
Abstract
Study Design/Setting
Prospective cohort study.
Objectives
To test whether the novel Forgotten Spine Surgery Score-Cervical (FS3-C) better differentiates outcomes between motion-preserving cervical disc replacement (CDR) and fusion via anterior cervical discectomy and fusion (ACDF) compared with the NDI.
Methods
The FS3-C was derived from a 20-item pool and reduced to 12 items after pilot testing in 41 CDR patients. Validation cohorts included 127 CDR and 112 ACDF patients who completed FS3-C and NDI. Internal consistency, ceiling/floor effects, and convergent validity were assessed. Group comparisons used appropriate parametric and nonparametric tests. Multivariable linear regression adjusting for age, Charlson Comorbidity Index, sex, and number of operated levels, as well as propensity score matching, were performed to address baseline differences.
Results
A total of 239 patients were included. Cronbach α was 0.95 (FS3-C) and 0.88 (NDI). FS3-C correlated inversely with NDI (r = −0.606, P < 0.001). Mean FS3-C was higher after CDR (59.9 ± 19.6) than ACDF (53.2 ± 22.2; P = 0.012), while NDI did not differ (P = 0.074). In multivariable analysis, CDR remained independently associated with higher FS3-C scores (β = 8.94, P = 0.009), with no association for NDI (P = 0.239). Propensity-matched analysis yielded consistent results (mean difference 9.22, P = 0.008), while NDI remained nonsignificant (P = 0.289).
Conclusions
The FS3-C detected differences between CDR and ACDF not detected by the NDI. Findings were consistent across adjusted and propensity-matched analyses, supporting its strong performance and greater discriminatory capacity as a cervical spine PROM.
Introduction
Patient-reported outcome measures (PROMs) anchor contemporary spine surgery research and quality improvement. The widely used Neck Disability Index (NDI) captures pain and function but not the degree to which an operated spinal segment fades from the patient’s awareness. In total joint arthroplasty, this concept, “joint forgetting”, is quantified by the Forgotten Joint Score (FJS), a 12-item instrument that shows excellent validity, reliability and reduced ceiling effects compared with legacy hip and knee scores.1-4 The term “forgotten” refers to joint awareness rather than absence of symptoms, and reflects a patient’s ability to perform activities without conscious perception of the operated segment.
Motion-preserving cervical disc replacement (CDR) and motion-eliminating anterior cervical discectomy and fusion (ACDF) address similar radiculopathic and myelopathic pathologies yet differ biomechanically. Randomized and prospective studies demonstrate that CDR maintains range of motion, lowers adjacent-segment degeneration and produces equal or better long-term pain relief than ACDF.5-8 Standard neck PROMs, however, often fail to distinguish the patient experience of these procedures due to limited responsiveness, ceiling effects, and minimal sensitivity to differences in motion or proprioception.9-13
To bridge this gap, we adapted the FJS framework to create the Forgotten Spine Surgery Score-Cervical (FS3-C) and, in Part 1 of this project, verified its reliability, validity and responsiveness in a cervical cohort. 14 The present report (Part 2) compares FS3-C outcomes between CDR and ACDF. We hypothesized (1) that CDR patients would report higher FS3-C scores than ACDF patients and (2) that the FS3-C would demonstrate greater discriminatory capacity than the NDI.
Methods
Study Design and Patient Selection
This prospective study included all patients who underwent primary, one- or two-level cervical disc replacement (CDR) or anterior cervical discectomy and fusion (ACDF) at a single academic center between 2017 and 2023. Patients were eligible if they completed a minimum 3-month follow-up survey. Procedures involving three levels, revision of a CDR implant, or hybrid CDR–ACDF constructs were excluded.
Questionnaire Development (Pilot Phase)
A candidate pool of twenty items was generated through literature review and expert consensus to capture activities relevant to the typical cervical-spine population. The pilot questionnaire was administered to an initial CDR cohort. Item selection relied on three metrics: internal consistency expressed as Cronbach α, the proportion of missing responses for each item, and distribution of response categories. Twelve items that satisfied these criteria were retained, producing the final Forgotten Spine Surgery Score-Cervical (FS3-C).
Validation Cohorts and Survey Administration
The CDR validation cohort subsequently completed both the FS3-C and the Neck Disability Index (NDI). An independent ACDF validation cohort then completed the same two instruments. All surveys were delivered electronically via REDCap or, when necessary, by structured telephone interview.
Scoring Procedure
FS3-C scores were calculated by summing raw item responses, dividing by the number of completed items, multiplying the result by 25, and subtracting that value from 100, yielding a scale from 0 to 100. Higher scores reflect superior outcomes, indicating a greater degree of “forgetting” the operated segment. In contrast, higher NDI scores represent worse disability. Ceiling effects were defined as the proportion of patients achieving the best possible score, whereas floor effects represented the proportion scoring the worst possible value.
Statistical Analysis
Continuous data are presented as means with standard deviations and ranges; categorical data are presented as counts and percentages. Item-level and scale-level ceiling and floor effects are reported as percentages. Normality of continuous variables was assessed before hypothesis testing. Independent-sample t tests were applied to normally distributed variables, and the Wilcoxon rank-sum test was used for non-parametric data. Convergent validity of the FS3-C was examined by calculating Pearson correlation coefficients between FS3-C and NDI scores. All tests were two-sided, and a P value less than 0.05 was considered statistically significant.
To account for baseline differences between cohorts, we performed multivariable linear regression with FS3-C as the dependent variable. Independent variables included procedure type (CDR vs ACDF), age, Charlson Comorbidity Index (CCI), sex, and number of operated levels. A parallel model was constructed using NDI as the dependent variable for comparison. All variables were entered simultaneously into the model, and statistical significance was defined as P < 0.05.
To further address potential baseline differences and provide a complementary analysis, propensity score matching was performed. A logistic regression model estimated each patient’s probability of undergoing CDR (vs ACDF) based on age, Charlson Comorbidity Index, sex, and number of operated levels. One-to-one nearest-neighbor matching without replacement was performed using a caliper of 0.5 standard deviations of the logit of the propensity score, yielding 50 matched pairs (N = 100). Covariate balance was assessed using standardized mean differences (SMDs), with SMD <0.20 considered adequate. Outcomes were compared between matched groups using paired t-tests, with Wilcoxon signed-rank tests as a non-parametric sensitivity check. All statistical analyses were performed in Python (Python Software Foundation), using the pandas, NumPy, SciPy, and statsmodels libraries.
Results
Baseline Demographics of Cohorts
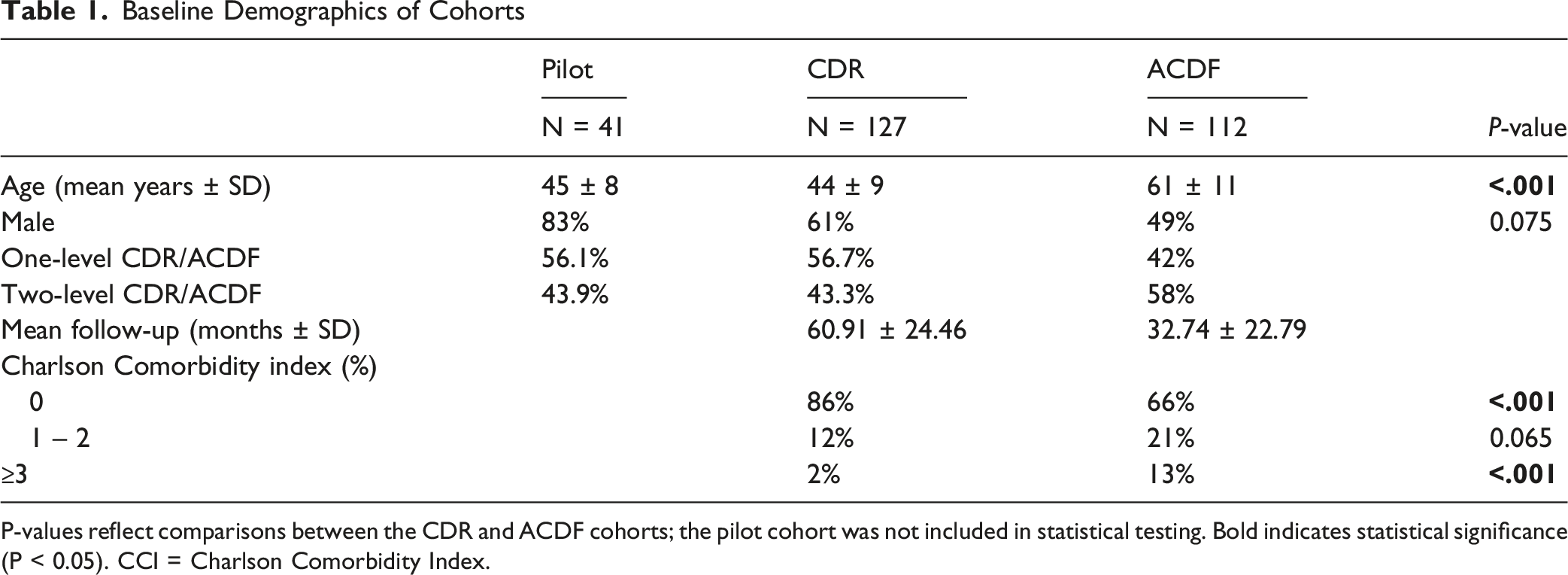
P-values reflect comparisons between the CDR and ACDF cohorts; the pilot cohort was not included in statistical testing. Bold indicates statistical significance (P < 0.05). CCI = Charlson Comorbidity Index.
Psychometric Properties of the 20-Item Pilot Survey
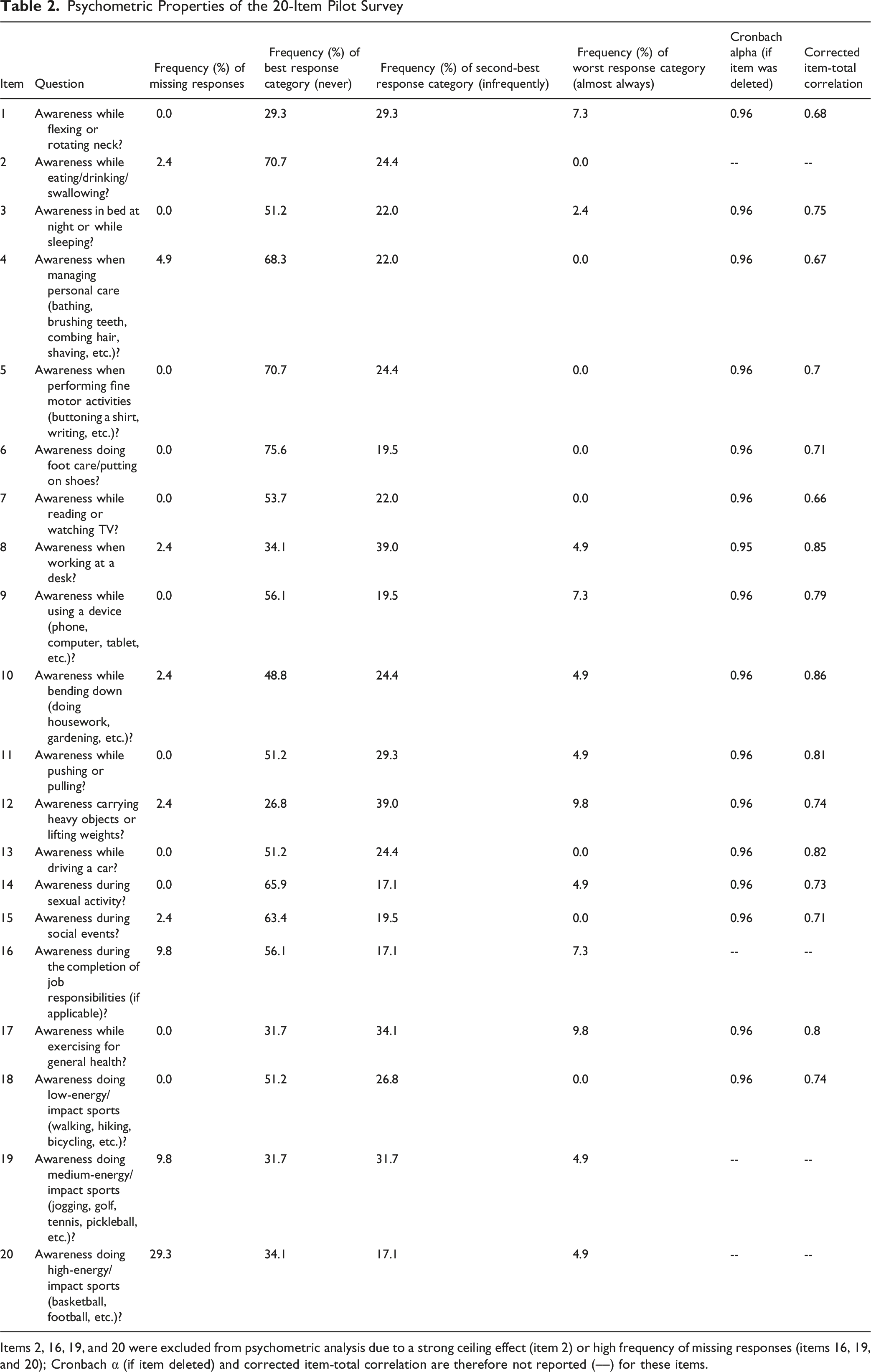
Items 2, 16, 19, and 20 were excluded from psychometric analysis due to a strong ceiling effect (item 2) or high frequency of missing responses (items 16, 19, and 20); Cronbach α (if item deleted) and corrected item-total correlation are therefore not reported (––) for these items.
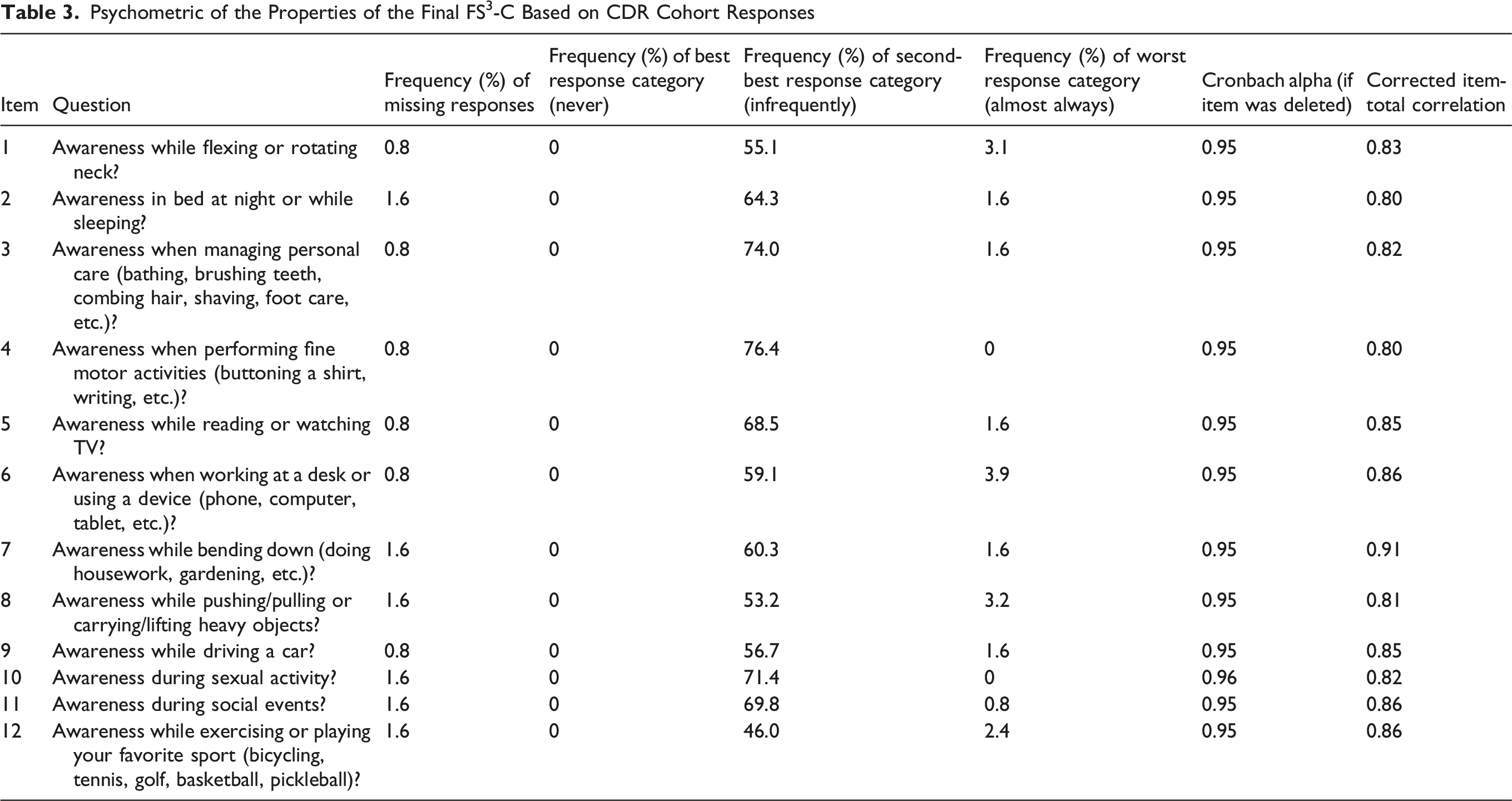
Psychometric of the Properties of the Final FS 3 -C Based on CDR Cohort Responses
Psychometric of the Properties of the Final FS 3 -C Based on ACDF Cohort Responses
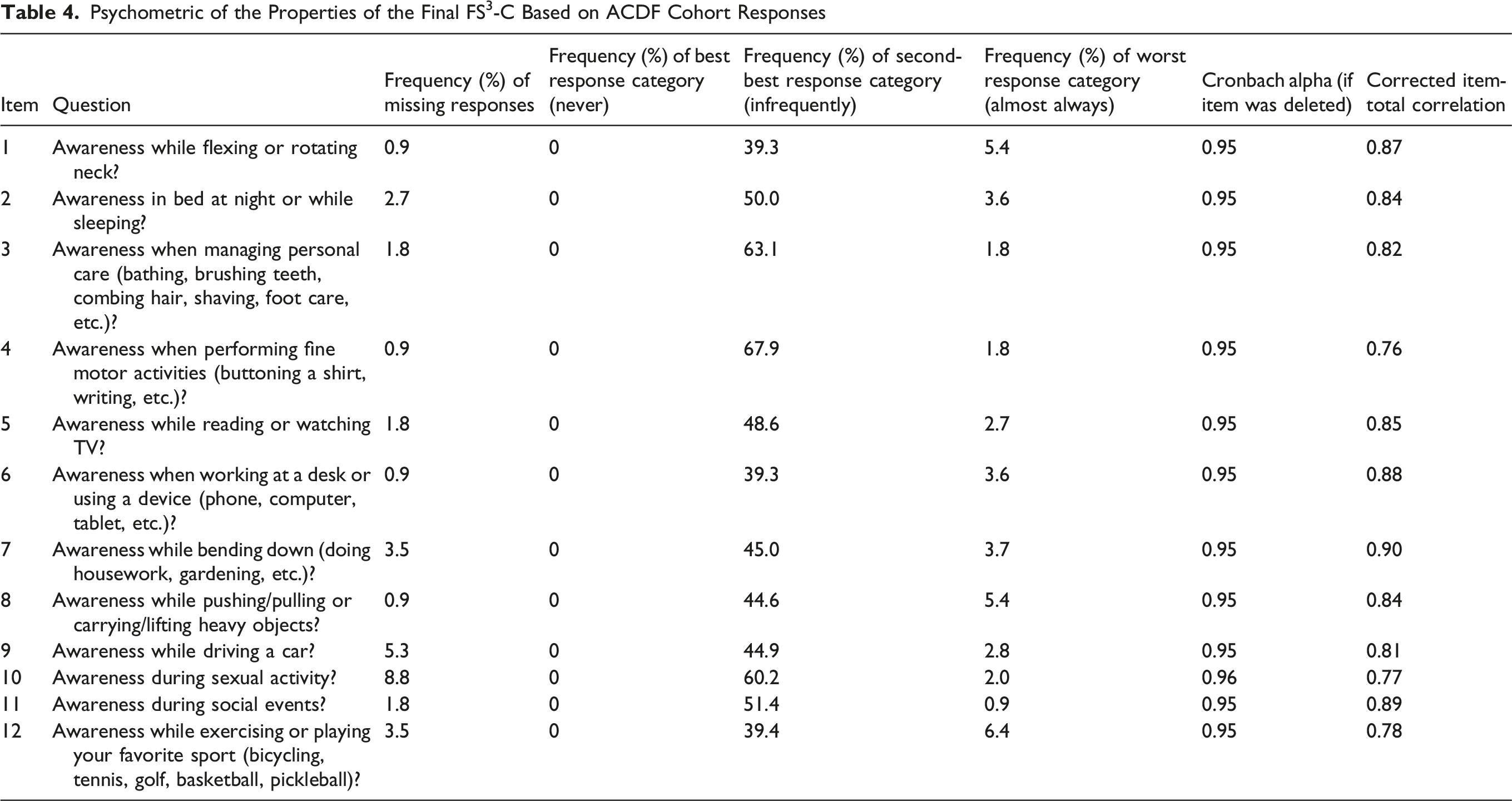
The average item-deleted Cronbach’s alpha was 0.88 for the NDI and 0.95 for the FS3-C. The average NDI scores for the CDR and ACDF cohorts were 5.2 ± 6.2 and 6.3 ± 6.2, respectively (P = 0.074). The average FS3-C score was 59.9 ± 19.6 for the CDR cohort and 53.2 ± 22.2 for the ACDF cohort (P = 0.012). The effect size between the CDR and ACDF cohorts was 0.17 for the NDI and 0.33 for the FS3-C.
Multivariable Linear Regression Results for FS3-C and NDI Outcomes
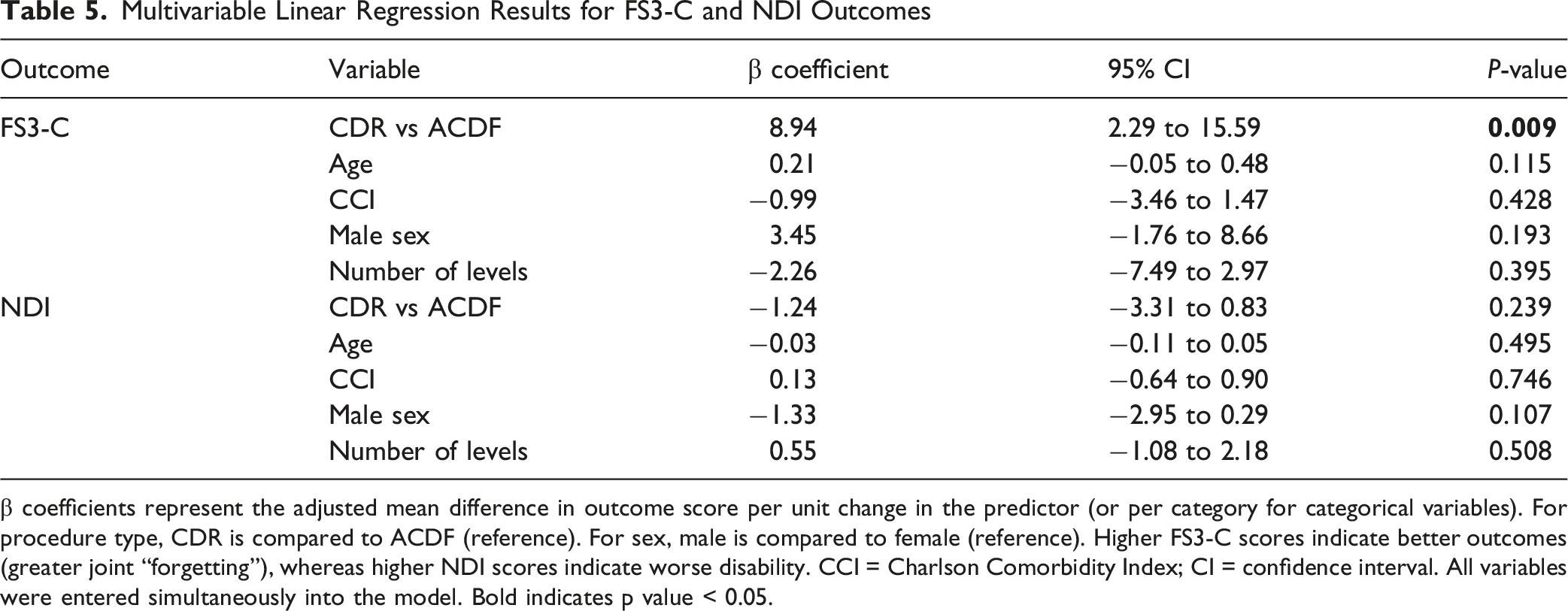
β coefficients represent the adjusted mean difference in outcome score per unit change in the predictor (or per category for categorical variables). For procedure type, CDR is compared to ACDF (reference). For sex, male is compared to female (reference). Higher FS3-C scores indicate better outcomes (greater joint “forgetting”), whereas higher NDI scores indicate worse disability. CCI = Charlson Comorbidity Index; CI = confidence interval. All variables were entered simultaneously into the model. Bold indicates p value < 0.05.
Baseline Characteristics before and after Propensity Score Matching
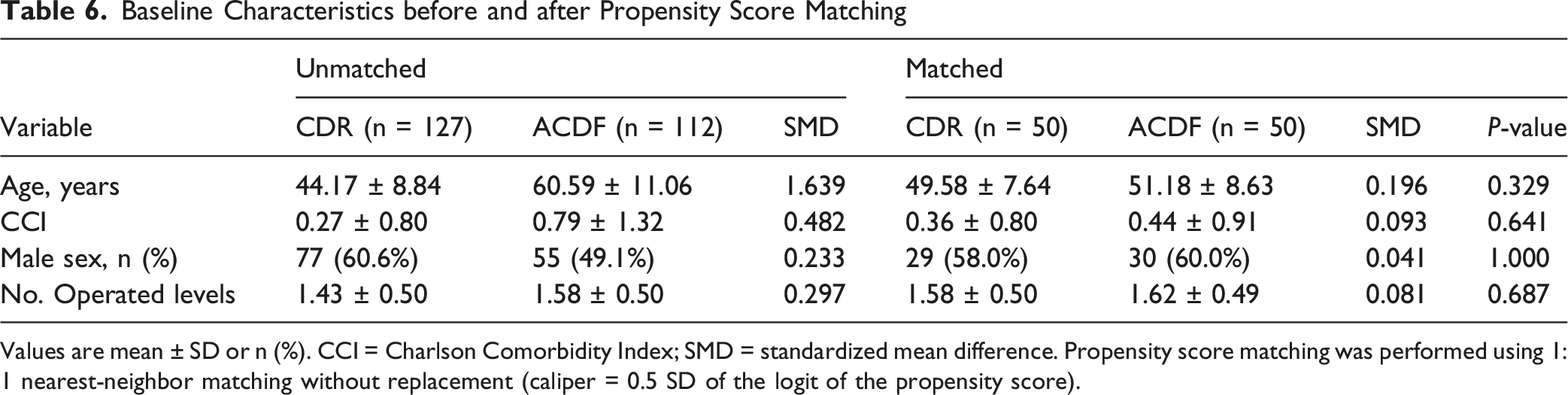
Values are mean ± SD or n (%). CCI = Charlson Comorbidity Index; SMD = standardized mean difference. Propensity score matching was performed using 1:1 nearest-neighbor matching without replacement (caliper = 0.5 SD of the logit of the propensity score).
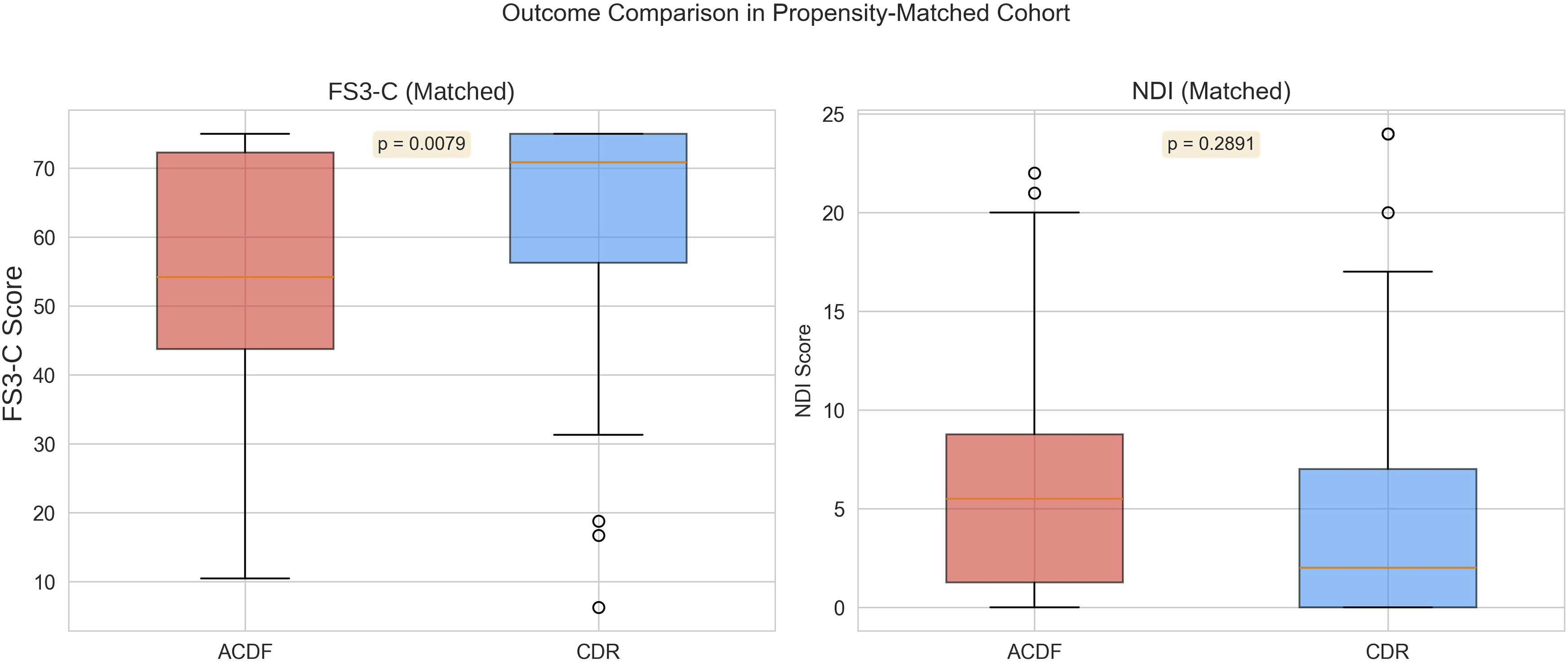
Outcome comparison between cervical disc replacement (CDR) and anterior cervical discectomy and fusion (ACDF) in the propensity-matched cohort (n = 50 pairs). Box plots display the median (orange line), interquartile range (box), and 1.5× IQR (whiskers), with outliers shown as open circles. The Forgotten Spine Surgery Score-Cervical (FS3-C), transformed to a 0–100 scale, was significantly higher in the CDR group than the ACDF group (p = 0.0079), indicating greater joint awareness “forgetting” following motion-preserving surgery. Neck Disability Index (NDI) scores did not differ significantly between groups (p = 0.2891).
Discussion
This prospective cohort study is the first to apply a joint-awareness construct to a head-to-head comparison of motion preservation and fusion in the cervical spine. Patients who underwent CDR reported Forgotten Spine Surgery Score-Cervical (FS3-C) values that were 6.7 and 9.2 points higher than those of patients treated with ACDF in the unmatched and matched analyses respectively. Although a formal minimal clinically important difference (MCID) is yet to be established, this gap was large enough to be detected by the FS3-C but not by the legacy Neck Disability Index (NDI). The FS3-C was modeled after the Forgotten Joint Score, a validated and widely adopted tool in arthroplasty outcomes research. 1 The comparable NDI scores between cohorts provide important context for interpreting the FS3-C difference. The absence of a corresponding NDI difference suggests that FS3-C may be capturing a distinct dimension of postoperative recovery and joint awareness rather than simply reflecting global functional improvement. Notably, this pattern of comparable NDI scores alongside divergent FS3-C scores was observed across unadjusted, multivariable, and propensity-matched analyses, supporting the discriminatory capacity of the FS3-C relative to the NDI.
Existing long-term studies using conventional outcome tools have yielded mixed results when comparing CDR and ACDF, underscoring the need for more sensitive instruments like the FS3-C. While some studies, such as Gornet et al, have demonstrated lower NDI and higher SF-36 physical-component scores after CDR in an FDA-IDE cohort, 15 these results remain the exception; most comparative studies and meta-analyses report minimal or no difference in PROMs like the NDI between CDR and ACDF.10-13 Other investigations have focused on structural or radiographic outcomes rather than patient experience. For instance, meta-analysis of more than 4000 levels by Zou et al showed sustained functional benefit and reduced adjacent-segment degeneration with motion preservation. 8 Lavelle et al similarly found favorable long-term outcomes following CDR with the BRYAN disc, including low rates of reoperation and adjacent segment disease. 16 None of these studies, however, explored joint awareness; our data extend the evidence base by suggesting that a joint-awareness PROM may capture differences between CDR and ACDF not detected by traditional outcome measures.
One hypothesis for observed differences in “forgetting” between cohorts may relate to preserved biomechanics after CDR. This perhaps fosters more natural proprioception and muscle activation patterns, reducing subconscious awareness when the neck is challenged by rapid gaze shifts or high-demand activities. Biomechanical modeling confirms that fusion increases moment transfer and intradiscal pressure at adjacent levels while altering facet loading. 17 Such changes can evoke muscular guarding or stiffness that may heighten segment awareness even in the absence of frank pain, a nuance captured by the FS3-C but obscured by the NDI’s pain-driven weighting.
While our FS3-C results support the notion that preserved segmental motion in CDR may contribute to greater joint “forgetting” and functional confidence, this difference should be interpreted in the context of broader literature. Prior studies have shown that although CDR maintains motion at the index level, 18 ACDF patients often compensate with adjacent segment mobility, preserving global function and reporting comparable clinical satisfaction. 19 Additionally, long-term studies reveal that despite CDR’s theoretical biomechanical advantages, improvements in pain, disability, and quality-of-life measures are often modest and may not reach clinically meaningful thresholds.10,20 These studies support that while CDR has clear advantages in motion preservation and possibly in quality-of-life metrics, 21 the clinical benefits may be modest, not always durable, and often statistically but not clinically significant. 22 Additionally, ACDF continues to perform robustly across all major outcome domains including pain, function, satisfaction, and cost-efficiency. 23 Therefore, FS3-C differences observed in this study, while notable, should be interpreted within the context of overall outcome equivalence between these procedures in long-term follow-up.
From a counseling perspective, the probability of “forgetting” a cervical implant is intuitively meaningful for athletes, manual laborers, and other high-functioning patients. The FS3-C requires less than two minutes to complete, demonstrates higher discriminatory power, and correlates strongly with the NDI (r = −0.61 in our cohort), suggesting it contributes unique information. This discriminatory capacity is important, given prior reviews have identified significant ceiling effects in the NDI, limiting its utility in high-functioning populations. 9
Limitations must be acknowledged. The single-center design, while facilitating protocol consistency, may restrict external validity. Multi-center trials should confirm generalizability and establish MCID thresholds across diverse cultural and linguistic groups. Longitudinal work could evaluate FS3-C responsiveness to perioperative rehabilitation, enhanced-recovery pathways, and next-generation motion-preserving implants. Extending the “forgotten spine” concept to lumbar arthroplasty or minimally invasive fusion may further enrich outcome assessment portfolios.
Our cohorts were not age-matched, which introduces the possibility of confounding due to baseline differences in physical activity, comorbidity burden, or other age-related factors. However, this imbalance reflects real-world surgical selection, where CDR is typically performed in younger, more active patients, and ACDF in older individuals. To address potential confounding, we performed both multivariable regression and propensity score matching adjusting for age, comorbidity burden, sex, and number of operated levels. Procedure type remained independently associated with FS3-C across these analyses, suggesting that baseline differences alone are unlikely to fully account for the observed association. Despite these demographic differences, NDI scores were comparable between groups, and no association with procedure type was observed in adjusted or matched analyses, suggesting that traditional outcome metrics may lack sensitivity to detect experiential differences in function. The FS3-C, by contrast, may be more responsive to differences in proprioception or joint awareness that are particularly relevant to younger, motion-sensitive patients.
Follow-up duration also differed between cohorts, with longer follow-up in the CDR group. As patient-reported outcomes may evolve over time, this difference could influence measures such as joint awareness and should be considered when interpreting the observed FS3-C differences. However, the absence of a corresponding NDI difference provides important context and supports the possibility that FS3-C captures a dimension of recovery not reflected in traditional disability metrics. Future studies with longitudinal follow-up at standardized postoperative time points should further evaluate the relationship between procedure type, recovery duration, and FS3-C scores.
Conclusion
In summary, the FS3-C offers a novel, joint-awareness-based perspective on recovery after cervical spine surgery. By capturing experiential differences that conventional disability metrics may overlook, it has the potential to complement existing PROMs and refine outcome assessment in patients undergoing CDR or ACDF.
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval for this study was obtained from the Hospital for Special Surgery Institutional Review Board (IRB #2023-2507).
Consent to Participate
All participants provided informed consent for both study participation and publication, as approved by the Institution Review Board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, the data was collected and managed using REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384. REDCap is a secure, HIPAA-compliant web-based software platform designed to support data capture and data management for research studies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.