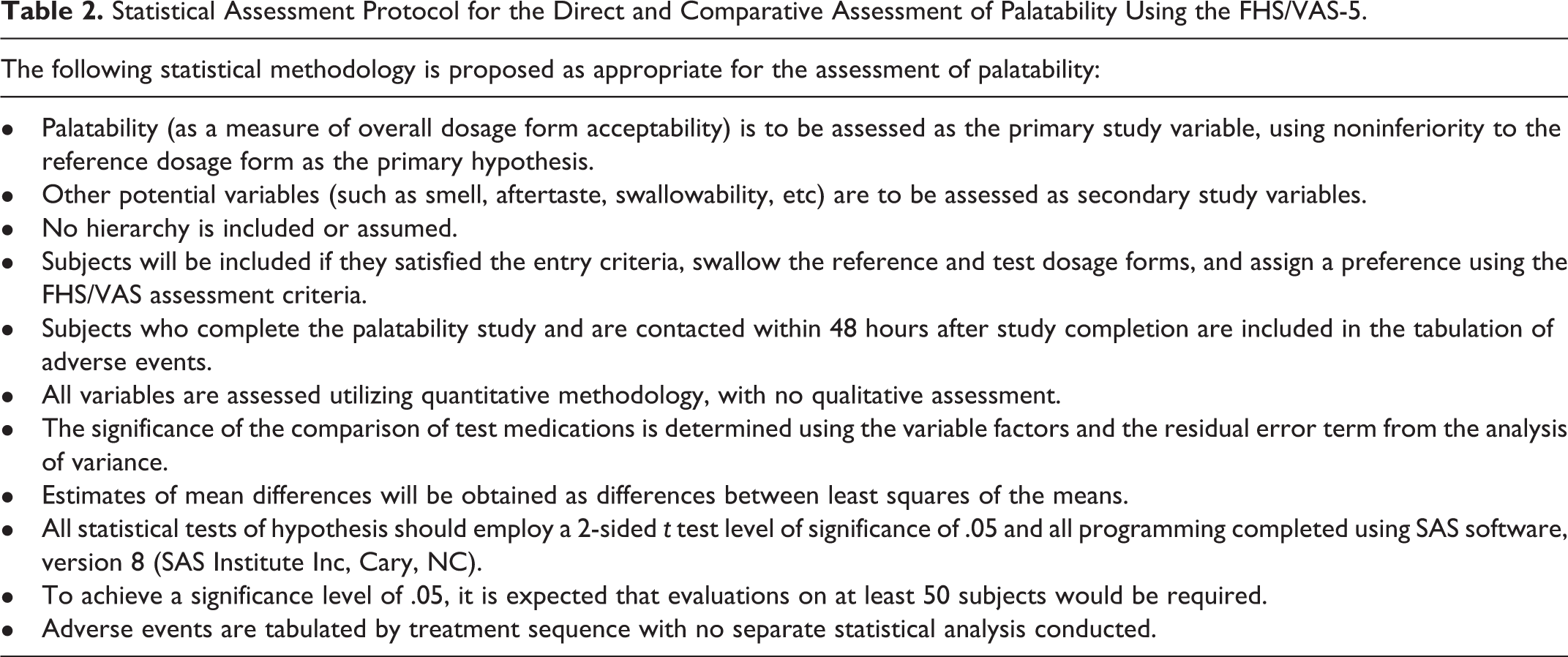
To directly compare and contrast palatability using the FHS/VAS scale, an appropriate statistical analysis plan should be developed to enable the direct and comparative assessment of the test oral dosage form to a reference dosage form (Table 2).
Statistical Assessment Protocol for the Direct and Comparative Assessment of Palatability Using the FHS/VAS-5.
Visualization of Palatability Assessment Using the FHS/VHS
It is suggested that 2 standardized graphics visualizations be used to display statistical results of palatability assessment using the FHS/VHS. To directly compare and contrast the palatability of the test oral dosage form to a reference dosage form, a horizontal, grouped bar chart using the 2 independent variables is proposed. This chart would report the mean scores for each item of the FHS for the reference and test dosage forms (Figure 3). The Alliance proposes the use of a forest plot to visualize the direct assessment of palatability, where least-squared mean scores of the 100-point VAS are plotted with the 95% confidence interval. No weighting of the mean score is proposed, but may be used when large study populations are used (Figure 4). The use of a forest plot for visualization of the comparative assessment of palatability is also proposed, where the test oral dosage form and a reference dosage form are compared using the 100-point VAS (Figure 5). Least-squared mean difference scores are plotted, along with the 95% confidence interval, with no weighting of the mean score. Alternatively, if assessment of palatability is being conducted in an open-label clinical trial design, it may be appropriate to comparatively assess palatability and swallowability using an odds ratio with 95% confidence intervals.
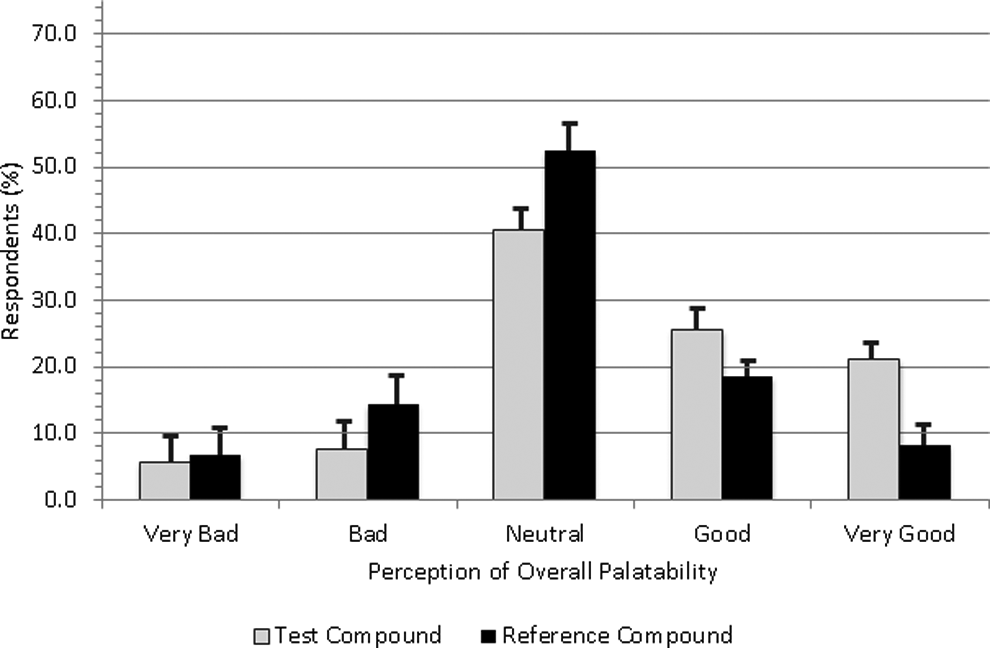
Proposed visual depiction of direct evaluation of palatability based on the visual hedonic scale subscale.
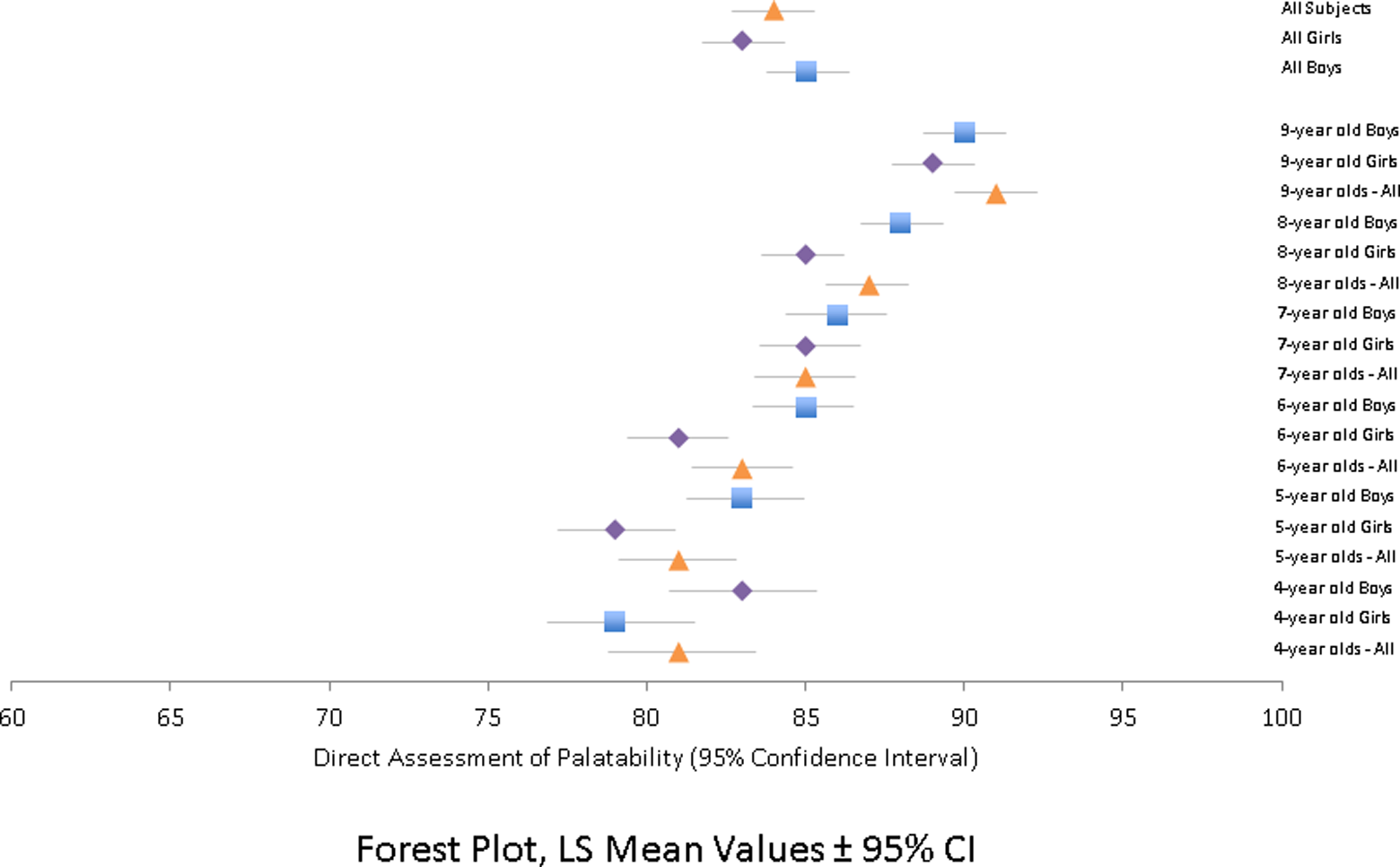
Proposed visual depiction of direct assessment of palatability based on mean score on the 100-point visual analog scale subscale.
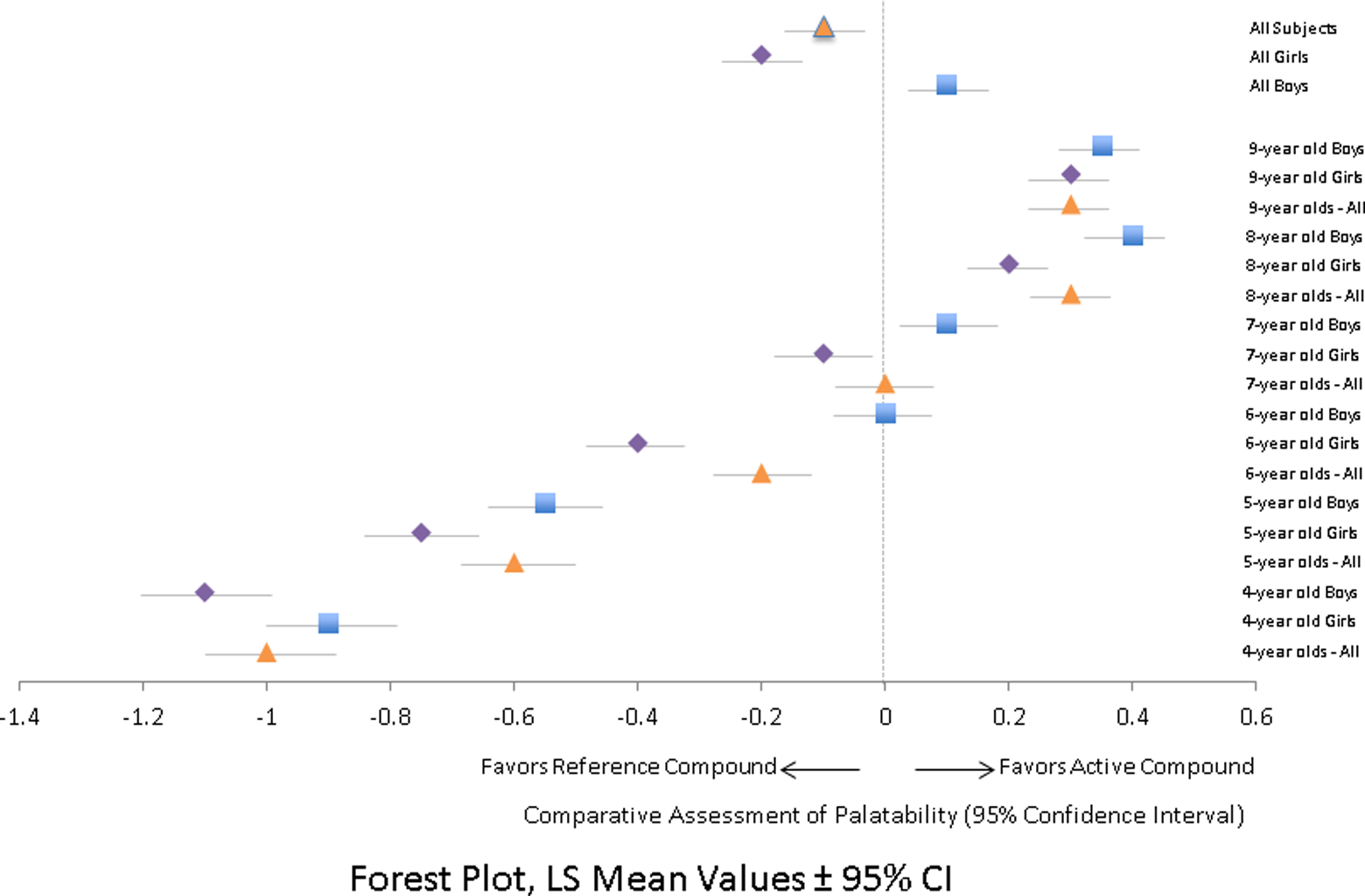
Proposed visual depiction of comparative assessment of palatability based on mean difference on the 100-point visual analog scale subscale.
Timing for Palatability Assessment Within the Overall Drug Development Timeline for Oral Dosage Forms Targeted for Pediatric Populations
The project timelines for the pharmaceutical drug development differ significantly between manufacturers. However, the FDA has established a standardized operational procedure for its interactions with the pharmaceutical industry during drug development. To assist in regulatory discussions, the Alliance Palatability Working Group has developed a proposed case report form for the FHS/VAS-5 (Figure 6; also available for download at http://pediatricinnovation.org/publications) and proposes that palatability assessment be incorporated into the overall drug development process, including: Assessment of API palatability through the use of adult taste test panels or electronic taste-sensing technology after the Pre-IND Meeting, to ensure that API palatability data can be included in the IND Submission (if required). Direct, single-dose palatability and swallowability assessment of the oral dosage form during phase 2 clinical development in children to ensure that issues related to palatability and swallowability will not impact adherence or compliance in phase 3 pediatric clinical trials. Documentation of compliance/adherence of the oral dosage form during large-scale phase 3 clinical development in the target pediatric population, along with patient-reported safety and tolerability.
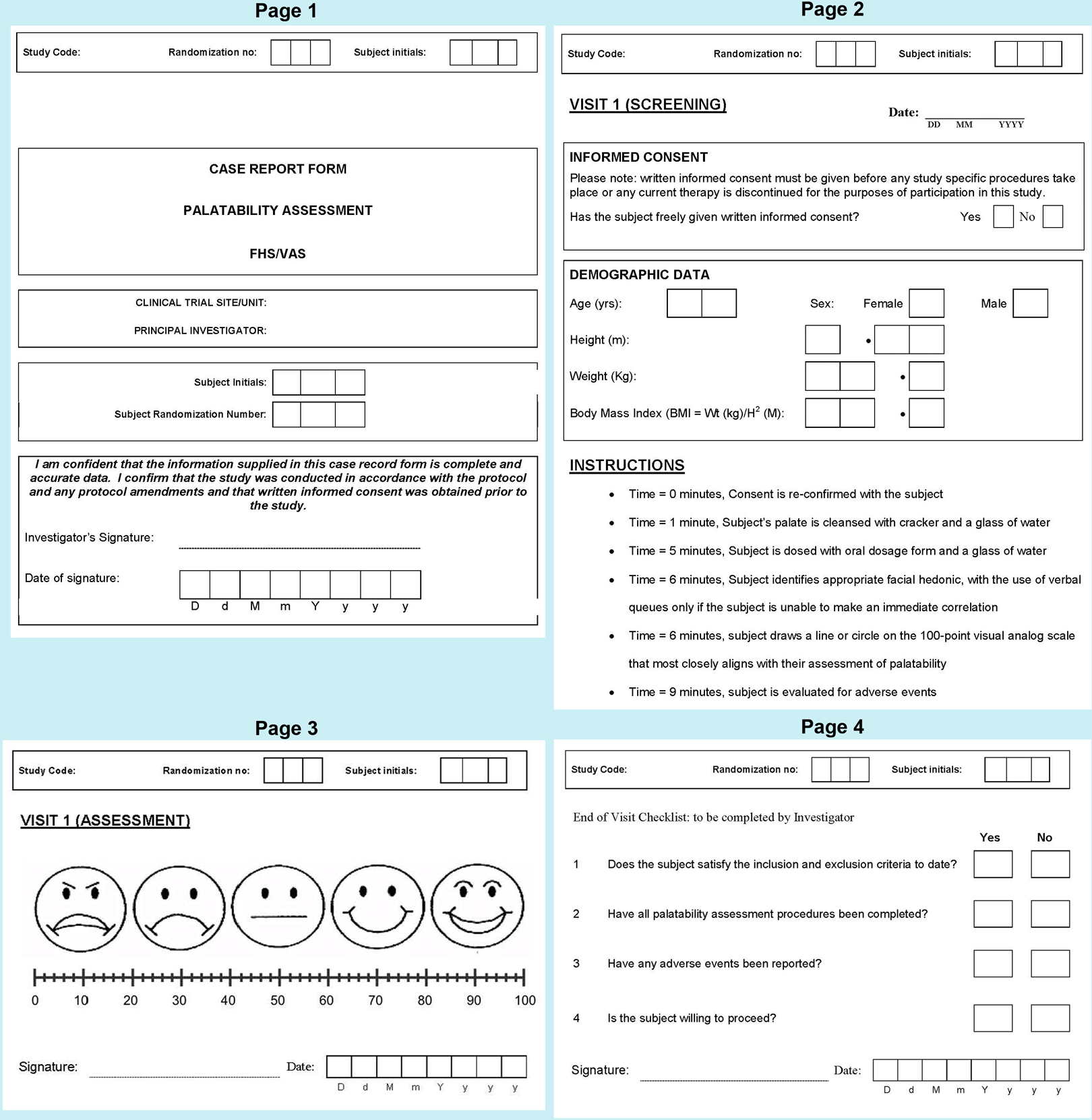
Proposed case report form for the facial hedonic scale.
Conclusions
Based on the results of the scientific literature search, multicompany industry survey, the expertise of the members of the Alliance Palatability Working Group, and a series of focused working group sessions, 3 best practice recommendations have been made regarding the assessment of palatability in the development of oral dosage forms in pediatric drug development. In providing these best practice recommendations, the Alliance hopes to offer industry and researchers a suite of best practice suggestions for the preclinical and clinical assessment of palatability of oral dosage forms, as well as operationalize the overall assessment process within the drug development program.
Footnotes
Acknowledgments
The authors thank the members of the Global Alliance on Pediatric Therapeutics, especially Scott Herbig, Ron Portman, Daniel Schaufelberger, Robert Ternik, and Laura Trespedi, for their valuable insight and direction into the development and implementation of the industry survey. The authors wish to acknowledge the clinical expertise, guidance, and consultancy of the members of the Alliance Palatability Working Group, including Melodi McNeil and Mei Khong (AbbVie); Katie Murray, Gary Noel, and Jeffrey Skolnik (AstraZeneca); Ronald Portman (Bristol-Myers Squibb); Allen Albert and Robert Ternik (Eli Lilly & Company); Samuel Maldonado, Daniel Schaufelberger, and William Treem (Janssen LLC); Tracy Gaebele (Merck); Christina Bucci-Rechtweg (Novartis US); Gesine Winzenburg (Novartis Pharma HG); Scott Herbig (Pfizer); Deborah Steiner (Purdue Pharma); and Laura Trespedi (Shire). In addition, the authors thank The Medicine Group for coordinating the survey, as well as for editorial assistance.
Declaration of Conflicting Interests
CT is a full-time employee of, and holds stock in, Pfizer Inc. DL is a full-time employee of the Institute for Pediatric Innovation. PS is a consultant to the Institute for Pediatric Innovation. LS is a full-time employee of, and holds stock in, Shire LLC.
Funding
The industry survey was sponsored by the Global Alliance for Pediatric Therapeutics, a public–private consortium of industry, clinical, and pediatric advocacy groups convened by the Institute for Pediatric Innovation, which has received membership fees from Shire LLC and Pfizer Inc and small grants from Eli Lilly, Janssen, and Bristol-Myers Squibb.